Prevalence and Sources of Second-Hand Smoking Exposure among Non-Smoking Pregnant Women in an Urban Setting of Vietnam

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Designs
2.2. Measurements
2.3. Statistical Analysis
2.4. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lieberman, E.; Gremy, I.; Lang, J.M.; Cohen, A.P. Low birthweight at term and the timing of fetal exposure to maternal smoking. Am. J. Public Health 1994, 84, 1127–1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aagaard-Tillery, K.M.; Porter, T.F.; Lane, R.H.; Varner, M.W.; Lacoursiere, D.Y. In utero tobacco exposure is associated with modified effects of maternal factors on fetal growth. Am. J. Obs. Gynecol. 2008, 198, 66.e1–66.e6. [Google Scholar] [CrossRef] [PubMed]
- Marufu, T.C.; Ahankari, A.; Coleman, T.; Lewis, S. Maternal smoking and the risk of still birth: Systematic review and meta-analysis. BMC Public Health 2015, 15, 239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harger, J.H.; Hsing, A.W.; Tuomala, R.E.; Gibbs, R.S.; Mead, P.B.; Eschenbach, D.A.; Knox, G.E.; Polk, B.F. Risk factors for preterm premature rupture of fetal membranes: A multicenter case-control study. Am. J. Obs. Gynecol. 1990, 163, 130–137. [Google Scholar] [CrossRef]
- Wijs, L.A.; Graaff, E.C.; Leemaqz, S.; Dekker, G. Causes of stillbirth in a socioeconomically disadvantaged urban Australian population—A comprehensive analysis. J. Matern. Fetal Neonatal Med. 2017, 30, 2851–2857. [Google Scholar] [CrossRef] [PubMed]
- Raymond, E.G.; Mills, J.L. Placental abruption. Maternal risk factors and associated fetal conditions. Acta Obs. Gynecol. Scand. 1993, 72, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Chelmow, D.; Andrew, D.E.; Baker, E.R. Maternal cigarette smoking and placenta previa. Obs. Gynecol. 1996, 87, 703–706. [Google Scholar] [CrossRef]
- Wang, L.; Yang, Y.; Liu, F.; Yang, A.; Xu, Q.; Wang, Q.; Shen, H.; Zhang, Y.; Yan, D.; Peng, Z.; et al. Paternal smoking and spontaneous abortion: A population-based retrospective cohort study among non-smoking women aged 20-49 years in rural China. J. Epidemiol. Community Health 2018, 72, 783–789. [Google Scholar] [CrossRef]
- Leonardi-Bee, J.; Britton, J.; Venn, A. Secondhand smoke and adverse fetal outcomes in nonsmoking pregnant women: A meta-analysis. Pediatrics 2011, 127, 734–741. [Google Scholar] [CrossRef] [Green Version]
