Global Lifetime and 12-Month Prevalence of Suicidal Behavior, Deliberate Self-Harm and Non-Suicidal Self-Injury in Children and Adolescents between 1989 and 2018: A Meta-Analysis

 , , and
, , and 
Abstract
1. Introduction
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
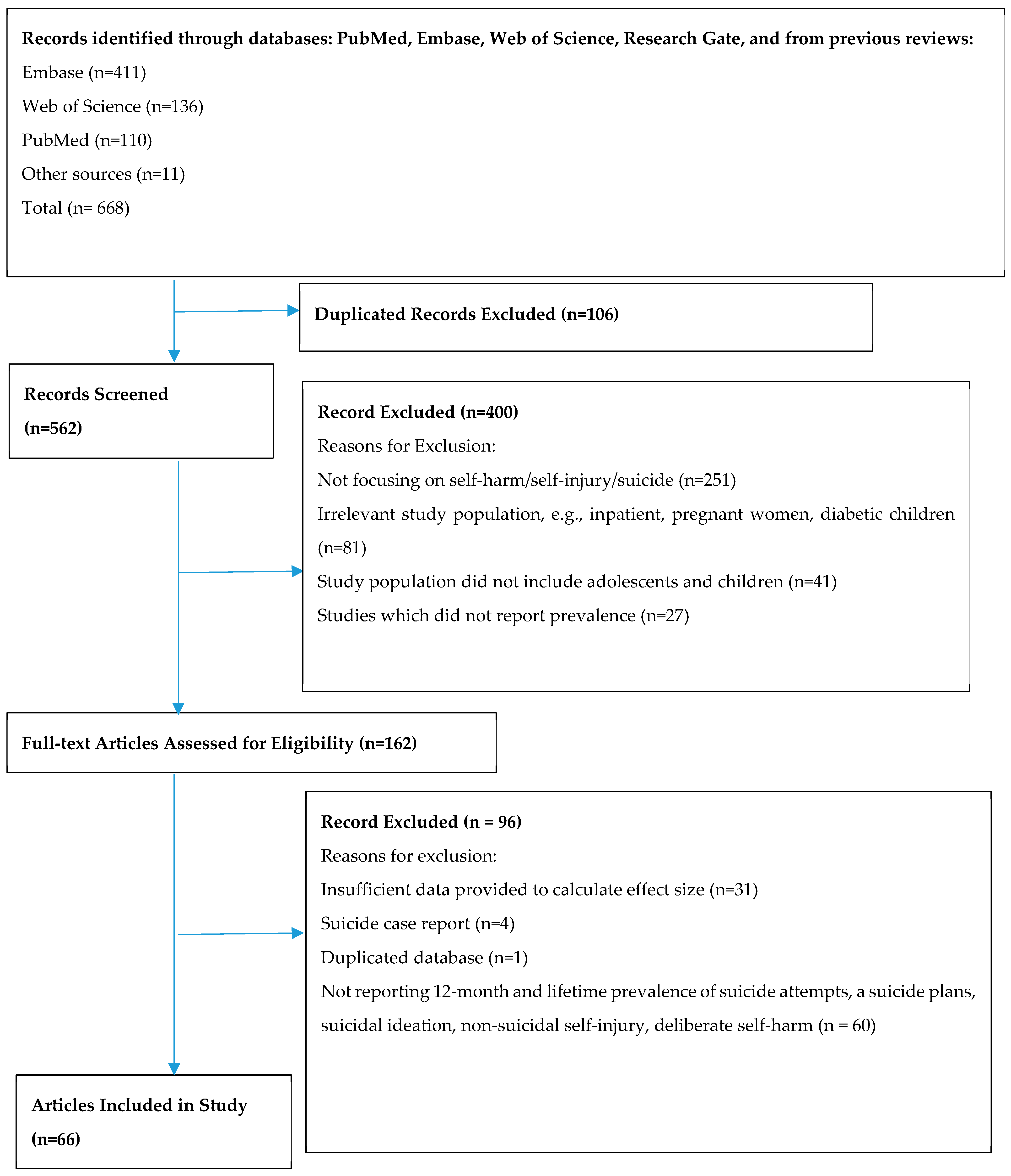
3.1. Selection Results and Study Characteristics
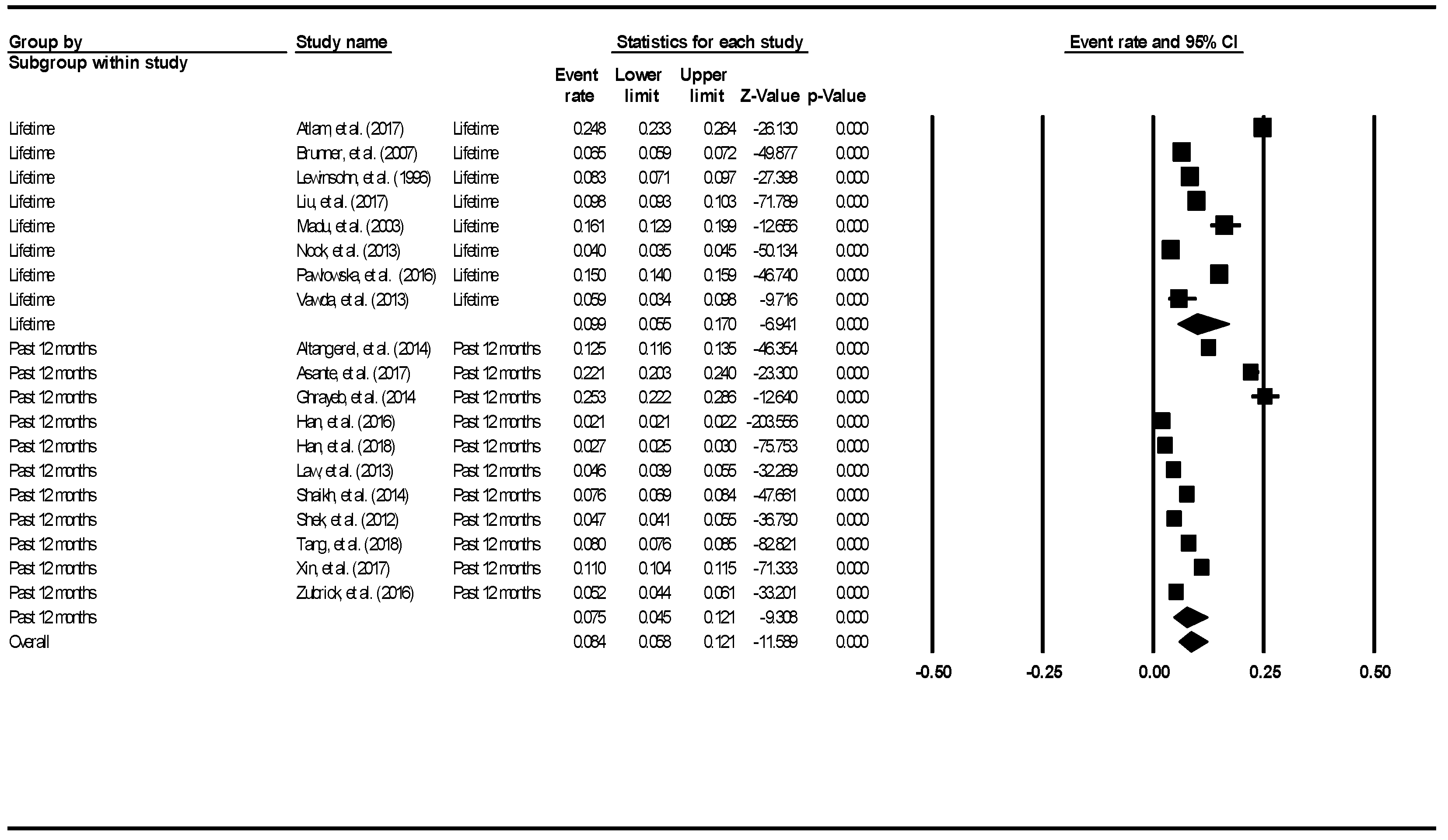
3.2. Aggregate Prevalence of Suicide Attempts in Children and Adolescents
3.3. Aggregate Prevalence of Suicide Plans in Children and Adolescents
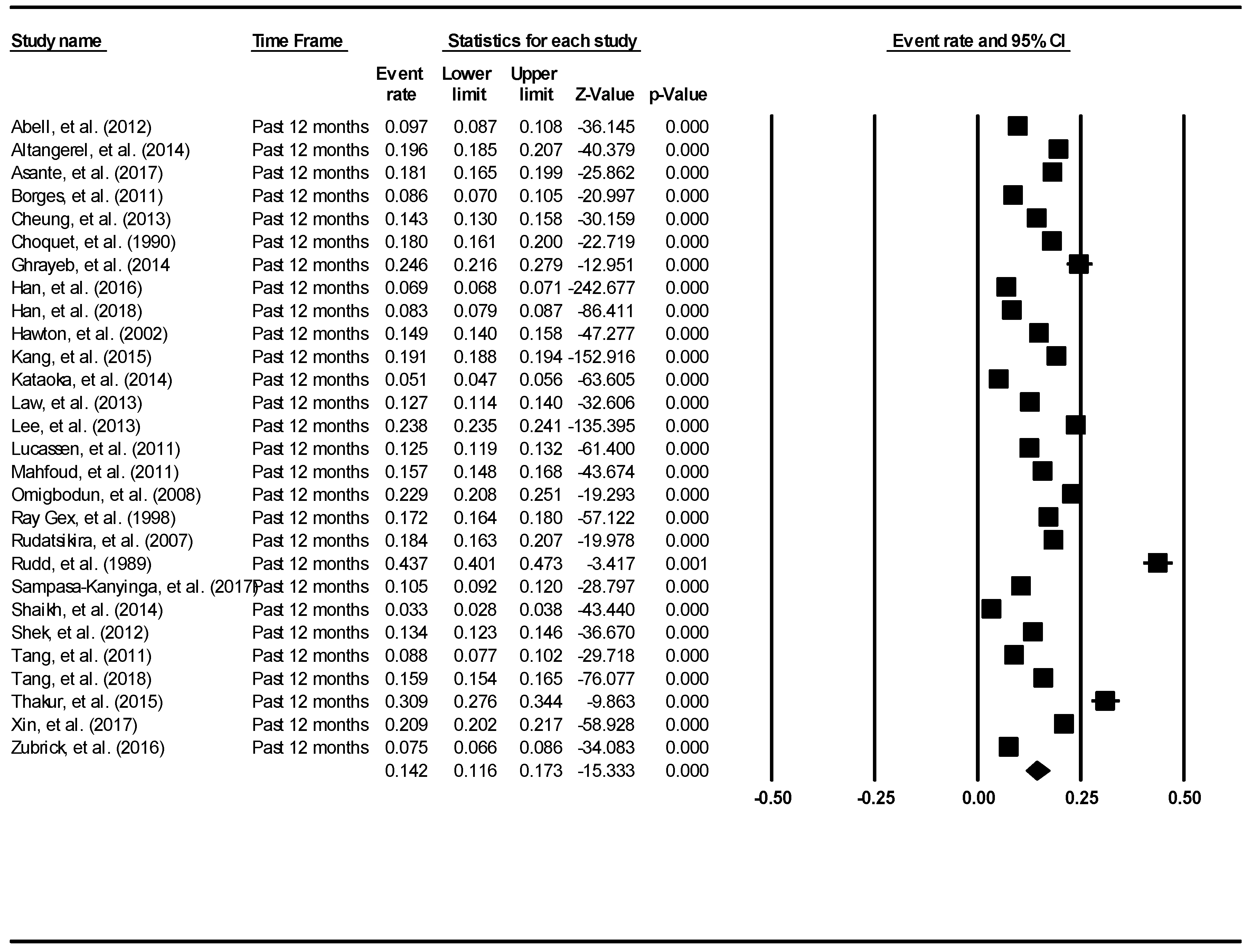
3.4. Aggregate Prevalence of Suicide Ideation in Children and Adolescents
3.5. Aggregate prevalence of Non-Suicidal Self Injury in Children and Adolescents
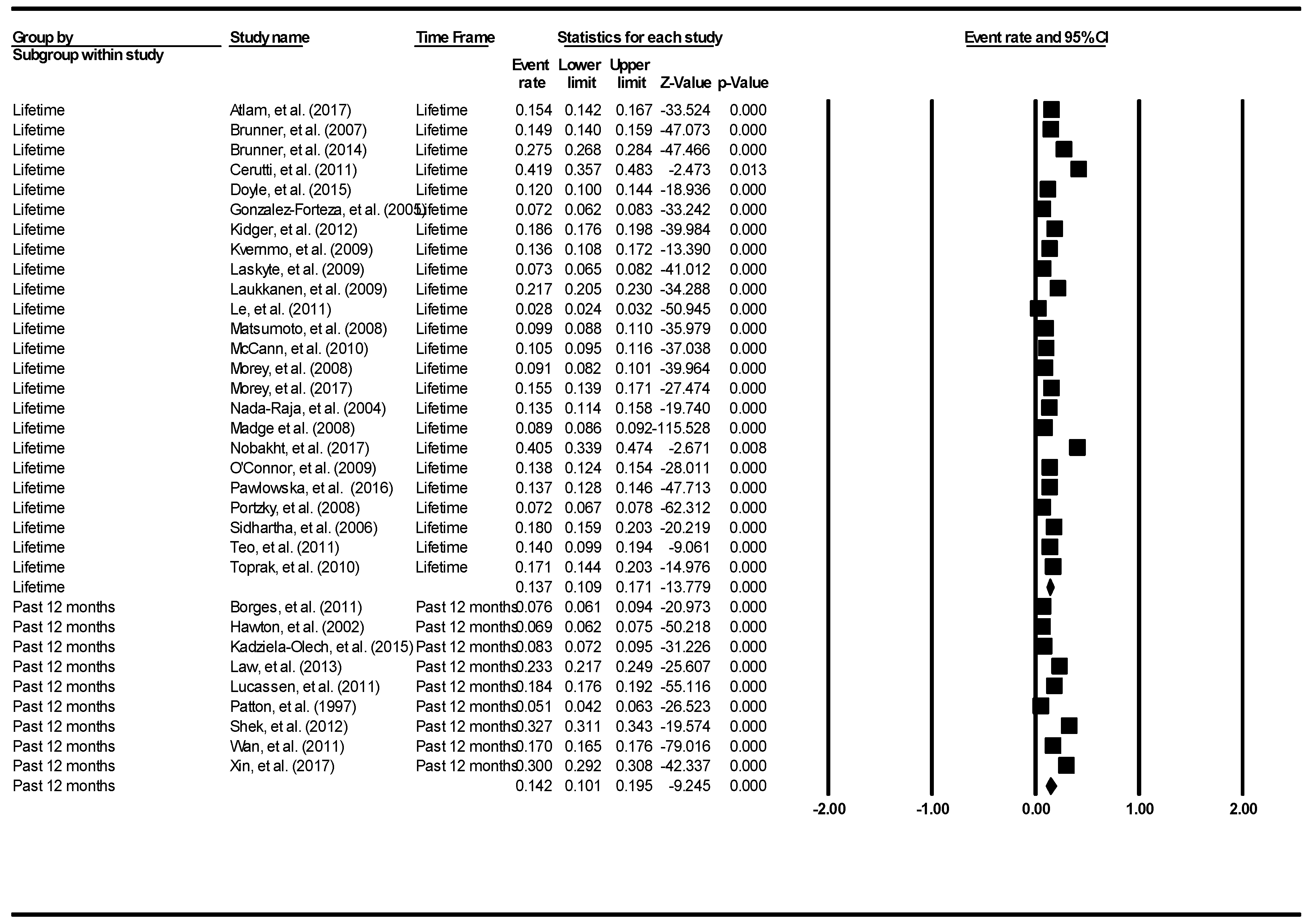
3.6. Aggregate Prevalence of Deliberate Self-Harm in Children and Adolescents
3.7. Subgroup Analyses Based on School Attendance
3.8. Subgroup Analyses Based on Western and Non-Western Countries
3.9. Subgroup Analyses Based on Developing and Developed Countries
3.10. Subgroup Analyses Based on Continents
3.11. Meta-Regression Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Suicide Rates 2017. Available online: http://www.who.int/gho/mental_health/suicide_rates/en/ (accessed on 26 April 2019).
- Aggarwal, S.; Patton, G.; Reavley, N.; Sreenivasan, S.A.; Berk, M. Youth self-harm in low-and middle-income countries: Systematic review of the risk and protective factors. Int. J. Soc. Psychiatry 2017, 63, 359–375. [Google Scholar] [CrossRef]
- Ho, C.S.; Ong, Y.L.; Tan, G.H.; Yeo, S.N.; Ho, R.C. Profile differences between overdose and non-overdose suicide attempts in a multi-ethnic Asian society. BMC Psychiatry 2016, 16, 379. [Google Scholar] [CrossRef]
- Whitlock, J.; Muehlenkamp, J.; Eckenrode, J.; Purington, A.; Baral Abrams, G.; Barreira, P.; Kress, V. Nonsuicidal self-injury as a gateway to suicide in young adults. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2013, 52, 486–492. [Google Scholar] [CrossRef]
