Assessing the Impact of the Twin Track Socio-Economic Intervention on Reducing Leprosy-Related Stigma in Cirebon District, Indonesia

 ,
,
Abstract
1. Introduction
Theoretical Framework: Stigma and Socio-Economic Transformation
2. Materials and Methods
2.1. Study Design and Study Area
2.2. Study Population
2.3. Research Methods and Sampling
2.3.1. Quantitative Measures
2.3.2. Qualitative Measures
2.4. Analysis
2.5. Overview of the SED Intervention and How It Is Embedded in the Local System
2.6. Ethics
3. Results
3.1. Participants of the SED Intervention
3.2. Characteristics of the Study Population
3.3. Economic Transformation: Impact of SED on Socio-Economic Status of the Clients
We can use [the profit] for daily needs and for school… My wife can open a business. We opened a Rujak [traditional fruit and vegetable dish] shop.(FGD 2 client SED)
Interviewer: How much income did you get from that IDR 200,000 capital?Interviewee: Yah, IDR 50,000 [US$ 4]Interviewer: You got IDR 50,000? [US$ 4]Interviewee: If it’s afternoon I earn IDR 25,000 [US $2].Interviewer: ... So if its morning and afternoon you got IDR 75,000 [US $6] per day, right, is it enough for your family daily needs?Interviewee: Thank God, it’s enough.Interviewer: Is it the same between now and before, sir?Interviewee: It’s different.Interviewer: What is the difference, sir?Interviewee: Yes, capital increased, more progress.(IDI S-CS18-Man-50)
I became happier. I have more money. I can go to the market to sell something. I used to only stay at home and have no activity. I have a capital so I can go to the market. So I have a happy feeling.(FGD 1 client SED)
I save at school [microcredit group meeting] ...I save at home too. I save the change from the money spent on daily needs.(IDI S-CS01-woman-35)
3.4. Changes in Well-Being: Impact of Sed on Stigma, the Effects of Stigma and Quality of Life
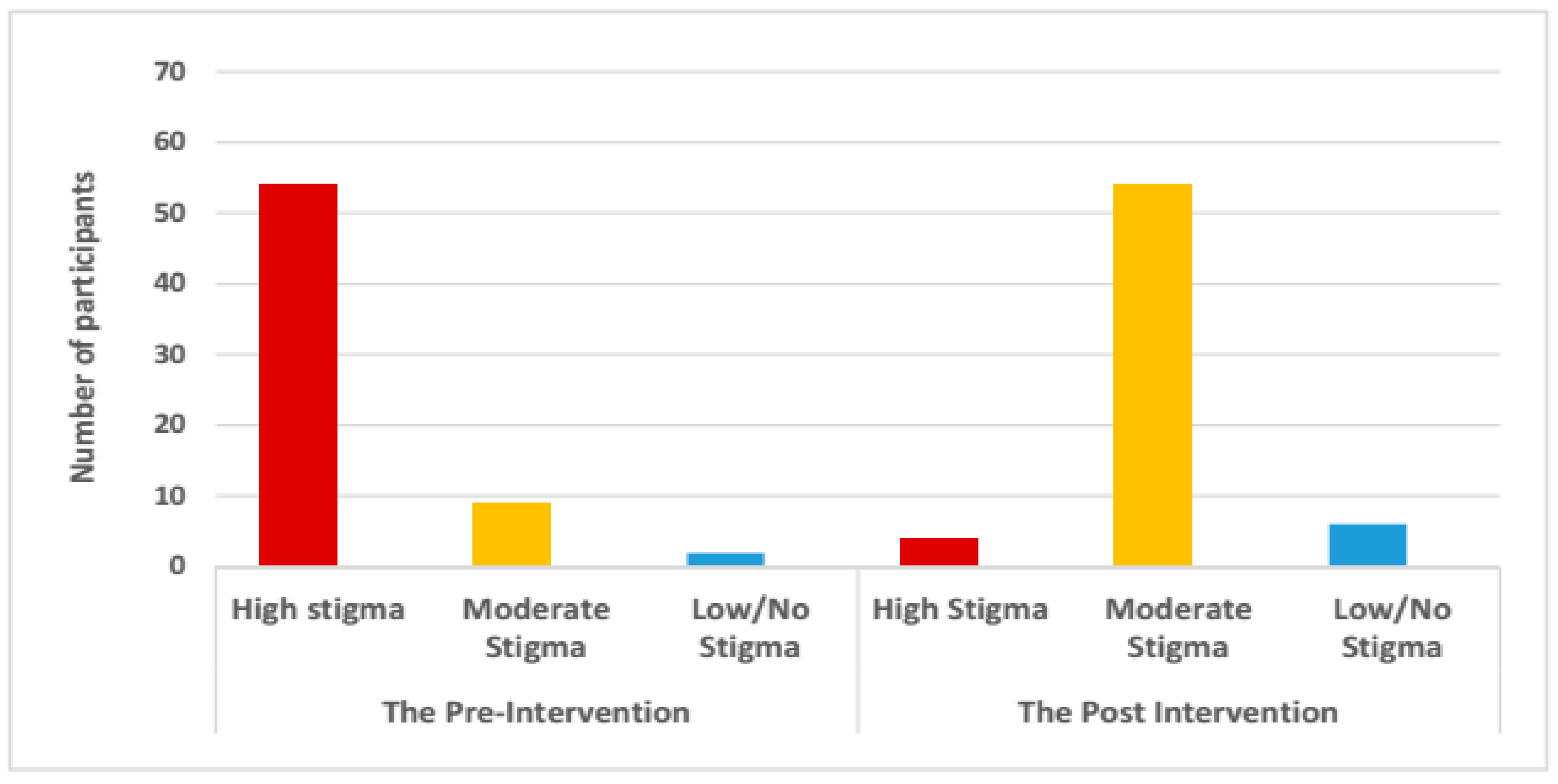
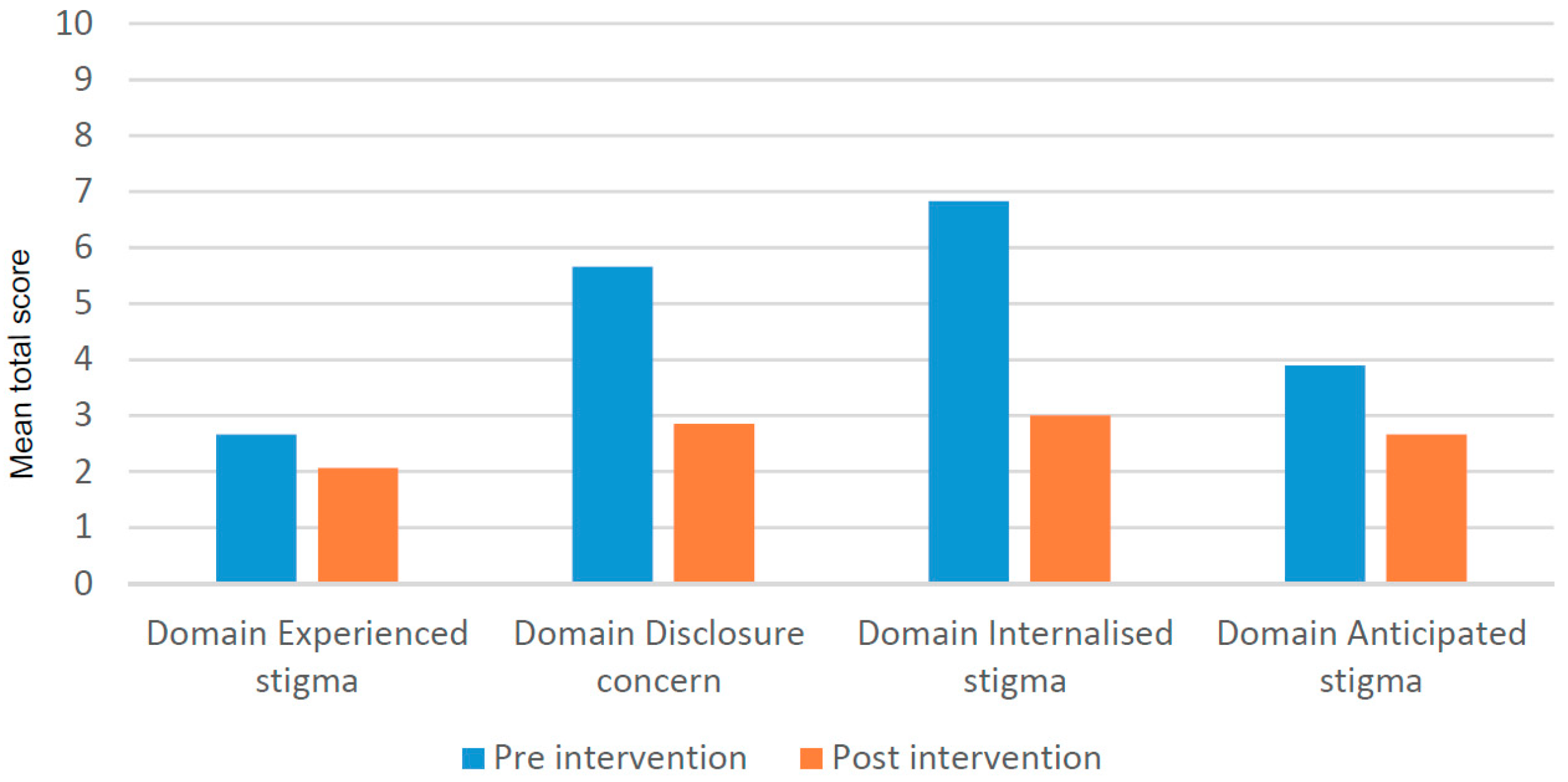
3.4.1. Impact on Different Types of Stigma and Disclosure Concerns
My husband has changed. He used to be quiet, didn’t interact or have friends but after SARI came, he has changed. He interacts and doesn’t hide himself any more.(FGD family counselling-SED client)
Interviewer: What do you feel after you joined [the SED activity]?Interviewee: Maybe I’ve become better, more courageous. Basically I’ve been better than before.Interviewer: Do you still have any bad feelings about leprosy?Interviewee: I used to, but now I don’t think about it too much.Interviewer: Did you ever talk to anyone else [about your disease]?Interviewee: Some people, yes.Interviewer: What do you talk about?Interviewee: About the disease—the symptoms, the medicines, how to treat it, etc. we basically explained to everyone about what leprosy is?(IDI S-CS09-female-43)