- Crane, J.M.; Keough, M.; Murphy, P.; Burrage, L.; Hutchens, D. Effects of environmental tobacco smoke on perinatal outcomes: A retrospective cohort study. BJOG 2011, 118, 865–871. [Google Scholar] [CrossRef]
- Salmasi, G.; Grady, R.; Jones, J.; McDonald, S.D. Knowledge Synthesis Group Environmental tobacco smoke exposure and perinatal outcomes: A systematic review and meta-analyses. Acta Obs. Gynecol. Scand. 2010, 89, 423–441. [Google Scholar] [CrossRef] [PubMed]
- Moritsugu; Kenneth, P. A Report of the Surgeon General. In The Health Consequences of Involuntary Exposure to Tobacco Smoke; Atlanta (GA): Centers for Disease Control and Prevention (US): Atlanta, GA, USA, 2006. [Google Scholar]
- Huang, J.; Wen, G.; Yang, W.; Yao, Z.; Wu, C.; Ye, X. The association between second-hand smoke exposure and depressive symptoms among pregnant women. Psychiatry Res. 2017, 256, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Vardavas, C.I.; Patelarou, E.; Chatzi, L.; Roumeliotaki, T.; Sarri, K.; Murphy, S.; Koutis, A.; Kafatos, A.G.; Kogevinas, M. Factors associated with active smoking, quitting, and secondhand smoke exposure among pregnant women in Greece. J. Epidemiol. 2010, 20, 355–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishnamurthy, A.V.; Chinnakali, P.; Dorairajan, G.; Sundaram, S.P.; Sarveswaran, G.; Sivakumar, M.; Krishnamoorthy, K.; Dayalane, H.; Sinouvassan, V. Tobacco use, exposure to second-hand smoke among pregnant women and their association with birth weight: A retrospective cohort study. J. Fam. Med. Prim. Care 2018, 7, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Malhotra, A.K.; Verma, S.K.; Deka, M.; Yadav, R.; Singh, S. Effects of passive smoking (environmental tobacco smoke) on pregnancy outcome at district hospital, Jhansi, Uttar Pradesh. Int. J. Med. Sci. Public Health 2015, 4. [Google Scholar] [CrossRef] [Green Version]
- Mojibyan, M.; Karimi, M.; Bidaki, R.; Rafiee, P.; Zare, A. Exposure to Second-hand Smoke During Pregnancy and Preterm Delivery. Int. J. High. Risk. Behav. Addict. 2013, 1, 149–153. [Google Scholar] [CrossRef] [Green Version]
- Pizacani, B.A.; Martin, D.P.; Stark, M.J.; Koepsell, T.D.; Thompson, B.; Diehr, P. Household smoking bans: Which households have them and do they work? Prev. Med. 2003, 36, 99–107. [Google Scholar] [CrossRef]
