Social Media-Based Health Management Systems and Sustained Health Engagement: TPB Perspective

 ,
,
Abstract
1. Introduction
1.1. Openness to Experience
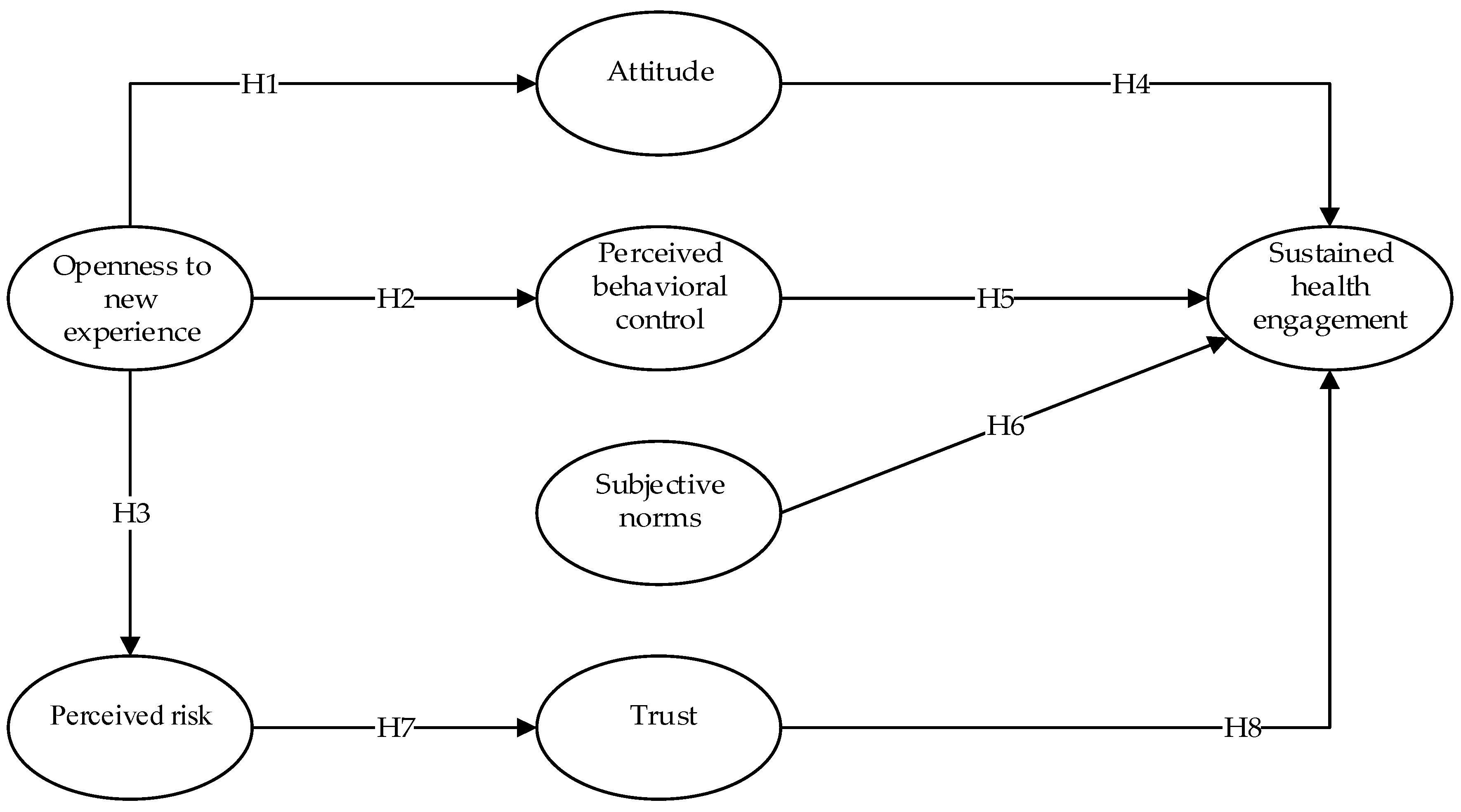
1.2. Theory of Planned Behavior
1.3. Perceived Risk and Trust
2. Methodology
2.1. Toolkits
2.2. Sample and Data Collection
3. Results
3.1. Analysis of Measurement Model
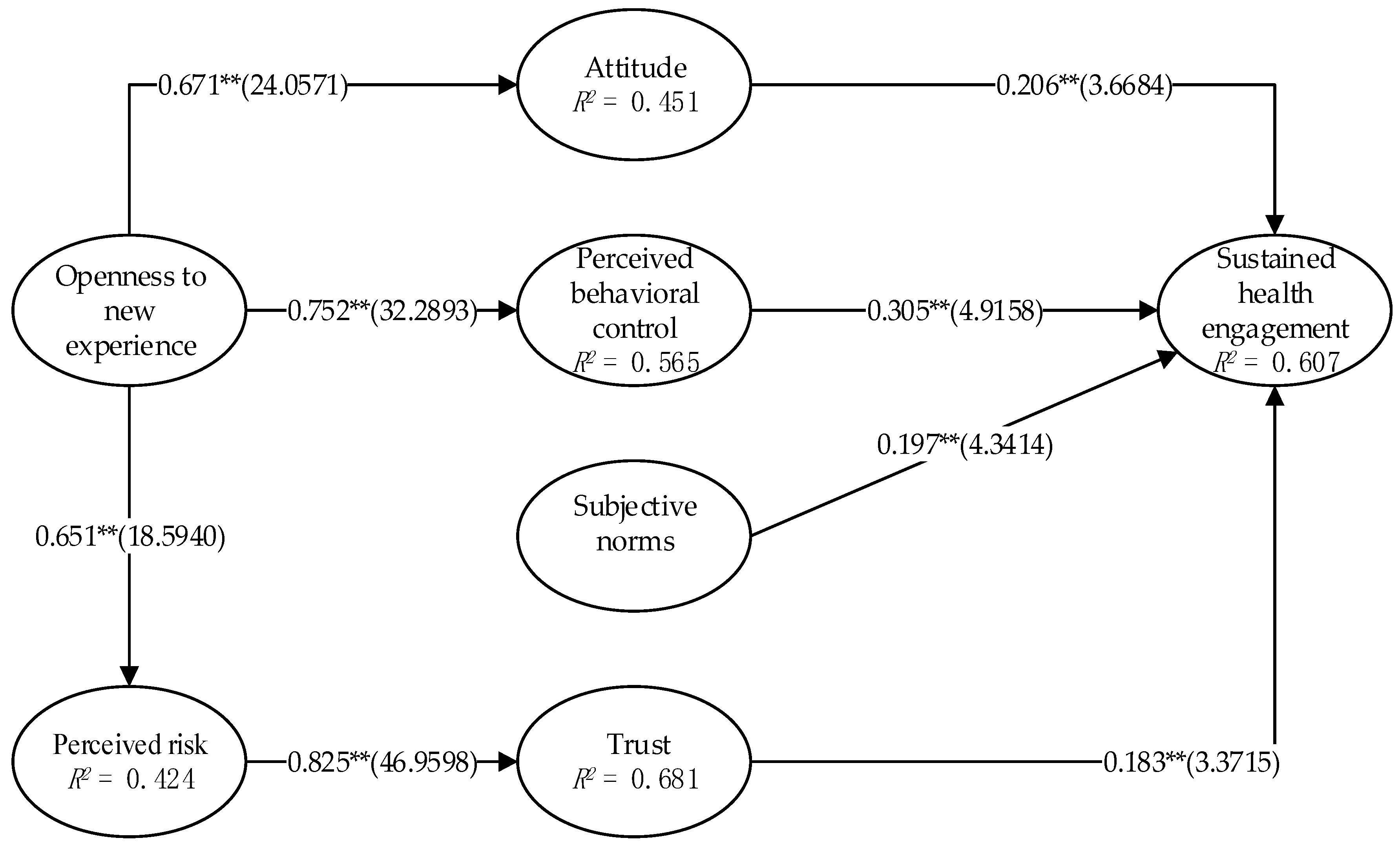
3.2. Analysis of Structural Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- De Brún, A.; McAuliffe, E. Social Network Analysis as a Methodological Approach to Explore Health Systems: A Case Study Exploring Support among Senior Managers/Executives in a Hospital Network. Int. J. Environ. Res. Public Health 2018, 15, 511. [Google Scholar] [CrossRef] [PubMed]
- Khajeheian, D.; Colabi, A.M.; Shah, N.B.A.K.; Wan Mohamed Radzi, C.W.J.B.; Jenatabadi, H.S. Effect of Social Media on Child Obesity: Application of Structural Equation Modeling with the Taguchi Method. Int. J. Environ. Res. Public Health 2018, 15, 1343. [Google Scholar] [CrossRef] [PubMed]
- Marqués-Sánchez, P.; Muňoz-Doyague, M.F.; Martínez, Y.V.; Everett, M.; Serrano-Fuentes, N.; Van Bogaert, P.; Vassilev, I.; Reeves, D. The Importance of External Contacts in Job Performance: A Study in Healthcare Organizations Using Social Network Analysis. Int. J. Environ. Res. Public Health 2018, 15, 1345. [Google Scholar] [CrossRef]
- Mikkelsen, B.E.; Bloch, P.; Reinbach, H.C.; Buch-Andersen, T.; Winkle, L.L.; Toft, U.; Glumer, C.; Jensen, B.B.; Aagaaed-Hansen, J. Project SoL—A Community-Based, Multi-Component Health Promotion Intervention to Improve Healthy Eating and Physical Activity Practices among Danish Families with Young Children Part 2: Evaluation. Int. J. Environ. Res. Public Health 2018, 15, 1513. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Wu, S.; Wu, H.; Xia, Q.; Li, N. Living Arrangements and Health-Related Quality of Life in Chinese Adolescents Who Migrate from Rural to Urban Schools: Mediating Effect of Social Support. Int. J. Environ. Res. Public Health 2017, 14, 1249. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, M.S.; Nørrevang, O. A model for managing patient booking in a radiotherapy department with differentiated waiting times. Acta Oncol. 2009, 48, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Liu, Z.; Wu, S.; Wang, L.; Yang, G. Study on the medical information service system based on the WeChat platform. Chin. Med. Devices 2015, 30, 82–84. [Google Scholar]
