Accelerometer-Measured Physical Activity in Children and Adolescents at Altitudes over 3500 Meters: A Cross-Sectional Study in Tibet


 ,
,
Abstract
1. Introduction
2. Materials and Methods
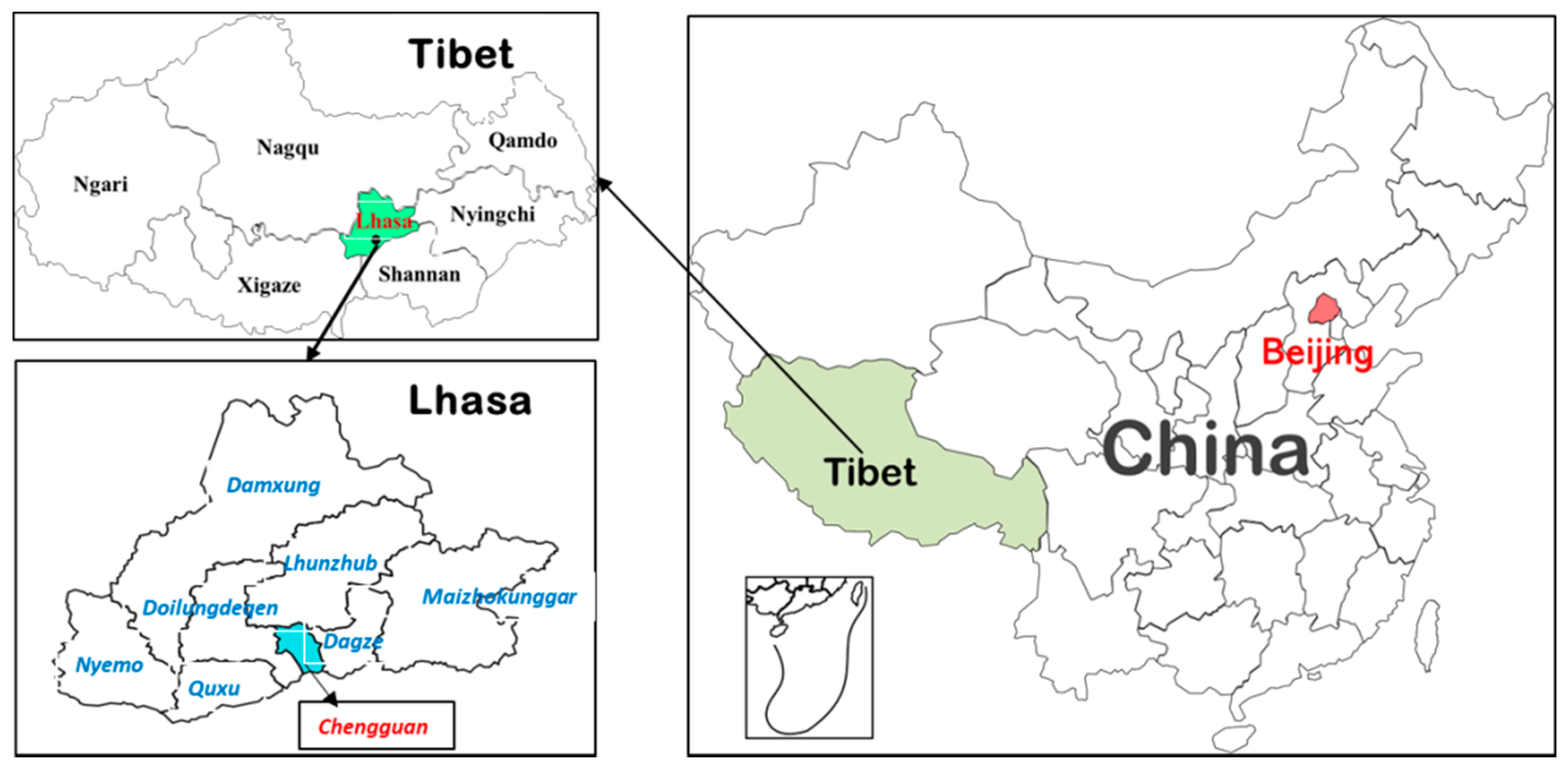
2.1. Design and Participants
2.2. Procedure
2.3. Measures
2.3.1. Demographic Characteristics
2.3.2. Height, Weight, and Body Mass Index (BMI)
2.3.3. Physical Activity
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
3.2. PA Levels
3.3. Meeting PA Guidelines
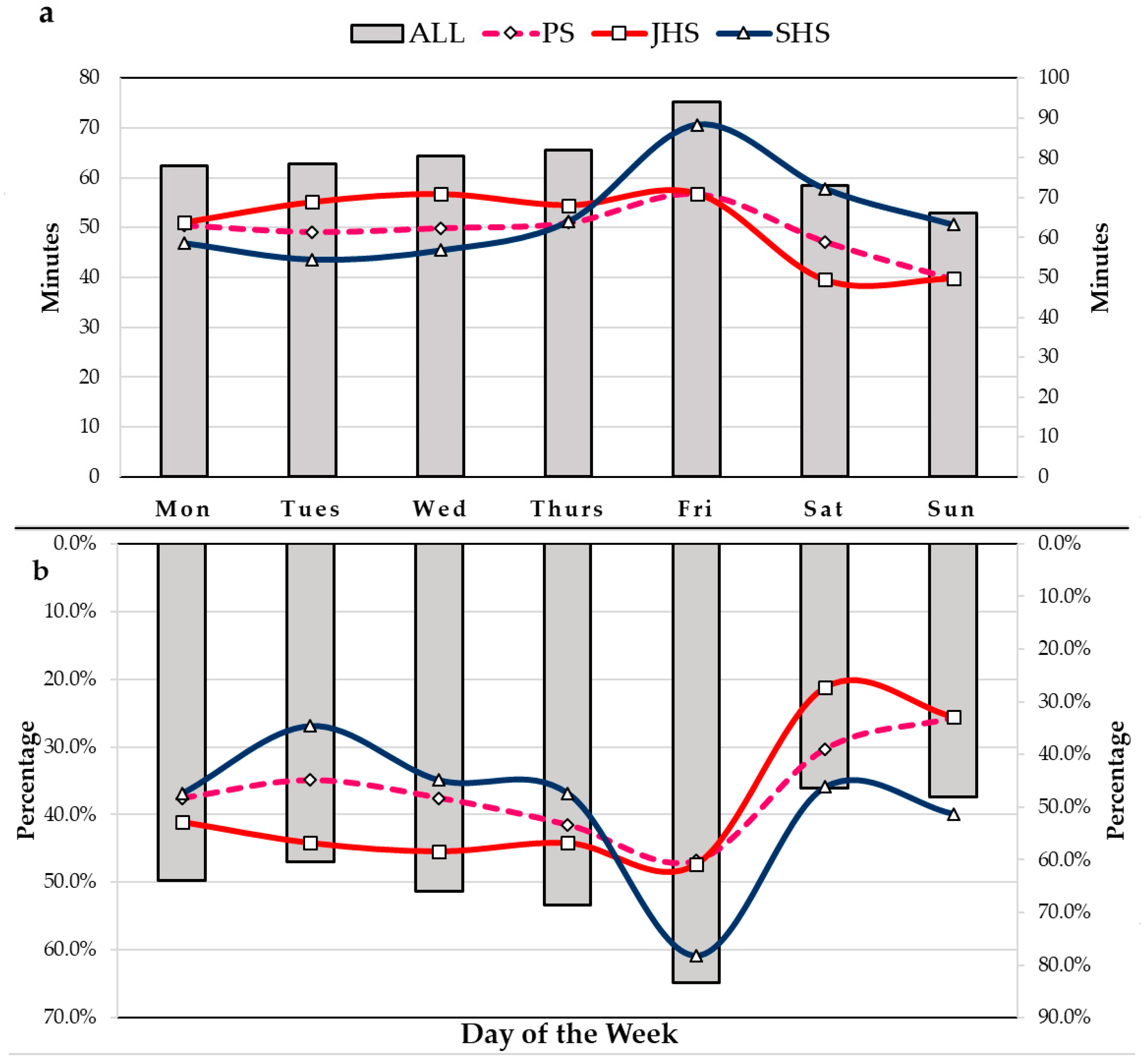
3.4. Daily Changes in PA Levels
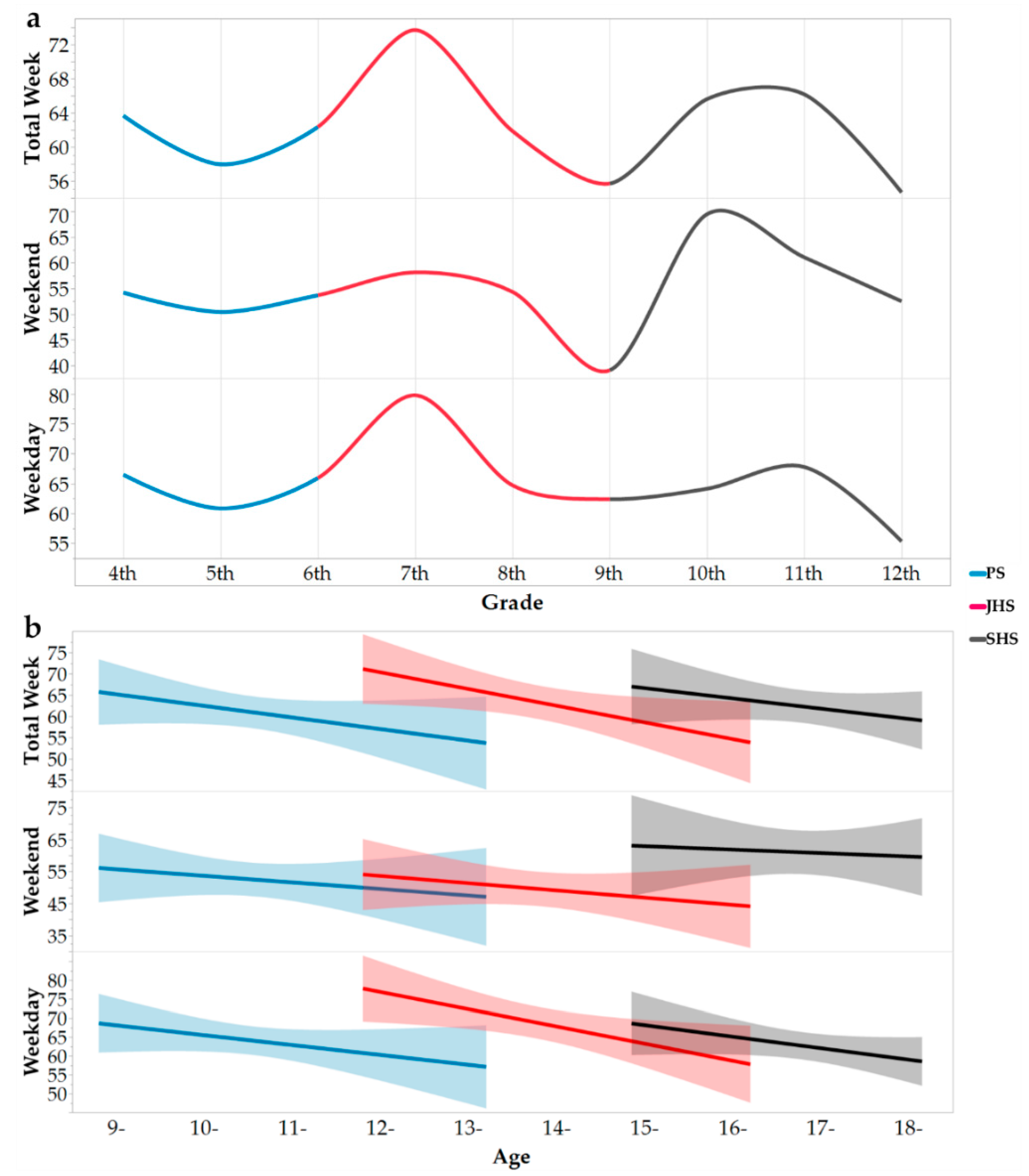
3.5. PA Differences in Ethnicity, Gender, Age/Grade, and Weight Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wareham, N.J.; van Sluijs, E.M.; Ekelund, U. Physical activity and obesity prevention: A review of the current evidence. Proc. Nutr. Soc. 2005, 64, 229. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.B.; Riddoch, C.; Kriemler, S.; Hills, A. Physical activity and cardiovascular risk factors in children. Br. J. Sports Med. 2011, 45, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.J.; Barnett, L.M.; Cliff, D.P.; Okely, A.D.; Scott, H.A.; Cohen, K.E.; Lubans, D.R. Fundamental movement skill interventions in youth: A systematic review and meta-analysis. Pediatrics 2013, 132, e1361. [Google Scholar] [CrossRef] [PubMed]
- Esteban-Cornejo, I.; Tejero-Gonzalez, C.M.; Sallis, J.F.; Veiga, O.L. Physical activity and cognition in adolescents: A systematic review. J. Sci. Med. Sport 2015, 18, 534–539. [Google Scholar] [CrossRef] [PubMed]
