Health Disparities in Czechia and Portugal at Country and Municipality Levels





Abstract
1. Introduction
2. Data and Method
2.1. Areas of Interest
2.2. Variables: Health Outcomes and Determinants
3. Results
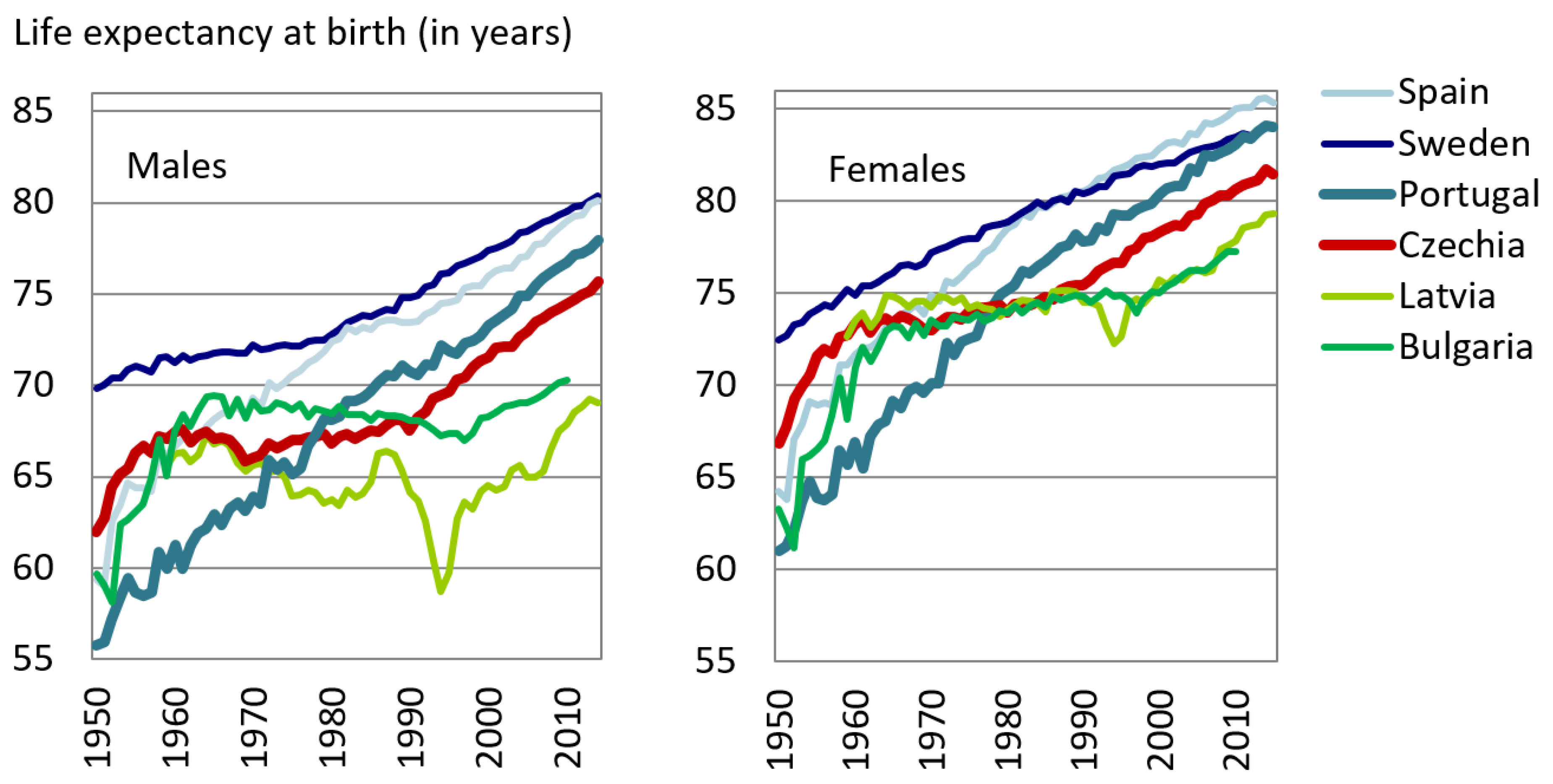
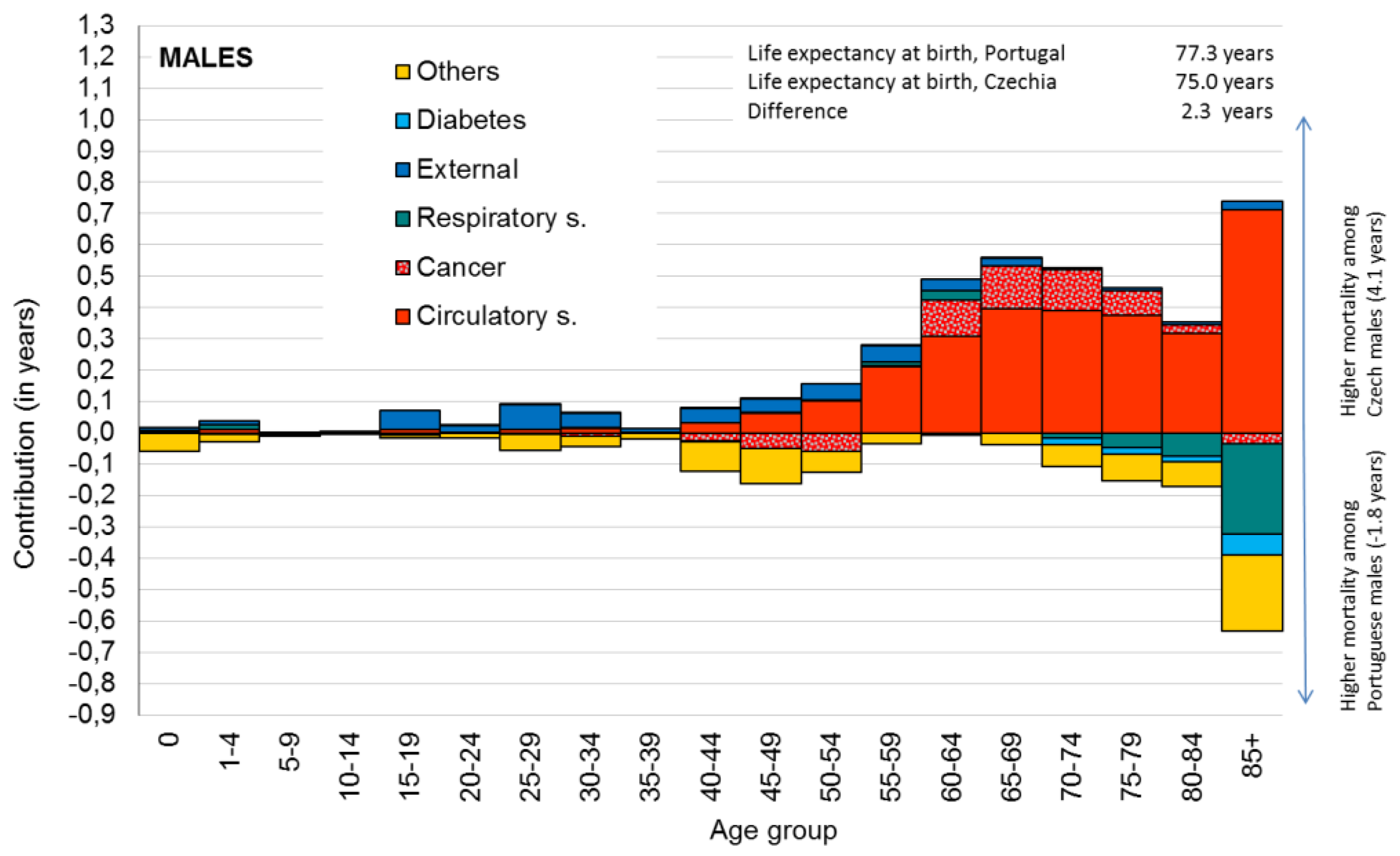
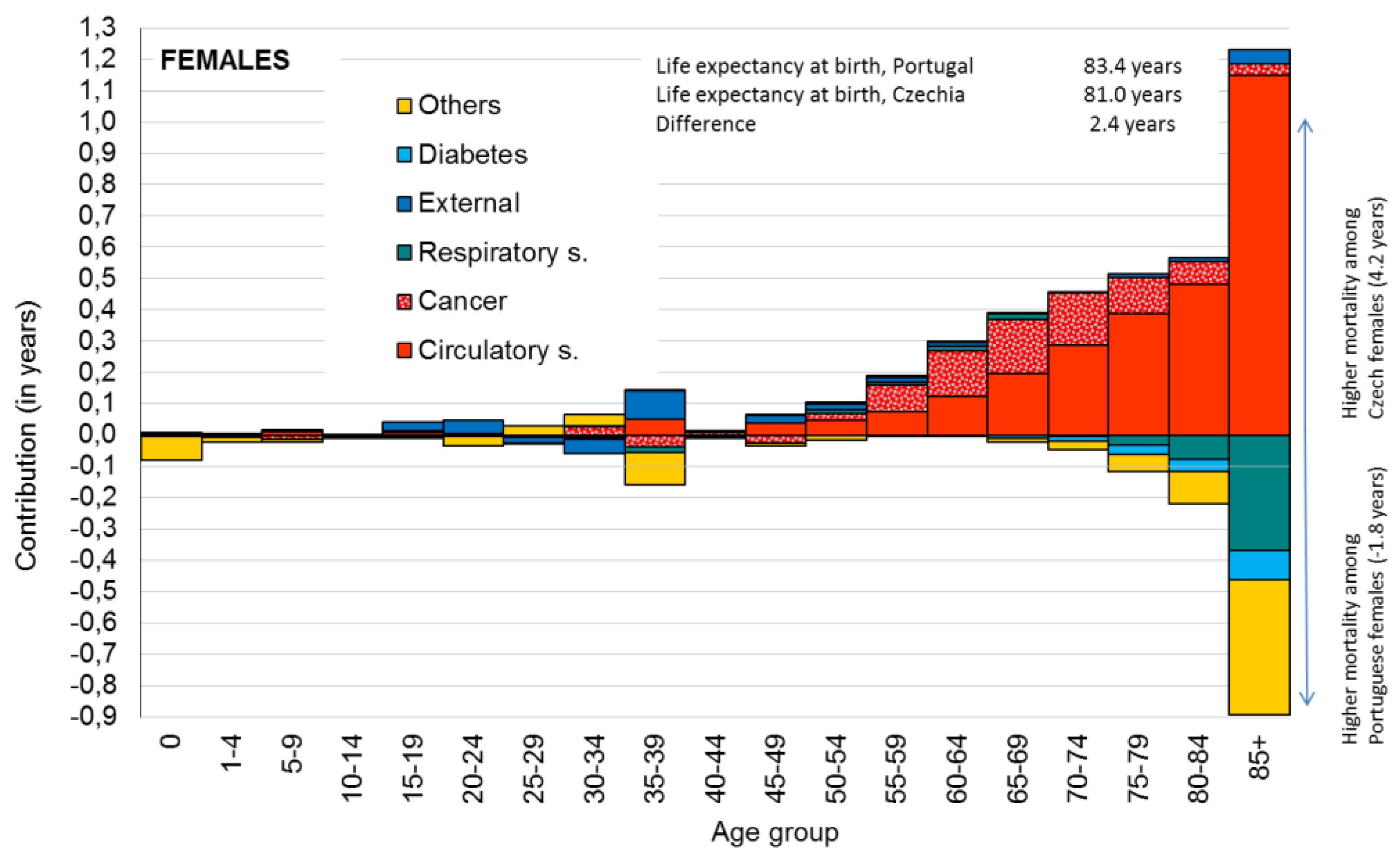
3.1. Country Level: Epidemiological Profile of Czech and Portuguese Population in 2012
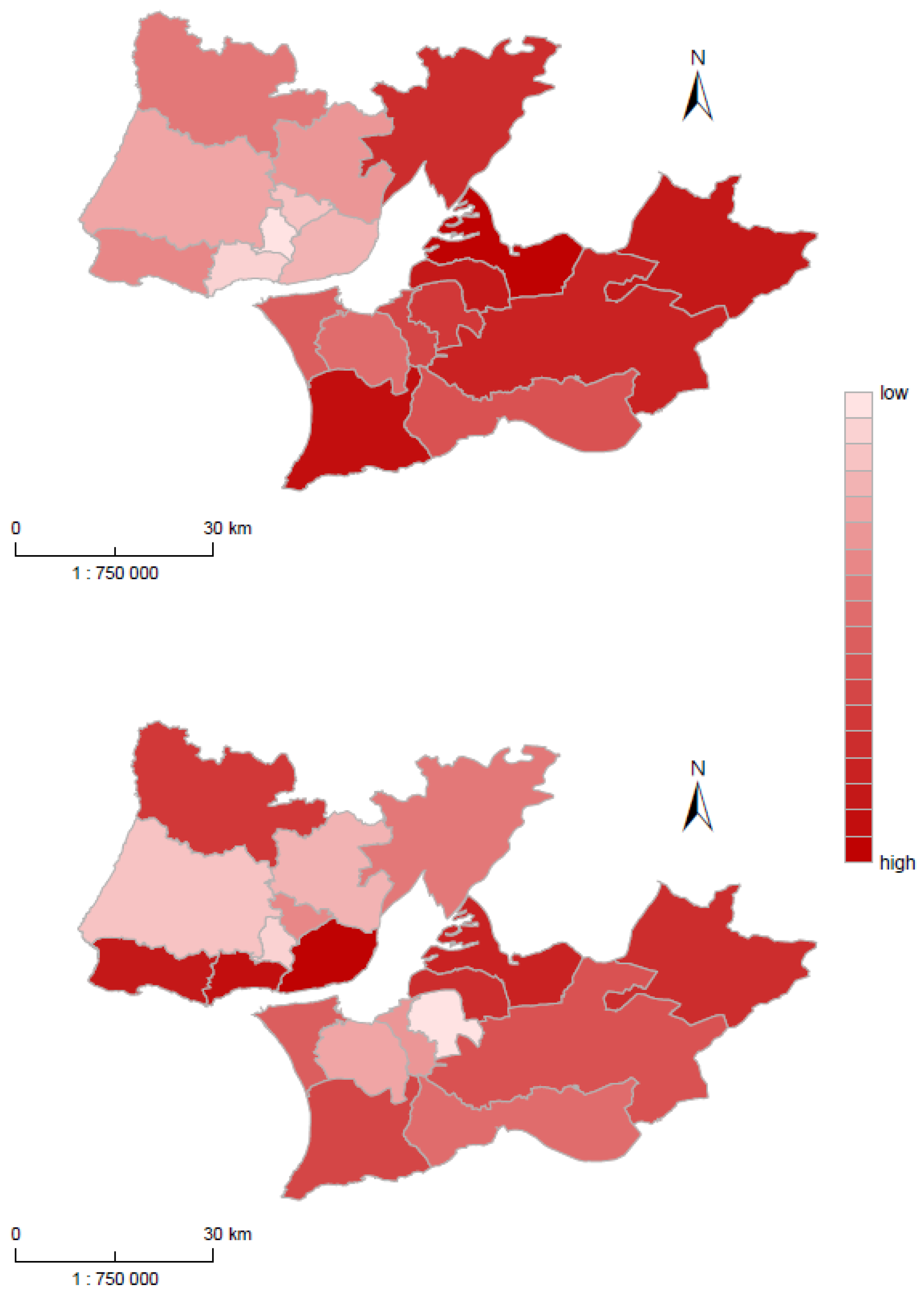
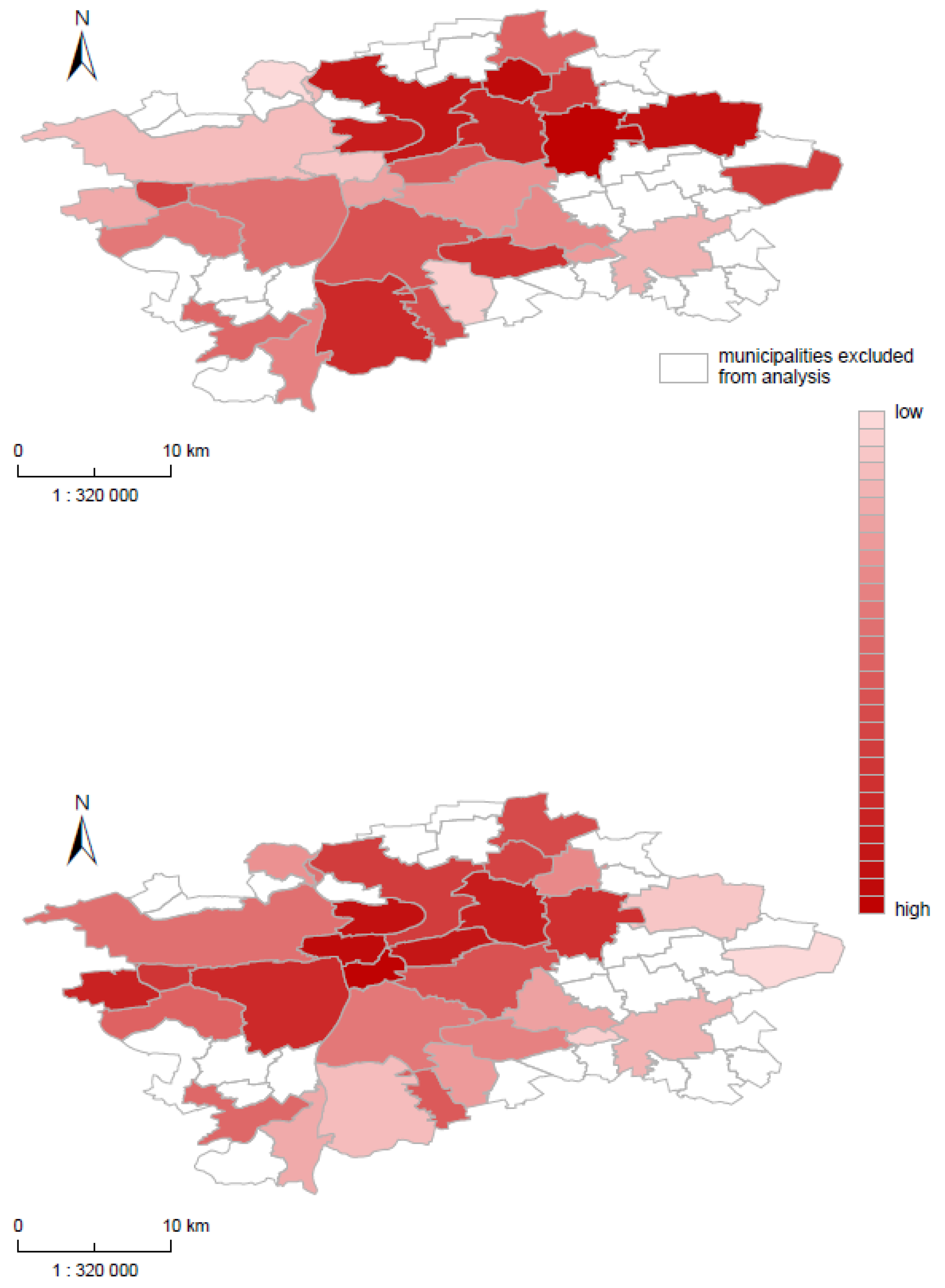
3.2. Municipality Level: Prague and Lisbon
4. Discussion
4.1. Principal Findings and Strengths of the Study