- Madge, N.; Hewitt, A.; Hawton, K.; de Wilde, E.J.; Corcoran, P.; Fekete, S.; van Heeringen, K.; De Leo, D.; Ystgaard, M. Deliberate self-harm within an international community sample of young people: Comparative findings from the Child & Adolescent Self-harm in Europe (CASE) Study. J. Child Psychol. Psychiatry Allied Discip. 2008, 49, 667–677. [Google Scholar] [CrossRef]
- Choo, C.; Diederich, J.; Song, I.; Ho, R. Cluster analysis reveals risk factors for repeated suicide attempts in a multi-ethnic Asian population. Asian J. Psychiatry 2014, 8, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, P.; Kelvin, R.; Roberts, C.; Dubicka, B.; Goodyer, I. Clinical and psychosocial predictors of suicide attempts and nonsuicidal self-injury in the Adolescent Depression Antidepressants and Psychotherapy Trial (ADAPT). Am. J. Psychiatry 2011, 168, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Mak, K.K.; Ho, C.S.; Chua, V.; Ho, R.C. Ethnic differences in suicide behavior in Singapore. Transcult. Psychiatry 2015, 52, 3–17. [Google Scholar] [CrossRef]
- Choo, C.C.; Ho, R.C.; Burton, A.A.D. Thematic Analysis of Medical Notes Offers Preliminary Insight into Precipitants for Asian Suicide Attempters: An Exploratory Study. Int. J. Environ. Res. Public Health 2018, 15, 809. [Google Scholar] [CrossRef]
- Skinner, R.; McFaull, S. Suicide among children and adolescents in Canada: Trends and sex differences, 1980-2008. CMAJ 2012, 184, 1029–1034. [Google Scholar] [CrossRef]
- Beautrais, A.L.; Joyce, P.R.; Mulder, R.T. Youth suicide attempts: A social and demographic profile. Aust. N. Z. J. Psychiatry 1998, 32, 349–357. [Google Scholar] [CrossRef]
- Choo, C.C.; Chew, P.K.H.; Ho, R.C. Suicide Precipitants Differ Across the Lifespan but Are Not Significant in Predicting Medically Severe Attempts. Int. J. Environ. Res. Public Health 2018, 15, 691. [Google Scholar] [CrossRef] [PubMed]
- Law, B.M.; Shek, D.T. Self-harm and suicide attempts among young Chinese adolescents in Hong Kong: Prevalence, correlates, and changes. J. Pediatric Adolesc. Gynecol. 2013, 26, S26–S32. [Google Scholar] [CrossRef] [PubMed]