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Connor, G.S.; Kho, M.E. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Physiol. Appl. Nutr. Et Métab. 2016, 41, S197. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.E.; Hillman, C.H.; Castelli, D.; Etnier, J.L.; Lee, S.; Tomporowski, P.; Lambourne, K.; Szaboreed, A.N. Physical activity, fitness, cognitive function, and academic achievement in children: A systematic review. Med. Sci. Sports Exerc. 2016, 48, 1197–1222. [Google Scholar] [CrossRef] [PubMed]
- Ekeland, E.; Heian, F.; Hagen, K.B.; Abbott, J.; Nordheim, L. Exercise to improve self-esteem in children and young people. Cochrane Database Syst. Rev. 2004, CD003683. [Google Scholar] [CrossRef] [PubMed]
- Paffenbarger, R.S., Jr.; Hyde, R.T.; Wing, A.L.; Hsieh, C.C. Physical activity, all-cause mortality, and longevity of college alumni. N. Engl. J. Med. 1986, 314, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Booth, F.W.; Laye, M.J.; Lees, S.J.; Rector, R.S.; Thyfault, J.P. Reduced physical activity and risk of chronic disease: The biology behind the consequences. Eur. J. Appl. Physiol. 2008, 102, 381–390. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Who global status report on noncommunicable diseases 2010. Women 2011, 47, 2562–2563. [Google Scholar]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010; pp. 1–58. [Google Scholar]