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Frenk, J.; Bobadilla, J.L.; Stern, C.; Frejka, T.; Lozano, R. Elements for a theory of the health transition. Health Transit. Rev. Cult. Soc. Behav. Determ. Health 1991, 1, 21–38. [Google Scholar]
- Vallin, J.; Meslé, F. Convergences and divergences in mortality. A new approach to health transition. Demogr. Res. 2004. [Google Scholar] [CrossRef]
- Meslé, F.; Vallin, J. Mortality in Europe: The Divergence between East and West. Population 2002, 57, 157. [Google Scholar] [CrossRef]
- Bobak, M.; Marmot, M. Coronary Heart Disease in Central and Eastern Europe and the Former Soviet Union; Marmot, M., Elliott, P., Eds.; Oxford University Press: Oxford, UK, 2005. [Google Scholar] [CrossRef]
- Bobak, M.; Marmot, M. East-west mortality divide and its potential explanations: Proposed research agenda. BMJ 1996, 312. [Google Scholar] [CrossRef]
- Velkova, A.; Wolleswinkel-van den Bosch, J.H.; Mackenbach, J.P. The East-West life expectancy gap: Differences in mortality from conditions amenable to medical intervention. Int. J. Epidemiol. 1997, 26, 75–84. [Google Scholar] [CrossRef]
- Fihel, A.; Pechholdová, M. Between ‘Pioneers’ of the Cardiovascular Revolution and Its ‘Late Followers’: Mortality Changes in the Czech Republic and Poland Since 1968. Eur. J. Popul. 2017, 33, 651–678. [Google Scholar] [CrossRef] [PubMed]