- Lewinsohn, P.M.; Rohde, P.; Seeley, J.R.; Baldwin, C.L. Gender differences in suicide attempts from adolescence to young adulthood. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Choo, C.C.; Harris, K.M.; Ho, R.C. Prediction of Lethality in Suicide Attempts: Gender Matters. OMEGA 2017. [Google Scholar] [CrossRef] [PubMed]
- Walsh, E.; Eggert, L.L. Suicide risk and protective factors among youth experiencing school difficulties. Int. J. Ment. Health Nurs. 2007, 16, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Do, T.T.T.; Le, M.D.; Van Nguyen, T.; Tran, B.X.; Le, H.T.; Nguyen, H.D.; Nguyen, L.H.; Nguyen, C.T.; Tran, T.D.; Latkin, C.A.; et al. Receptiveness and preferences of health-related smartphone applications among Vietnamese youth and young adults. BMC Public Health 2018, 18, 764. [Google Scholar] [CrossRef]
- Robertson, L.; Skegg, K.; Poore, M.; Williams, S.; Taylor, B. An adolescent suicide cluster and the possible role of electronic communication technology. Crisis 2012, 33, 239–245. [Google Scholar] [CrossRef]
- Luxton, D.D.; June, J.D.; Fairall, J.M. Social media and suicide: A public health perspective. Am. J. Public Health 2012, 102 (Suppl. 2), S195–S200. [Google Scholar] [CrossRef]
- Puri, B.; Hall, A.; Ho, R. Revision Notes in Psychiatry, 3rd ed.; CRC Press: New York, NY, USA, 2013. [Google Scholar]
- Silverman, M.M.; Berman, A.L.; Sanddal, N.D.; O’Carroll, P.W.; Joiner, T.E. Rebuilding the tower of Babel: A revised nomenclature for the study of suicide and suicidal behaviors. Part 2: Suicide-related ideations, communications, and behaviors. Suicide Life Threat. Behav. 2007, 37, 264–277. [Google Scholar] [CrossRef]
- O’Carroll, P.W.; Berman, A.L.; Maris, R.W.; Moscicki, E.K.; Tanney, B.L.; Silverman, M.M. Beyond the Tower of Babel: A nomenclature for suicidology. Suicide Life Threat. Behav. 1996, 26, 237–252. [Google Scholar]
- International Soceity for the Study of Self-Injury. Available online: http://www.itriples.org/isss-aboutself-i.html (accessed on 29 April 2019).