- Wang, H.; Zhang, Q.; Ip, M.; Lau, J.T.F. Social media-based conversational agents for health management and interventions. Computer 2018, 51, 26–33. [Google Scholar] [CrossRef]
- Velasco, E.; Agheneza, T.; Denecke, K.; Kirchner, G.; Eckmanns, T. Social media and internet-based data in global systems for public health surveillance: A systematic review. Milbank Q. 2014, 92, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Li, G.-C.; Chen, C.-L.; Chen, H.-C.; Lin, F.; Gu, C. Design of a secure and effective medical cyber-physical system for ubiquitous telemonitoring pregnancy. Concurr. Comput. 2018, 30, e4236. [Google Scholar] [CrossRef]
- Archer, N.; Cocosila, M. A Comparison of Physician Pre-Adoption and Adoption Views on Electronic Health Records in Canadian Medical Practices. J. Med. Internet Res. 2011, 13, e57. [Google Scholar] [CrossRef] [PubMed]
- Baker, A. Crossing the Quality Chasm: A New Health System for the 21st Century. BMJ 2011, 323, 1192. [Google Scholar] [CrossRef]
- Shortell, S.M.; O’Brien, J.L.; Carman, J.M.; Foster, R.W.; Hughes, E.F.; Boerstler, H.; O’Connor, E.J. Assessing the impact of continuous quality improvement/total quality management: Concept versus implementation. Health Serv. Res. 1995, 30, 377–401. [Google Scholar] [PubMed]
- March, J.G. Continuity and change in theories of organizational action. Adm. Sci. Q. 1996, 41, 278–287. [Google Scholar] [CrossRef]
- Otte, E.; Rousseau, R. Social network analysis: A powerful strategy, also for the information sciences. J. Inf. Sci. 2002, 28, 441–453. [Google Scholar] [CrossRef]
- Fareedi, A.A.; Hassan, S. The impact of social media networks on healthcare process knowledge management (using of semantic web platforms). In Proceedings of the 2014 14th International Conference on Control, Automation and Systems, Seoul, South Korea, 22–25 October 2014; IEEE: Piscatvi, NJ, USA, 2014. [Google Scholar] [CrossRef]
- Bhattacherjee, A. Understanding information systems continuance: An expectation-confirmation model. MIS Q. 2001, 25, 351–370. [Google Scholar] [CrossRef]
- Bhattacherjee, A.; Premkumar, G. Understanding Changes in Belief and Attitude toward Information Technology Usage: A Theoretical Model and Longitudinal Test. MIS Q. 2004, 28, 229–254. [Google Scholar] [CrossRef]
- Venkatesh, V.; Goyal, S. Expectation disconfirmation and technology adoption: Polynomial modeling and response surface analysis. MIS Q. 2010, 34, 281–303. [Google Scholar] [CrossRef]
- Pavlou, P.; Fygenson, M. Understanding and predicting electronic commerce adoption: An extension of the theory of planned behavior. MIS Q. 2006, 30, 115–143. [Google Scholar] [CrossRef]