- Bosakova, L.; Rosicova, K.; Filakovska Bobakova, D.; Rosic, M.; Dzurova, D.; Pikhart, H.; Lustigova, M.; Santana, P. Mortality in the Visegrad countries from the perspective of socioeconomic inequalities. Int. J. Public Health 2018. [Google Scholar] [CrossRef]
- Townsend, N.; Wilson, L.; Bhatnagar, P.; Wickramasinghe, K.; Rayner, M.; Nichols, M. Cardiovascular disease in Europe: Epidemiological update 2016. Eur. Heart J. 2016, 37, 3232–3245. [Google Scholar] [CrossRef]
- Santana, P.; Almendra, R. The health of the Portuguese over the last four decades. Méditerranée [Online], 130|2018, Online since 07 February 2019. 2018. Available online: http://journals.openedition.org/mediterranee/10348 (accessed on 28 March 2019). [CrossRef]
- Dragano, N.; Bobak, M.; Wege, N.; Peasey, A.; Verde, P.E.; Kubinova, R.; Weyers, S.; Moebus, S.; Möhlenkamp, S.; Stang, A.; et al. Neighbourhood socioeconomic status and cardiovascular risk factors: A multilevel analysis of nine cities in the Czech Republic and Germany. Bmc Public Health 2007, 7, 255. [Google Scholar] [CrossRef] [PubMed]
- Arnold, J.M.; Farinha Rodrigues, C. Reducing Inequality and Poverty in Portugal. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2873041 (accessed on 21 August 2015).
