Effect of Generational Status on Child Well-Being: Mediating Effects of Social Support and Residential Instability



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Sample, and Procedure
2.2. Measures
2.3. Statistical Analysis
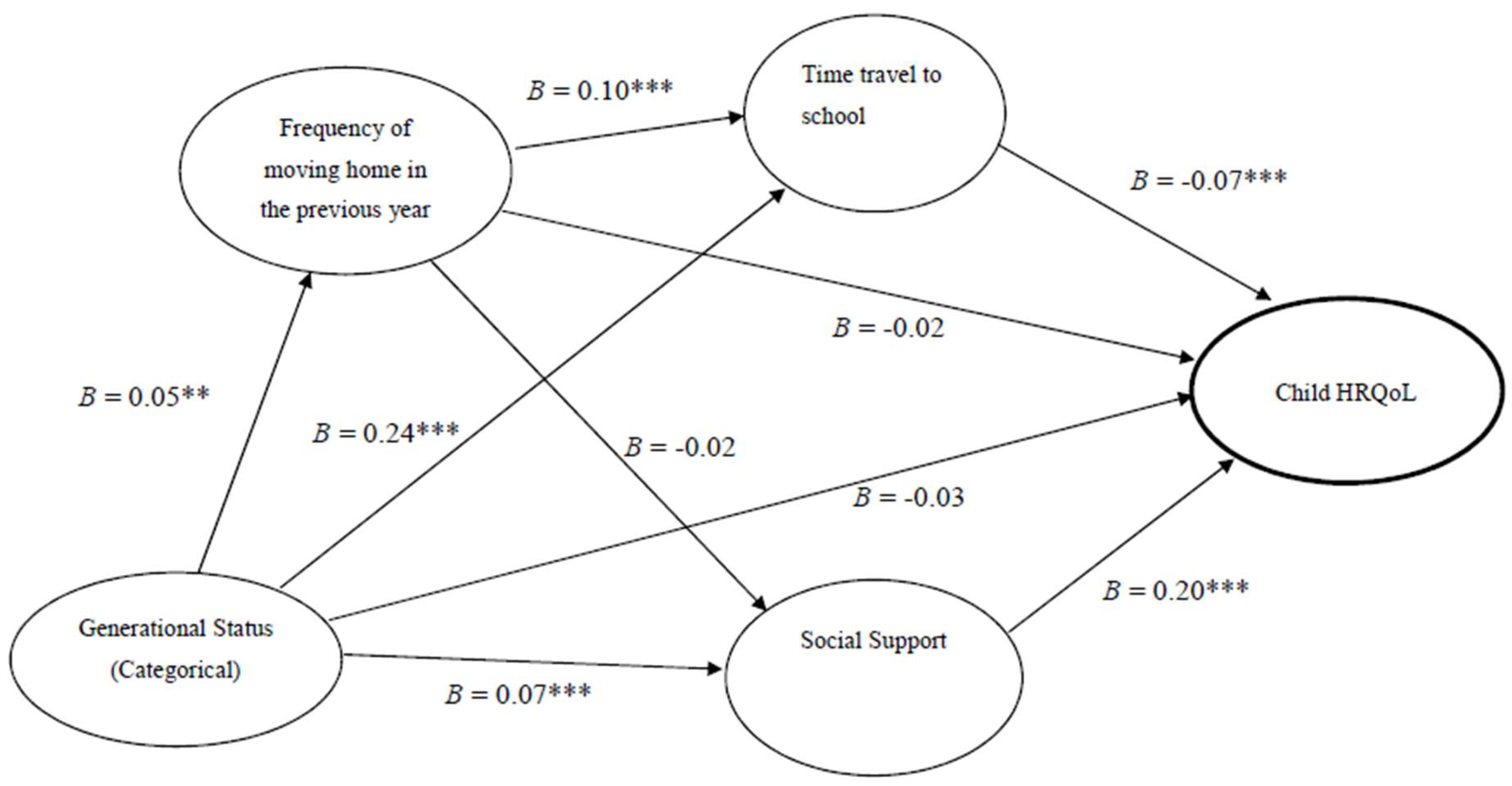
3. Results
4. Discussion
Limitations
5. Implications
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Garcia, C.C.; Lamberty, G.; Jenkins, R.; McAdoo, H.P.; Cmic, K.; Wasik, B.H.; Vazquez, G.H. An integrative model for the study of developmental competencies in minority children. Child Dev. 1996, 67, 1891–1914. [Google Scholar]
- Finch, B.K.; Hummer, R.A.; Kol, B.; Vega, W.A. The role of discrimination acculturative stress in the physical health of Mexican-origin adults. Hisp. J. Behav. Sci. 2001, 23, 399–429. [Google Scholar] [CrossRef]
- Harker, K. Immigrant generation, assimilation, and adolescent psychological well-being. Soc. Forces 2000, 79, 57–65. [Google Scholar] [CrossRef]
- Kaufman, P.; Chavez, L.; Lauen, D.; Carroll, C.D. Generational Status and Educational Outcomes among Asian and Hispanic 1988 Eighth Graders. 1988. Available online: http://nces.ed.gov/pubs99/1999020.pdf (accessed on 3 October 2018).