- Janssen, I.; Leblanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I. Physical activity guidelines for children and youth. Can. J. Public Health 2007, 98 (Suppl. 2), S109–S121. [Google Scholar] [CrossRef]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Pei, H.L.; Mei, W. Investigation on chinese children and youth physical activity status and influence factors. Chin. J. Sch. Health 2016, 37, 805–809. (In Chinese) [Google Scholar] [CrossRef]
- Fan, X.; Cao, Z.B. Physical activity among chinese school-aged children:National prevalence estimates from the 2016 physical activity and fitness in china—The youth study. J. Sport Health Sci. 2017. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Chen, P.; Zhuang, J. A national survey of physical activity and sedentary behavior of chinese city children and youth using accelerometers. Res. Quart. Exerc. Sport 2013, 84 (Suppl. 2), S12. [Google Scholar] [CrossRef]
- Tian, Y.W. The challenge of low oxygen environment in plateau to human being. J. Med. Res. 2006, 35, 1–3. (In Chinese) [Google Scholar] [CrossRef]
- Qi, X.; Cui, C.; Ouzhuluobu; Wu, T.; Su, B. Prehistoric Colonization and Demographic History of Modern Humans on the Tibetan Plateau; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2014. [Google Scholar] [CrossRef]
- Yun, F.S. Analysis on the structural characteristics of Tibetan population. Theor. Platform Tibetan Dev. 2012, 26–31. (In Chinese) [Google Scholar] [CrossRef]
- National Bureau of Statistics of China. Available online: http://data.stats.gov.cn/adv.htm?m=advquery&cn=E0103 (accessed on 19 February 2019).