- Layte, R.; McCrory, C.; Cheallaigh, C.N.; Bourke, N.; Kivimaki, M.; Ribeiro, A.I.; Stringhini, S.; Vineis, P. A Comparative Analysis of the Status Anxiety Hypothesis of Socio-economic Inequalities in Health Based on 18,349 individuals in Four Countries and Five Cohort Studies. Sci. Rep. 2019, 9, 796. [Google Scholar] [CrossRef] [PubMed]
- Santana, P. Poverty, social exclusion and health in Portugal. Soc. Sci. Med. 2002, 55, 33–45. [Google Scholar] [CrossRef]
- Santana, P.; Krafft, T.; Pilot, E.; Stefanik, I.; Costa, C.B.e.; Borrell, C. Atlas of Population Health in European Union Regions; Imprensa da Universidade de Coimbra: Coimbra, Portugal, 2017. [Google Scholar]
- Costa, C.; Santana, P.; Dimitroulopoulou, S.; Burstrom, B.; Borrell, C.; Schweikart, J.; Dzurova, D.; Zangarini, N.; Katsouyanni, K.; Deboseree, P.; et al. Population Health Inequalities Across and Within European Metrpolitan Areas through the Lens of the EURO-HEALTHY Population Health Index. Int. J. Environ. Res. Public Health 2019, 16, 836. [Google Scholar] [CrossRef] [PubMed]
- Arcaya, M.C.; Arcaya, A.L.; Subramanian, S.V. Inequalities in health: Definitions, concepts, and theories. Glob. Health Action 2015, 8, 27106. [Google Scholar] [CrossRef] [PubMed]
- Osborn, D.; Cutter, A.; Ullah, F. Universal Sustainable Development Goals Understanding the Transformational Challenge for Developed Countries Report of a Study by Stakeholder Forum May 2015. Available online: https://sustainabledevelopment.un.org/content/documents/1684SF_-_SDG_Universality_Report_-_May_2015.pdf (accessed on 5 February 2019).
- Mackenbach, J.P.; Stirbu, I.; Roskam, A.-J.R.; Schaap, M.M.; Menvielle, G.; Leinsalu, M.; Kunst, A.E. Socioeconomic Inequalities in Health in 22 European Countries. New Engl. J. Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef] [PubMed]
- Santana, P.; Costa, C.; Cardoso, G.; Loureiro, A.; Ferrão, J. Suicide in Portugal: Spatial determinants in a context of economic crisis. Health Place 2015, 35, 85–94. [Google Scholar] [CrossRef]
- Hoffmann, R.; Borsboom, G.; Saez, M.; Dell’Olmo, M.; Burström, B.; Corman, D.; Costa, C.; Deboosere, P.; Domínguez-Berjón, M.F.; Dzúrová, D.; et al. Social differences in avoidable mortality between small areas of 15 European cities: An ecological study. Int. J. Health Geogr. 2014, 13, 8. [Google Scholar] [CrossRef]
- Marí-Dell’Olmo, M.; Gotsens, M.; Palència, L.; Burström, B.; Corman, D.; Costa, G.; Deboosere, P.; Díez, È.; Domínguez-Berjón, F.; Dzúrová, D.; et al. Socioeconomic inequalities in cause-specific mortality in 15 European cities. J. Epidemiol. Community Health 2015, 69, 432–441. [Google Scholar] [CrossRef]
- Borrell, C.; Marí-Dell’olmo, M.; Palència, L.; Gotsens, M.; Burström, B.; Domínguez-Berjón, F.; Rodríguez-Sanz, M.; Dzúrová, D.; Gandarillas, A.; Hoffmann, R.; et al. Socioeconomic inequalities in mortality in 16 European cities. Scand. J. Public Health 2014, 42, 245–254. [Google Scholar] [CrossRef]
- Borrel, C.; Palència, L.; Gotsens, M.; Marí Dell’Olmo, M.; Rodríguez-Sanz, M.; Bosáková, L.; Rosičová, K.; Hajduová, Z.; Seidlova, M.; Lustigova, M.; et al. The evolution of socioeconomic inequalities in mortality in nine metropolitan areas. In Promoting Population Health and Equity in Europe: From Evidence to Policy; Imprensa da Universidade de Coimbra: Coimbra, Portugal, 2017; 103p, ISBN 978-989-20-8021-5. [Google Scholar]
- Samoli, E.; Stergiopoulou, A.; Santana, P.; Rodopoulou, S.; Mitsakou, C.; Dimitroulopoulou, C.; Bauwelinck, M.; de Hoogh, K.; Costa, C.; Marí-Dell’Olmo, M.; et al. Spatial variability in air pollution exposure in relation to socioeconomic indicators in nine European metropolitan areas: A study on environmental inequality. Environ. Pollut. 2019, 249, 345–353. [Google Scholar] [CrossRef]
- Mitsakou, C.; Dimitroulopoulou, S.; Heaviside, C.; Katsouyanni, K.; Samoli, E.; Rodopoulou, S.; Costa, C.; Almendra, R.; Santana, P.; Dell’Olmo, M.M.; et al. Environmental public health risks in European metropolitan areas within the EURO-HEALTHY project. Sci. Total Environ. 2019, 658, 1630–1639. [Google Scholar] [CrossRef]
- Human Mortality Database. University of California, Berkeley (USA), and Max Planck Institute for Demographic Research (Germany). 2019. Available online: www.mortality.org or www.humanmortality.de (accessed on 10 March 2019).
- WHO Mortality Database (2018). Available online: https://www.who.int/healthinfo/mortality_data/en/ (accessed on 11 March 2019).