- Cheung, M.W.; Ho, R.C.; Lim, Y.; Mak, A. Conducting a meta-analysis: Basics and good practices. Int. J. Rheum. Dis. 2012, 15, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Ho, R.C.; Ong, H.S.; Kudva, K.G.; Cheung, M.W.; Mak, A. How to critically appraise and apply meta-analyses in clinical practice. Int. J. Rheum. Dis. 2010, 13, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Lim, G.Y.; Tam, W.W.; Lu, Y.; Ho, C.S.; Zhang, M.W.; Ho, R.C. Prevalence of Depression in the Community from 30 Countries between 1994 and 2014. Sci. Rep. 2018, 8, 2861. [Google Scholar] [CrossRef] [PubMed]
- Abraham, N.; Buvanaswari, P.; Rathakrishnan, R.; Tran, B.X.; Thu, G.V.; Nguyen, L.H.; Ho, C.S.; Ho, R.C. A Meta-Analysis of the Rates of Suicide Ideation, Attempts and Deaths in People with Epilepsy. Int. J. Environ. Res. Public Health 2019, 16, 1451. [Google Scholar] [CrossRef]
- Foo, S.Q.; Tam, W.W.; Ho, C.S.; Tran, B.X.; Nguyen, L.H.; McIntyre, R.S.; Ho, R.C. Prevalence of Depression among Migrants: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 1986. [Google Scholar] [CrossRef]
- Lim, R.B.C.; Zhang, M.W.B.; Ho, R.C.M. Prevalence of All-Cause Mortality and Suicide among Bariatric Surgery Cohorts: A Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 1519. [Google Scholar] [CrossRef]
- Ng, A.; Tam, W.W.; Zhang, M.W.; Ho, C.S.; Husain, S.F.; McIntyre, R.S.; Ho, R.C. IL-1beta, IL-6, TNF-alpha and CRP in Elderly Patients with Depression or Alzheimer’s disease: Systematic Review and Meta-Analysis. Sci. Rep. 2018, 8, 12050. [Google Scholar] [CrossRef]
- Liang, E.F.; Lim, S.Z.; Tam, W.W.; Ho, C.S.; Zhang, M.W.; McIntyre, R.S.; Ho, R.C. The Effect of Methylphenidate and Atomoxetine on Heart Rate and Systolic Blood Pressure in Young People and Adults with Attention-Deficit Hyperactivity Disorder (ADHD): Systematic Review, Meta-Analysis, and Meta-Regression. Int. J. Environ. Res. Public Health 2018, 15, 1789. [Google Scholar] [CrossRef]
- United Nation. Available online: https://unstats.un.org/unsd/methodology/m49/overview/ (accessed on 26 April 2019).
