Associations of Objectively-Assessed Smartphone Use with Physical Activity, Sedentary Behavior, Mood, and Sleep Quality in Young Adults: A Cross-Sectional Study





Abstract
1. Introduction
2. Materials and Methods
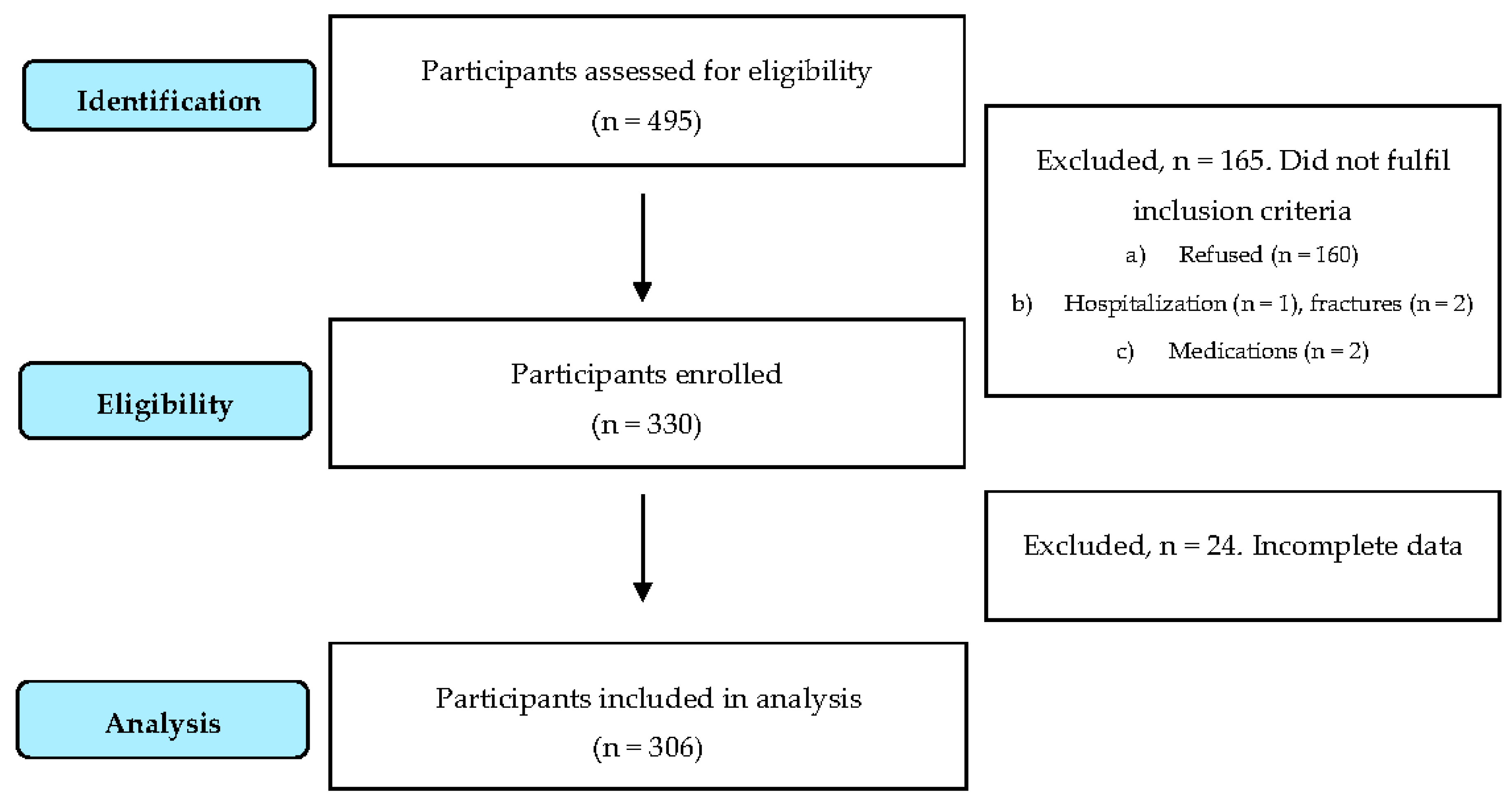
2.1. Participants
2.2. Procedures
2.3. Outcome Measures
2.3.1. Smartphone Use and Screen Time
2.3.2. Physical Activity
2.3.3. Profile of Mood State
2.3.4. Pittsburgh Sleep Quality Index
2.3.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lindsay, T.; Westgate, K.; Wijndaele, K.; Hollidge, S.; Kerrison, N.; Forouhi, N.; Griffin, S.; Wareham, N.; Brage, S. Descriptive epidemiology of physical activity energy expenditure in UK adults (The Fenland study). Int. J. Behav. Nutr. Phys. Act. 2019, 16, 126. [Google Scholar] [CrossRef] [PubMed]
- Füzéki, E.; Engeroff, T.; Banzer, W. Health benefits of light-intensity physical activity: A systematic review of accelerometer data of the national health and nutrition examination survey (NHANES). Sport. Med. 2017, 47, 1769–1793. [Google Scholar] [CrossRef] [PubMed]
- Staiano, A.E.; Martin, C.K.; Champagne, C.M.; Rood, J.C.; Katzmarzyk, P.T. Sedentary time, physical activity, and adiposity in a longitudinal cohort of nonobese young adults. Am. J. Clin. Nutr. 2018, 108, 946–952. [Google Scholar] [CrossRef] [PubMed]
- Ingrid Lunden. 6.1B Smartphone Users Globally By 2020, Overtaking Basic Fixed Phone Subscriptions; Tech Crunch: Bay Area, CA, USA, 2015. [Google Scholar]
- INE. Encuesta sobre Equipamiento y Uso de Tecnologías de Información y Comunicación en los Hogares. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=estadistica_C&cid=1254736176741&menu=ultiDatos&idp=1254735976608 (accessed on 10 February 2020).
- Kolovos, S.; Jimenez-Moreno, A.C.; Pinedo-Villanueva, R.; Cassidy, S.; Zavala, G.A. Association of sleep, screen time and physical activity with overweight and obesity in Mexico. Eat. Weight Disord. 2019, 1–11. [Google Scholar] [CrossRef]
- Madhav, K.C.; Sherchand, S.P.; Sherchan, S. Association between screen time and depression among US adults. Prev. Med. Rep. 2017, 8, 67–71. [Google Scholar] [CrossRef]
- Ghekiere, A.; Van Cauwenberg, J.; Vandendriessche, A.; Inchley, J.; de Matos, G.M.; Borraccino, A.; Gobina, I.; Tynjälä, J.; Deforche, B.; De Clercq, B. Trends in sleeping difficulties among European adolescents: Are these associated with physical inactivity and excessive screen time? Int. J. Public Health 2019, 64, 487–498. [Google Scholar] [CrossRef]
- Panahi, S.; Tremblay, A. Sedentariness and health: Is sedentary behavior more than just physical inactivity? Front. Public Heal. 2018, 6, 258. [Google Scholar] [CrossRef]
- Healy, G.N.; Wijndaele, K.; Dunstan, D.W.; Shaw, J.E.; Salmon, J.; Zimmet, P.Z.; Owen, N. Objectively measured sedentary time, physical activity, and metabolic risk the Australian diabetes, obesity and lifestyle study (AusDiab). Diabetes Care 2008, 31, 369–371. [Google Scholar] [CrossRef]