- Pollard, J.H. On the Decomposition of Changes in Expectation of Life and Differentials in Life Expectancy. Demography 1988, 25, 265. [Google Scholar] [CrossRef] [PubMed]
- Pollard, J.H. Macquarie University. School of Economic and Financial Studies. In The Expectation of Life and Its Relationship to Mortality; Macquarie University, School of Economic and Financial Studies: North Ryde, Australia, 1982. Available online: https://catalogue.nla.gov.au/Record/303551 (accessed on 5 February 2019).
- Santana, P.; Costa, C.; Loureiro, A.; Raposo, J.; Boavida, J.M. Geografias da Diabetes Mellitus em Portugal: Como as Condições do Contexto Influenciam o Risco de Morrer. Acta Médica Port. 2014, 27, 309. [Google Scholar] [CrossRef]
- Almendra, R.; Santana, P.; Freire, E.; Vasconcelos, J. Seasonal mortality patterns and regional contrasts in Portugal. Bull. Geogr. Soc.-Econ. Ser. 2016, 32, 7–18. [Google Scholar] [CrossRef]
- Lustigova, M.; Dzurova, D.; Pikhart, H.; Kubinova, R.; Bobak, M. Cardiovascular health among the Czech population at the beginning of the 21st century: A 12-year follow-up study. J. Epidemiol. Community Health 2018, 72, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Santana, P.; Costa, C.; Marí-Dell’Olmo, M.; Gotsens, M.; Borrell, C. Mortality, material deprivation and urbanization: Exploring the social patterns of a metropolitan area. Int. J. Equity Health 2015, 14, 55. [Google Scholar] [CrossRef]
- Mahishale, V. Climate change and respiratory health: Time to act! J. Sci. Soc. 2014, 41, 149. [Google Scholar] [CrossRef]
- Mendes, A.; Pereira, C.; Mendes, D.; Aguiar, L.; Neves, P.; Silva, S.; Batterman, S.; Teixeira, J.P. Indoor Air Quality and Thermal Comfort—Results of a Pilot Study in Elderly Care Centers in Portugal. J. Toxicol. Environ. Healthpart A 2013, 76, 333–344. [Google Scholar] [CrossRef]
- Almendra, R.; Santana, P.; Vasconcelos, J. Evidence of social deprivation on the spatial patterns of excess winter mortality. Int. J. Public Health 2017, 62, 849–856. [Google Scholar] [CrossRef]
- Almendra, R.; Perelman, J.; Vasconcelos, J.; Santana, P. Excess winter mortality and morbidity before, during, and after the Great Recession: The Portuguese case. Int. J. Biometeorol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Thun, M.; Peto, R.; Boreham, J.; Lopez, A.D. Stages of the cigarette epidemic on entering its second century. Tob. Control 2012, 21, 96–101. [Google Scholar] [CrossRef]
- Eurostat database. Smoking of tobacco products by sex, age and educational attainment level. 2019. Available online: http://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=hlth_ehis_sk1e&lang=en (accessed on 13 March 2019).
- van Lenthe, F.J. Aggregate Deprivation and Effects on Health; Siegrist, J., Marmot, M., Eds.; Oxford University Press: Oxford, UK, 2006. [Google Scholar] [CrossRef]
- Macintyre, S.; Ellaway, A. Ecological approaches: Rediscovering the role of the physical and social environment. In Social Epidemiology; Berkman, L.F., Kawachi, I., Eds.; Oxford University Press: New York, NY, USA, 2000. [Google Scholar]
- Pickett, K.E.; Pearl, M. Multilevel analyses of neighbourhood socioeconomic context and health outcomes: A critical review. J. Epidemiol. Community Health 2001, 55. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Area of Concern | Dimension | Indicator * |
|---|---|---|
| Economic environment | Employment | Youth unemployment rate (%) |
| Long-term unemployment rate: 12 months or more (%) | ||
| Social environment | Education | Population aged 25–64 with lower secondary education attainment (%) |
| Population aged 25–64 with upper secondary or tertiary education attainment (%) | ||
| Built environment | Housing conditions | Number of rooms per person |
| Population density | Population density (inhabitants/km2) | |
| Demographic change | Migration | Population born in EU28 countries, excluding the reporting country (%) |
| Population born in non-EU28 countries (%) |
| Indicator/Variable | Prague (N = 29 Municipality Units) | Lisbon (N = 18 Municipality Units) | ||||||
|---|---|---|---|---|---|---|---|---|