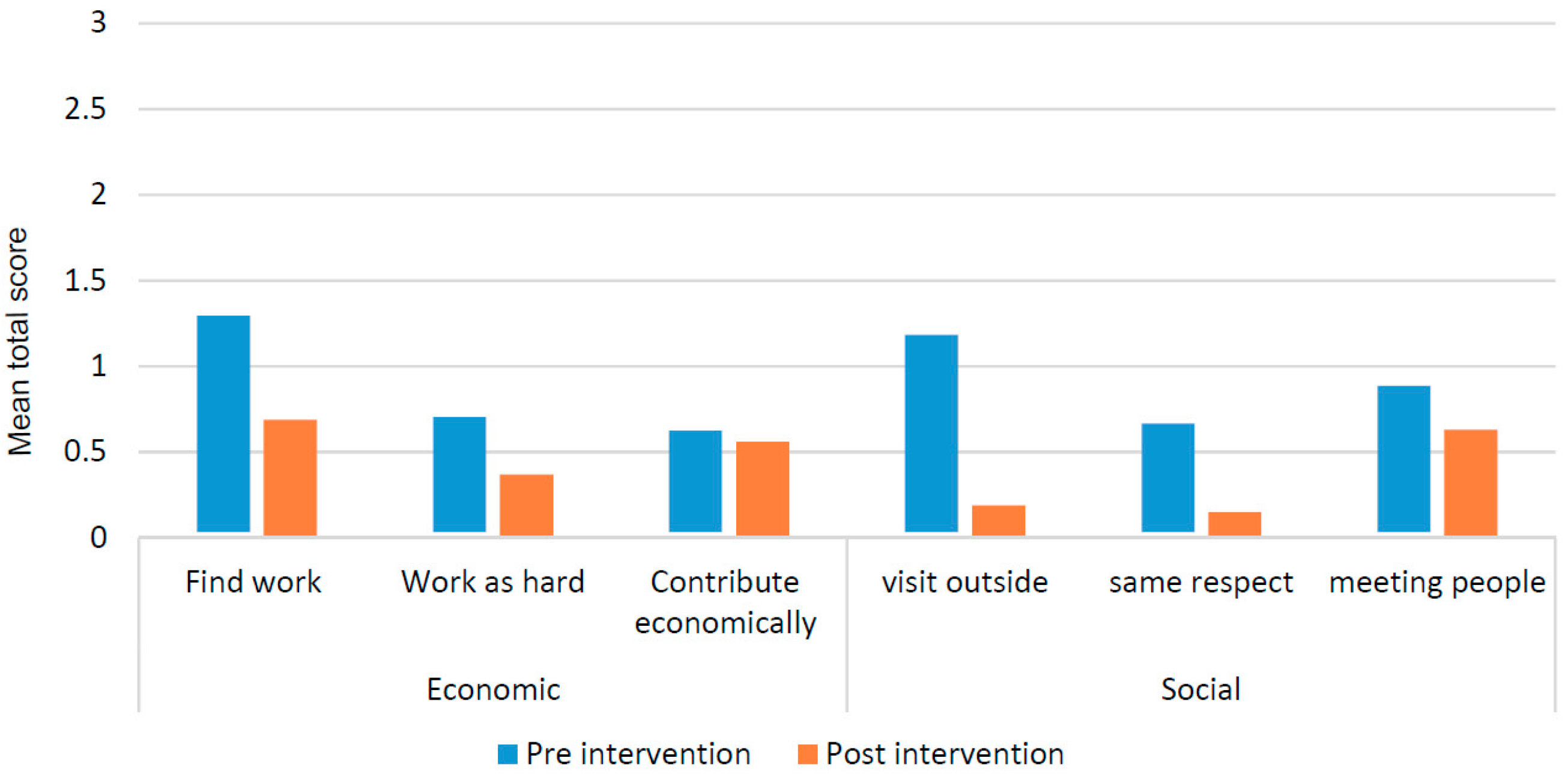
3.4.2. Impact on Participation Restriction
When I had leprosy, I felt numbness so I never went out of the house. After SARI came to my house, I became confident and capable to socialize with other people.(FGD 2 client SED)
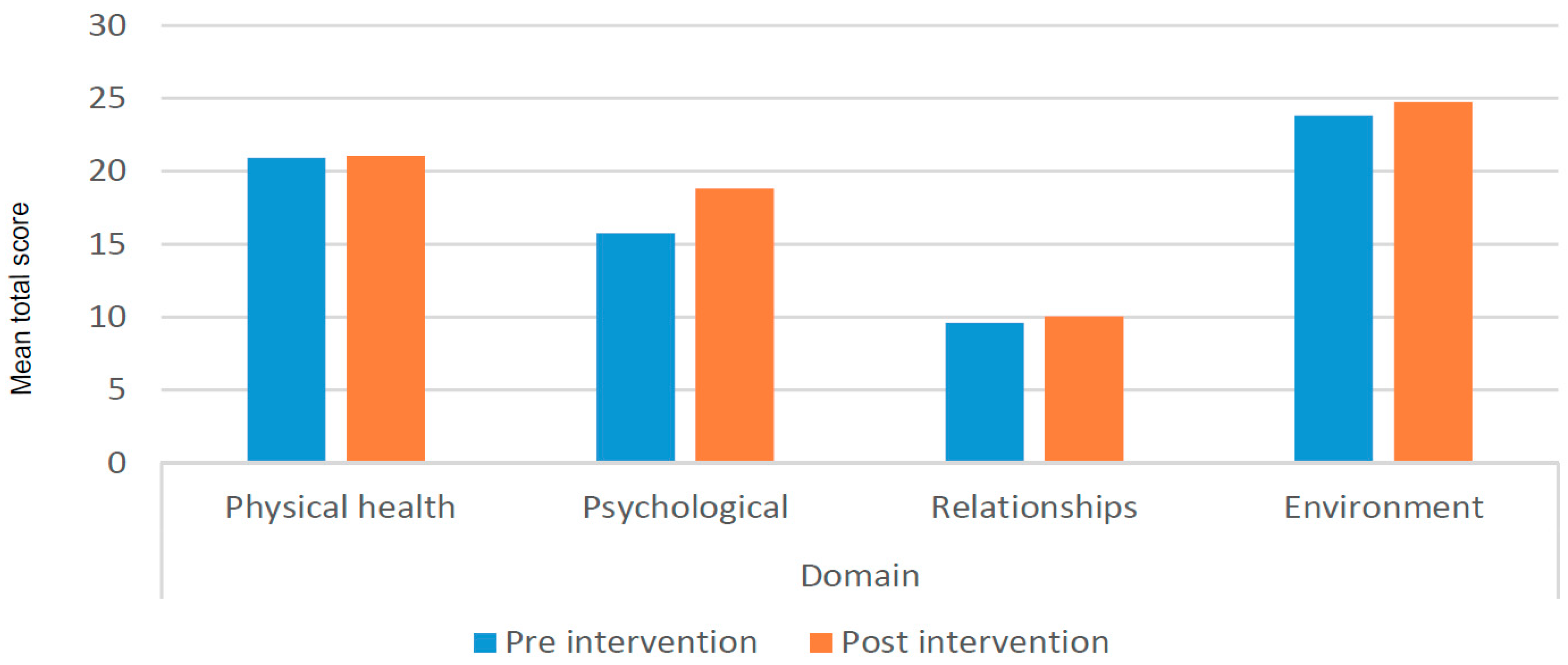
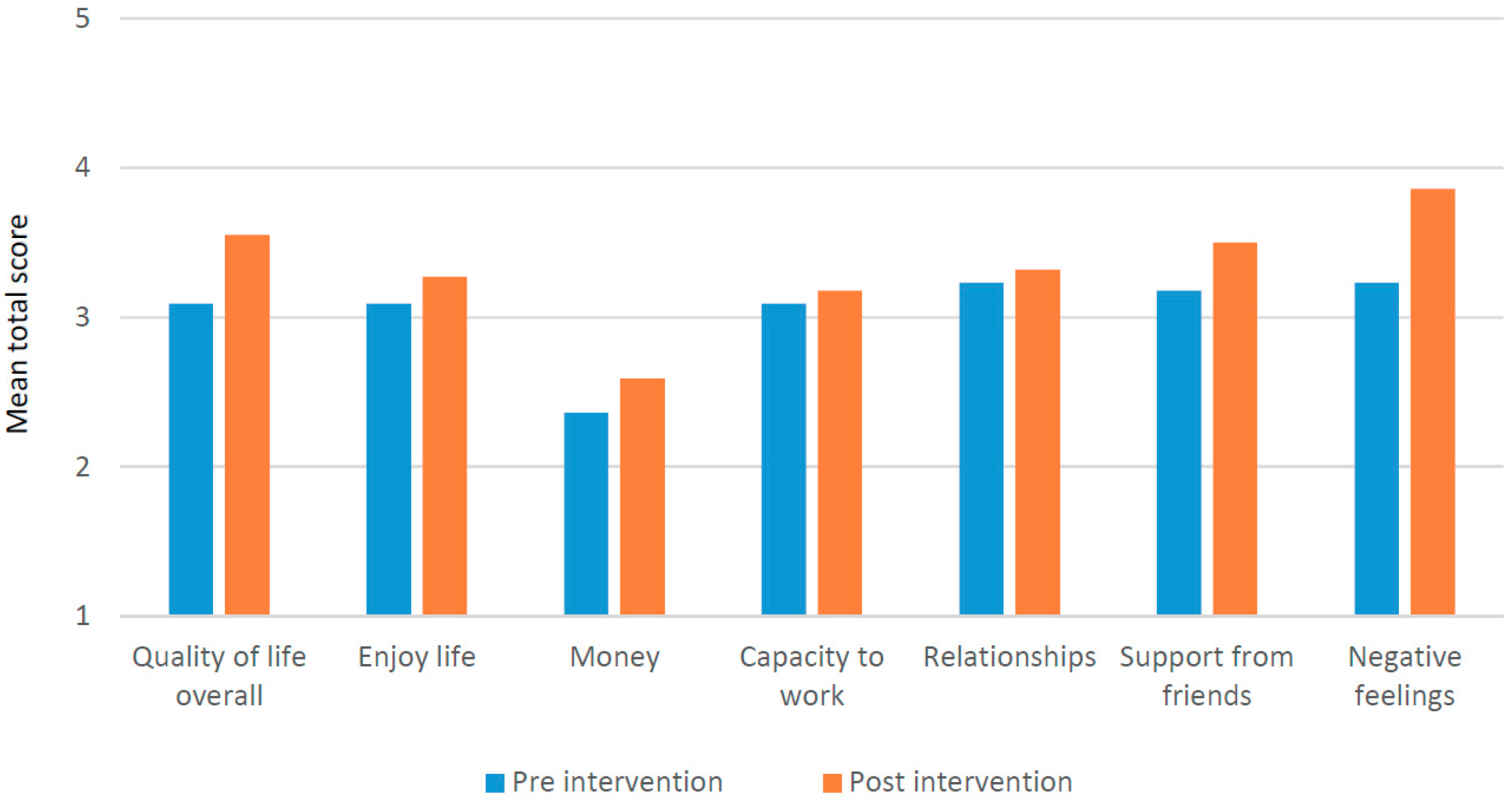
3.4.3. Impact on Quality of Life
3.5. Social Transformation: Re-Integration of People Affected by Leprosy into the Community
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Stevelink, S.A.M.; Van Brakel, W.H.; Augustine, V. Stigma and social participation in Southern India: Differences and commonalities among persons affected by leprosy and persons living with HIV/AIDS. Psychol. Health Med. 2011, 16, 695–707. [Google Scholar] [CrossRef] [PubMed]
- Rüsch, N.; Angermeyer, M.C.; Corrigan, P.W. Mental illness stigma: Concepts, consequences, and initiatives to reduce stigma. Eur. Psychiatry 2005, 20, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Peters, R.M.H.; Dadun; Lusli, M.; Miranda-Galarza, B.; Van Brakel, W.H.; Zweekhorst, M.B.M.; Damayanti, R.; Seda, F.S.S.E.; Bunders, J.F.G.; Irwanto. The meaning of leprosy and everyday experiences: An exploration in Cirebon, Indonesia. J. Trop. Med. 2013. [Google Scholar] [CrossRef] [PubMed]
- Kinsman, J. “A time of fear”: Local, national, and international responses to a large Ebola outbreak in Uganda. Globalization Health 2012, 8, 1. [Google Scholar] [CrossRef] [PubMed]
- Somma, D.; Thomas, B.E.; Karim, F.; Kemp, J.; Arias, N.; Auer, C.; Gosoniu, G.D.; Abouihia, A.; Weiss, M.G. Gender and socio-cultural determinants of TB-related stigma in Bangladesh, India, Malawi and Colombia. Int. J. Tuberc. Lung Dis. 2008, 12, 856–866. [Google Scholar] [PubMed]
- van Brakel, W.H.; Sihombing, B.; Djarir, H.; Beise, K.; Kusumawardhani, L.; Yulihane, R.; Kurniasari, I.; Kasim, M.; Kesumaningsih, K.I.; Wilder-Smith, A. Disability in people affected by leprosy: The role of impairment, activity, social participation, stigma and discrimination. Glob. Health Action 2012, 5, 18394. [Google Scholar] [CrossRef]
- Tsutsumi, A.; Izutsu, T.; Islam, A.M.; Maksuda, A.N.; Kato, H.; Wakai, S. The quality of life, mental health, and perceived stigma of leprosy patients in Bangladesh. Soc. Sci. Med. 2007, 64, 2443–2453. [Google Scholar] [CrossRef]
