Maximum Temperature and Solar Radiation as Predictors of Bipolar Patient Admission in an Emergency Psychiatric Ward


 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Assessment
2.3. Statistical Analyses
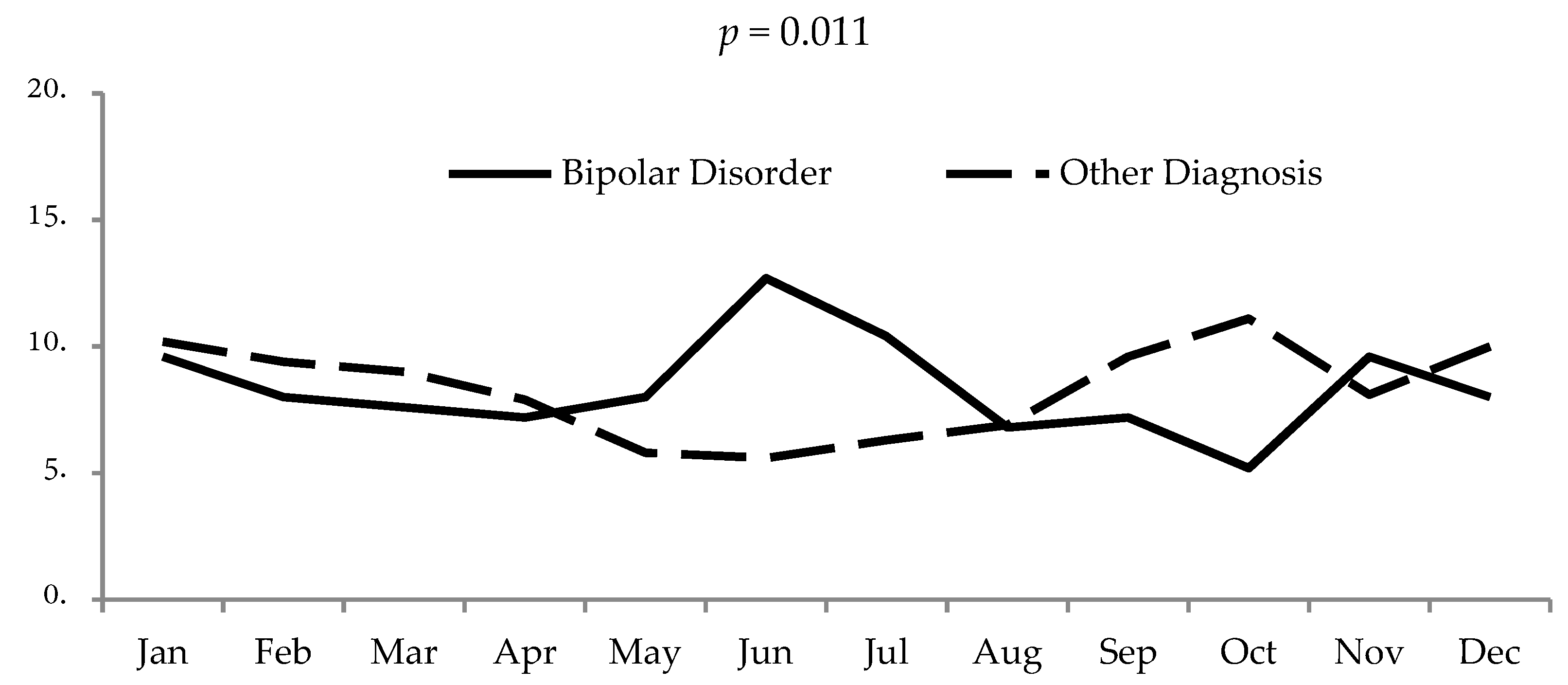
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kronfeld-Schor, N.; Visser, M.E.; Salis, L.; van Gils, J.A. Chronobiology of interspecific interactions in a changing world. Philos. Trans. R. Soc. Lond. B. Biol. Sci. 2017, 372. [Google Scholar] [CrossRef] [PubMed]
- Kalachanis, K.; Michailidis, I.E. The Hippocratic View on Humors and Human Temperament. Eur. J. Soc. Behav. 2015, 2, 1–5. [Google Scholar]
- Lombroso, C. Azione degli astri e delle meteore sulla mente umana. Memoria premiata dal R. Istituto Lombardo. In Osservazioni Meteorologico-Psichiatriche; Bologna, Italy, 1869. [Google Scholar]
- Kristensen, M.; Nierenberg, A.A.; Østergaard, S.D. Face and predictive validity of the ClockΔ19 mouse as an animal model for bipolar disorder: A systematic review. Mol. Psychiatry. 2018, 23, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Moreira, J.; Geoffroy, P.A. Lithium and bipolar disorder: Impacts from molecular to behavioural circadian rhythms. Chronobiol. Int. 2016, 33, 351–373. [Google Scholar] [CrossRef]
- Muneer, A. The Neurobiology of Bipolar Disorder: An Integrated Approach. Chonamm. Med. J. 2016, 52, 18–37. [Google Scholar] [CrossRef] [PubMed]
- Pagani, L.; St Clair, P.A.; Teshiba, T.M.; Service, S.K.; Fears, S.C.; Araya, C.; Araya, X.; Bejarano, J.; Ramirez, M.; Castrillón, G.; et al. Genetic contributions to circadian activity rhythm and sleep pattern phenotypes in pedigrees segregating for severe bipolar disorder. Proc. Natl. Acad. Sci. USA 2016, 113, E754–E761. [Google Scholar] [CrossRef]
- Melo, M.C.; Abreu, R.L.; Linhares Neto, V.B.; de Bruin, P.F.; de Bruin, V.M. Chronotype and circadian rhythm, in bipolar disorder: A systematic review. Sleep. Med. Rev. 2017, 34, 46–58. [Google Scholar] [CrossRef]
- Pawlak, J.; Szczepankiewicz, A.; Kapelski, P.; Rajewska-Rager, A.; Slopien, A.; Skibinska, M.; Czerski, P.; Hauser, J.; Dmitrzak-Weglarz, M. Suicidal behavior in the context of disrupted rhythmicity in bipolar disorder-Complementary research of clock genes with suicide risks factors and course of disease. Psychiatry. Res. 2017, 257, 446–449. [Google Scholar] [CrossRef] [PubMed]