- Healy, G.N.; Dunstan, D.W.; Salmon, J.; Shaw, J.E.; Zimmet, P.Z.; Owen, N. Television time and continuous metabolic risk in physically active adults. Med. Sci. Sports Exerc. 2008, 40, 639–645. [Google Scholar] [CrossRef]
- Anderson, M.; Jiang, J. Teens, Social Media & Technology 2018; Pew Research Center: Washington, DC, USA, 2018. [Google Scholar]
- Fennell, C.; Barkley, J.E.; Lepp, A. The relationship between cell phone use, physical activity, and sedentary behavior in adults aged 18–80. Comput. Hum. Behav. 2019, 90, 53–59. [Google Scholar] [CrossRef]
- Barkley, J.E.; Lepp, A. Mobile phone use among college students is a sedentary leisure behavior which may interfere with exercise. Comput. Hum. Behav. 2016, 56, 29–33. [Google Scholar] [CrossRef]
- Smetaniuk, P. A preliminary investigation into the prevalence and prediction of problematic cell phone use. J. Behav. Addict. 2014, 3, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Katapally, T.R.; Chu, L.M. Methodology to derive objective screen-state from smartphones: A smart platform study. Int. J. Environ. Res. Public Health 2019, 16, 2275. [Google Scholar] [CrossRef] [PubMed]
- Castro, O.; Bennie, J.; Vergeer, I.; Bosselut, G.; Biddle, S.J.H. How sedentary are university students? A systematic review and meta-analysis. Prev. Sci. 2020, 21, 332–343. [Google Scholar] [CrossRef] [PubMed]
- Grøntved, A.; Ried-Larsen, M.; Møller, N.C.; Kristensen, P.L.; Wedderkopp, N.; Froberg, K.; Hu, F.B.; Ekelund, U.; Andersen, L.B. Youth screen-time behaviour is associated with cardiovascular risk in young adulthood: The European youth heart study. Eur. J. Prev. Cardiol. 2014, 21, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Andrew, P. Social Media Usage: 2005–2015; Pew Research Center: Washington, DC, USA, 2015. [Google Scholar]
- Lepp, A.; Barkley, J.E.; Karpinski, A.C. The relationship between cell phone use, academic performance, anxiety, and satisfaction with life in college students. Comput. Hum. Behav. 2014, 31, 343–350. [Google Scholar] [CrossRef]
- Weisser, B.; Hacke, C.; Wegner, M. Sedentary behavior is a risk factor for higher exercise blood pressure independent of moderate-to-vigorous physical activity (MVPA) in young subjects. J. Am. Soc. Hypertens. 2014, 8, e131. [Google Scholar] [CrossRef]
- Lepp, A.; Barkley, J.E.; Sanders, G.J.; Rebold, M.; Gates, P. The relationship between cell phone use, physical and sedentary activity, and cardiorespiratory fitness in a sample of U.S. college students. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 79. [Google Scholar] [CrossRef]
- Biddle, S.J.H.; Bengoechea-García, E.; Pedisic, Z.; Bennie, J.; Vergeer, I.; Wiesner, G. Screen time, other sedentary behaviours, and obesity risk in adults: A review of reviews. Curr. Obes. Rep. 2017, 6, 134–147. [Google Scholar] [CrossRef]
- Kerrigan, D.J.; Rukstalis, M.R.; Ehrman, J.K.; Keteyian, S.J.; She, R.; Alexander, G.L. 5-2-1-0 Lifestyle risk factors predict obesity in millennials. Clin. Obes. 2019, 9, e12306. [Google Scholar] [CrossRef]