- Abell, W.D.; Sewell, C.; Martin, J.S.; Bailey-Davidson, Y.; Fox, K. Suicide ideation in Jamaican youth: Sociodemographic prevalence, protective and risk factors. West Indian Med. J. 2012, 61, 521–525. [Google Scholar] [CrossRef]
- Altangerel, U.; Liou, J.C.; Yeh, P.M. Prevalence and predictors of suicidal behavior among Mongolian high school students. Community Ment. Health J. 2014, 50, 362–372. [Google Scholar] [CrossRef]
- Oppong Asante, K.; Meyer-Weitz, A. Prevalence and predictors of suicidal ideations and attempts among homeless children and adolescents in Ghana. J. Child Adolesc. Ment. Health 2017, 29, 27–37. [Google Scholar] [CrossRef]
- Atlam, D.H.; Altinoprak, A.E.; Adam, D. Prevalence of risky behaviors and relationship of risky behaviors with substance use among university students. J. Psychiatry Neurol. Sci. 2017, 30, 287–298. [Google Scholar]
- Baetens, I.; Claes, L.; Muehlenkamp, J.; Grietens, H.; Onghena, P. Non-suicidal and suicidal self-injurious behavior among Flemish adolescents: A web-survey. Arch. Suicide Res. Off. J. Int. Acad. Suicide Res. 2011, 15, 56–67. [Google Scholar] [CrossRef] [PubMed]
- Begum, A.; Rahman, A.K.M.F.; Rahman, A.; Soares, J.; Reza Khankeh, H.; Macassa, G. Prevalence of suicide ideation among adolescents and young adults in rural Bangladesh. Int. J. Ment. Health 2017, 46, 177–187. [Google Scholar] [CrossRef]
- Benjet, C.; Gonzalez-Herrera, I.; Castro-Silva, E.; Mendez, E.; Borges, G.; Casanova, L.; Medina-Mora, M.E. Non-suicidal self-injury in Mexican young adults: Prevalence, associations with suicidal behavior and psychiatric disorders, and DSM-5 proposed diagnostic criteria. J. Affect. Disord. 2017, 215, 1–8. [Google Scholar] [CrossRef]
- Borges, G.; Azrael, D.; Almeida, J.; Johnson, R.M.; Molnar, B.E.; Hemenway, D.; Miller, M. Immigration, suicidal ideation and deliberate self-injury in the Boston youth survey 2006. Suicide Life Threat. Behav. 2011, 41, 193–202. [Google Scholar] [CrossRef]
- Brunner, R.; Parzer, P.; Haffner, J.; Steen, R.; Roos, J.; Klett, M.; Resch, F. Prevalence and psychological correlates of occasional and repetitive deliberate self-harm in adolescents. Arch. Pediatrics Adolesc. Med. 2007, 161, 641–649. [Google Scholar] [CrossRef]
- Brunner, R.; Kaess, M.; Parzer, P.; Fischer, G.; Carli, V.; Hoven, C.W.; Wasserman, C.; Sarchiapone, M.; Resch, F.; Apter, A.; et al. Life-time prevalence and psychosocial correlates of adolescent direct self-injurious behavior: A comparative study of findings in 11 European countries. J. Child Psychol. Psychiatry Allied Discip. 2014, 55, 337–348. [Google Scholar] [CrossRef]
- Calvete, E.; Orue, I.; Aizpuru, L.; Brotherton, H. Prevalence and functions of non-suicidal self-injury in Spanish adolescents. Psicothema 2015, 27, 223–228. [Google Scholar] [CrossRef]
- Barreto Carvalho, C.; da Motta, C.; Sousa, M.; Cabral, J. Biting myself so I don’t bite the dust: Prevalence and predictors of deliberate self-harm and suicide ideation in Azorean youths. Rev. Bras. Psiquiatr. (Sao Paulo Braz. 1999) 2017, 39, 252–262. [Google Scholar] [CrossRef]
- Cerutti, R.; Manca, M.; Presaghi, F.; Gratz, K.L. Prevalence and clinical correlates of deliberate self-harm among a community sample of Italian adolescents. J. Adolesc. 2011, 34, 337–347. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.L.; Straus, M.A.; Brownridge, D.A.; Tiwari, A.; Leung, W.C. Prevalence of dating partner violence and suicidal ideation among male and female university students worldwide. J. Midwifery Women’s Health 2008, 53, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Cheung, Y.T.; Wong, P.W.; Lee, A.M.; Lam, T.H.; Fan, Y.S.; Yip, P.S. Non-suicidal self-injury and suicidal behavior: Prevalence, co-occurrence, and correlates of suicide among adolescents in Hong Kong. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 1133–1144. [Google Scholar] [CrossRef]
- Choquet, M.; Menke, H. Suicidal thoughts during early adolescence: Prevalence, associated troubles and help-seeking behavior. Acta Psychiatr. Scand. 1990, 81, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.H.; Ko, H.C.; Wu, J.Y.; Cheng, C.P. The prevalence of and psychosocial risks for suicide attempts in male and female college students in Taiwan. Suicide Life Threat. Behav. 2013, 43, 185–197. [Google Scholar] [CrossRef]
- Claes, L.; Muehlenkamp, J. The Relationship between the UPPS-P Impulsivity Dimensions and Nonsuicidal Self-Injury Characteristics in Male and Female High-School Students. Psychiatry J. 2013, 2013, 654847. [Google Scholar] [CrossRef]
- Coughlan, H.; Tiedt, L.; Clarke, M.; Kelleher, I.; Tabish, J.; Molloy, C.; Harley, M.; Cannon, M. Prevalence of DSM-IV mental disorders, deliberate self-harm and suicidal ideation in early adolescence: An Irish population-based study. J. Adolesc. 2014, 37, 1–9. [Google Scholar] [CrossRef]
- Donald, M.; Dower, J.; Lucke, J.; Raphael, B. Prevalence of adverse life events, depression and suicidal thoughts and behaviour among a community sample of young people aged 15-24 years. Aust. N. Z. J. Public Health 2001, 25, 426–432. [Google Scholar]
- Doyle, L.; Treacy, M.P.; Sheridan, A. Self-harm in young people: Prevalence, associated factors, and help-seeking in school-going adolescents. Int. J. Ment. Health Nurs. 2015, 24, 485–494. [Google Scholar] [CrossRef]
- Fleming, T.M.; Merry, S.N.; Robinson, E.M.; Denny, S.J.; Watson, P.D. Self-reported suicide attempts and associated risk and protective factors among secondary school students in New Zealand. Aust. N. Z. J. Psychiatry 2007, 41, 213–221. [Google Scholar] [CrossRef]
