Reduction of Dental Caries Among Children and Adolescents From a 15-Year Community Water Fluoridation Program in a Township Area, Korea


Abstract
1. Introduction
2. Materials and Methods
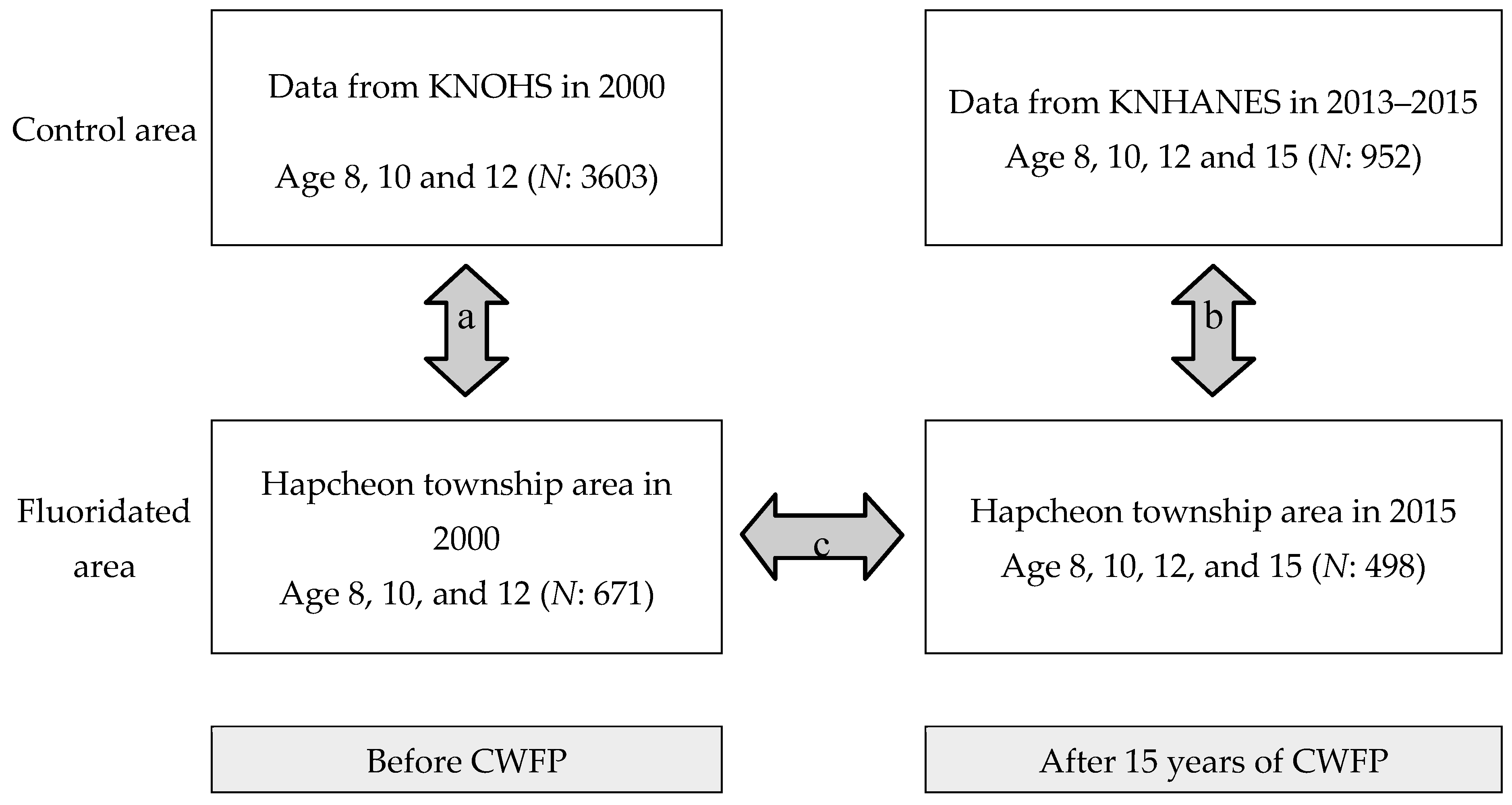
2.1. Participants
2.2. Oral Examination
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Health Insurance Review and Assessment Service. 2017 Medical Treatment Expense Statistics; National Health Insurance Service: Osong, Korea, 2017; pp. 59–62. [Google Scholar]
- Lee, S.K.; Lee, K.W. Reasons for extracted permanent teeth in Korean population. J. Kor. Acad. Oral Health 2001, 25, 139–163. [Google Scholar]
- Kim, H.N.; Han, D.H.; Jun, E.J.; Kim, S.Y.; Jeong, S.H.; Kim, J.B. The decline in dental caries among Korean children aged 8 and 12 years from 2000 to 2012 focusing SiC Index and DMFT. BMC Oral Health 2016, 16, 38. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ministry of Health and Welfare. 2015 Korean Children’s Oral Health Survey; Ministry of Health and Welfare: Osong, Korea, 2015; pp. 145–146. ISBN 11-1352000-001513-12.