- Wu, X.; Tao, S.; Zhang, Y.; Zhang, S.; Tao, F. Low physical activity and high screen time can increase the risks of mental health problems and poor sleep quality among chinese college students. PLoS ONE 2015, 10, e0119607. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Clark, B.K.; Winkler, E.A.H.; Gardiner, P.A.; Brown, W.J.; Matthews, C.E. Measurement of adults’ sedentary time in population-based studies. Am. J. Prev. Med. 2011, 41, 216–227. [Google Scholar] [CrossRef] [PubMed]
- Rebold, M.J.; Sheehan, T.; Dirlam, M.; Maldonado, T.; O’Donnell, D. The impact of cell phone texting on the amount of time spent exercising at different intensities. Comput. Hum. Behav. 2016, 55, 167–171. [Google Scholar] [CrossRef]
- Fennell, C.; Lepp, A.; Barkley, J. Smartphone use predicts being an “active couch potato” in sufficiently active adults. Am. J. Lifestyle Med. 2019. [Google Scholar] [CrossRef]
- Barkley, J.E.; Lepp, A.; Salehi-Esfahani, S. College students’ mobile telephone use is positively associated with sedentary behavior. Am. J. Lifestyle Med. 2016, 10, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Prince, S.A.; Adamo, K.B.; Hamel, M.; Hardt, J.; Connor Gorber, S.; Tremblay, M. A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 56. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F. Measuring physical activity. J. Public Heal. Manag. Pr. 2010, 16, 404–410. [Google Scholar] [CrossRef]
- Menaspà, P. Effortless activity tracking with google fit. Br. J. Sports Med. 2015, 49, 1598. [Google Scholar] [CrossRef]
- Degroote, L.; De Bourdeaudhuij, I.; Verloigne, M.; Poppe, L.; Crombez, G. The accuracy of smart devices for measuring physical activity in daily life: Validation study. JMIR Mhealth Uhealth 2018, 6, e10972. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-Country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Lorr, M.; McNair, D.M.; Droppleman, L.F. Manual: Profile of Mood States; Educational and Industrial Testing Service: San Diego, CA, USA, 1971. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Fakhouri, T.H.I.; Hughes, J.P.; Brody, D.J.; Kit, B.K.; Ogden, C.L. Physical activity and screen-time viewing among elementary school-aged children in the United States from 2009 to 2010. JAMA Pediatr. 2013, 167, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Vrijheid, M.; Armstrong, B.K.; Bédard, D.; Brown, J.; Deltour, I.; Iavarone, I.; Krewski, D.; Lagorio, S.; Moore, S.; Richardson, L.; et al. Recall bias in the assessment of exposure to mobile phones. J. Expo. Sci. Environ. Epidemiol. 2009, 19, 369–381. [Google Scholar] [CrossRef] [PubMed]
- Biddle, S.J.H.; Pearson, N.; Ross, G.M.; Braithwaite, R. Tracking of sedentary behaviours of young people: A systematic review. Prev. Med. 2010, 51, 345–351. [Google Scholar] [CrossRef]
- Falbe, J.; Rosner, B.; Willett, W.C.; Sonneville, K.R.; Hu, F.B.; Field, A.E. Adiposity and different types of screen time. Pediatrics 2013, 132, e1497. [Google Scholar] [CrossRef]