- Garisch, J.A.; Wilson, M.S. Prevalence, correlates, and prospective predictors of non-suicidal self-injury among New Zealand adolescents: Cross-sectional and longitudinal survey data. Child Adolesc. Psychiatry Ment. Health 2015, 9, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Ghrayeb, F.A.; Mohamed, R.A.; Ismail, I.M.; Raifai, A.A. Prevalence of Suicide Ideation and Attempt among Palestinian Adolescents: Across-Sectional Study. World J. Med. Sci. 2014, 10, 261–266. [Google Scholar]
- Giletta, M.; Scholte, R.H.; Engels, R.C.; Ciairano, S.; Prinstein, M.J. Adolescent non-suicidal self-injury: A cross-national study of community samples from Italy, the Netherlands and the United States. Psychiatry Res. 2012, 197, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Grunbaum, J.A.; Kann, L.; Kinchen, S.A.; Williams, B.; Ross, J.G.; Lowry, R.; Kolbe, L. Youth risk behavior surveillance—United States, 2001. Morb. Mortal. Wkly. Rep. Surveill. Summ. (Wash. DC 2002) 2002, 51, 1–62. [Google Scholar] [CrossRef] [PubMed]
- Han, B.; Compton, W.M.; Eisenberg, D.; Milazzo-Sayre, L.; McKeon, R.; Hughes, A. Prevalence and Mental Health Treatment of Suicidal Ideation and Behavior Among College Students Aged 18-25 Years and Their Non-College-Attending Peers in the United States. J. Clin. Psychiatry 2016, 77, 815–824. [Google Scholar] [CrossRef] [PubMed]
- Han, H.; Park, B.; Park, B.; Park, N.; Park, J.O.; Ahn, K.O.; Tak, Y.J.; Lee, H.A.; Park, H. The Pyramid of Injury: Estimation of the Scale of Adolescent Injuries According to Severity. J. Prev. Med. Public Health Yebang Uihakhoe Chi 2018, 51, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; Rodham, K.; Evans, E.; Weatherall, R. Deliberate self harm in adolescents: Self report survey in schools in England. BMJ (Clin. Res. Ed.) 2002, 325, 1207–1211. [Google Scholar] [CrossRef]
- Hesketh, T.; Ding, Q.J.; Jenkins, R. Suicide ideation in Chinese adolescents. Soc. Psychiatry Psychiatr. Epidemiol. 2002, 37, 230–235. [Google Scholar] [CrossRef]
- Kadziela-Olech, H.; Zak, G.; Kalinowska, B.; Wagrocka, A.; Perestret, G.; Bielawski, M. The prevalence of Non-suicidal Self-Injury (NSSI) among high school students in relation to age and sex. Psychiatr. Pol. 2015, 49, 765–778. [Google Scholar] [CrossRef]
- Kang, E.H.; Hyun, M.K.; Choi, S.M.; Kim, J.M.; Kim, G.M.; Woo, J.M. Twelve-month prevalence and predictors of self-reported suicidal ideation and suicide attempt among Korean adolescents in a web-based nationwide survey. Aust. N. Z. J. Psychiatry 2015, 49, 47–53. [Google Scholar] [CrossRef]
- Kataoka, C.; Nozu, Y.; Kudo, M.; Sato, Y.; Kubo, M.; Nakayama, N.; Iwata, H.; Watanabe, M. Relationships between prevalence of youth risk behaviors and sleep duration among Japanese high school students. [Nihon Koshu Eisei Zasshi] Jpn. J. Public Health 2014, 61, 535–544. [Google Scholar]
- Kidger, J.; Heron, J.; Lewis, G.; Evans, J.; Gunnell, D. Adolescent self-harm and suicidal thoughts in the ALSPAC cohort: A self-report survey in England. BMC Psychiatry 2012, 12, 69. [Google Scholar] [CrossRef] [PubMed]
- Kvernmo, S.; Rosenvinge, J.H. Self-mutilation and suicidal behaviour in Sami and Norwegian adolescents: Prevalence and correlates. Int. J. Circumpolar Health 2009, 68, 235–248. [Google Scholar] [CrossRef] [PubMed]
- Kirmayer, L.J.; Malus, M.; Boothroyd, L.J. Suicide attempts among Inuit youth: A community survey of prevalence and risk factors. Acta Psychiatr. Scand. 1996, 94, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Larsson, B.; Sund, A.M. Prevalence, course, incidence, and 1-year prediction of deliberate self-harm and suicide attempts in early Norwegian school adolescents. Suicide Life Threat. Behav. 2008, 38, 152–165. [Google Scholar] [CrossRef] [PubMed]
- Laskyte, A.; Zemaitiene, N. The types of deliberate self-harm and its prevalence among Lithuanian teenagers. Medicina 2009, 45, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Laukkanen, E.; Rissanen, M.L.; Honkalampi, K.; Kylma, J.; Tolmunen, T.; Hintikka, J. The prevalence of self-cutting and other self-harm among 13-to 18-year-old Finnish adolescents. Soc. Psychiatry Psychiatr. Epidemiol. 2009, 44, 23–28. [Google Scholar] [CrossRef]
- Le, L.C.; Blum, R.W. Intentional injury in young people in Vietnam: Prevalence and social correlates. MEDICC Rev. 2011, 13, 23–28. [Google Scholar]
- Lee, H.S.; Kim, S.; Choi, I.; Lee, K.U. Prevalence and risk factors associated with suicide ideation and attempts in korean college students. Psychiatry Investig. 2008, 5, 86–93. [Google Scholar] [CrossRef]
- Lee, C.G.; Cho, Y.; Yoo, S. The relations of suicidal ideation and attempts with physical activity among Korean adolescents. J. Phys. Act. Health 2013, 10, 716–726. [Google Scholar] [CrossRef]
- Lewinsohn, P.M.; Rohde, P.; Seeley, J.R. Adolescent Suicidal Ideation and Attempts: Prevalence, Risk Factors, and Clinical Implications. Clin. Psychol. Sci. Pract. 1996, 3, 25–46. [Google Scholar] [CrossRef]
- Lin, M.P.; You, J.; Wu, Y.W.; Jiang, Y. Depression Mediates the Relationship between Distress Tolerance and Nonsuicidal Self-Injury among Adolescents: One-Year Follow-Up. Suicide Life Threat. Behav. 2018, 48, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.Z.; Chen, H.; Bo, Q.G.; Chen, R.H.; Li, F.W.; Lv, L.; Jia, C.X.; Liu, X. Psychological and behavioral characteristics of suicide attempts and non-suicidal self-injury in Chinese adolescents. J. Affect. Disord. 2018, 226, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Lucassen, M.F.; Merry, S.N.; Robinson, E.M.; Denny, S.; Clark, T.; Ameratunga, S.; Crengle, S.; Rossen, F.V. Sexual attraction, depression, self-harm, suicidality and help-seeking behaviour in New Zealand secondary school students. Aust. N. Z. J. Psychiatry 2011, 45, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Madu, S.N.; Matla, M.P. Correlations for perceived family environmental factors with substance use among adolescents in South Africa. Psychol. Rep. 2003, 92, 403–415. [Google Scholar] [CrossRef] [PubMed]