- Borniger, J.C.; Maurya, S.K.; Periasamy, M.; Nelson, R.J. Acute dim light at night increases body mass, alters metabolism, and shifts core body temperature circadian rhythms. Chronobiol. Int. 2014, 31, 917–925. [Google Scholar] [CrossRef] [PubMed]
- Alloy, L.B.; Ng, T.H.; Titone, M.K.; Boland, E.M. Circadian Rhythm Dysregulation in Bipolar Spectrum Disorders. Curr. Psychiatry. Rep. 2017, 19, 21. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Glenn, T.; Alda, M.; Andreassen, O.A.; Angelopoulos, E.; Ardau, R.; Baethge, C.; Bauer, R.; Bellivier, F.; Belmaker, R.H.; et al. Relationship between sunlight and the age of onset of bipolar disorder: An international multisite study. J. Affect. Disord. 2014, 167, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Glenn, T.; Alda, M.; Andreassen, O.A.; Angelopoulos, E.; Ardau, R.; Baethge, C.; Bauer, R.; Baune, B.T.; Bellivieri, F.; et al. Influence of light exposure during early life on the age of onset of bipolar disorder. J. Psychiatr. Res. 2015, 64, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Aguglia, A.; Borsotti, A.; Cuniberti, F.; Serafini, G.; Amore, M.; Maina, G. The influence of sunlight exposure on hospitalization in emergency psychiatry. Chronobiol. Int. 2017, 34, 1413–1422. [Google Scholar] [CrossRef]
- Bauer, M.; Glenn, T.; Alda, M.; Aleksandrovich, M.A.; Andreassen, O.A.; Angelopoulos, E.; Ardau, R.; Ayhan, Y.; Baethge, C.; Bharathram, S.R.; et al. Solar insolation in springtime influence age at onset of bipolar I disorder. Acta. Psychiatr. Scand. 2017, 136, 571–582. [Google Scholar] [CrossRef] [PubMed]
- Aguglia, A.; Borsotti, A.; Maina, G. Bipolar disorders: Is there an influence of seasonality or photoperiod? Rev. Bras. Psiquiatr. 2018, 40, 6–11. [Google Scholar] [CrossRef]
- Lee, H.C.; Tsai, S.Y.; Lin, H.C. Seasonal variations in bipolar disorder admissions and the association with climate: A population-based study. J. Affect. Disord. 2007, 97, 61–69. [Google Scholar] [CrossRef]
- Christensen, E.M.; Larsen, J.K.; Gjerris, A.; Peacock, L.; Jacobi, M.; Hassenbalch, E. Climatic factors and bipolar affective disorder. Nord. J. Psychiatry. 2008, 62, 55–58. [Google Scholar] [CrossRef]
- Volpe, F.M.; Tavares, A.; Del Porto, J.A. Seasonality of three dimensions of mania: Psychosis, aggression and suicidality. J. Affect. Disord. 2008, 108, 95–100. [Google Scholar] [CrossRef]