- Wang, G.Q.; Bai, Z.X.; Shi, J.; Luo, S.; Chang, H.F.; Sai, X.Y. Prevalence and risk factors for eye diseases, blindness, and low vision in lhasa, tibet. Int. J. Ophthalmol. 2013, 6, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, R.P.; Lee, T.K. Adverse effects of ultraviolet radiation: A brief review. Prog. Biophys. Mol. Biol. 2006, 92, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Qian, X.; Liu, B.; Wang, J.; Wei, N.; Qi, X.; Li, X.; Li, J.; Zhang, Y.; Hua, N.; Ning, Y. Prevalence of refractive errors in tibetan adolescents. Bmc Ophthalmol. 2018, 18, 118. [Google Scholar] [CrossRef] [PubMed]
- Xi, H.; Chen, Z.; Li, W.; Wen, Y.; Zhang, H.; Xiao, Y.; Liu, S.; Pei, L.; Zhang, M.; Lv, P. Chest circumference and sitting height among children and adolescents from lhasa, tibet compared to other high altitude populations. Am. J. Hum. Biol. 2016, 28, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.L.; Fu, Q.; Li, W.H.; Liu, S.W.; Zhong, H.; Duoji, B.M.; Zhang, M.Z.; Lv, P.; Xi, H.J. Gender differences and age-related changes in body fat mass in tibetan children and teenagers: An analysis by the bioelectrical impedance method. J. Pediatr. Endocrinol. Metab. Jpem 2015, 28, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Li, H.; Yang, L.; Wang, W.; Li, Y.; Gong, H.; Guo, M.; Nima, C.; Zhao, S.; Wang, J. Hair selenium levels of school children in kashin-beck disease endemic areas in tibet, china. Biol. Trace Elem. Res. 2015, 168, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Rooze, S.; Mathieu, F.; Claus, W.; Yangzom, T.; Yangzom, D.; Goyens, P.; De, M.V. Effect of calcium and vitamin d on growth, rickets and kashin-beck disease in 0- to 5-year-old children in a rural area of central tibet. Trop. Med. Int. Health 2016, 21, 768–775. [Google Scholar] [CrossRef] [PubMed]
- Dermience, M.; Mathieu, F.; Li, X.W.; Vandevijvere, S.; Claus, W.; De, M.V.; Dufourny, G.; Bin, L.; Yangzom, D.; Lognay, G. Minerals and trace elements intakes and food consumption patterns of young children living in rural areas of tibet autonomous region, p.R. China: A cross-sectional survey. Healthcare 2017, 5, 12. [Google Scholar] [CrossRef] [PubMed]
- Dang, S.; Yan, H.; Wang, D. Implication of world health organization growth standards on estimation of malnutrition in young chinese children: Two examples from rural western china and the tibet region. J. Child Health Care Prof. Work. Child. Hosp. Commun. 2014, 18, 358. [Google Scholar] [CrossRef] [PubMed]
- Rooze, S.; Mathieu, F.; Bally, P.; Yangzom, D.; Li, J.Z.; Goyens, P. Growth, nutritional status, and signs of rickets in 0–5-year-old children in a kashin–beck disease endemic area of central tibet. Eur. J. Pediatr. 2012, 171, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Reading, J.; Shephard, R.J. Revision of the physical activity readiness questionnaire (par-q). Can. J. Sport Sci. 1992, 17, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, M.; Tynjälä, J.; Lv, Y.; Villberg, J.; Zhang, Z.; Kannas, L. Test-retest reliability of selected items of health behaviour in school-aged children (hbsc) survey questionnaire in beijing, china. Bmc Med. Res. Methodol. 2010, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Group of China Obesity Force. Body mass index reference norm for screening overweight and obesity in Chinese children and adolescents. Chin. J. Epidemiol. 2004, 25, 97–102. (In Chinese) [Google Scholar] [CrossRef]
- Wang, J.J.; Baranowski, T.; Lau, P.W.C.; Chen, T.A.; Zhang, S.G. Psychological correlates of self-reported and objectively measured physical activity among chinese children—Psychological correlates of pa. Int. J. Environ. Res. Public Health 2016, 13, 1006. [Google Scholar] [CrossRef] [PubMed]
- Denton, J.; Dawe, R.; Fisher-Edwards, A.; Board, L. Assessment of Physical Activity at High Altitude: A Comparison of the Fitbit Charge and Actigraph gt3x+ Devices 225 Activity at High Altitude: A Comparison of the Fitbit Charge and Actigraph gt3x+ Devices; British Association of Sport and Exercise Sciences Conference: Leicester, UK, 2015. [Google Scholar] [CrossRef]