- Heijnders, M.L. Experiencing leprosy: Perceiving and coping with leprosy and its treatment. A qualitative study conducted in Nepal. Leprosy Rev. 2004, 75, 327–337. [Google Scholar]
- Goffman, E. Stigma: Notes on the Management of Spoiled Identity; Simon & Schuster, Inc.: New York, NY, USA, 1963. [Google Scholar]
- Velema, J.P. Guest Editorial Best Practices in the Socio-Economic Rehabilitation of Persons Affected by Leprosy and other Marginalised People in Their Communities: Findings From Nine Evaluations in Bangladesh, India And Africa. Asia Pac. Disabil. Rehabil. J. 2008, 19, 3–18. [Google Scholar]
- Ebenso, B.; Fashona, A.; Ayuba, M.; Idah, M.; Adeyemi, G.; S-fada, S. Impact of Socio-Economic Rehabilitation on Leprosy Stigma in Northern Nigeria: Findings of a Retrospective Study. Asia Pac. Disabil. Rehabil. J. 2007, 18, 98–119. [Google Scholar]
- Cabral-Miranda, W.; Chiaravalloti Neto, F.; Barrozo, L.V. Socio-economic and environmental effects influencing the development of leprosy in Bahia, North-Eastern Brazil. Trop. Med. Int. Health 2014, 19, 1504–1514. [Google Scholar] [CrossRef] [PubMed]
- Sales, A.M.; Campos, D.P.; Hacker, M.A.; da Costa Nery, J.A.; Düppre, N.C.; Rangel, E.; Sarno, E.N.; Penna, M.L.F. Progression of leprosy disability after discharge: Is multidrug therapy enough? Trop. Med. Int. Health 2013, 18, 1145–1153. [Google Scholar] [CrossRef]
- Nicholls, P.G.; Wiens, C.; Smith, W.C.S. Delay in Presentation in the Context of Local Knowledge and Attitude Towards Leprosy—The Results of Qualitative Fieldwork in Paraguay. Int. J. Lepr. Mycobact. Dis. 2003, 71, 198–209. [Google Scholar] [CrossRef]
- Heijnders, M. The dynamics of stigma in leprosy. Int. J. Lepr. Mycobact. Dis. 2004, 72, 437–447. [Google Scholar] [CrossRef]
- Peters, R.M.; Hofker, M.E.; van Brakel, W.H.; Marjolein, Z.B.; Seda, F.S.; Irwanto, I.; Bunders, J.F. Narratives Around Concealment and Agency for Stigma-reduction: A Study of Women Affected by Leprosy in Cirebon District, Indonesia. Disabil. CBR Incl Dev. 2014, 25, 5–21. [Google Scholar] [CrossRef]
- Calcraft, J.H. The effects of the stigma of leprosy on the income generation of leprosy affected people in the Terai area of South East Nepal. Asia Pac. Disabil. Rehabil. J. 2006, 17, 73–89. [Google Scholar]
- Heidinger, M.; Simonnet, E.; Karippadathu, S.F.; Puchinger, M.; Pfeifer, J.; Grisold, A. Analysis of Social Determinants of Health and Disability Scores in Leprosy-Affected Persons in Salem, Tamil Nadu, India. Int. J. Environ. Res. Public Health 2018, 15, 2769. [Google Scholar] [CrossRef]