- Durazo, E.M.; Wallace, S.P. Access to health care across generational status for Mexican-origin immigrants in California. FACTS Rep. 2014, 10, 1–10. [Google Scholar]
- Hummer, R.A.; Powers, D.A.; Pullum, S.G.; Gossman, G.L.; Frisbie, W.P. Paradox found (again): Infant mortality among the Mexican-origin population in the United States. Demography 2007, 44, 441–457. [Google Scholar] [CrossRef] [PubMed]
- Alegria, M.; Mulvaney-Day, N.; Torres, M.; Polo, A.; Cao, Z.; Canino, G. Prevalence of psychiatric disorders across Latino subgroups in the United States. Am. J. Public Health 2007, 91, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S. Health Needs Assessment of Asian People Living in the Auckland Region. Available online: http://www.countiesmanukau.health.nz/assets/About-CMH/Performance-and-planning/health-status/2012-health-needs-of-asian-people.pdf (accessed on 30 September 2018).
- Wang, C.C.; Castaneda-Sound, C. The role of generational status, self-esteem, academic self-efficacy, and perceived social support in college students’ psychological well-being. J. Coll. Couns. 2008, 11, 101–118. [Google Scholar] [CrossRef]
- Rumbaut, R.G. Ages, life stages, and generational cohorts: Decomposing the immigrant first and second generations in the United States. Int. Migr. Rev. 2004, 38, 1160–1205. [Google Scholar] [CrossRef]
- Lederer, J. “Anchor baby”: A conceptual explanation for pejoration. J. Pragmat. 2013, 57, 248–266. [Google Scholar] [CrossRef]
- BeLue, R.; Miranda, P.Y.; Elewonibi, B.R.; Hillemeier, M.M. The Association of Generation Status and Health Insurance Among US Children. Pediatrics 2014, 134, 307–314. [Google Scholar] [CrossRef]
- Huang, Z.J.; Yu, S.M.; Ledsky, R. Health status and health service access and use among children in the U.S. immigrant families. Am. J. Public Health 2006, 96, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Orozco, C.; Yoshikawa, H. Undocumented status: Implications for child development, policy, and ethical research. New Dir. Child Adolesc. Dev. 2013, 141, 61–78. [Google Scholar] [CrossRef] [PubMed]
- Yuen, C.Y.M. Towards inclusion of cross-boundary students from Mainland China in educational policies and practices in Hong Kong. Educ. Citizensh. Soc. Justice 2011, 6, 251–264. [Google Scholar] [CrossRef]
- Scottish Executive Central Research Unit. Review of Research on School Travel. 2016. Available online: https://www2.gov.scot/Publications/2002/05/14690/4177 (accessed on 27 September 2018).
- Oppedal, B.; Roysamb, E.; Sam, D.L. The effect of acculturation and social support on chance in mental health among young immigrants. Int. J. Behav. Dev. 2004, 28, 481–494. [Google Scholar] [CrossRef]
- Salinero-Fort, M.A.; Otero-Sanz, L.; Martin-Madrazo, C.; Burgos-Lunar, C.; Chico-Moraleja, B.M.; Rodes-Soldevila, B.; Jimenez-Garcia, R.; Gomez-Campelo, P. The relationship between social support and self-reported health status in immigrants: An adjusted analysis in the Madrid Cross Sectional Study. BMC Fam. Pract. 2011, 12, 46. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.K.F.; Chou, K.L.; Chow, N.W.S. Correlates of quality of life in new migrants to Hong Kong from mainland China. Soc. Indic. Res. 2012, 107, 373–391. [Google Scholar] [CrossRef] [PubMed]
- Herz, M.; Johansson, T. The experience of being stopped: Young immigrants, social exclusion and strategies. Young 2012, 20, 157–176. [Google Scholar] [CrossRef]
- Lau, J.T.; Yu, X.N.; Chu, Y.; Shing, M.M.; Wong, E.M.; Leung, T.F.; Li, C.K.; Fok, C.K.; Mak, W.W. Validation of the Chinese version of the Pediatric Quality of Life Inventory (PedsQL) cancer module. J. Pediatr. Psychol. 2010, 35, 99–109. [Google Scholar] [CrossRef]