- Gang, H.; Ya, J.H.; Xiang, S.W. Physical activity assessment using accelerometers among children. China Sport Sci. 2011, 72–77. (In Chinese) [Google Scholar] [CrossRef]
- Broell, F.; Noda, T.; Wright, S.; Domenici, P.; Steffensen, J.F.; Auclair, J.P.; Taggart, C.T. Accelerometer tags: Detecting and identifying activities in fish and the effect of sampling frequency. J. Exp. Biol. 2013, 216, 1255–1264. [Google Scholar] [CrossRef] [PubMed]
- Brønd, J.C.; Arvidsson, D. Sampling frequency affects the processing of actigraph raw acceleration data to activity counts. J. Appl. Physiol. 2015, 120, jap.00628.02015. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.; Gomes, T.N.; Borges, A.; Santos, D.; Souza, M.; Santos, F.K.D.; Chaves, R.N.; Katzmarzyk, P.T.; Maia, J.A.R. Variability and stability in daily moderate-to-vigorous physical activity among 10 year old children. Int. J. Environ. Res. Public Health 2015, 12, 9248–9263. [Google Scholar] [CrossRef] [PubMed]
- Newton, R.L.; Han, H.; Sothern, M.; Martin, C.K.; Webber, L.S.; Williamson, D.A. Accelerometry measured ethnic differences in activity in rural adolescents. J. Phys. Act. Health 2011, 8, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Cain, K.L.; Sallis, J.F.; Conway, T.L.; Van, D.D.; Calhoon, L. Using accelerometers in youth physical activity studies: A review of methods. J. Phys. Act. Health 2013, 10, 437. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Loprinzi, P.D.; Moore, R.; Pfeiffer, K.A. Comparison of accelerometer cut points for predicting activity intensity in youth. Med. Sci. Sports Exerc. 2011, 43, 1360–1368. [Google Scholar] [CrossRef] [PubMed]
- Guinhouya, B.C.; Samouda, H.; Beaufort, C.D. Level of physical activity among children and adolescents in europe: A review of physical activity assessed objectively by accelerometry. Public Health 2013, 127, 301–311. [Google Scholar] [CrossRef] [PubMed]
- Diouf, A.; Thiam, M.; Idohou-Dossou, N.; Diongue, O.; Mégné, N.; Diallo, K.; Sembène, P.M.; Wade, S. Physical activity level and sedentary behaviors among public school children in dakar (senegal) measured by paq-c and accelerometer: Preliminary results. Int. J. Environ. Res. Public Health 2016, 13, 998. [Google Scholar] [CrossRef] [PubMed]
- Cooper, A.R.; Jago, R.; Southward, E.F.; Page, A.S. Active travel and physical activity across the school transition: The peach project. Med. Sci. Sports Exerc. 2012, 44, 1890–1897. [Google Scholar] [CrossRef] [PubMed]
- Ben Jemaa, H.; Mankai, A.; Mahjoub, F.; Kortobi, B.; Khlifi, S.; Draoui, J.; Minaoui, R.; Karmous, I.; Ben Hmad, H.; Ben Slama, F.; et al. Physical activity level assessed by accelerometer and paq-c in tunisian children. Ann. Nutr. Metab. 2018, 73, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Decelis, A.; Jago, R.; Fox, K.R. Physical activity, screen time and obesity status in a nationally representative sample of maltese youth with international comparisons. Bmc Public Health 2014, 14, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Mccoy, T.A.; Vander Veur, S.S.; Mallya, G.; Duffy, M.L.; Foster, G.D. Physical activity patterns of inner-city elementary schoolchildren. Med. Sci. Sports Exerc. 2013, 45, 470–474. [Google Scholar] [CrossRef] [PubMed]
- Rajala, K.; Kankaanpaa, A.; Laine, K.; Itkonen, H.; Goodman, E.; Tammelin, T. Associations of subjective social status with accelerometer-based physical activity and sedentary time among adolescents. J. Sports Sci. 2018, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Telford, R.M.; Telford, R.D.; Cunningham, R.B.; Cochrane, T.; Davey, R.; Waddington, G. Longitudinal patterns of physical activity in children aged 8 to 12 years: The look study. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 81. [Google Scholar] [CrossRef] [PubMed]