- Dadun, D.; Peters, R.; Lusli, M.; Miranda-Galarza, B.; van Brakel, W.; Zweekhorst, M.; Damayanti, R.; Irwanto, I.; Bunders, J. Exploring the complexities of leprosy-related stigma and the potential of a socio-economic intervention in a public health context in Indonesia. Disabil. CBR Incl. Dev. 2016, 27, 5–23. [Google Scholar] [CrossRef]
- Velema, J.P.; Ebenso, B.; Fuzikawa, L. Evidence for the effectiveness of rehabilitation-in-the-community programmes. Lepr. Rev. 2008, 79, 65–82. [Google Scholar]
- Abera, M.; Shanko, M. Small loan schemes: The experience of Ethiopia. Lepr. Rev. 2000, 71, 517–520. [Google Scholar] [CrossRef]
- Croft, R.P.; Croft, R.A. Knowledge, attitude and practice regarding leprosy and tuberculosis in Bangladesh. Lepr. Rev. 1999, 70, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Briden, A.; Maguire, E. An assessment of knowledge and attitudes towards leprosy/Hansen’s disease amongst healthcare workers in Guyana. Lepr. Rev. 2003, 74, 154–162. [Google Scholar] [PubMed]
- Pati, A.P.; Lyngdoh, B.F. Microfinance Intervention and Socio-Economic Transformation: An Application of Propensity Score Matching and Difference-in-Difference Technique. 2010. Available online: http://papers.ssrn.com/sol3/papers.cfm?abstract_id=1630268 (accessed on 18 January 2019).
- Withington, S.G.; Joha, S.; Baird, D.; Brink, M.; Brink, J. Assessing socio-economic factors in relation to stigmatization, impairment status, and selection for socio-economic rehabilitation: A 1-year cohort of new leprosy cases in north Bangladesh. Lepr. Rev. 2003, 74, 120–132. [Google Scholar] [PubMed]
- Jayadevan, P.; Balakrishnan, R. Socio-economic rehabilitation in leprosy—An example. Lepr. Rev. 2002, 73, 88–89. [Google Scholar] [PubMed]
- Devadas, T.J. Socio Economic Rehabilitation in Leprosy- Current Status and future needs. Heal Adm. 2006, XVIII-2, 86–90. [Google Scholar]
- Ebenso, B.; Idah, M.; Anyor, T.; Opakunmi, F. Lessons from the evolution of a CBR programme for people affected by leprosy in Northern Nigeria. Lepr. Rev. 2010, 81, 318–331. [Google Scholar] [PubMed]
- Weiss, M.G. Stigma and the social burden of neglected tropical diseases. PLoS Negl. Trop. Dis. 2008, 2, e237. [Google Scholar] [CrossRef]
- Peters, R.M.H.; Zweekhorst, M.B.M.; Bunders, J.F.G.; van Brakel, W.H. A Cluster-Randomized Controlled Intervention Study to Assess the Effect of a Contact Intervention in Reducing Leprosy-Related Stigma in Indonesia. PLoS Negl. Trop. Dis. 2015, 9, e0004003. [Google Scholar] [CrossRef]