- Venkatesh, V.; Thong, J.Y.L.; Chan, F.K.Y.; Hu, P.J.-H.; Brown, S.A. Extending the two-stage information systems continuance model: Incorporating UTAUT predictors and the role of context. Inf. Syst. J. 2011, 21, 527–555. [Google Scholar] [CrossRef]
- Sun, Y.; Jeyaraj, A. Information technology adoption and continuance: A longitudinal study of individuals’ behavioral intentions. Inf. Manag. 2013, 50, 457–465. [Google Scholar] [CrossRef]
- Fishbein, M. A theory of reasoned action: Some applications and implications. Nebr. Symp. Motiv. 1980, 27, 65. [Google Scholar]
- Ajzen, I. The theory of planned behavior, organizational behavior and human decision processes. J. Leis. Res. 1991, 50, 176–211. [Google Scholar]
- Ajzen, I.; Fishbein, M. Attitudes and the Attitude-Behavior Relation: Reasoned and Automatic Processes. Eur. Rev. Soc. Psychol. 2000, 11, 1–33. [Google Scholar] [CrossRef]
- Fishbein, M.; Ajzen, I. Belief, Attitude, Intention and Behaviour: An introduction to theory and research. Philos. Rhetor. 1977, 41, 842–844. [Google Scholar]
- Ajzen, I. Attitudes, Personality, and Behavior; McGraw-Hill Education: New York, NY, USA, 2005. [Google Scholar]
- Maio, G.R.; Haddock, G. The Psychology of Attitudes and Attitude Change; Sage: London, UK, 2019. [Google Scholar]
- Saroglou, V.; Jaspard, J.-M. Personality and religion: From eysenck’s taxonomy to the five-factor model. Arch. Psychol. Relig. 2000, 23, 41–70. [Google Scholar] [CrossRef]
- Schmitt, D.P.; Allik, J.; Mccrae, R.R.; Benetmartínez, V. The Geographic Distribution of Big Five Personality Traits: Patterns and Profiles of Human Self-Description across 56 Nations. J. Cross Cult. Psychol. 2007, 38, 173–212. [Google Scholar] [CrossRef]
- Larsen, R.J.; Buss, D.M. Personality Psychology: Domains of Knowledge about Human Nature; McGraw Hill Education: New York, NY, USA, 2017. [Google Scholar]
- Kapogiannis, D.; Sutin, A.; Davatzikos, C.; Costa, P., Jr.; Resnick, S. The five factors of personality and regional cortical variability in the Baltimore longitudinal study of aging. Hum. Brain Mapp. 2013, 34, 2829–2840. [Google Scholar] [CrossRef]
- Davis, D.D.; Bjornberg, N.H. Flourishing in the Workplace through Meditation and Mindfulness. Ind. Organ. Psychol. 2015, 8, 667–674. [Google Scholar] [CrossRef]
- Bauer, R.A. Consumer Behavior as Risk Taking. In Proceedings of the 43rd National Conference of the American Marketing Assocation, Chicago, IL, USA, 15–17 June 1960; American Marketing Association: Chicago, IL, USA, 1960. [Google Scholar]