- De Oliveira, R.G.; Guedes, D.P. Determinants of lifestyle associated with metabolic syndrome in brazilian adolescents. Nutr. Hosp. 2019, 36, 826–833. [Google Scholar] [CrossRef]
- Stuckey, M.I.; Carter, S.W.; Knight, E. The role of smartphones in encouraging physical activity in adults. Int. J. Gen. Med. 2017, 10, 293–303. [Google Scholar] [CrossRef]
- Shimoga, S.V.; Erlyana, E.; Rebello, V. Associations of social media use with physical activity and sleep adequacy among adolescents: Cross-sectional survey. J. Med. Internet Res. 2019, 21, e14290. [Google Scholar] [CrossRef]
- Fanning, J.; Mullen, S.P.; Mcauley, E. Increasing physical activity with mobile devices: A meta-analysis. J. Med. Internet Res. 2012, 14, e161. [Google Scholar] [CrossRef]
- Barkley, J.E.; Lepp, A. Cellular telephone use during free-living walking significantly reduces average walking speed. BMC Res. Notes 2016, 9, 195. [Google Scholar] [CrossRef]
- Rebold, M.J.; Sheehan, T.; Dirlam, M.; Maldonado, T.; O’Donnell, D. The Impact of Cell Phone Texting on the Amount of Time Spent Exercising at Different Intensities; Educational and Industrial Testing Service: San Diego, CA, USA, 2015. [Google Scholar]
- Tebar, W.R.; Ritti Dias, R.M.; Scarabottolo, C.C.; Gil, F.C.S.; Saraiva, B.T.C.; Delfino, L.D.; Zanuto, E.F.; Vanderlei, L.C.M.; Christofaro, D.G.D. Sedentary behavior is more related with cardiovascular parameters in normal weight than overweight adolescents. J. Public Health 2019. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Alkandari, J.R.; Andersen, L.B.; Bauman, A.E.; Brownson, R.C.; et al. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too much sitting: The population health science of sedentary behavior. Exerc. Sport Sci. Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Tao, S.; Zhang, S.; Zhang, Y.; Chen, K.; Yang, Y.; Hao, J.; Tao, F. Impact of screen time on mental health problems progression in youth: A 1-year follow-up study. BMJ Open 2016, 6, e011533. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Li, K.; Kim, M.; Lee, S.; Seo, D.C. Association between psychological distress and elevated use of electronic devices among U.S. adolescents: Results from the youth risk behavior surveillance 2009–2017. Addict. Behav. 2019, 90, 112–118. [Google Scholar]
- Kwon, S.; Janz, K.F.; Letuchy, E.M.; Burns, T.L.; Levy, S.M. Developmental trajectories of physical activity, sports, and television viewing during childhood to young adulthood: Iowa bone development study. JAMA Pediatr. 2015, 169, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Foley, L.; Dumuid, D.; Atkin, A.J.; Olds, T.; Ogilvie, D. Patterns of health behaviour associated with active travel: A compositional data analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 26. [Google Scholar] [CrossRef] [PubMed]
- Börnhorst, C.; Wijnhoven, T.M.A.; Kunešová, M.; Yngve, A.; Rito, A.I.; Lissner, L.; Duleva, V.; Petrauskiene, A.; Breda, J. WHO European childhood obesity surveillance initiative: Associations between sleep duration, screen time and food consumption frequencies. BMC Public Health 2015, 15, 442. [Google Scholar] [CrossRef]