- Lusli, M.; Peters, R.; Van Brakel, W.; Zweekhorst, M.; Iancu, S.; Bunders, J.; Regeer, B. The Impact of a Rights-Based Counselling Intervention to Reduce Stigma in People Affected by Leprosy in Indonesia. PLoS Negl. Trop. Dis. 2016, 10, 1–25. [Google Scholar] [CrossRef]
- Lusli, M.; Peters, R.; Bunders, J.; Irwanto, I.; Zweekhorst, M. Development of a rights-based counselling practice and module to reduce leprosy-related stigma and empower people affected by leprosy in Cirebon District, Indonesia. Lepr. Rev. 2017, 88, 318–333. [Google Scholar]
- van Brakel, W.H. Measuring leprosy stigma—A preliminary review of the leprosy literature. Int. J. Lepr. Mycobact. Dis. 2003, 71, 190–197. [Google Scholar] [CrossRef]
- Nyblade, L.C. Measuring HIV stigma: Existing knowledge and gaps. Psychol. Health Med. 2006, 11, 335–345. [Google Scholar] [CrossRef] [PubMed]
- Cross, H.A.; Heijnders, M.; Dalal, A.; Sermrittirong, S.; Mak, S. Interventions for Stigma Reduction—Part 1: Theoretical Considerations. Disabil. CBR Incl. Dev. 2011, 22, 62–70. [Google Scholar] [CrossRef]
- Berger, B.E.; Ferrans, C.E.; Lashley, F.R. Measuring stigma in people with HIV: Psychometric assessment of the HIV stigma scale. Res. Nurs. Health 2001, 24, 518–529. [Google Scholar] [CrossRef] [PubMed]
- Van Brakel, W.; Lusli, M. Cultural validation of a new instrument to measure leprosy-related stigma: The SARI Stigma Scale. Lepr. Rev. 2017, 88, 23–42. [Google Scholar]
- Stevelink, S.A.M.; Hoekstra, T.; Nardi, S.M.T.; van der Zee, C.H.; Banstola, N.; Premkumar, R.; Nicholls, P.G.; van Brakel, W.H. Development and structural validation of a shortened version of the Participation Scale. Disabil. Rehabil. 2012, 34, 1596–1607. [Google Scholar] [CrossRef] [PubMed]
- Van Brakel, W.H.; Anderson, A.M.; Mutatkar, R.K.; Bakirtzief, Z.; Nicholls, P.G.; Raju, M.S.; Das-Pattanayak, R.K. The Participation Scale: Measuring a key concept in public health. Disabil. Rehabil. 2006, 28, 193–203. [Google Scholar] [CrossRef]
- Rensen, C.; Bandyopadhyay, S.; Gopal, P.K.; van Brakel, W.H. Measuring leprosy-related stigma—A pilot study to validate a toolkit of instruments. Disabil. Rehabil. 2010, 33, 711–719. [Google Scholar] [CrossRef]
- Stevelink, S.A.M.; Terwee, C.B.; Banstola, N.; van Brakel, W.H. Testing the psychometric properties of the Participation Scale in Eastern Nepal. Qual. Life Res. 2013, 22, 137–144. [Google Scholar] [CrossRef]
- Ebenso, J.; Velema, J.P. Test-retest reliability of the Screening Activity Limitation and Safety Awareness (SALSA) scale in North-West Nigeria. Lepr. Rev. 2009, 80, 197–204. [Google Scholar]