- van der Weerd, W.; Timmermans, D.R.; Beaujean, D.J.; Oudhoff, J.; van Steenbergen, J.E. Monitoring the level of government trust, risk perception and intention of the general public to adopt protective measures during the influenza A (H1N1) pandemic in the Netherlands. BMC Public Health 2011, 11, 575. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.; Lin, H.-N.; Liu, Y.-P. Predicting the use of pirated software: A contingency model integrating perceived risk with the theory of planned behavior. J. Bus. Ethics 2010, 91, 237–252. [Google Scholar] [CrossRef]
- McCrae, R.R.; Terracciano, A. Universal features of personality traits from the observer’s perspective: Data from 50 cultures. J. Pers. Soc. Psychol. 2005, 88, 547. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.H.; Lee, J.Y. Nursing Students’ Perception, Experience and Attitude on Complementary and Alternative Therapies. J. East West Nurs. Res. 2015, 21, 110–118. [Google Scholar]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall, Inc.: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Hascher, T.; Hagenauer, G. Openness to theory and its importance for pre-service teachers’ self-efficacy, emotions, and classroom behaviour in the teaching practicum. Int. J. Educ. Res. 2016, 77, 15–25. [Google Scholar] [CrossRef]
- Hull, D.M.; Booker, D.D.; Näslund-Hadley, E.I. Teachers’ self-efficacy in Belize and experimentation with teacher-led math inquiry. Teach. Teach. Educ. 2016, 56, 14–24. [Google Scholar] [CrossRef]
- Manstead, A.S.R.; van Eekelen, S.A.M. Distinguishing between perceived behavioral control and self-efficacy in the domain of academic achievement intentions and behaviors. J. Appl. Soc. Psychol. 1998, 28, 1375–1392. [Google Scholar] [CrossRef]
- Xie, C. The Influence of Perceived Risk on Purchase Intention—A Case study of Taobao Online Shopping of Fresh Fruit. Asian Agric. Res. 2017, 9, 30–35. [Google Scholar]
- Miyazaki, A.D.; Fernandez, A. Consumer perceptions of privacy and security risks for online shopping. J. Consum. Aff. 2001, 35, 27–44. [Google Scholar] [CrossRef]
- Pathman, D.E.; Konrad, T.R.; Freed, G.L.; Freeman, V.A.; Koch, G.G. The awareness-to-adherence model of the steps to clinical guideline compliance: The case of pediatric vaccine recommendations. Med. Care 1996, 34, 873–889. [Google Scholar] [CrossRef]