- Moon, H.S.; Paik, D.I.; Horowitz, A.M.; Kim, J. National survey of Korean dentists’ knowledge and opinions: Dental caries etiology and prevention. J. Public Health Dent. 1998, 58, 51–66. [Google Scholar] [CrossRef]
- Tahani, B.; Yadegarfar, G.; Ahmadi, A. Knowledge, attitude, and practice of parents of 7–12-year-old children regarding fissure sealant therapy and professional fluoride therapy. J. Educ. Health Promot. 2017, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Neenan, E.M.; Easley, M.W.; Ruiz, M. Water fluoridation. In Harris NO, Garcia-Godoy F. Primary Preventive Dentistry, 6th ed.; Pearson Education Inc.: New York, NY, USA, 2004; pp. 45–72. [Google Scholar]
- Pizzo, G.; Piscopo, M.R.; Pizzo, I.; Giuliana, G. Community water fluoridation and caries prevention: A critical review. Clin. Oral Investig. 2007, 11, 189–193. [Google Scholar] [CrossRef] [PubMed]
- WHO Strategies and Approaches in Oral Disease Prevention and Health Promotion. Available online: https://www.who.int/oral_health/strategies/cont/en/ (accessed on 7 February 2019).
- Ministry of Health and Welfare. Guideline for Oral Health Program in 2004: Status of Water Fluoridation Program; Ministry of Health and Welfare: Seoul, Korea, 2003; pp. 70–72.
- Korea Health Promotion Institute. Status of Water Fluoridation Program in 2016; Korea Health Promotion Institute: Seoul, Korea, 2016. [Google Scholar]
- Ha, T.G.; Gong, W.S.; Kim, S.Y.; Kim, J.S.; Lee, S.H.; Kim, H.N.; Kim, J.B. Caries preventive effect from community water fluoridation program. J. Kor. Dent. Assoc. 2018, 56, 194–207. [Google Scholar]
- Ast, D.; Fitzgerald, B. Effectiveness of water fluoridation. J. Am. Dent. Assoc. 1962, 65, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Harding, M.A.; O’Mullane, D.M. Water fluoridation and oral health. Acta. Med. Acad. 2013, 42, 131–139. [Google Scholar]
- Kim, J.B.; Paik, D.I.; Moon, H.S.; Song, Y.H.; Park, D.Y. A study of the effect of water fluoridation in the Chungju City. Kor. Acd. Oral Health 1992, 16, 505–521. [Google Scholar]
- Anaise, J.Z. Measurement of dental caries experience-modification of the DMFT index. Commun. Dent. Oral Epidemiol. 1984, 12, 43–46. [Google Scholar] [CrossRef]
- Kim, S.C.; Lee, S.M.; Kim, J.Y.; Kim, J.B. Caries preventive effects of a fissure sealant program in Habchon-gun, Korea. J. Kor. Acad. Oral Health 2003, 27, 417–486. [Google Scholar]
- Ahn, S.H.; You, H.Y.; Kim, M.J.; Han, D.H.; Kim, J.B.; Jeong, S.H. Caries preventive effect of permanent teeth using pit and fissure sealant program and community water fluoridation program. J. Kor. Acad. Oral Health 2012, 36, 289–296. [Google Scholar] [CrossRef][Green Version]
- Ministry of Health and Welfare. National Oral Health Survey in 2012; Ministry of Health and Welfare: Seoul, Korea, 2012; pp. 299–300. ISBN 11-1352000-00951-12.
- Meyer, J.; Margaritis, V.; Mendelsohn, A. Consequences of community water fluoridation cessation for Medicaid eligible children and adolescents. BMC Oral Health 2018, 18, 215. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare. 2000 National Oral Health Survey; Ministry of Health and Welfare: Seoul, Korea, 2001; ISBN 11-1460000-000874-12.