- Chou, K.L. Assessing Chinese adolescents’ social support: The Multidimensional Scale of Perceived Social Support. Pers. Individ. Differ. 2000, 28, 299–307. [Google Scholar] [CrossRef]
- Turner, H.A.; Finkelhor, D.; Hamby, S.L.; Shattuck, A. Family structure, victimization, and child mental health in a nationally representative sample. Soc. Sci. Med. 2013, 87, 39–51. [Google Scholar] [CrossRef]
- Efron, B.; Tibshirani, R.J. An Introduction to the Bootstrap; Chapman & Hall: Boca Raton, FL, USA, 1993; ISBN 9780412042317. [Google Scholar]
- MacKinnon, D.P.; Lockwood, C.M.; Hoffman, J.M.; West, S.G.; Sheets, V. A comparison of methods to test mediation and other intervening variable effects. Psychol. Methods 2002, 7, 83–104. [Google Scholar] [CrossRef] [PubMed]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indices in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Methen, L.K.; Muthen, B.O. Mplus User’s Guide, 6th ed.; Muthen & Muthen: Los Angeles, CA, USA, 2007. [Google Scholar]
- George, D.; Mallery, P. IBM SPSS Statistics 23 Step by Step: A Simple Guide and Reference; Routledge: Oxford, UK, 2016; ISBN 9780134320250. [Google Scholar]
- Kingsley, G.T.; Jordan, A.; Traynor, W. Addressing residential instability: Options for cities and community initiatives. Cityscape 2012, 14, 161–184. [Google Scholar]
- Berry, J.W. Immigration, acculturation, and adaptation. Appl. Psychol. 1997, 46, 5–68. [Google Scholar] [CrossRef]
- Haller, W.; Landolt, P. The transnational dimensions of identity formation: Adult children of immigrants in Miami. Ethn. Racial Stud. 2005, 28, 1182–1214. [Google Scholar] [CrossRef]
- Miller-Thayer, J. Health Migration: Crossing Borders for Affordable Health Care. Field Actions Sci. Rep. 2010, 2, 1–6. [Google Scholar]
- Wickramage, K.; Vearey, J.; Zwi, A.B.; Robinson, C.; Knipper, M. Migration and health: A global public health research priority. BMC Public Health 2018, 18, 987. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Frequency (Percentage %) | p-Value | |||
|---|---|---|---|---|---|
| All (N = 4807) | By Generational Status | ||||
| 1.75-Generation (n = 818) | Second-Generation (n = 531) | Third-or-Higher-Generation (n = 3458) | |||
| Gender | 0.14 | ||||
| Male | 2130 (44.1) | 302 (34.7) | 218 (40.1) | 1610 (44.4) | |
| Female | 2009 (44.0) | 321 (40.4) | 210 (39.2) | 1478 (44.2) | |
| Missing | 668 (11.9) | 195 (24.9) | 103 (20.8) | 370 (11.4) | |
| Age [mean (SD)] | 7.47 (2.86) | 6.59 (2.35) | 6.69 (2.67) | 7.50 (2.87) | 0.03 |
| Age range | 3–19 | 3–15 | 3–16 | 3–19 | |
| No. of siblings | <0.001 | ||||
| None | 2432 (45.2) | 488 (59.9) | 297 (58.3) | 1647 (44.6) | |
| One | 1902 (42.6) | 245 (30.1) | 198 (34.2) | 1459 (43.0) | |
| Two or more | 473 (12.2) | 85 (10.0) | 36 (7.5) | 352 (12.4) | |
| Unemployed parent(s) | 387 (8.1) | 75 (9.2) | 63 (11.9) | 249 (7.2) | 0.001 |
| Living with parents | 4643 (97.2) | 768 (94.4) | 517 (97.8) | 3358 (97.2) | 0.002 |
| Frequency of moving home in the previous year [mean (SD)] | 0.16 (0.48) | 0.21 (0.48) | 0.17 (0.45) | 0.16 (0.48) | 0.002 |
| Average commute time needed to travel between home and school (one-way) (min) [mean (SD)] | 34.32 (28.89) | 59.08 (43.30) | 37.33 (33.26) | 28.01 (27.93) | <0.001 |
| Measure | Number of Items | Cronbach’s Alpha | Mean (SD) | p-Value | |||
|---|---|---|---|---|---|---|---|
| All (N = 4807) | By Generational Status | ||||||
| 1.75-Generation (n = 818) | Second-Generation (n = 531) | Third-or-Higher-Generation (n = 3458) | |||||
| Child health-related quality of life (HRQoL) | 23 | 0.92 | 77.40 (15.18) | 74.26 (16.88) | 75.15 (16.51) | 77.51 (15.10) | 0.063 |
| Physical functioning | 8 | 0.87 | 82.83 (18.48) | 77.34 (21.47) | 78.91 (22.09) | 83.02 (18.32) | <0.001 |