- Fobian, A.D.; Avis, K.; Schwebel, D.C. Impact of media use on adolescent sleep efficiency. J. Dev. Behav. Pediatr. 2016, 37, 9–14. [Google Scholar] [CrossRef]
- Perrault, A.A.; Bayer, L.; Peuvrier, M.; Afyouni, A.; Ghisletta, P.; Brockmann, C.; Spiridon, M.; Hulo Vesely, S.; Haller, D.M.; Pichon, S.; et al. Reducing the use of screen electronic devices in the evening is associated with improved sleep and daytime vigilance in adolescents. Sleep 2019, 42, 125. [Google Scholar] [CrossRef]
- Leech, J.A. Changes in sleep duration and recreational screen time among Canadians, 1998–2010. J. Sleep Res. 2017, 26, 202–209. [Google Scholar] [CrossRef]
- Wang, X.; Perry, A.C. Metabolic and physiologic responses to video game play in 7-to 10-year-old boys. Arch. Pediatr. Adolesc. Med. 2006, 160, 411–415. [Google Scholar] [CrossRef] [PubMed]
- King, D.L.; Delfabbro, P.H.; Zwaans, T.; Kaptsis, D. Sleep interference effects of pathological electronic media use during adolescence. Int. J. Ment. Health Addict. 2014, 12, 21–35. [Google Scholar] [CrossRef]
- Faught, E.L.; Qian, W.; Carson, V.L.; Storey, K.E.; Faulkner, G.; Veugelers, P.J.; Leatherdale, S.T. The longitudinal impact of diet, physical activity, sleep, and screen time on Canadian adolescents’ academic achievement: An analysis from the COMPASS study. Prev. Med. 2019, 125, 24–31. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Male (n = 184) | Female (n = 122) | Total (n = 306) |
|---|---|---|---|
| Age, mean (SD) | 20.8 (1.3) | 20.7 (1.6) | 20.7 (1.4) |
| Sex (%) | 60 | 40 | - |
| Professional status, n (%) | |||
| Work full/part time | 112 (62) | 68 (38) | 180 (59) |
| Unemployed | 72 (57) | 54 (43) | 126 (41) |
| Smartphone use | |||
| Weekday use (min/day) | 266 (94) | 238 (105) | 254 (99) |
| Weekend use (min/day) | 259 (111) | 220 (104) | 243 (110) |
| Subjectively measured physical activity | |||
| Walking time (min/week) | 264 (171) | 240 (165) | 253 (168) |
| Moderate PA (min/week) | 192 (153) | 114 (136) | 157 (151) |
| Vigorous PA (min/week) | 240 (149) | 127 (143) | 190 (156) |
| Objectively measured physical activity | |||
| Weekday steps (steps/day) | 8117 (3439) | 7046 (3724) | 7623 (3606) |
| Weekend steps (steps/day) | 7848 (3583) | 7047 (3938) | 7486 (3761) |
| Sedentary behavior | |||
| Sitting time (hours/day) | 4.6 (2.4) | 5.5 (2.7) | 5.1 (2.6) |
| Meeting WHO PA guidelines, yes (%) c | 66.8 | 33.2 | 71.3 |
| POMS Global Score a | 22.2 (22.4) | 21.0 (22.4) | 21.8 (22.4) |
| Vigor, mean (SD) | 16.0 (5.0) | 16.3 (4.6) | 16.1 (4.8) |
| Fatigue, mean (SD) | 8.6 (6.5) | 7.5 (5.7) | 8.2 (6.3) |
| Tension, mean (SD) | 9.27 (5.8) | 9.6 (5.2) | 9.4 (5.6) |
| Depression, mean (SD) | 3.54 (4.9) | 3.8 (4.9) | 3.7 (4.9) |
| Anger, mean (SD) | 10.6 (6.9) | 10.1 (6.6) | 10.4 (6.7) |
| Confusion, mean (SD) | 5.92 (4.1) | 6.3 (3.9) | 6.1 (4.0) |
| PSQI Global Score (0–21) b | 3.5 (2.9) | 3.9 (3.0) | 3.7 (3.0) |