- World Health Organization. Oral Health Surveys–Basic Methods; WHO publication: Geneva, Switzerland, 1997. [Google Scholar]
- Korea Statistics. Available online: http://kosis.kr/index/index.do (accessed on 8 January 2019).
- Lukacs, J.R. Sex differences in dental caries experience: Clinical evidence, complex etiology. Clin. Oral Investig. 2011, 15, 649–656. [Google Scholar] [CrossRef]
- Choi, J.S.; Ma, D.S.; Jung, S.H.; Cho, E.; ParK, D.Y. Changes in the amount of pit and fissure sealants supplied in Korea after inclusion in the National Health Insurance coverage. J. Kor. Acad. Oral Health 2015, 39, 69–77. [Google Scholar] [CrossRef]
- Jeong, J.I.; Kim, J.E.; Kim, S.Y.; Lee, J.H.; Kim, J.B.; Jeong, S.H. Caries-preventing effects of a suburban community water fluoridation program on permanent dentition after adjusting for the number of fissure-sealed teeth. J. Kor. Acad. Oral Health 2016, 40, 61–68. [Google Scholar] [CrossRef]
- Groeneveld, A.; Van Eck, A.A. Fluoride in caries prevention: Is the effect pre-or post-eruptive? J. Dent. Res. 1990, 69, 751–755. [Google Scholar] [CrossRef]
- Newbrun, E. Systemic benefits of fluoride and fluoridation. J. Public Health Dent. 2004, 64, 35–39. [Google Scholar] [CrossRef]
- Singh, K.A.; Spencer, A.J. Relative effects of pre- and post-eruption water fluoride on caries experience by surface type of permanent first molars. Commun. Dent. Oral Epidemiol. 2004, 32, 435–446. [Google Scholar] [CrossRef]
- Kim, J.B. A study on the children’s dental caries of permanent teeth in rural area. J. Kor. Acad. Dent. Health 1991, 15, 197–208. [Google Scholar]
- Saliba, N.A.; Moimaz, S.A.S.; Casotti, C.A.; Pagliari, A.V. Dental caries of lifetime residents in baixo guandu, brazil, fluoridated since 1953—A brief communication. J. Public Health Dent. 2008, 68, 119–121. [Google Scholar] [CrossRef]
- Mahoney, G.; Slade, G.D.; Kitchener, S.; Barnett, A. Lifetime fluoridation exposure and dental caries experience in a military population. Commun. Dent. Oral Epidemiol. 2008, 36, 485–492. [Google Scholar] [CrossRef]
- Do, L.; Ha, D.; Peres, M.; Skinner, J.; Byun, R.; Spencer, A.J. Effectiveness of water fluoridation in the prevention of dental caries across adult age groups. Commun. Dent. Oral Epidemiol. 2017, 45, 225–232. [Google Scholar] [CrossRef]
- Crocombe, L.; Brennan, D.; Slade, G.; Stewart, J.; Spencer, A. The effect of lifetime fluoridation exposure on dental caries experience of younger rural adults. Aust. Dent. J. 2015, 60, 30–37. [Google Scholar] [CrossRef]