- Arnold, C.L.; Davis, T.C.; Berkel, H.J.; Jackson, R.H.; Nandy, I.; London, S. Smoking status, reading level, and knowledge of tobacco effects among low-income pregnant women. Prev. Med. 2001, 32, 313–320. [Google Scholar] [CrossRef]
- Loke, A.Y.; Lam, T.H. A randomized controlled trial of the simple advice given by obstetricians in Guangzhou, China, to non-smoking pregnant women to help their husbands quit smoking. Patient Educ. Couns. 2005, 59, 31–37. [Google Scholar] [CrossRef]
- Huang, C.M.; Wu, H.L.; Huang, S.H.; Chien, L.Y.; Guo, J.L. Transtheoretical model-based passive smoking prevention programme among pregnant women and mothers of young children. Eur. J. Public Health 2013, 23, 777–782. [Google Scholar] [CrossRef] [Green Version]
- El-Mohandes, A.A.; Kiely, M.; Blake, S.M.; Gantz, M.G.; El-Khorazaty, M.N. An intervention to reduce environmental tobacco smoke exposure improves pregnancy outcomes. Pediatrics 2010, 125, 721–728. [Google Scholar] [CrossRef] [Green Version]
- Nichter, M.; Greaves, L.; Bloch, M.; Paglia, M.; Scarinci, I.; Tolosa, J.E.; Novotny, T.E. Tobacco use and secondhand smoke exposure during pregnancy in low- and middle-income countries: The need for social and cultural research. Acta Obs. Gynecol. Scand. 2010, 89, 465–477. [Google Scholar] [CrossRef]
- King, B.A.; Mirza, S.A.; Babb, S.D.; Group, G.C. A cross-country comparison of secondhand smoke exposure among adults: Findings from the Global Adult Tobacco Survey (GATS). Tob. Control 2013, 22, e5. [Google Scholar] [CrossRef]
- Shafey, O.; Eriksen, M.; Ross, H.; Mackay, J. The Tobacco Atlas, 3rd ed.; The American Cancer Society: Atlanta, GA, USA, 2009. [Google Scholar]
- Centers for Disease Control and Prevention. Current tobacco use and secondhand smoke exposure among women of reproductive age—14 countries, 2008–2010. Mmwr. Morb. Mortal. Wkly. Rep. 2012, 61, 877–882. [Google Scholar]
- Liu, W.; Huang, C.; Cai, J.; Wang, X.; Zou, Z.; Sun, C. Household environmental exposures during gestation and birth outcomes: A cross-sectional study in Shanghai, China. Sci. Total Environ. 2018, 615, 1110–1118. [Google Scholar] [CrossRef]
- Steve Robertson, R.W. Masculinities, men and public health policy. Int. J. Interdiscip. Soc. Sci. 2007, 2, 361–368. [Google Scholar] [CrossRef]