- Morgan, K.; Hallingberg, B.; Littlecott, H.; Murphy, S.; Fletcher, A.; Roberts, C.; Moore, G. Predictors of physical activity and sedentary behaviours among 11–16 year olds: Multilevel analysis of the 2013 health behaviour in school-aged children (hbsc) study in wales. Bmc Public Health 2016, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Fairclough, S.J.; Ridgers, N.D.; Welk, G. Correlates of children’s moderate and vigorous physical activity during weekdays and weekends. J. Phys. Act. Health 2012, 9, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Treuth, M.S.; Catellier, D.J.; Schmitz, K.H.; Pate, R.R.; Elder, J.P.; Mcmurray, R.G.; Blew, R.M.; Yang, S.; Webber, L. Weekend and weekday patterns of physical activity in overweight and normal-weight adolescent girls. Obesity 2007, 15, 1782–1788. [Google Scholar] [CrossRef] [PubMed]
- Jurak, G.; Soric, M.; Starc, G.; Kovac, M.; Misigoj-Durakovic, M.; Borer, K.; Strel, J. School day and weekend patterns of physical activity in urban 11-year-olds: A cross-cultural comparison. Am. J. Hum. Biol. 2015, 27, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Chan, N.Y.; Lam, S.P.; Zhang, J.; Yu, M.W.M.; Li, S.X.; Li, A.M.; Yun, K.W. Sleep education in hong kong. Sleep Biol. Rhythm. 2016, 14, 1–5. [Google Scholar] [CrossRef]
- Xiao, Y.D. Growth and Development and Its Influence Factors of Tibetan and Han Children and Adolescents. Master’s Thesis, Zhengzhou University, Zhengzhou, China, 2011. (In Chinese). [Google Scholar] [CrossRef]
- Bi, K.Z.; Qian, Z.; Guo, Z.; Ju, Z.; Xiao, J.T.; Zhi, W.W.; Xiao, Q.H. Physical activity patterns of students from grade 3 in elementary school to senior high school of tibetan, qiang and han nationality in sichuan province. Mod. Prev. Med. 2007, 34, 2028–2030. (In Chinese) [Google Scholar] [CrossRef]
- Wu, T. The qinghai-tibetan plateau: How high do tibetans live? High Alt. Med. Biol. 2001, 2, 489. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Kayser, B. High altitude adaptation in tibetans. High Alt. Med. Biol. 2006, 7, 193. [Google Scholar] [CrossRef] [PubMed]
- Weitz, C.A.; Garruto, R.M.; Chin, C.T.; Liu, J.C. Morphological growth and thorax dimensions among tibetan compared to han children, adolescents and young adults born and raised at high altitude. Ann. Hum. Biol. 2004, 31, 292–310. [Google Scholar] [CrossRef] [PubMed]
- Beall, C.M. Two routes to functional adaptation: Tibetan and andean high-altitude natives. Proc. Natl. Acad. Sci. USA 2007, 104, 8655–8660. [Google Scholar] [CrossRef] [PubMed]
- Shu, X.W. Analysis on Migration and Migrants in Tebat. Popul. Res. 2004, 28, 60–65. (In Chinese) [Google Scholar] [CrossRef]
- Wu, T.Y. Chronic mountain sickness on the qinghai-tibetan plateau. Chin Med. J. (Engl.) 2005, 118, 161–168. [Google Scholar] [PubMed]
- Chen, Q.H.; Ge, R.L.; Wang, X.Z.; Chen, H.X.; Wu, T.Y.; Kobayashi, T.; Yoshimura, K. Exercise performance of tibetan and han adolescents at altitudes of 3417 and 4300 m. J. Appl. Physiol. 1997, 83, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Bing, L. Initial Study of the Folk-custom Physical Culture in the Tibetan Temple. J. South-Cent. Univ. Natl. 2001, 21, 44–47. (In Chinese) [Google Scholar] [CrossRef]
- Wei, L.; Cong, H. Relationship Between Tibetan Traditional Sports Development and Tibetan Buddhism. J. Wuhan Inst. Phys. Educ. 2013, 47, 54–58. (In Chinese) [Google Scholar] [CrossRef]
- Verloigne, M.; Lippevelde, W.V.; Maes, L.; Yıldırım, M.; Mai, C.; Manios, Y.; Androutsos, O.; Kovács, É.; Bringolfisler, B.; Brug, J. Levels of physical activity and sedentary time among 10- to 12-year-old boys and girls across 5 european countries using accelerometers: An observational study within the energy-project. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 34. [Google Scholar] [CrossRef] [PubMed]
- Belcher, B.R.; Berrigan, D.; Dodd, K.W.; Emken, B.A.; Chihping, C.; Spruijtmetz, D. Physical activity in us youth: Effect of race/ethnicity, age, gender, and weight status. Med. Sci. Sports Exerc. 2010, 42, 2211–2221. [Google Scholar] [CrossRef] [PubMed]