- Kim, H.N.; Cho, H.H.; Kim, M.J.; Jun, E.J.; Han, D.H.; Jeong, S.H. Caries prevention effect of water fluoridation in gimhae, Korea. J. Dent. Hyg. Sci. 2014, 14, 448–454. [Google Scholar] [CrossRef][Green Version]
- Son, S.G.; Choi, Y.H.; Hong, S.J.; Kim, J.B. Dental caries prevalence in relation to socioeconomic factors and dental health behaviors among Korean adults. J. Kor. Acad. Dent. Health 2003, 27, 319–328. [Google Scholar]
- Kim, N.H.; Hwang, S.J.; Choi, J.A.; Mun, S.J.; Chung, W.G. Quartile present teeth related socioeconomic status and oral health behaviors among Korean elderly. J. Kor. Acad. Oral Health 2009, 33, 254–266. [Google Scholar]
- Kim, Y.H.; Lee, J.H. Relationship between unmet dental needs and the general and oral health status of adults. J. Kor. Acad. Oral Health 2018, 42, 16–23. [Google Scholar] [CrossRef]
- Schwendicke, F.; Dörfer, C.E.; Schlattmann, P.; Page, L.F.; Thomson, W.M.; Paris, S. Socioeconomic inequality and caries. J. Dent. Res. 2015, 94, 10–18. [Google Scholar] [CrossRef]
- Crocombe, L.; Brennan, D.; Slade, G. Does lower lifetime fluoridation exposure explain why people outside capital cities have poor clinical oral health? Aust. Dent. J. 2016, 61, 93–101. [Google Scholar] [CrossRef]
- McGrady, M.G.; Ellwood, R.P.; Maguire, A.; Goodwin, M.; Boothman, N.; Pretty, I.A. The association between social deprivation and the prevalence and severity of dental caries and fluorosis in populations with and without water fluoridation. BMC Public Health 2012, 12, 1122. [Google Scholar] [CrossRef]
- Slade, G.D.; Sanders, A.E.; Do, L.; Roberts-Thomson, K.; Spencer, A.J. Effects of fluoridated drinking water on dental caries in australian adults. J. Dent. Res. 2013, 92, 376–382. [Google Scholar] [CrossRef]
- Evans, R.W.; Beck, D.J.; Brown, R.H.; Silva, P.A. Relationship between fluoridation and socioeconomic status on dental caries experience in 5-year-old New Zealand children. Commun. Dent. Oral Epidemiol. 1984, 12, 5–9. [Google Scholar] [CrossRef]
- Burt, B.A. Fluoridation and social equity. J. Public Health Dent. 2002, 62, 195–200. [Google Scholar] [CrossRef]
- Cho, H.J.; Jin, B.H.; Park, D.Y.; Jung, S.H.; Lee, H.S.; Paik, D.I.; Bae, K.H. Systemic effect of water fluoridation on dental caries prevalence. Commun. Dent. Oral Epidemiol. 2014, 42, 341–348. [Google Scholar] [CrossRef]
- Kim, H.N.; Kim, J.H.; Kim, S.Y.; Kim, J.B. Associations of community water fluoridation with caries prevalence and oral health inequality in children. Int. J. Environ. Res. Public Health 2017, 14, 631. [Google Scholar] [CrossRef]