- Morrow, M.; Barraclough, S. Gender equity and tobacco control: Bringing masculinity into focus. Glob. Health Promot. 2010, 17, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Azagba, S. Effect of smoke-free patio policy of restaurants and bars on exposure to second-hand smoke. Prev. Med. 2015, 76, 74–78. [Google Scholar] [CrossRef] [Green Version]
- Buettner-Schmidt, K.; Boursaw, B.; Lobo, M.L.; Travers, M.J. Tobacco Smoke Pollution in Hospitality Venues Before and After Passage of Statewide Smoke-Free Legislation. Public Health Nurs. 2017, 34, 166–175. [Google Scholar] [CrossRef]
- Heloma, A.; Jaakkola, M.S.; Kahkonen, E.; Reijula, K. The short-term impact of national smoke-free workplace legislation on passive smoking and tobacco use. Am. J. Public Health 2001, 91, 1416–1418. [Google Scholar] [CrossRef]
- Bauer, J.E.; Hyland, A.; Li, Q.; Steger, C.; Cummings, K.M. A longitudinal assessment of the impact of smoke-free worksite policies on tobacco use. Am. J. Public Health 2005, 95, 1024–1029. [Google Scholar] [CrossRef]
- Marcus, B.H.; Emmons, K.M.; Abrams, D.B.; Marshall, R.J.; Kane, M.; Novotny, T.E.; Etzel, R.A. Restrictive workplace smoking policies: Impact on nonsmokers’ tobacco exposure. J. Public Health Policy 1992, 13, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Huisman, M.; Kunst, A.E.; Mackenbach, J.P. Inequalities in the prevalence of smoking in the European Union: Comparing education and income. Prev. Med. 2005, 40, 756–764. [Google Scholar] [CrossRef] [PubMed]
- Giskes, K.; Kunst, A.E.; Benach, J.; Borrell, C.; Costa, G.; Dahl, E.; Dalstra, J.A.; Federico, B.; Helmert, U.; Judge, K.; et al. Trends in smoking behaviour between 1985 and 2000 in nine European countries by education. J. Epidemiol. Community Health 2005, 59, 395–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dherani, M.; Zehra, S.N.; Jackson, C.; Satyanaryana, V.; Huque, R.; Chandra, P.; Rahman, A.; Siddiqi, K. Behaviour change interventions to reduce second-hand smoke exposure at home in pregnant women—A systematic review and intervention appraisal. BMC Pregnancy Childbirth 2017, 17, 378. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Mao, Z. Intervention on the exposure to passive smoking for non-smoking pregnant women. Chin. J. Prev. Control Chronic Dis. 2010, 3, 226–228. [Google Scholar]
- Callinan, J.E.; Clarke, A.; Doherty, K.; Kelleher, C. Legislative smoking bans for reducing secondhand smoke exposure, smoking prevalence and tobacco consumption. Cochrane Database Syst. Rev. 2010. [Google Scholar] [CrossRef]