- Howes, O.D.; Vergunst, F.; Gee, S.; Mcguire, P.; Kapur, S.; Taylor, D. Adherence to treatment guidelines in clinical practice: Study of antipsychotic treatment prior to clozapine initiation. Br. J. Psychiatry 2012, 201, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Solà, I.; Carrasco, J.M.; del Campo, P.D.; Gracia, J.; Orrego, C.; Martínez, F.; de Gaminde, I. Attitudes and perceptions about clinical guidelines: A qualitative study with Spanish physicians. PLoS ONE 2014, 9, e86065. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I.; Madden, T.J. Prediction of goal-directed behavior: Attitudes, intentions, and perceived behavioral control. J. Exp. Soc. Psychol. 1986, 22, 453–474. [Google Scholar] [CrossRef]
- Bhattacherjee, A. Acceptance of e-commerce services: The case of electronic brokerages. IEEE Trans. Syst. Man. Cybern. A. Syst. Hum. 2000, 30, 411–420. [Google Scholar] [CrossRef]
- Venkatesh, V.; Davis, F.D. A theoretical extension of the technology acceptance model: Four longitudinal field studies. Manag. Sci. 2000, 46, 186–204. [Google Scholar] [CrossRef]
- Bagozzi, R.P.; Dholakia, U.M. Intentional social action in virtual communities. J. Interact. Mark. 2002, 16, 2–21. [Google Scholar] [CrossRef]
- Bock, G.-W.; Zmud, R.W.; Kim, Y.-G.; Lee, J.-N. Behavioral intention formation in knowledge sharing: Examining the roles of extrinsic motivators, social-psychological forces, and organizational climate. MIS Q. 2005, 29, 87–111. [Google Scholar] [CrossRef]
- Fraedrich, J.P.; Ferrell, O. The impact of perceived risk and moral philosophy type on ethical decision making in business organizations. J. Bus. Res. 1992, 24, 283–295. [Google Scholar] [CrossRef]
- Doolin, B. Power and resistance in the implementation of a medical management information system. Inf. Syst. J. 2004, 14, 343–362. [Google Scholar] [CrossRef]
- Kesharwani, A.; Bisht, S.S. The impact of trust and perceived risk on internet banking adoption in India: An extension of technology acceptance model. Int. J. Bank Mark. 2012, 30, 303–322. [Google Scholar] [CrossRef]
- McKnight, D.H.; Chervany, N.L. What trust means in e-commerce customer relationships: An interdisciplinary conceptual typology. Int. J. Electron. Comer. 2001, 6, 35–59. [Google Scholar] [CrossRef]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the sem. J. Strength Cond. Res. 2005, 19, 231–240. [Google Scholar] [PubMed]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis. Technometrics 2013, 49, 103–104. [Google Scholar]