- Casper, J.M.; Bocarro, J.N.; Kanters, M.A.; Floyd, M.F. Just let me play!—Understanding constraints that limit adolescent sport participation. J. Phys. Act. Health 2011, 8 (Suppl. 1), S32. [Google Scholar] [CrossRef]
- Shaw, S.M.; Henderson, K.A. Gender, leisure, and constraint: Towards a framework for the analysis of women’s leisure. J. Leis. Res. 1994, 26, 8–22. [Google Scholar] [CrossRef]
- Dunton, G.F.; Berrigan, D.; Ballardbarbash, R.; Perna, F.M.; Graubard, B.I.; Atienza, A.A. Adolescents’ sports and exercise environments in a U.S. Time use survey. Am. J. Prev. Med. 2010, 39, 122. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.D.; Chung, P.K.; Chen, W.P. Constraints of recreational sport participation: Measurement invariance and latent mean differences across sex and physical activity status. Percept. Mot. Skills 2014, 119, 363–376. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.W. Shanghai Middle School’s Expectancy-Value Motivation, Fitness Knowledge, and Physical Activity. Master‘s Thesis, Shanghai University of Sport, Shanghai, China, 2014. (In Chinese). [Google Scholar]
- Hong, J.L.; Xin, L.; Zheng, Z.W.; Juan, W.; Yin, K.C. Objective assessment of school-time physical activity of a grade 1–2 junior school students in Beijing. J. Hygien. Res. 2013, 42, 589–595. (In Chinese) [Google Scholar]
- Sallis, J.F. Epidemiology of physical activity and fitness in children and adolescents. Crit. Rev. Food Sci. Nutr. 1993, 33, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Kimm, S.Y.; Glynn, N.W.; Kriska, A.M.; Fitzgerald, S.L.; Aaron, D.J.; Similo, S.L.; Mcmahon, R.P.; Barton, B.A. Longitudinal changes in physical activity in a biracial cohort during adolescence. Med. Sci. Sports Exerc. 2000, 32, 1445–1454. [Google Scholar] [CrossRef] [PubMed]
- Dumith, S.C.; Gigante, D.P.; Domingues, M.R.; Kohl, H.W. Physical activity change during adolescence: A systematic review and a pooled analysis. Int. J. Epidemiol. 2011, 40, 685–698. [Google Scholar] [CrossRef] [PubMed]
- Harding, S.K.; Page, A.S.; Falconer, C.; Cooper, A.R. Longitudinal changes in sedentary time and physical activity during adolescence. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lobstein, T.; Jacksonleach, R.; Moodie, M.L.; Hall, K.D.; Gortmaker, S.L.; Swinburn, B.A.; James, W.P.; Wang, Y.; Mcpherson, K. Child and adolescent obesity: Part of a bigger picture. Lancet 2015, 385, 2510–2520. [Google Scholar] [CrossRef]
- Lee, Y.S. Consequences of childhood obesity. Ann. Acad. Med. Singap. 2009, 38, 75. [Google Scholar] [PubMed]
- Kerr, L.M. Physical activity and determinants of physical activity in obese and non-obese children. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 822–829. [Google Scholar] [CrossRef]
- Lohman, T.G.; Ring, K.; Pfeiffer, K.; Camhi, S.; Arredondo, E.; Pratt, C.; Pate, R.; Webber, L.S. Relationships among fitness, body composition, and physical activity. Med. Sci. Sports Exerc. 2008, 40, 1163. [Google Scholar] [CrossRef] [PubMed]
- De Bourdeaudhuij, I.; Verloigne, M.; Maes, L.; Van Lippevelde, W.; Chinapaw, M.J.M.; Te Velde, S.J.; Manios, Y.; Androutsos, O.; Kovacs, E.; Dössegger, A. Associations of physical activity and sedentary time with weight and weight status among 10- to 12-year-old boys and girls in europe: A cluster analysis within the energy project. Pediatr. Obes. 2013, 8, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Hong, I.; Cokerbolt, P.; Anderson, K.R.; Lee, D.; Velozo, C.A. Relationship between physical activity and overweight and obesity in children: Findings from the 2012 national health and nutrition examination survey national youth fitness survey. Am. J. Occup. Ther. 2016, 70, 7005180060p1–7005180060p8. [Google Scholar] [CrossRef] [PubMed]
- Annette, R.; Filip, M.; Alexander, W. The relationship between physical activity, physical fitness and overweight in adolescents: A systematic review of studies published in or after 2000. Bmc Pediatri. 2013, 13, 1–9. [Google Scholar] [CrossRef]