- Mahfoud, Z.R.; Afifi, R.A.; Haddad, P.H.; Dejong, J. Prevalence and determinants of suicide ideation among Lebanese adolescents: Results of the GSHS Lebanon 2005. J. Adolesc. 2011, 34, 379–384. [Google Scholar] [CrossRef]
- Matsumoto, T.; Imamura, F.; Chiba, Y.; Katsumata, Y.; Kitani, M.; Takeshima, T. Prevalences of lifetime histories of self-cutting and suicidal ideation in Japanese adolescents: Differences by age. Psychiatry Clin. Neurosci. 2008, 62, 362–364. [Google Scholar] [CrossRef]
- McCann, M.; Schubotz, D.; McCartan, C.; McCrystall, P. 023 Prevalence of self-harm and help-seeking behaviours among young people in Northern Ireland. J. Epidemiol. Community Health 2010, 64, A9. [Google Scholar] [CrossRef][Green Version]
- Meehan, P.J.; Lamb, J.A.; Saltzman, L.E.; O’Carroll, P.W. Attempted suicide among young adults: Progress toward a meaningful estimate of prevalence. Am. J. Psychiatry 1992, 149, 41–44. [Google Scholar] [CrossRef]
- Bo, M.; Peter, C.; Annika, S. Non-Suicidal Self-Injury and Indirect Self-Harm Among Danish High School Students. Scand. J. Child Adolesc. Psychiatry Psychol. 2014, 2, 11–18. [Google Scholar]
- Mojs, E.; Warchol-Biedermann, K.; Glowacka, M.D.; Strzelecki, W.; Ziemska, B.; Marcinkowski, J.T. Are students prone to depression and suicidal thoughts? Assessment of the risk of depression in university students from rural and urban areas. Ann. Agric. Environ. Med. AAEM 2012, 19, 770–774. [Google Scholar] [PubMed]
- Morey, C.; Corcoran, P.; Arensman, E.; Perry, I.J. The prevalence of self-reported deliberate self harm in Irish adolescents. BMC Public Health 2008, 8, 79. [Google Scholar] [CrossRef] [PubMed]
- Morey, Y.; Mellon, D.; Dailami, N.; Verne, J.; Tapp, A. Adolescent self-harm in the community: An update on prevalence using a self-report survey of adolescents aged 13-18 in England. J. Public Health (Oxf. Engl.) 2017, 39, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Muehlenkamp, J.J.; Williams, K.L.; Gutierrez, P.M.; Claes, L. Rates of non-suicidal self-injury in high school students across five years. Arch. Suicide Res. Off. J. Int. Acad. Suicide Res. 2009, 13, 317–329. [Google Scholar] [CrossRef] [PubMed]
- Muehlenkamp, J.J.; Ertelt, T.W.; Miller, A.L.; Claes, L. Borderline personality symptoms differentiate non-suicidal and suicidal self-injury in ethnically diverse adolescent outpatients. J. Child Psychol. Psychiatry Allied Discip. 2011, 52, 148–155. [Google Scholar] [CrossRef]
- Nada-Raja, S.; Skegg, K.; Langley, J.; Morrison, D.; Sowerby, P. Self-harmful behaviors in a population-based sample of young adults. Suicide Life Threat. Behav. 2004, 34, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Nath, Y.; Paris, J.; Thombs, B.; Kirmayer, L. Prevalence and social determinants of suicidal behaviours among college youth in India. Int. J. Soc. Psychiatry 2012, 58, 393–399. [Google Scholar] [CrossRef]
- Nixon, M.K.; Cloutier, P.; Jansson, S.M. Nonsuicidal self-harm in youth: A population-based survey. CMAJ 2008, 178, 306–312. [Google Scholar] [CrossRef]
- Nobakht, H.N.; Dale, K.Y. The prevalence of deliberate self-harm and its relationships to trauma and dissociation among Iranian young adults. J. Trauma Dissociation Off. J. Int. Soc. Study Dissociation (ISSD) 2017, 18, 610–623. [Google Scholar] [CrossRef]
- Nock, M.K.; Green, J.G.; Hwang, I.; McLaughlin, K.A.; Sampson, N.A.; Zaslavsky, A.M.; Kessler, R.C. Prevalence, correlates, and treatment of lifetime suicidal behavior among adolescents: Results from the National Comorbidity Survey Replication Adolescent Supplement. JAMA Psychiatry 2013, 70, 300–310. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Rasmussen, S.; Miles, J.; Hawton, K. Self-harm in adolescents: Self-report survey in schools in Scotland. Br. J. Psychiatry J. Ment. Sci. 2009, 194, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Omigbodun, O.; Dogra, N.; Esan, O.; Adedokun, B. Prevalence and correlates of suicidal behaviour among adolescents in southwest Nigeria. Int. J. Soc. Psychiatry 2008, 54, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Patton, G.C.; Harris, R.; Carlin, J.B.; Hibbert, M.E.; Coffey, C.; Schwartz, M.; Bowes, G. Adolescent suicidal behaviours: A population-based study of risk. Psychol. Med. 1997, 27, 715–724. [Google Scholar] [CrossRef] [PubMed]
- Pawlowska, B.; Potembska, E.; Zygo, M.; Olajossy, M.; Dziurzynska, E. Prevalence of self-injury performed by adolescents aged 16-19 years. Psychiatr. Pol. 2016, 50, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Perez-Amezcua, B.; Rivera-Rivera, L.; Atienzo, E.E.; Castro, F.; Leyva-Lopez, A.; Chavez-Ayala, R. Prevalence and factors associated with suicidal behavior among Mexican students. Salud Publica Mex. 2010, 52, 324–333. [Google Scholar]
- Plener, P.L.; Libal, G.; Keller, F.; Fegert, J.M.; Muehlenkamp, J.J. An international comparison of adolescent non-suicidal self-injury (NSSI) and suicide attempts: Germany and the USA. Psychol. Med. 2009, 39, 1549–1558. [Google Scholar] [CrossRef]
- Portzky, G.; De Wilde, E.J.; van Heeringen, K. Deliberate self-harm in young people: Differences in prevalence and risk factors between the Netherlands and Belgium. Eur. Child Adolesc. Psychiatry 2008, 17, 179–186. [Google Scholar] [CrossRef]
- Rey Gex, C.; Narring, F.; Ferron, C.; Michaud, P.A. Suicide attempts among adolescents in Switzerland: Prevalence, associated factors and comorbidity. Acta Psychiatr. Scand. 1998, 98, 28–33. [Google Scholar] [CrossRef]
- Rudatsikira, E.; Muula, A.S.; Siziya, S. Prevalence and associated factors of suicidal ideation among school-going adolescents in Guyana: Results from a cross sectional study. Clin. Pract. Epidemiol. Ment. Health CP EMH 2007, 3, 13. [Google Scholar] [CrossRef]
- Rudd, M.D. The prevalence of suicidal ideation among college students. Suicide Life Threat. Behav. 1989, 19, 173–183. [Google Scholar] [CrossRef]