- Carrasco, J.-L.; Jover, L. Assessing individual bioequivalence using the structural equation model. Stat. Med. 2003, 22, 901–912. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, R.; Lilien, G.L.; Rangaswamy, A. Technological opportunism and radical technology adoption: An application to e-business. J. Mark. 2002, 66, 47–60. [Google Scholar] [CrossRef]
- Multivariate Data Analysis: Pearson New International Education. Available online: https://is.muni.cz/el/1423/podzim2017/PSY028/um/_Hair_-_Multivariate_data_analysis_7th_revised.pdf (accessed on 18 March 2019).
- Brislin, R.W. Cross-cultural research methods. Environ. Cult. 1980, 4, 47–82. [Google Scholar]
- Sykes, T.A.; Venkatesh, V.; Gosain, S. Model of acceptance with peer support: A social network perspective to understand employees’ system use. MIS Q. 2009, 33, 371–393. [Google Scholar] [CrossRef]
- Vozniuk, A.; Holzer, A.C.; Govaerts, S.; Mazuze, J.; Gillet, D. Graspeo: A Social Media Platform for Knowledge Management in NGOs. In Proceedings of the International Conference on Information & Communication Technologies and Development, Singapore, 15–18 May 2015; EPFL Scientific Publications: Lausanne, Switzerland, 2015. [Google Scholar]
- Cameron, D.; Smith, G.A.; Daniulaityte, R.; Sheth, A.P.; Dave, D.; Chen, L.; Anand, G.; Carlson, R.; Watkins, K.Z.; Falck, R. PREDOSE: A semantic web platform for drug abuse epidemiology using social media. J. Biomed. Inform. 2013, 46, 985–997. [Google Scholar] [CrossRef] [PubMed]
- Razmerita, L.; Phillips-Wren, G.; Jain, L.C. Innovations in Knowledge Management—The Impact of Social Media, Semantic Web and Cloud Computing; Springer: Berlin, Germany, 2016. [Google Scholar]
- Tyagi, A.; Tyagi, R. Social media: Opportunities and challenges for human resource management. IJKBO 2012, 2. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Construct | Item Statistics | |||
|---|---|---|---|---|
| Construct Items | Mean | Std. Deviation | Loading | |
| Openness to New Experience | OtE1 * | 5.44 | 1.35 | 0.856783 |
| OtE2 * | 5.64 | 1.28 | 0.905741 | |
| OtE3 * | 5.26 | 1.44 | 0.837521 | |
| Attitude | Attitude1 | 6.07 | 1.1 | 0.826909 |
| Attitude2 | 6.02 | 1.1 | 0.827472 | |
| Attitude3 | 6.02 | 1.05 | 0.848277 | |
| Attitude4 | 5.93 | 1.16 | 0.822302 | |
| Perceived Behavioral Control | PBC1 * | 5.77 | 1.2 | 0.829332 |
| PBC2 * | 5.86 | 1.19 | 0.862304 | |
| PBC3 * | 5.65 | 1.28 | 0.820957 | |
| Subjective Norms | SN1 | 4.96 | 1.71 | 0.756089 |
| SN2 | 5.62 | 1.35 | 0.819427 | |
| SN3 | 5.55 | 1.31 | 0.822804 | |
| Perceived Risk | PR1 | 5.75 | 1.26 | 0.891781 |
| PR2 | 5.63 | 1.24 | 0.917101 | |
| Trust | Trust1 | 5.6 | 1.23 | 0.804032 |