- Leeuw, E.D.; Borgers, N.; Smits, A. Pretesting Questionnaires for Children and Adolescents; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2004; pp. 409–429. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Variables | Sample size n (%) | Age (years) M (SD) | Height (cm) M (SD) | Weight (kg) M (SD) | BMI (kg/m2) M (SD) |
|---|---|---|---|---|---|
| Overall | 397 (100%) | 13.5 (2.7) | 154.3 (12.9) | 45.4 (13.4) | 18.7 (3.3) |
| Race | |||||
| Tibetan | 200 (50.4%) | 13.6 (2.8) | 154.9 (12.0) | 46.4 (12.8) | 18.9 (3.2) |
| Han | 197 (49.6%) | 13.3 (2.7) | 153.6 (13.7) | 44.4 (14.0) | 18.4 (3.3) |
| Gender | |||||
| Male | 195 (49.1%) | 13.5 (2.8) | 156.9 (15.1) | 47.0 (15.3) | 18.5 (3.3) |
| Female | 202 (50.9%) | 13.4 (2.7) | 151.7 (9.6) a (***) | 43.8 (11.1) | 18.8 (3.2) |
| Grade by School Level | |||||
| PS | 139 (35.0%) | 10.5 (1.0) | 141.8 (8.5) | 32.6 (7.3) | 16.1 (2.1) |
| JHS | 145 (36.5%) | 13.7 (1.3) | 158.3 (8.5) | 48.9 (9.1) | 19.4 (2.6) |
| SHS | 113 (28.5%) | 16.8 (0.9) | 164.4 (9.1) | 56.8 (10.7) | 20.9 (3.2) |
| Weight Status | |||||
| Non-OW | 356 (89.7%) | 13.3 (2.7) | 153.6 (12.9) | 43.2 (11.6) | 17.9 (2.4) |
| OW/OB | 41 (10.3%) | 14.5 (2.6) b (*) | 160.4 (10.7) b (**) | 64.6 (13.0) b (***) | 24.9 (3.1) b (***) |
| PA (Min/Day) | Whole Week M (SD) | Weekend M (SD) | Weekdays M (SD) |
|---|---|---|---|
| LPA | 207.9 (48.5) | 185.0 (52.8) | 216.7 (53.7) φ (***) |
| MPA | 43.0 (13.4) | 37.5 (21.0) | 45.1 (14.0) φ (***) |
| VPA | 19.3 (10.7) | 16.6 (14.5) | 20.4 (11.0) φ (***) |
| MVPA | 62.3 (21.7) | 54.1 (32.2) | 65.5 (22.3) φ (***) |
| Study Variables | MVPA (Min/day) M (SD) | ≥60 Min MVPA % δ | |||
|---|---|---|---|---|---|
| Total Week | Weekend | Weekday γ | All Days | 5 Days | |
| Overall | 62.3 (21.7) | 54.1 (32.2) | 65.5 (22.3) φ (***) | 9.1% | 34.8% |
| Race α | |||||
| Tibetan | 67.4 (22.7) | 63.7 (34.4) | 68.6 (23.7) φ (**) | 13.5% | 41.5% |
| Han | 57.2 (19.5) a (***) | 44.4(26.6) a (***) | 62.3 (20.4) a (**) φ (***) | 4.6% a (**) | 27.9% a (**) |
| Gender α | |||||
| Male | 71.5 (22.3) | 60.7 (35.1) | 75.6 (22.5) φ (***) | 13.8% | 51.3% |
| Female | 53.5 (17.0) b (***) | 47.8 (27.8) b (***) | 55.7 (17.2) b (***) φ (***) | 4.5% b (**) | 18.8% b (***) |
| Grade by School Level β | |||||
| PS | 61.5 (21.8) | 53.1 (30.4) | 64.5 (22.0) φ (***) | 10.1% | 35.3% |
| JHS | 63.5 (22.8) | 50.2 (30.4) | 68.8 (24.3) φ (***) | 9.7% | 37.9% |
| SHS | 61.9 (20.4) | 60.4 (36.0) | 62.4 (19.4) | 7.1% | 30.1% |
| Weight Status α | |||||
| Non-OW | 62.3 (22.0) | 54.1 (32.6) | 65.5 (22.6) φ (***) | 9.0% | 33.7% |
| OW/OB | 62.6 (19.5) | 54.4 (29.2) | 65.7 (20.3) φ (**) | 9.8% | 43.9% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nie, M.-j.; Fan, C.-q.; Sun, R.-z.; Wang, J.-j.; Feng, Q.; Zhang, Y.-f.; Yao, Z.; Wang, M. Accelerometer-Measured Physical Activity in Children and Adolescents at Altitudes over 3500 Meters: A Cross-Sectional Study in Tibet. Int. J. Environ. Res. Public Health 2019, 16, 686. https://doi.org/10.3390/ijerph16050686
Nie M-j, Fan C-q, Sun R-z, Wang J-j, Feng Q, Zhang Y-f, Yao Z, Wang M. Accelerometer-Measured Physical Activity in Children and Adolescents at Altitudes over 3500 Meters: A Cross-Sectional Study in Tibet. International Journal of Environmental Research and Public Health. 2019; 16(5):686. https://doi.org/10.3390/ijerph16050686
Chicago/Turabian StyleNie, Ming-jian, Chao-qun Fan, Rui-zhe Sun, Jing-jing Wang, Qiang Feng, Yan-feng Zhang, Zhi Yao, and Mei Wang. 2019. "Accelerometer-Measured Physical Activity in Children and Adolescents at Altitudes over 3500 Meters: A Cross-Sectional Study in Tibet" International Journal of Environmental Research and Public Health 16, no. 5: 686. https://doi.org/10.3390/ijerph16050686
APA StyleNie, M.-j., Fan, C.-q., Sun, R.-z., Wang, J.-j., Feng, Q., Zhang, Y.-f., Yao, Z., & Wang, M. (2019). Accelerometer-Measured Physical Activity in Children and Adolescents at Altitudes over 3500 Meters: A Cross-Sectional Study in Tibet. International Journal of Environmental Research and Public Health, 16(5), 686. https://doi.org/10.3390/ijerph16050686