- Kim, M.K.; Jung, J.I.; Kim, M.J.; Jun, E.J.; Kim, H.N.; Kim, S.Y.; Han, D.H.; Jeong, S.H.; Kim, J.B. Cost-benefit analysis of a water fluoridation program for 11 years in Jinju, Korea. J. Kor. Acad. Oral Health 2014, 38, 118–128. [Google Scholar] [CrossRef]
- Cho, H.J.; Lee, H.S.; Paik, D.I.; Bae, K.H. Association of dental caries with socioeconomic status in relation to different water fluoridation levels. Commun. Dent. Oral Epidemiol. 2014, 42, 536–542. [Google Scholar] [CrossRef]
- Hwang, S.S.; You, M.S.; Lee, W.J.; Lee, K.S.; Son, H.J.; Jung, S.H.; Chun, J.H. Study on Safety Evaluation of Fluoride Concentration in Tap Water; Inha University: Incheon, Korea, 2014; pp. 9–11. [Google Scholar]



{kind=link}
{kind=link}
| Before CWFP | Control (National Data in 2000) * | Hapcheon in 2000 ** | p-Value ‡ | ||||
| Total (Gender) | Boy | Girl | Total (Gender) | Boy | Girl | ||
| Total (Age) | 3602 | 1797 | 1805 | 671 | 363 | 308 | 0.048 |
| 8 | 1194 | 592 | 602 | 213 | 127 | 86 | 0.007 |
| 10 | 1205 | 600 | 605 | 198 | 98 | 100 | 0.939 |
| 12 | 1203 | 604 | 599 | 260 | 138 | 122 | 0.412 |
| After 15 Years of CWFP | Control (National Oral Health Data in 2013–2015) † | Hapcheon in 2015 | p-Value ‡ | ||||
| Total (Gender) | Boy | Girl | Total (Gender) | Boy | Girl | ||
| Total (Age) | 952 | 519 | 433 | 498 | 174 | 162 | 0.698 |
| 8 | 243 | 122 | 121 | 103 | 53 | 50 | 0.906 |
| 10 | 239 | 133 | 106 | 116 | 58 | 58 | 0.364 |
| 12 | 239 | 130 | 109 | 117 | 63 | 54 | 1.000 |
| 15 | 231 | 134 | 97 | 162 | 92 | 70 | 0.836 |
| Before CWFP | Control (National Data in 2000) * | Hapcheon in 2000 ** | p-Value‡ | ||||
| N | Mean | SE ‡ | N | Mean | SE ‡ | ||
| Total (Age) | 3602 | 0.47 | 0.02 | 671 | 2.24 | 0.10 | <0.001 |
| 8 | 1194 | 0.49 | 0.03 | 213 | 1.90 | 0.08 | <0.001 |
| 10 | 1205 | 0.48 | 0.04 | 198 | 5.06 | 0.19 | <0.001 |
| 12 | 1203 | 0.44 | 0.04 | 260 | 0.36 | 0.07 | 0.397 |
| After 15 Years of CWFP | Control (National Data in 2013–2015) † | Hapcheon in 2015 | p-Value‡ | ||||
| N | Mean | SE ‡ | N | Mean | SE ‡ | ||
| Total (Age) | 952 | 1.67 | 0.07 | 498 | 1.48 | 0.08 | 0.077 |
| 8 | 243 | 1.62 | 0.11 | 103 | 1.61 | 0.15 | 0.959 |
| 10 | 239 | 1.76 | 0.11 | 116 | 1.26 | 0.13 | 0.005 |
| 12 | 239 | 1.85 | 0.16 | 117 | 1.14 | 0.14 | 0.001 |
| 15 | 231 | 1.42 | 0.18 | 162 | 1.80 | 0.17 | 0.149 |
| Before CWFP in 2000 | Control in 2000 * | Hapcheon in 2000 ** | p-Value | |||||
| N | Mean | SE ‡ | N | Mean | SE ‡ | |||