- Trompenaars, F.J.; Masthoff, E.D.; Van Heck, G.L.; Hodiamont, P.P.; De Vries, J. Content validity, construct validity, and reliability of the WHOQOL-Bref in a population of Dutch adult psychiatric outpatients. Qual. Life Res. 2005, 14, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Skevington, S.M.; Lotfy, M.; O’Connell, K.A. The World Health Organization’s WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial. A Report from the WHOQOL Group. Qual. Life Res. 2004, 13, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Salim, O.C.; Sudharma, N.I.; Kusumaratna, R.K.; Hidayat, A. Validitas dan reliabilitas World Health Organization Quality of Life -BREF untuk mengukur kualitas hidup lanjut usia. Universa Med. 2007, 26, 27–38. [Google Scholar]
- Jones, D.; Webster, L. A Handbook on Mainstreaming Disability; VSO United Kingdom: London, UK, 2006. [Google Scholar]
- Albert, B. In or Out of The Mainstream? Lessons from Research on Disability and Development Cooperation; Edited by Lessons from the Disability Knowledge and Research Programme; Disability Press: Leeds, UK, 2006. [Google Scholar]
- Miller, C.; Albert, B. Mainstreaming Disability in Development Cooperation: Lessons from Gender Mainstreaming. Available online: https://assets.publishing.service.gov.uk/media/57a08c5be5274a27b2001147/RedPov_gender.pdf (accessed on 31 October 2018).
- DFID. Disability, Poverty and Development; DFID: London, UK, 2000. [Google Scholar]
- Cornielje, H.; Piefer, A.; Khasnabis, C.; Thomas, M.; Velema, J.P. Inclusion of persons affected by leprosy in CBR. Lepr. Rev. 2008, 79, 30–35. [Google Scholar]
- Hossain, M. Credit for Alleviation of Rural Poverty: The Grameen Bank in Bangladesh; Intl Food Policy Res Inst: Washington, DC, USA, 1988. [Google Scholar]
- KOMIDA. History of KOMIDA. 2016. Available online: http://mitradhuafa.com/index.php/history/ (accessed on 31 October 2018).
- Farida, F.; Hermanto, S.; Nunung, N. Micro Enterprises â€TM Access to People Business Credit Program in Indonesia: Credit Rationed or Non-Credit Rationed? Int. J. Econ. Perspect. 2015, 9, 57–70. [Google Scholar]
- Okten, C.; Osili, U.O. Social networks and credit access in Indonesia. World Dev. 2004, 32, 1225–1246. [Google Scholar] [CrossRef]
- Mustapha, B.R.; Jung, J.; Veronica, Z. Social Entrepreneurship in Indonesia and China: From Micro Credit to Community Developement. 2007. Available online: http://www.ufhrd.co.uk/wordpress/wp-content/uploads/2008/06/must-186-wp.pdf (accessed on 31 October 2018).