- Volpe, F.M.; da Silva, E.M.; dos Santos, T.N.; de Freitas, D.E. Further evidence of seasonality of mania in the tropics. J. Affect. Disord. 2010, 124, 178–182. [Google Scholar] [CrossRef]
- Geoffroy, P.A.; Bellivier, F.; Scott, J.; Etain, B. Seasonality and bipolar disorder: A systematic review, from admission rates to seasonality of symptoms. J. Affect. Disord. 2014, 168, 210–223. [Google Scholar] [CrossRef]
- Medici, C.R.; Vestergaard, C.H.; Hadzi-Pavlovic, D.; Munk-Jørgensen, P.; Parker, G. Seasonal variations in hospital admissions for mania: Examining for associations with weather variables over time. J. Affect. Disord. 2016, 205, 81–86. [Google Scholar] [CrossRef]
- Bullock, B.; Murray, G.; Meyer, D. Highs and lows, ups and downs: Meteorology and mood in bipolar disorder. PLoS ONE. 2017, 12, e0173431. [Google Scholar] [CrossRef]
- Parker, G.B.; Hadzi-Pavlovic, D.; Graham, R.K. Examining for any impact of climate change on the association between seasonality and hospitalization for mania. J. Affect. Disord. 2017, 208, 431–435. [Google Scholar] [CrossRef]
- Parker, G.; Hadzi-Pavlovic, D.; Bayes, A.; Graham, R. Relationship between photoperiod and hospital admissions for mania in New South Wales, Australia. J. Affect. Disord. 2018, 226, 72–76. [Google Scholar] [CrossRef]
- Chan, E.Y.Y.; Lam, H.C.Y.; So, S.H.W.; Goggins, W.B.; Ho, J.Y.; Liu, S.; Chung, P.P.W. Association between Ambient Temperatures and Mental Disorder Hospitalizations in a Subtropical City: A Time-Series Study of Hong Kong Special Administrative Region. Int. J. Environ. Res. Public Health. 2018, 15, E754. [Google Scholar] [CrossRef]
- Lee, S.; Lee, H.; Myung, W.; Kim, E.J.; Kim, H. Mental disease-related emergency admissions attributable to hot temperatures. Sci. Total Environ. 2018, 616–617, 688–694. [Google Scholar] [CrossRef]
- Sherbakov, T.; Malig, B.; Guirguis, K.; Gershunov, A.; Basu, R. Ambient temperature and added heat wave effects on hospitalizations in California from 1999 to 2009. Environ. Res. 2018, 160, 83–90. [Google Scholar] [CrossRef]
- Zhang, S.; Mellsop, G.; Brink, J.; Wang, X. Involuntary admission and treatment of patients with mental disorder. Neurosci. Bull. 2015, 31, 99–112. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Stazione Meteorologica di Fisica dell’Atmosfera. Available online: http://www.meteo.dfg.unito.it/ (accessed on 29 March 2019).