- Haw, S.J.; Gruer, L. Changes in exposure of adult non-smokers to secondhand smoke after implementation of smoke-free legislation in Scotland: National cross sectional survey. BMJ 2007, 335, 549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrelly, M.C.; Nonnemaker, J.M.; Chou, R.; Hyland, A.; Peterson, K.K.; Bauer, U.E. Changes in hospitality workers’ exposure to secondhand smoke following the implementation of New York’s smoke-free law. Tob. Control 2005, 14, 236–241. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Characteristics | n | % |
|---|---|---|
| Age group | ||
| 18–25 | 118 | 27.3 |
| 26–30 | 200 | 46.3 |
| 31–35 | 79 | 18.3 |
| >35 | 35 | 8.1 |
| Educational attainment | ||
| <High school | 16 | 3.7 |
| High school | 72 | 16.7 |
| >High school | 344 | 79.6 |
| Occupation | ||
| Self-employed | 120 | 27.8 |
| Employed | 262 | 60.7 |
| Unemployed/Housewife | 50 | 11.6 |
| Living area | ||
| Urban | 372 | 86.1 |
| Rural | 60 | 13.9 |
| Gestation week | ||
| <30 weeks | 163 | 37.7 |
| 30–37 weeks | 200 | 46.3 |
| >37 weeks | 69 | 16.0 |
| Ever heard about second-hand smoking | 281 | 65.1 |
| Smoking is allowed at home | 179 | 41.4 |
| Characteristics | Lifetime Second-Hand Smoking Exposure | 30-Days Second-Hand Smoking Exposure | ||||
|---|---|---|---|---|---|---|
| n | % | p-Value | n | % | p-Value | |
| Age group | ||||||
| 18–25 | 112 | 94.9 | 0.41 | 76 | 67.9 | 0.07 |
| 26–30 | 186 | 93.0 | 111 | 59.7 | ||
| 31–35 | 70 | 88.6 | 53 | 75.7 | ||
| >35 | 32 | 91.4 | 18 | 56.3 | ||
| Educational attainment | ||||||
| <High school | 12 | 75.0 | 0.02 | 6 | 50.0 | 0.41 |
| High school | 68 | 94.4 | 47 | 69.1 | ||
| >High school | 320 | 93.0 | 205 | 64.1 | ||
| Occupation | ||||||
| Self-employed | 110 | 91.7 | 0.87 | 71 | 64.6 | 0.74 |
| Employed | 244 | 93.1 | 155 | 63.5 | ||
| Unemployed/Housewife | 46 | 92.0 | 32 | 69.6 | ||
| Living area | ||||||
| Urban | 345 | 92.7 | 0.77 | 221 | 64.1 | 0.64 |
| Rural | 55 | 91.7 | 37 | 67.3 | ||
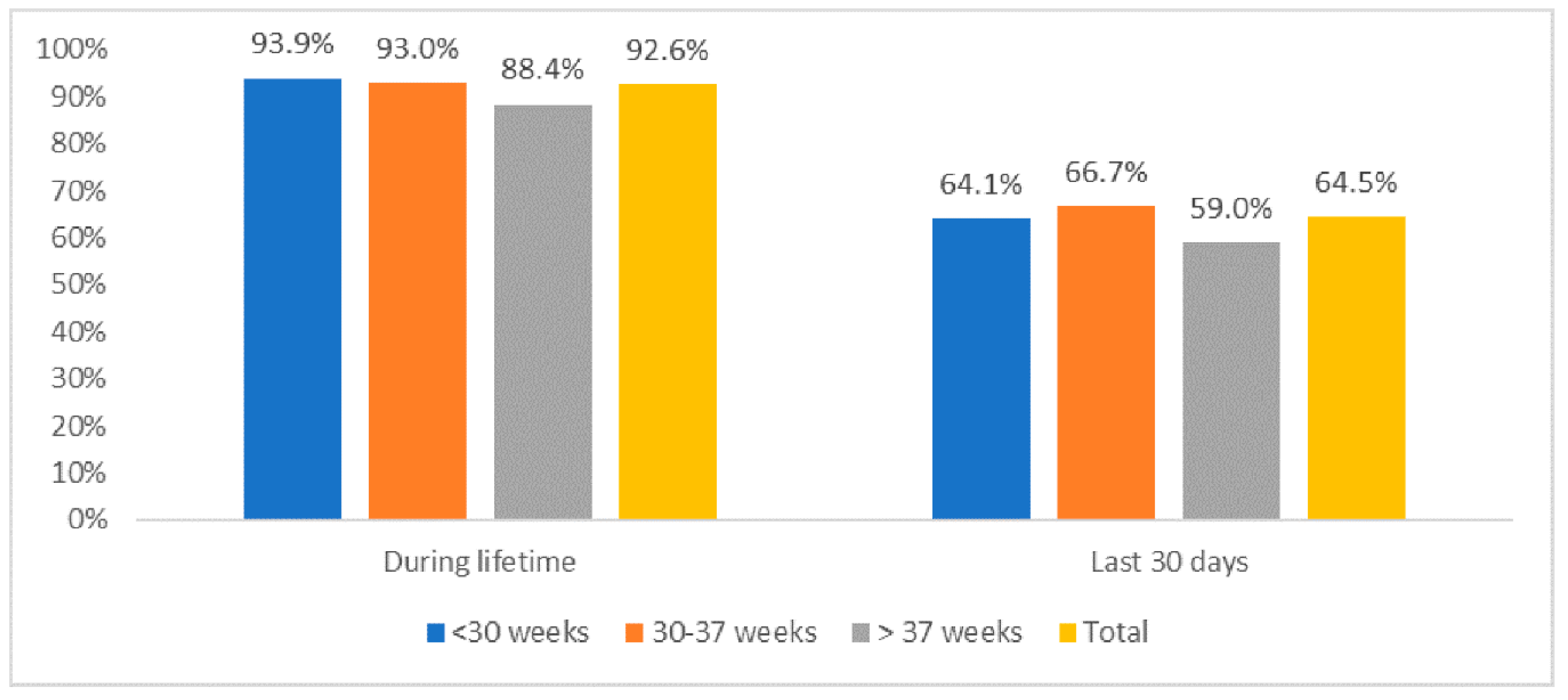
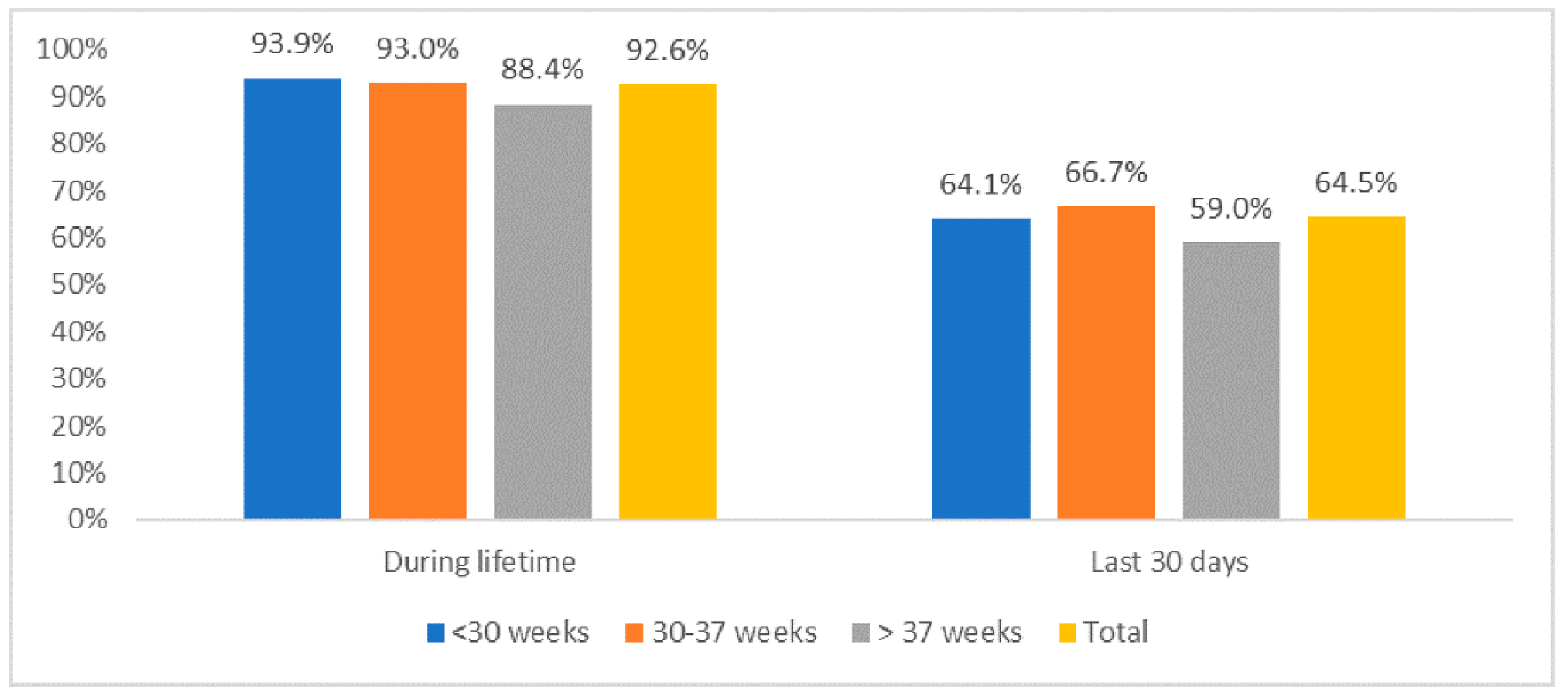
| Gestation week | ||||||
| <30 weeks | 153 | 93.9 | 0.33 | 98 | 64.1 | 0.55 |
| 30–37 weeks | 186 | 93.0 | 124 | 66.7 | ||
| >37 weeks | 61 | 88.4 | 36 | 59.0 | ||