| Minimum | Maximum | Mean | Std. Deviation | Minimum | Maximum | Mean | Std. Deviation | |
| Health Outcomes | ||||||||
| Deaths from diseases of the circulatory system * | 417.3 | 675.5 | 544.7 | 63.3 | 276.3 | 442.1 | 353.2 | 38.5 |
| Death from cancer * | 245.2 | 339.2 | 287.5 | 25.2 | 236.6 | 280.7 | 257.5 | 14.6 |
| Death from diseases of respiratory system * | 17.3 | 77.0 | 60.0 | 14.5 | 85.48 | 157.7 | 113.3 | 20.5 |
| Death from diabetes * | 4.1 | 27.4 | 13.5 | 5.1 | 29.57 | 78.14 | 47.9 | 12.9 |
| Health Determinants | ||||||||
| Youth unemployment rate (%) | 2.9 | 6.1 | 4.8 | 0.81 | 7.7 | 16.3 | 11.6 | 2.47 |
| Long term unemployment rate (%) | 0.2 | 1.1 | 0.6 | 0.22 | 2.3 | 5.0 | 3.5 | 0.76 |
| Population with lower secondary education (%) | 3.1 | 7.1 | 5.1 | 0.92 | 25.7 | 46.7 | 38.9 | 5.54 |
| Population with upper secondary or tertiary education (%) | 67.1 | 88.5 | 83.4 | 4.72 | 29.2 | 52.5 | 38.3 | 5.98 |
| Housing condition (Average number of rooms per person) | 1.1 | 1.5 | 1.3 | 0.08 | 1.7 | 2.0 | 1.8 | 0.08 |
| Population density (inhabitants/km2) | 564.7 | 11,747 | 3781.4 | 3078.49 | 135.5 | 7370.6 | 2038.8 | 2235.60 |
| Population born in EU28 countries (%) | 3.0 | 9.9 | 5.0 | 1.38 | 0.2 | 2.4 | 0.9 | 0.60 |
| Population born in non-EU28 countries (%) | 4.5 | 15.8 | 10.1 | 2.86 | 2.0 | 9.5 | 5.1 | 2.00 |
| Component | Indicators | Factor 1 High Mortality & Social and Housing Deprivation | Factor 2 Low Mortality & Economic, Social, and Housing Prosperity |
| Factor Loading | Factor Loading | ||
| Health Outcomes | Deaths from diseases of the circulatory system | 0.794 | −0.148 |
| Death from diseases of respiratory system | 0.760 | −0.162 | |
| Death from diabetes | 0.833 | ||
| Death from cancer | 0.428 | 0.389 | |
| Health Determinants | Youth unemployment rate | 0.239 | −0.320 |
| Long term unemployment rate | −0.151 | −0.447 | |
| Population with lower secondary education | 0.394 | −0.863 | |
| Population with upper secondary or tertiary education | −0.397 | 0.878 | |
| Population density | −0.842 | ||
| Housing condition | 0.851 | ||
| Population born in EU28 countries | 0.252 | 0.628 | |
| Population born in non-EU28 countries | −0.753 | −0.436 |
| Component | Indicators | Factor 1 High Circulatory Mortality & Economic and Social Deprivation | Factor 2 High Mortality & Social and Housing Deprivation |
| Factor Loading | Factor Loading | ||
| Health Outcomes | Deaths from diseases of the circulatory system | 0.632 | 0.430 |
| Death from diseases of respiratory system | 0.259 | ||
| Death from diabetes | −0.149 | 0.284 | |
| Death from cancer | 0.474 | ||
| Health Determinants | Youth unemployment rate | 0.861 | |
| Long term unemployment rate | 0.784 | ||
| Population with lower secondary education | 0.845 | −0.146 | |
| Population with upper secondary or tertiary education | −0.759 | ||
| Population density | 0.112 | 0.612 | |
| Housing condition | −0.238 | −0.795 | |
| Population born in EU28 countries | −0.484 | 0.505 | |
| Population born in non EU28 countries | −0.146 | 0.549 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lustigova, M.; Dzurova, D.; Costa, C.; Santana, P. Health Disparities in Czechia and Portugal at Country and Municipality Levels. Int. J. Environ. Res. Public Health 2019, 16, 1139. https://doi.org/10.3390/ijerph16071139
Lustigova M, Dzurova D, Costa C, Santana P. Health Disparities in Czechia and Portugal at Country and Municipality Levels. International Journal of Environmental Research and Public Health. 2019; 16(7):1139. https://doi.org/10.3390/ijerph16071139
Chicago/Turabian StyleLustigova, Michala, Dagmar Dzurova, Claudia Costa, and Paula Santana. 2019. "Health Disparities in Czechia and Portugal at Country and Municipality Levels" International Journal of Environmental Research and Public Health 16, no. 7: 1139. https://doi.org/10.3390/ijerph16071139
APA StyleLustigova, M., Dzurova, D., Costa, C., & Santana, P. (2019). Health Disparities in Czechia and Portugal at Country and Municipality Levels. International Journal of Environmental Research and Public Health, 16(7), 1139. https://doi.org/10.3390/ijerph16071139