- Bauer, M.; Glenn, T.; Alda, M.; Andreassen, O.A.; Ardau, R.; Bellivier, F.; Berk, M.; Bjella, T.D.; Bossini, L.; Zompo, M.D.; et al. Impact of sunlight on the age of onset of bipolar disorder. Bipolar. Disord. 2012, 14, 654–663. [Google Scholar] [CrossRef]
- Akther, A.; Fiedorowicz, J.G.; Zhang, T.; Potash, J.B.; Cavanaugh, J.; Solomon, D.A.; Coryell, W.H. Seasonal variation of manic and depressive symptoms in bipolar disorder. Bipolar. Disord. 2013, 15, 377–384. [Google Scholar] [CrossRef]
- Young, J.W.; Dulcis, D. Investigating the mechanism(s) underlying switching between states in bipolar disorder. Eur. J. Pharmacol. 2015, 759, 151–162. [Google Scholar] [CrossRef]
- Milhiet, V.; Etain, B.; Boudebesse, C.; Bellivier, F. Circadian biomarkers, circadian genes and bipolar disorders. J. Physiol. Paris. 2011, 105, 183–189. [Google Scholar] [CrossRef]
- McCarthy, M.J.; Welsh, D.K. Cellular Circadian Clocks in Mood Disorders. J. Biol. Rhythms. 2012, 27, 339–352. [Google Scholar] [CrossRef] [PubMed]
- Belvederi Murri, M.; Prestia, D.; Mondelli, V.; Pariante, C.; Patti, S.; Olivieri, B.; Arzani, C.; Masotti, M.; Respino, M.; Antonioli, M.; et al. The HPA axis in bipolar disorder: Systematic review and meta-analysis. Psychoneuroendocrinology 2016, 63, 327–342. [Google Scholar] [CrossRef] [PubMed]
- Kohno, K.; Hoaki, N.; Inoue, T.; Nakai, Y.; Toyomaki, A.; Araki, Y.; Hatano, K.; Terao, T. Latitude effect on bipolar temperaments. J. Affect. Disord. 2012, 142, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.C.; Yang, C.H.; Hong, C.J.; Liou, Y.J.; Shia, B.C.; Peng, C.K.; Huang, N.E.; Tsai, S.J. Effects of age, sex, index admission, and predominant polarity on the seasonality of acute admissions for bipolar disorder: A population-based study. Chronobiol. Int. 2013, 30, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Dominiak, M.; Swiecicki, L.; Rybakowski, J. Psychiatric hospitalizations for affective disorders in Warsaw, Poland: Effect of season and intensity of sunlight. Psychiatry. Res. 2015, 229, 287–294. [Google Scholar] [CrossRef]
- Lee, H.J.; Kim, L.; Joe, S.H.; Suh, K.Y. Effects of season and climate on the first manic episode of bipolar affective disorder in Korea. Psychiatry. Res. 2002, 113, 151–159. [Google Scholar] [CrossRef]
- Bauer, M.; Glenn, T.; Grof, P.; Rasgon, N.L.; Marsh, W.; Sagduyu, K.; Alda, M.; Murray, G.; Quiroz, D.; Malliaris, Y.; Sasse, J.; Pilhatsch, M.; Whybrow, P.C. Relationship among latitude, climate, season and self-reported mood in bipolar disorder. J. Affect. Disord. 2009, 116, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Inoue, T.; Kohno, K.; Baba, H.; Takeshima, M.; Honma, H.; Nakai, Y.; Suzuki, T.; Hatano, K.; Arai, H.; Matsubara, S.; Kusumi, I.; Terao, T. Does temperature or sunshine mediate the effect of latitude on affective temperaments? A study of 5 regions in Japan. J. Affect. Disord. 2015, 172, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, H.; Terao, T.; Inoue, T.; Takaesu, Y.; Ishii, N.; Kohno, K.; Takeshima, M.; Baba, H.; Honma, H. Re-analysis of the association of temperature or sunshine with hyperthymic temperament using lithium levels of drinking water. J. Affect. Disord. 2017, 223, 126–129. [Google Scholar] [CrossRef]