| Total (Age) | 3602 | 1.82 ‡ | 0.04 | 671 | 1.98 ‡ | 0.09 | - | 0.094 ‡ |
| 8 | 1194 | 1.00 § | 0.04 | 213 | 0.92 § | 0.10 | - | 0.456 § |
| 10 | 1205 | 1.59 § | 0.06 | 198 | 1.75 § | 0.18 | - | 0.402 § |
| 12 | 1203 | 2.86 § | 0.08 | 260 | 3.04 § | 0.17 | - | 0.346 § |
| After CWFP for 15 years | Control (National Data in 2013–2015) † | Hapcheon in 2015 | Caries Reducing Effects | p-Value | ||||
| N | Mean | SE ‡ | N | Mean | SE ‡ | % | ||
| Total (Age) | 952 | 1.42 ‡ | 0.06 | 498 | 1.00 ‡ | 0.09 | 29.6 | <0.001 ‡ |
| 8 | 243 | 0.44 § | 0.06 | 103 | 0.50 § | 0.10 | - | 0.615 § |
| 10 | 239 | 0.88 § | 0.08 | 116 | 0.50 § | 0.12 | 43.2 | 0.009 § |
| 12 | 239 | 1.38 § | 0.12 | 117 | 0.87 § | 0.17 | 37.0 | 0.017 § |
| 15 | 231 | 2.82 § | 0.20 | 162 | 2.10 § | 0.24 | 25.5 | 0.019 § |
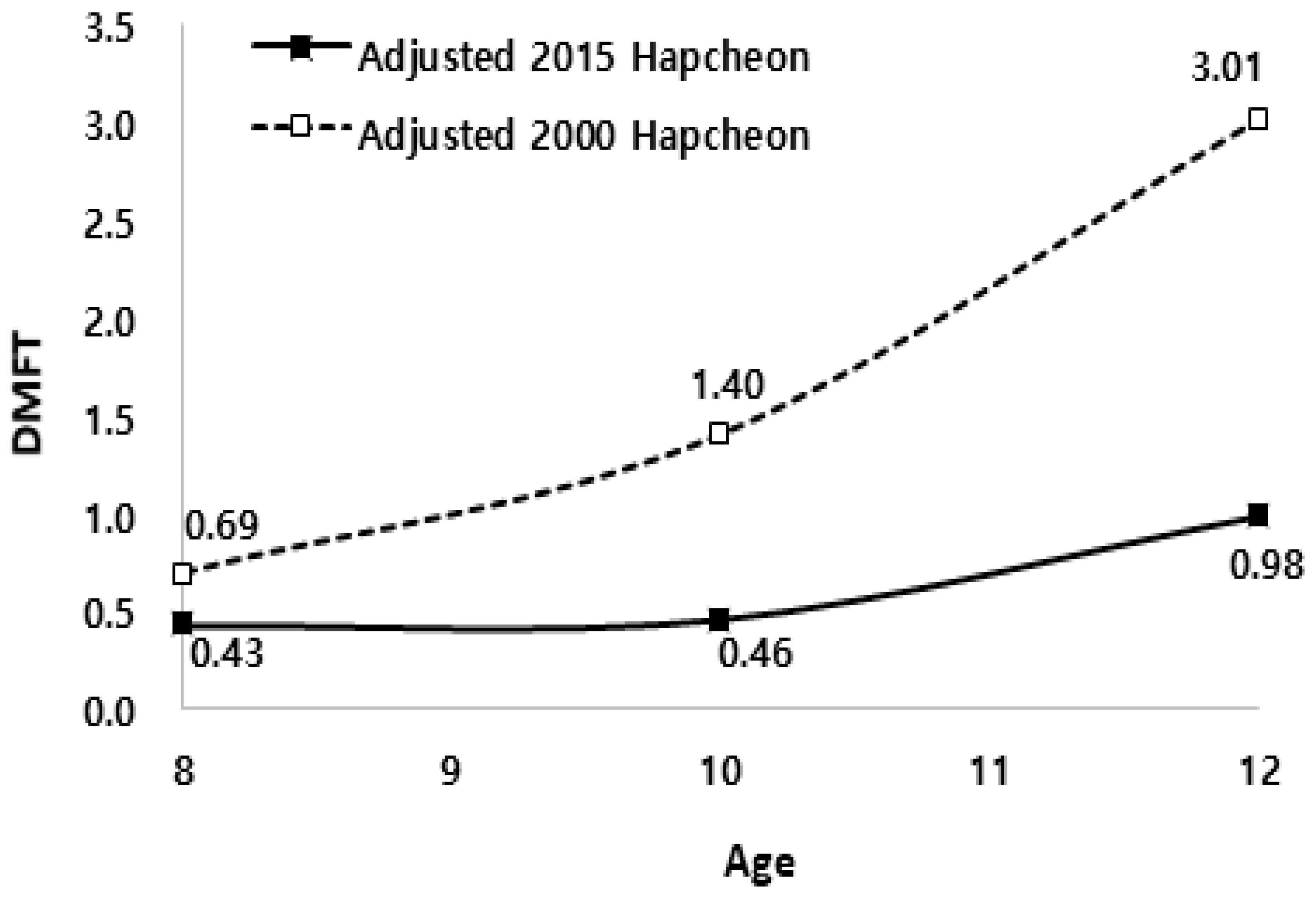
| Age | Hapcheon in 2000 * | Hapcheon in 2015 | Caries Reducing Effects (%) | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| N | Mean | SE † | N | Mean | SE † | |||
| Total | 671 | 1.81 ‡ | 0.07 | 336 | 0.60 ‡ | 0.10 | 66.9 | <0.001 ‡ |
| 8 | 213 | 0.69 § | 0.08 | 103 | 0.43 § | 0.11 | 37.7 | 0.001 § |
| 10 | 198 | 1.40 § | 0.11 | 116 | 0.46 § | 0.16 | 67.1 | 0.008 § |
| 12 | 260 | 3.01 § | 0.15 | 117 | 0.98 § | 0.22 | 67.4 | <0.001 § |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.-N.; Kong, W.-S.; Lee, J.-H.; Kim, J.-B. Reduction of Dental Caries Among Children and Adolescents From a 15-Year Community Water Fluoridation Program in a Township Area, Korea. Int. J. Environ. Res. Public Health 2019, 16, 1306. https://doi.org/10.3390/ijerph16071306
Kim H-N, Kong W-S, Lee J-H, Kim J-B. Reduction of Dental Caries Among Children and Adolescents From a 15-Year Community Water Fluoridation Program in a Township Area, Korea. International Journal of Environmental Research and Public Health. 2019; 16(7):1306. https://doi.org/10.3390/ijerph16071306
Chicago/Turabian StyleKim, Han-Na, Wook-Sung Kong, Jung-Ha Lee, and Jin-Bom Kim. 2019. "Reduction of Dental Caries Among Children and Adolescents From a 15-Year Community Water Fluoridation Program in a Township Area, Korea" International Journal of Environmental Research and Public Health 16, no. 7: 1306. https://doi.org/10.3390/ijerph16071306
APA StyleKim, H.-N., Kong, W.-S., Lee, J.-H., & Kim, J.-B. (2019). Reduction of Dental Caries Among Children and Adolescents From a 15-Year Community Water Fluoridation Program in a Township Area, Korea. International Journal of Environmental Research and Public Health, 16(7), 1306. https://doi.org/10.3390/ijerph16071306