- Lockwood, H.; Moriarty, P.; Verdemato, T. Providing Sustainable Water Services at Scale. Int. Symp. Rural Water Serv. 2010, 13, 1–37. [Google Scholar]
- Wagner, G.; Rana, Y.; Linnemayr, S.; Balya, J.; Buzaalirwa, L. A qualitative exploration of the economic and social effects of microcredit among people living with HIV/AIDS in Uganda. AIDS Res. Treat. 2012. [Google Scholar] [CrossRef]
- Heijnders, M.; van der Meij, S. The fight against stigma: An overview of stigma-reduction strategies and interventions. Psychol. Health Med. 2006, 11, 353–363. [Google Scholar] [CrossRef]
- Cross, H.A.; Heijnders, M.; Dalal, A.; Sermrittirong, S.; Mak, S. Interventions for Stigma Reduction—Part 2: Practical Applications. Disabil. CBR Incl. Dev. 2011, 22, 71–80. [Google Scholar] [CrossRef]
- Shumin, C.; Diangchang, L.; Bing, L.; Lin, Z.; Xioulu, Y. Assessment of disability, social and economic situations of people affected by leprosy in Shandong Province, People’s Republic of China. Lepr. Rev. 2003, 74, 215–221. [Google Scholar] [PubMed]
- Joseph, G.A.; Rao, P.S.S.S. Impact of leprosy on the quality of life. Bull. World Health Organ. 1999, 77, 515–517. [Google Scholar] [PubMed]
- Chien-Yi, O.W.; Lee, B.-O. Relationships Between Perceived Stigma, Coping Orientations, Self-esteem, and Quality of Life in Patients With Schizophrenia. Asia Pac. J. Public Health 2015, 27, NP1932–NP1941. [Google Scholar]
- UNITED NATIONS. Transforming our world: The 2030 Agenda for Sustainable Development. In Resolution Adopted by the General Assembly; UNITED NATIONS: New York, NY, USA, 2015. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Approach | Research Methods | Details | Phase | # | Study Population/Object | Stages of the Model of Pati and Lyngdoh |
|---|---|---|---|---|---|---|
| Quantitative | SARI Stigma Scale (SSS) | - Based on the Berger Scale [36] - Adequate cultural validity [37] - 4 Domains: Experienced stigma, Internalized stigma, Disclosure concerns and Anticipated stigma - The SSS asks if a certain experience/feeling occurs (e.g., feel unclean, feel guilty) and if so how frequent (scoring 0–3). | Baseline & Final survey | 143 | SED clients and people affected by leprosy who lived in the control and counselling/contact area | Well-being |
| Participation Scale Short (PSS) | - Shorter version of the Participation Scale which measures restriction in social participation [38,39]. - Participation Scale is validated in several countries [40,41,42] and used in Indonesia before [6]. - The PSS asks whether the interviewee takes part in, for example, family discussions, as their peers do. - The scale has 13 items and a scoring (0–3). | Well-being | ||||
| WHO Quality of Life BREF (WHOQOL-BREF) | - 4 Domains; Physical health, Psychological health, Relationships and Environment. - Has been validated, and is widely used in many countries including Indonesia [43,44,45]. | Well-being | ||||
| Qualitative | In-depth interview | - The interviews explored the changes clients experienced in their (i) financial situation, (ii) social situation, (iii) household situation, (iv) health and (v) general well-being. - Most interviews were conducted at the SED client’s house. | Final survey | 20 | SED clients | Economic transformation, well-being, social transformation |
| Focus Group Discussion | - Generally the following topics were discussed: (i) financial situation, (ii) social situation, (iii) household situation, (iv) health, (v) general well-being and (vi) the intervention itself. | Final survey | 43 | SED clients (2x), family of SED clients, leprosy workers, SED providers (2x), research assistants | Economic transformation, well-being, social transformation | |
| Profile participant SED | - Written by research assistants, who compared the socio-economic status (of the household and of the business) and stigma before and after the SED intervention. Special attention was paid to being afraid of leprosy, feelings of shame, ideas on concealment/disclosure, willingness to interact with community members. | Final survey | 74 | SED clients | Economic transformation, well-being, social transformation | |
| Logbooks, informal interviews, observation | - To assess sustainability of the intervention. - Focus on the demand for socio-economic intervention, the extent to which it addresses the needs of clients, the intensity of the relationship between client and credit provider, embedding in the local system, and the continuation of the intervention one year and two years after the project ended. | Continuously | NA | Study object: sustainability of intervention | N/A |
| Organization | Activity | Intensity of Relation Between Loan Provider and Client | Degree of Regulation | Degree of Disability-Specific (As Opposed to Mainstream) |
|---|---|---|---|---|
| KOMIDA 1 | Micro-credit | Low | High | Low |
| FKDC 2 | Micro-credit | High | Middle | High/middle |
| FKDC | Individual loans | Middle | Low | High |
| DSWO 3 | Livestock | Low | Middle | High |
| SARI 4 and DSWO | Skills training | Middle | Low | High |
| Microcredit | Livestock (Goats) | Skills Training | |||
|---|---|---|---|---|---|
| KOMIDA | FKDC | Individual | DSWO/Others | SARI and DSWO | |
| Persons affected by leprosy | 40 | 20 | 11 | 21 | 52 |
| Community members | 242 | 4 | - | - | 5 |
| Persons with disabilities | - | 8 | - | - | - |
| Total | 282 | 32 | 11 | 21 | 57 |
| Quantitative | Qualitative | ||||||
|---|---|---|---|---|---|---|---|
| Cohort (n = 237) | Profile Observation | In-Depth Interview | FGD | ||||
| SED Participants | Control | Counselling-Contact Area | SED Participants | SED Participants | Mixed | ||
| n | 29 (12%) | 57 (24%) | 57 (24%) | 65 | 20 | 43 | |
| Sex (male) | 13 (45%) | 37 (65%) | 38 (67%) | 29 (44%) | 5 (25%) | 29 (67%) | |
| Age (mean/range) in years | 33 | 38 | 33 | 43 (17–70) | 20–70 | 20–60 | |
| Marital status (married) | 12 (41%) | 23 (40%) | 21 (37%) | Mostly married | 15 (75%) | Mostly married | |
| Education | No schooling | 1 (3%) | 5 (9%) | 1 (2%) | 4 (6%) | 2 (10%) | - |
| >Junior high school | 28 (97%) | 52 (91%) | 56 (98%) | 61 (94%) | 18 (90%) | 30 (70%) | |