- Brandl, E.J.; Lett, T.A.; Bakanidze, G.; Heinz, A.; Bermpohl, F.; Schouler-Ocak, M. Weather conditions influence the number of psychiatric emergency room patients. Int. J. Biometeorol. 2018, 62, 843–850. [Google Scholar] [CrossRef]
- Sung, T.I.; Chen, M.J.; Su, H.J. A positive relationship between ambient temperature and bipolar disorder identified using a national cohort of psychiatric inpatients. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 295–302. [Google Scholar] [CrossRef]
- Volpe, F.M.; Del Porto, J.A. Seasonality of admissions for mania in a psychiatric hospital of Belo Horizonte, Brazil. J. Affect. Disord. 2006, 94, 61–69. [Google Scholar] [CrossRef]
- Shapira, A.; Shiloh, R.; Potchter, O.; Hermesh, H.; Popper, M.; Weizman, A. Admission rates of bipolar depressed patients increase during spring/summer and correlate with maximal environmental temperature. Bipolar. Disord. 2004, 6, 90–93. [Google Scholar] [CrossRef]
- Wang, H.; Wang, B.; Normoyle, K.P.; Jackson, K.; Spitler, K.; Sharrock, M.F.; Miller, C.M.; Best, C.; Llano, D.; Du, R. Brain temperature and its fundamental properties: A review for clinical neuroscientists. Front. Neurosci. 2014, 8, 307. [Google Scholar] [CrossRef]
- Bellivier, F.; Geoffroy, P.A.; Etain, B.; Scott, J. Sleep- and circadian rhythm-associated pathways as therapeutic targets in bipolar disorder. Expert. Opin. Ther. Targets 2015, 19, 747–763. [Google Scholar] [CrossRef]
- Geoffroy, P.A.; Samalin, L.; Llorca, P.M.; Curis, E.; Bellivier, F. Influence of lithium on sleep and chronotypes in remitted patients with bipolar disorder. J. Affect. Disord. 2016, 204, 32–39. [Google Scholar] [CrossRef]
- Yoshikawa, T.; Honma, S. Lithium lengthens circadian period of cultured brain slices in area specific manner. Behav. Brain. Res. 2016, 314, 30–37. [Google Scholar] [CrossRef]
- Geoffroy, P.A.; Curis, E.; Courtin, C.; Moreira, J.; Morvillers, T.; Etain, B.; Laplanche, J.L.; Bellivier, F.; Marie-Claire, C. Lithium response in bipolar disorders and core clock genes expression. World. J. Biol. Psychiatry 2018, 19, 619–632. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics of the 730 Patients Included | Total Sample |
|---|---|
| Gender (female), n (%) | 311 (42.6) |
| Age (years), mean ± SD | 43.4 ± 13.9 |
| Education level, n (%) | |
| Elementary | 67 (9.2) |
| Low school | 352 (48.2) |
| High school | 257 (35.2) |
| Graduation | 54 (7.4) |
| Marital status, n (%) | |
| Single | 406 (55.6) |
| Married | 190 (26.0) |
| Divorced | 106 (14.5) |
| Widowed | 28 (3.9) |
| Working status, n (%) | 245 (33.6) |
| Age at onset (years), mean ± SD | 28.5 ± 13.3 |
| Suicide, n (%) | |
| Ideation | 122 (16.7) |
| Attempt | 77 (10.5) |
| Admission, n (%) | |
| Involuntary | 112 (15.3) |
| Voluntary | 618 (84.7) |
| Length of stay, mean ± SD | 11.4 ± 8.9 |
| Diagnosis, n (%) | |
| Bipolar and related disorders | 251 (34.4) |
| Schizophrenia and related disorders | 192 (26.3) |
| Depressive disorders | 134 (18.3) |
| Others | 153 (21.0) |
| Meteorological Variables | Bipolar Disorder’ Admission (n = 251) | Other Diagnoses’ Admission (n = 479) | p |
|---|---|---|---|