| Emotional functioning | 5 | 0.83 | 76.09 (18.61) | 75.84 (17.53) | 75.22 (18.06) | 76.11 (18.64) | 0.307 |
| Social functioning | 5 | 0.80 | 78.49 (20.43) | 74.83 (21.40) | 76.51 (20.06) | 78.61 (20.41) | 0.276 |
| School functioning | 5 | 0.78 | 68.87 (19.76) | 67.08 (19.95) | 66.79 (19.88) | 68.95 (19.75) | 0.694 |
| Good communication with peers and teachers | 3 | 0.68 | 10.23 (1.73) | 10.29 (1.70) | 10.28 (1.61) | 10.22 (1.73) | 0.072 |
| Social support | 12 | 0.95 | 64.69 (13.58) | 66.37 (12.27) | 64.56 (12.98) | 64.65 (13.61) | <0.001 |
| Family | 4 | 0.93 | 22.70 (4.74) | 23.32 (4.31) | 22.46 (4.57) | 22.69 (4.76) | 0.01 |
| Friends | 4 | 0.94 | 20.83 (5.28) | 21.27 (4.66) | 20.73 (4.94) | 20.82 (5.30) | <0.001 |
| Significant other | 4 | 0.91 | 21.17 (5.18) | 21.65 (4.67) | 21.43 (4.75) | 21.16 (5.20) | <0.001 |
| Variable | B (Crude) | p-Value | β [95% Confidence Interval] | β (Adjusted) | p-Value |
|---|---|---|---|---|---|
| Generational status a | −0.03 * | 0.02 | −0.28 [−1.46, 0.898] | −0.01 | 0.64 |
| Gender b | 0.03 | 0.08 | −0.19 [−1.07, 0.87] | −0.003 | 0.84 |
| Age (year) | 0.05 ** | 0.003 | 0.46 [0.29, 0.63] | 0.09 | <0.001 |
| No. of siblings | 0.08 *** | <0.001 | 1.81 [1.08, 2.54] | 0.08 | <0.001 |
| Unemployed parent(s) c | −0.07 *** | <0.001 | −2.85 [−4.67, −1.03] | −0.05 | 0.002 |
| No. of times moved home in the previous year | −0.03 * | 0.03 | −0.63 [−1.74, 0.47] | −0.02 | 0.26 |
| Time needed to travel from home to school (one-way, in minute) | −0.08 *** | <0.001 | −0.03 [−0.04, −0.01] | −0.05 | 0.001 |
| Good communication | 0.32 *** | <0.001 | 2.74 [2/42, 3.05] | 0.30 | <0.001 |
| Social support | 0.19 *** | <0.001 | 0.10 [0.05, 0.14] | 0.08 | <0.001 |
| R2 | 0.135 | 0.135 | |||
| F for change in R2 | 58.673 | 58.673 | |||
| p-Value | <0.001 | <0.001 |
| Outcome Variable | Exogenous Variables | Effects | ||
|---|---|---|---|---|
| Direct | Indirect | Total | ||
| Child HRQoL | ||||
| Social Support | 0.20 *** | – | – | |
| Time travel to school | −0.07 *** | – | – | |
| Frequency of moving home in previous year | −0.02 | – | – | |
| Generational status a | −0.03 | – | – | |
| Time travel to school | ||||
| Generational status a | 0.24 *** | – | – | |
| Frequency of moving home in previous year | 0.10 *** | – | – | |
| Social Support | ||||
| Generational status a | 0.07 *** | – | – | |
| Frequency of moving home in previous year | −0.02 | – | – | |
| Generational status | ||||
| Frequency of moving home in previous year | 0.05 ** | – | – | |
| Child HRQoL | ||||
| Generational status a | −0.03 | – | −0.03 *** | |
| Via Social Support | − | 0.01 *** | – | |
| Via Time travel to school | − | −0.02 *** | – | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, K.L.; Lo, R. Effect of Generational Status on Child Well-Being: Mediating Effects of Social Support and Residential Instability. Int. J. Environ. Res. Public Health 2019, 16, 435. https://doi.org/10.3390/ijerph16030435
Chan KL, Lo R. Effect of Generational Status on Child Well-Being: Mediating Effects of Social Support and Residential Instability. International Journal of Environmental Research and Public Health. 2019; 16(3):435. https://doi.org/10.3390/ijerph16030435
Chicago/Turabian StyleChan, Ko Ling, and Ruby Lo. 2019. "Effect of Generational Status on Child Well-Being: Mediating Effects of Social Support and Residential Instability" International Journal of Environmental Research and Public Health 16, no. 3: 435. https://doi.org/10.3390/ijerph16030435
APA StyleChan, K. L., & Lo, R. (2019). Effect of Generational Status on Child Well-Being: Mediating Effects of Social Support and Residential Instability. International Journal of Environmental Research and Public Health, 16(3), 435. https://doi.org/10.3390/ijerph16030435