| Trust2 | 5.44 | 1.24 | 0.824332 | |
| Trust3 | 5.61 | 1.23 | 0.847866 | |
| Trust4 | 5.78 | 1.19 | 0.869369 | |
| Sustained Health Engagement | SU1 | 5.69 | 1.2 | 0.888886 |
| SU2 | 5.62 | 1.29 | 0.889958 | |
| Construct Items | AVE 1 | Composite Reliability | Cronbach’s Alpha | Attitude | SU | OtE | PBC | PR | SN | Trust |
|---|---|---|---|---|---|---|---|---|---|---|
| Attitude | 0.6911 | 0.8995 | 0.851 | 0.8313 * | ||||||
| SU | 0.792 | 0.8839 | 0.7374 | 0.6929 | 0.89 * | |||||
| OtE | 0.752 | 0.9008 | 0.835 | 0.6714 | 0.655 | 0.8672 * | ||||
| PBC | 0.7018 | 0.8759 | 0.788 | 0.7796 | 0.7148 | 0.7515 | 0.8377 * | |||
| PR | 0.8182 | 0.9 | 0.7786 | 0.6281 | 0.6234 | 0.651 | 0.654 | 0.9045 * | ||
| SN | 0.64 | 0.8419 | 0.7188 | 0.6269 | 0.6351 | 0.6408 | 0.6208 | 0.6024 | 0.8 * | |
| Trust | 0.7002 | 0.9032 | 0.8571 | 0.6897 | 0.6661 | 0.713 | 0.6961 | 0.8255 | 0.6562 | 0.8368 * |
| Hypothesized Path. | Standardized Path Coefficients | t-Value | Results |
|---|---|---|---|
| H1: OtE -> Attitude | 0.671 | 24.0571 | Yes |
| H2: OtE -> PBC | 0.752 | 32.2893 | Yes |
| H3: OtE -> PR | 0.651 | 18.594 | Yes |
| H4: Attitude -> SU | 0.206 | 3.6684 | Yes |
| H5: PBC -> SU | 0.305 | 4.9158 | Yes |
| H6: SN -> SU | 0.197 | 4.3414 | Yes |
| H7: PR -> Trust | 0.825 | 46.9598 | Yes |
| H8: Trust -> SU | 0.183 | 3.3715 | Yes |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gu, D.; Guo, J.; Liang, C.; Lu, W.; Zhao, S.; Liu, B.; Long, T. Social Media-Based Health Management Systems and Sustained Health Engagement: TPB Perspective. Int. J. Environ. Res. Public Health 2019, 16, 1495. https://doi.org/10.3390/ijerph16091495
Gu D, Guo J, Liang C, Lu W, Zhao S, Liu B, Long T. Social Media-Based Health Management Systems and Sustained Health Engagement: TPB Perspective. International Journal of Environmental Research and Public Health. 2019; 16(9):1495. https://doi.org/10.3390/ijerph16091495
Chicago/Turabian StyleGu, Dongxiao, Jingjing Guo, Changyong Liang, Wenxing Lu, Shuping Zhao, Bing Liu, and Tianyue Long. 2019. "Social Media-Based Health Management Systems and Sustained Health Engagement: TPB Perspective" International Journal of Environmental Research and Public Health 16, no. 9: 1495. https://doi.org/10.3390/ijerph16091495
APA StyleGu, D., Guo, J., Liang, C., Lu, W., Zhao, S., Liu, B., & Long, T. (2019). Social Media-Based Health Management Systems and Sustained Health Engagement: TPB Perspective. International Journal of Environmental Research and Public Health, 16(9), 1495. https://doi.org/10.3390/ijerph16091495