| Characteristics | Odds Ratio (OR) 1 | p-Value | 95% Confident Interval (CI) | |
|---|---|---|---|---|
| Age group (vs. 18–25) | ||||
| 26–30 | 0.69 | 0.18 | 0.40 | 1.18 |
| 31–35 | 1.82 | 0.11 | 0.88 | 3.76 |
| >35 | 0.52 | 0.14 | 0.21 | 1.24 |
| Smoking is allowed at home (Yes vs. No) | 3.18 | <0.01 | 1.97 | 5.13 |
| Going to working place in the last 30 days (Yes vs. No) | 1.86 | 0.03 | 1.08 | 3.19 |
| Going to any State authority offices in the last 30 days (Yes vs. No) | 1.98 | 0.01 | 1.15 | 3.41 |
| Going to any cafeterias in the last 30 days (Yes vs. No) | 1.96 | 0.01 | 1.22 | 3.16 |
| Going to any health facilities in the last 30 days (Yes vs. No) | 9.02 | 0.07 | 0.87 | 93.09 |
| Ever heard about second-hand smoking (Yes vs. No) | 1.41 | 0.17 | 0.86 | 2.31 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ngo, C.Q.; Phan, P.T.; Vu, G.V.; Chu, H.T.; Nguyen, T.T.; Nguyen, M.H.; Phan, H.T.; Ong, B.M.Y.; Vu, G.T.; Pham, K.T.H.; et al. Prevalence and Sources of Second-Hand Smoking Exposure among Non-Smoking Pregnant Women in an Urban Setting of Vietnam. Int. J. Environ. Res. Public Health 2019, 16, 5022. https://doi.org/10.3390/ijerph16245022
Ngo CQ, Phan PT, Vu GV, Chu HT, Nguyen TT, Nguyen MH, Phan HT, Ong BMY, Vu GT, Pham KTH, et al. Prevalence and Sources of Second-Hand Smoking Exposure among Non-Smoking Pregnant Women in an Urban Setting of Vietnam. International Journal of Environmental Research and Public Health. 2019; 16(24):5022. https://doi.org/10.3390/ijerph16245022
Chicago/Turabian StyleNgo, Chau Quy, Phuong Thu Phan, Giap Van Vu, Hanh Thi Chu, Toan Thi Nguyen, Mai Hong Nguyen, Hai Thanh Phan, Benjamin M. Y. Ong, Giang Thu Vu, Kiet Tuan Huy Pham, and et al. 2019. "Prevalence and Sources of Second-Hand Smoking Exposure among Non-Smoking Pregnant Women in an Urban Setting of Vietnam" International Journal of Environmental Research and Public Health 16, no. 24: 5022. https://doi.org/10.3390/ijerph16245022
APA StyleNgo, C. Q., Phan, P. T., Vu, G. V., Chu, H. T., Nguyen, T. T., Nguyen, M. H., Phan, H. T., Ong, B. M. Y., Vu, G. T., Pham, K. T. H., Tran, B. X., Latkin, C. A., Ho, C. S. H., & Ho, R. C. M. (2019). Prevalence and Sources of Second-Hand Smoking Exposure among Non-Smoking Pregnant Women in an Urban Setting of Vietnam. International Journal of Environmental Research and Public Health, 16(24), 5022. https://doi.org/10.3390/ijerph16245022