| Impaired sleep (PSQI score >5) % | 51 | 49 | 30.3 |
| Predictor | B | p-Value | Adjusted R2 | β | 95% Confidence Interval | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| PSQI Global Score | 16.36 | 0.265 | 0.12 | 0.076 | −0.058 | 0.209 |
| POMS Global Score | 4.95 | <0.001 | 0.185 | 0.052 | 0.318 | |
| Hours sitting/day | 22.4 | 0.155 | 0.13 | 0.089 | −0.034 | 0.211 |
| POMS_confusion | 36.4 | <0.001 | 0.218 | 0.097 | 0.339 | |
| N° steps/week | −0.01 | 0.619 | 0.13 | −0.08 | −0.202 | 0.048 |
| POMS Global Score | 5.81 | <0.001 | 0.213 | 0.091 | 0.336 | |
| Hours sitting/day | 4.68 | 0.049 | 0.12 | 0.126 | 0.003 | 0.249 |
| METs moderate PA | −0.03 | 0.012 | −0.161 | −0.2861 | −0.035 | |
| Hours sitting/day | 4.48 | 0.048 | 0.15 | 0.121 | 0.005 | 0.242 |
| METs moderate PA | −0.02 | 0.003 | −0.150 | −0.274 | −0.027 | |
| POMS Global Score | 0.69 | <0.001 | 0.176 | 0.057 | 0.296 | |
| Predictor | X2 | p | Odds Ratio | 95% Confidence Interval | |||
|---|---|---|---|---|---|---|---|
| Lower | Upper | p | |||||
| Smartphone Use | Low Physical Activity | 40.9 | <0.001 | 2.981 | 1.325 | 7.847 | 0.027 |
| Sitting time | 30.5 | <0.001 | 1.544 | 0.758 | 3.163 | 0.232 | |
| POMS_Vigor | 45.2 | <0.001 | 1.115 | 0.399 | 3.112 | 0.835 | |
| POMS_Fatigue | 45.0 | <0.001 | 1.644 | 0.610 | 4.436 | 0.326 | |
| POMS_Tension | 41.3 | <0.001 | 2.161 | 0.822 | 5.681 | 0.118 | |
| POMS_Depression | 46.9 | <0.001 | 2.400 | 0.948 | 6.077 | 0.065 | |
| POMS_Anger | 45.5 | <0.001 | 3.948 | 1.450 | 10.752 | 0.007 | |
| POMS_Confusion | 48.1 | <0.001 | 2.756 | 1.123 | 6.761 | 0.027 | |
| Poor sleep quality | 39.3 | <0.001 | 2.679 | 1.126 | 6.377 | 0.026 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grimaldi-Puyana, M.; Fernández-Batanero, J.M.; Fennell, C.; Sañudo, B. Associations of Objectively-Assessed Smartphone Use with Physical Activity, Sedentary Behavior, Mood, and Sleep Quality in Young Adults: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 3499. https://doi.org/10.3390/ijerph17103499
Grimaldi-Puyana M, Fernández-Batanero JM, Fennell C, Sañudo B. Associations of Objectively-Assessed Smartphone Use with Physical Activity, Sedentary Behavior, Mood, and Sleep Quality in Young Adults: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2020; 17(10):3499. https://doi.org/10.3390/ijerph17103499
Chicago/Turabian StyleGrimaldi-Puyana, Moisés, José María Fernández-Batanero, Curtis Fennell, and Borja Sañudo. 2020. "Associations of Objectively-Assessed Smartphone Use with Physical Activity, Sedentary Behavior, Mood, and Sleep Quality in Young Adults: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 17, no. 10: 3499. https://doi.org/10.3390/ijerph17103499
APA StyleGrimaldi-Puyana, M., Fernández-Batanero, J. M., Fennell, C., & Sañudo, B. (2020). Associations of Objectively-Assessed Smartphone Use with Physical Activity, Sedentary Behavior, Mood, and Sleep Quality in Young Adults: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 17(10), 3499. https://doi.org/10.3390/ijerph17103499