| Temperature minimum (Celsius), mean ± SD | 10.9 ± 7.4 | 9.5 ± 7.0 | 0.010 |
| Temperature maximum (Celsius), mean ± SD | 20.2 ± 9.0 | 17.7 ± 8.0 | <0.001 |
| Temperature medium (Celsius), mean ± SD | 15.2 ± 8.1 | 13.3 ± 7.5 | 0.002 |
| Humidity minimum (%), mean ± SD | 50.7 ± 16.2 | 51.2 ± 17.3 | 0.719 |
| Humidity maximum (%), mean ± SD | 86.5 ± 7.6 | 85.1 ± 8.8 | 0.027 |
| Humidity medium (%), mean ± SD | 69.3 ± 12.9 | 70.5 ± 12.5 | 0.238 |
| Wind maximum (km/h), mean ± SD | 14.7 ± 5.9 | 14.6 ± 5.6 | 0.866 |
| Wind medium (km/h), mean ± SD | 4.4 ± 1.6 | 4.2 ± 1.5 | 0.136 |
| Atmospheric Pressure minimum (hPa), mean ± SD | 1012.6 ± 8.0 | 1013.5 ± 8.1 | 0.136 |
| Atmospheric Pressure maximum (hPa), mean ± SD | 1018.2 ± 7.2 | 1019.1 ± 7.7 | 0.125 |
| Atmospheric Pressure medium (hPa), mean ± SD | 1015.4 ± 7.2 | 1016.3 ± 7.9 | 0.172 |
| Rain (mm), mean ± SD | 2.6 ± 6.3 | 2.9 ± 7.7 | 0.574 |
| *Solar Radiation (W/m2), mean ± SD | 6.9 ± 3.3 | 5.8 ± 3.2 | <0.001 |
| Humidex Index (Celsius), mean ± SD | 21.7 ± 10.1 | 19.3 ± 8.9 | 0.001 |
| Windchill Index (Celsius), mean ± SD | 9.4 ± 8.3 | 7.9 ± 7.8 | 0.017 |
| Hours of sunshine, mean ± SD | 12.1 ± 2.5 | 11.6 ± 2.3 | 0.030 |
| Variables | p | OR | 95% CI |
|---|---|---|---|
| Gender | 0.085 | 0.746 | 0.534–1.042 |
| Age | 0.004 | 1.018 | 1.006–1.030 |
| Temperature maximum | 0.030 | 1.162 | 1.011–1.231 |
| * Solar radiation | 0.025 | 1.146 | 1.017–1.292 |
| Hour of sunshine | 0.131 | 0.843 | 0.675–1.052 |
| Atmospheric Pressure maximum | 0.103 | 0.980 | 0.957–1.004 |
| Windchill index | 0.974 | 0.999 | 0.943–1.058 |
| Humidex index | 0.300 | 0.950 | 0.863–1.046 |
| Humidity maximum | 0.180 | 0.985 | 0.964–1.007 |
| Lenght of stay | <0.001 | 1.066 | 1.044–1.088 |
| Spring | 0.354 | 1.462 | 0.655–3.263 |
| Summer | 0.065 | 2.251 | 0.950–5.332 |
| Autumn | 0.528 | 1.185 | 0.699–2.011 |
| Winter | 0.149 | 0.962 | 0.901–1.112 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aguglia, A.; Serafini, G.; Escelsior, A.; Canepa, G.; Amore, M.; Maina, G. Maximum Temperature and Solar Radiation as Predictors of Bipolar Patient Admission in an Emergency Psychiatric Ward. Int. J. Environ. Res. Public Health 2019, 16, 1140. https://doi.org/10.3390/ijerph16071140
Aguglia A, Serafini G, Escelsior A, Canepa G, Amore M, Maina G. Maximum Temperature and Solar Radiation as Predictors of Bipolar Patient Admission in an Emergency Psychiatric Ward. International Journal of Environmental Research and Public Health. 2019; 16(7):1140. https://doi.org/10.3390/ijerph16071140
Chicago/Turabian StyleAguglia, Andrea, Gianluca Serafini, Andrea Escelsior, Giovanna Canepa, Mario Amore, and Giuseppe Maina. 2019. "Maximum Temperature and Solar Radiation as Predictors of Bipolar Patient Admission in an Emergency Psychiatric Ward" International Journal of Environmental Research and Public Health 16, no. 7: 1140. https://doi.org/10.3390/ijerph16071140
APA StyleAguglia, A., Serafini, G., Escelsior, A., Canepa, G., Amore, M., & Maina, G. (2019). Maximum Temperature and Solar Radiation as Predictors of Bipolar Patient Admission in an Emergency Psychiatric Ward. International Journal of Environmental Research and Public Health, 16(7), 1140. https://doi.org/10.3390/ijerph16071140