| >College/University | - | - | - | - | - | 13 (30%) | |
| Pre | Post | Difference | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Median | IRQ | N | Median | IRQ | N | Mean | 95% CI | ||
| SED participants | 26 | 750 | 500 | 29 | 1000 | 750 | 26 | 554 | 99 | 1009 |
| Contact/counselling area | 47 | 600 | 700 | 57 | 1125 | 1000 | 47 | 175 | −539 | 888 |
| Control | 50 | 650 | 500 | 57 | 1000 | 600 | 50 | 363 | 145 | 580 |
| n | Pre | Post | Difference | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | CI 95% | Mean | CI 95% | Mean | CI 95% | p-Value 1 | ||||||
| SSS | SED participants | 29 | 19.03 | 14.05 | 24.02 | 10.59 | 5.95 | 15.23 | −8.45 | −13.94 | −2.96 | 0.0038 |
| Contact-counselling | 57 | 17.30 | 13.90 | 20.69 | 10.75 | 8.19 | 13.31 | −6.54 | −9.60 | −3.48 | 0.0001 | |
| Control | 57 | 15.42 | 12.47 | 18.37 | 9.79 | 6.88 | 12.70 | −5.63 | −8.92 | −2.34 | 0.0011 | |
| PSS | SED participants | 29 | 8.44 | 4.34 | 12.55 | 4.89 | 1.46 | 8.32 | −3.56 | −6.07 | −1.04 | 0.0074 |
| Contact-counselling | 57 | 6.41 | 4.51 | 8.31 | 3.59 | 1.76 | 5.42 | −2.82 | −4.85 | −0.79 | 0.0074 | |
| Control | 57 | 5.42 | 3.80 | 7.04 | 4.05 | 2.19 | 5.92 | −1.36 | −3.01 | −0.29 | 0.1044 | |
| WHO QOL- BREF | SED participants | 28 | 82.59 | 78.20 | 86.99 | 86.91 | 82.04 | 91.78 | 4.32 | −1.38 | 10.09 | 0.1302 |
| Contact-counselling | 50 | 84.16 | 81.17 | 87.14 | 88.34 | 85.05 | 91.62 | 4.18 | −0.28 | 8.07 | 0.0358 | |
| Control | 55 | 85.83 | 83.36 | 88.30 | 83.83 | 81.32 | 86.35 | −2.00 | −5.49 | 1.56 | 0.2644 | |
| Indicators | Quote | Examples of What Set Things in Motion: |
|---|---|---|
| Satisfaction with life | ‘Well, I am happy now, yeah. My husband and I earn enough [money]’. (IDI S-CS01-woman-35). | -Being able to meet daily needs -Knowing and sharing correct medical information about leprosy |
| ‘I am very happy because I can talk to many people and tell them about the correct understanding of leprosy—that it is curable and cannot infect(other) easily.’ (IDI S-CS14-woman-33) | ||
| Decision-making | ‘My husband once wanted to buy something. I told him not to buy it now, because we need to buy a window for our house. When he wanted to buy a sofa because sometimes we have people coming by our house, I said to him to buy it in credit.’ (IDI S-CS11-woman-33) | -Women have more authority if they contributed to the family income |
| Health | ‘I think it is going better now. I didn’t take medication very diligently, but now I always take it. It’s like I have motivation.’ (In-depth-S-CS16-man-37) | - Increased confidence of SED clients helped them to visit the healthcare provider for advice |
| ‘I was afraid of getting infected again. But [now after visiting the doctor] I understand that once we had medication leprosy will be over. It cannot infect me again. So I am calm after I understand.’ (IDI S-CS06-woman-35) | ||
| ‘They [health providers] told me not to worry, that the disease would be cured. They counselled me by telling me that I was not the only one suffering from the disease. There were many other people who sought medication for the same disease.’ (IDI S-CS05-woman-26) | ||
| Travel and mobility | ‘Well, I used to stay at home. Then I thought that it would be better if I joined any kind of social gathering rather than staying at home.’ (IDI S-CS05-woman-26) | -Realization that clients can take action |
| ‘Yes, I was invited to become the administrator for national election booth but I gave it to my husband and I became election witness.’ (IDI S-CS06-woman-35) | ||
| Recognition and acceptance | ‘I used to get scared when having the disease. I thought nobody would be willing to buy my merchandise. It turns out that I was wrong, they still want to buy it.’ (IDI S-CT06-man-60) | -Respect because of business -Awareness of wrong assumptions |
| ‘We have two groups [for micro-credit gathering]. We were asked to move one group to another house. But they refused: “No, I don’t want. It is more enjoyable to be in this house. I don’t want to move” [house belongs to people affected by leprosy].’ (FGD 2 client SED) | ||
| ‘Yes, all my neighbours became nicer to me and respect me. ... If there is something like cake, they share it with me. They are nicer and more friendly.’ (FGD 2 client SED) | ||
| Capacity | ‘I had no ability to start anything in the past, but now I can start my small business.’ (IDI S-CT02-woman-21) | -Increased capacity (e.g., because of training) to run a business |
| ‘I used to be very down. I was very poor, I hardly had anything to eat. Now, I have built [renovated] a house in the last 2 years. My children’s school fees are paid. My economy is getting better.’ (FGD 1 Client SED) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dadun, D.; Peters, R.M.H.; van Brakel, W.H.; Bunders, J.G.F.; Irwanto, I.; Regeer, B.J. Assessing the Impact of the Twin Track Socio-Economic Intervention on Reducing Leprosy-Related Stigma in Cirebon District, Indonesia. Int. J. Environ. Res. Public Health 2019, 16, 349. https://doi.org/10.3390/ijerph16030349
Dadun D, Peters RMH, van Brakel WH, Bunders JGF, Irwanto I, Regeer BJ. Assessing the Impact of the Twin Track Socio-Economic Intervention on Reducing Leprosy-Related Stigma in Cirebon District, Indonesia. International Journal of Environmental Research and Public Health. 2019; 16(3):349. https://doi.org/10.3390/ijerph16030349
Chicago/Turabian StyleDadun, Dadun, Ruth M. H. Peters, Wim H. van Brakel, Joske G. F. Bunders, Irwanto Irwanto, and Barbara J. Regeer. 2019. "Assessing the Impact of the Twin Track Socio-Economic Intervention on Reducing Leprosy-Related Stigma in Cirebon District, Indonesia" International Journal of Environmental Research and Public Health 16, no. 3: 349. https://doi.org/10.3390/ijerph16030349
APA StyleDadun, D., Peters, R. M. H., van Brakel, W. H., Bunders, J. G. F., Irwanto, I., & Regeer, B. J. (2019). Assessing the Impact of the Twin Track Socio-Economic Intervention on Reducing Leprosy-Related Stigma in Cirebon District, Indonesia. International Journal of Environmental Research and Public Health, 16(3), 349. https://doi.org/10.3390/ijerph16030349