- Sampasa-Kanyinga, H.; Dupuis, L.C.; Ray, R. Prevalence and correlates of suicidal ideation and attempts among children and adolescents. Int. J. Adolesc. Med. Health 2017, 29. [Google Scholar] [CrossRef] [PubMed]
- Sarno, I.; Madeddu, F.; Gratz, K.L. Self-injury, psychiatric symptoms, and defense mechanisms: Findings in an Italian nonclinical sample. Eur. Psychiatry J. Assoc. Eur. Psychiatr. 2010, 25, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, M.A. Prevalence and correlates of suicidal expression among school attending adolescents in Pakistan. JPMA J. Pak. Med. Assoc. 2014, 64, 99–100. [Google Scholar] [PubMed]
- Shek, D.T.; Yu, L. Self-harm and suicidal behaviors in Hong Kong adolescents: Prevalence and psychosocial correlates. Sci. World J. 2012, 2012, 932540. [Google Scholar] [CrossRef] [PubMed]
- Sidhartha, T.; Jena, S. Suicidal behaviors in adolescents. Indian J. Pediatrics 2006, 73, 783–788. [Google Scholar] [CrossRef]
- Silviken, A.; Kvernmo, S. Suicide attempts among indigenous Sami adolescents and majority peers in Arctic Norway: Prevalence and associated risk factors. J. Adolesc. 2007, 30, 613–626. [Google Scholar] [CrossRef]
- Soares, M.J.; Amaral, A.; Pereira, A.T.; Madeira, N.; Bos, S.; Valente, J.; Nogueira, V.; Oliveira, L.A.; Roque, C.; Macedo, A. Prevalence of Suicidal Ideation Among Students. Eur. Psychiatry 2015, 30, 1802. [Google Scholar] [CrossRef]
- Somer, O.; Bildik, T.; Kabukcu-Basay, B.; Gungor, D.; Basay, O.; Farmer, R.F. Prevalence of non-suicidal self-injury and distinct groups of self-injurers in a community sample of adolescents. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1163–1171. [Google Scholar] [CrossRef]
- Sornberger, M.J.; Heath, N.L.; Toste, J.R.; McLouth, R. Nonsuicidal self-injury and gender: Patterns of prevalence, methods, and locations among adolescents. Suicide Life Threat. Behav. 2012, 42, 266–278. [Google Scholar] [CrossRef]
- Straub, J.; Keller, F.; Sproeber, N.; Koelch, M.G.; Plener, P.L. Suicidal behavior in german adolescents. Prevalence and association with depressive and manic symptoms. Z. Kinder Jugendpsychiatrie Psychother. 2015, 43, 39–45. [Google Scholar] [CrossRef]
- Tang, J.; Yu, Y.; Wu, Y.; Du, Y.; Ma, Y.; Zhu, H.; Zhang, P.; Liu, Z. Association between non-suicidal self-injuries and suicide attempts in Chinese adolescents and college students: A cross-section study. PLoS ONE 2011, 6, e17977. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Li, G.; Chen, B.; Huang, Z.; Zhang, Y.; Chang, H.; Wu, C.; Ma, X.; Wang, J.; Yu, Y. Prevalence of and risk factors for non-suicidal self-injury in rural China: Results from a nationwide survey in China. J. Affect. Disord. 2018, 226, 188–195. [Google Scholar] [CrossRef] [PubMed]
- YW, T. Non-Suicidal Self-injury in a Singaporean Community Adolescent Population: Prevalence and Risk Factors. Asian J. Psychiatry 2011, 4, S49–S50. [Google Scholar]
- Thakur, D.; Gupta, A.; Thakur, A.; Mazta, S.R.; Sharma, D. Prevalence and predictors of suicidal ideations among school going adolescents in a hilly state of India. Ind. Psychiatry J. 2015, 24, 140–143. [Google Scholar] [CrossRef]
- Toprak, S.; Cetin, I.; Guven, T.; Can, G.; Demircan, C. Self-harm, suicidal ideation and suicide attempts among college students. Psychiatry Res. 2011, 187, 140–144. [Google Scholar] [CrossRef]
- Tresno, F.; Ito, Y.; Mearns, J. Self-injurious behavior and suicide attempts among Indonesian college students. Death Stud. 2012, 36, 627–639. [Google Scholar] [CrossRef]
- Valdez-Santiago, R.; Solorzano, E.H.; Iniguez, M.M.; Burgos, L.A.; Gomez Hernandez, H.; Martinez Gonzalez, A. Attempted suicide among adolescents in Mexico: Prevalence and associated factors at the national level. Inj. Prev. J. Int. Soc. Child Adolesc. Inj. Prev. 2018, 24, 256–261. [Google Scholar] [CrossRef]
- Vawda, N. The prevalence of suicidal behaviour and associated risk factors in grade 8 learners in Durban. S. Afr. Fam. Pract. 2014, 56, 37–42. [Google Scholar] [CrossRef]
- Ventura-Junca, D.R.; Carvajal, C.; Undurraga, S.; Vicuna, P.; Egana, J.; Garib, M.J. Prevalence of suicidal ideations and suicidal attempts among adolescents living in Metropolitan Santiago. Rev. Med. Chile 2010, 138, 309–315. [Google Scholar]
- Wan, Y.H.; Hu, C.L.; Hao, J.H.; Sun, Y.; Tao, F.B. Deliberate self-harm behaviors in Chinese adolescents and young adults. Eur. Child Adolesc. Psychiatry 2011, 20, 517–525. [Google Scholar] [CrossRef]
- Whitlock, J.; Muehlenkamp, J.; Purington, A.; Eckenrode, J.; Barreira, P.; Baral Abrams, G.; Marchell, T.; Kress, V.; Girard, K.; Chin, C.; et al. Nonsuicidal self-injury in a college population: General trends and sex differences. J. Am. Coll. Health 2011, 59, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Xin, X.; Wang, Y.; Fang, J.; Ming, Q.; Yao, S. Prevalence and Correlates of Direct Self-Injurious Behavior among Chinese Adolescents: Findings from a Multicenter and Multistage Survey. J. Abnorm. Child Psychol. 2017, 45, 815–826. [Google Scholar] [CrossRef] [PubMed]
- Zetterqvist, M.; Lundh, L.G.; Dahlstrom, O.; Svedin, C.G. Prevalence and function of non-suicidal self-injury (NSSI) in a community sample of adolescents, using suggested DSM-5 criteria for a potential NSSI disorder. J. Abnorm. Child Psychol. 2013, 41, 759–773. [Google Scholar] [CrossRef] [PubMed]
- Zubrick, S.R.; Hafekost, J.; Johnson, S.E.; Lawrence, D.; Saw, S.; Sawyer, M.; Ainley, J.; Buckingham, W.J. Self-harm: Prevalence estimates from the second Australian Child and Adolescent Survey of Mental Health and Wellbeing. Aust. N. Z. J. Psychiatry 2016, 50, 911–921. [Google Scholar] [CrossRef] [PubMed]
- Snowdon, J. Differences between patterns of suicide in East Asia and the West. The importance of sociocultural factors. Asian J. Psychiatry 2018, 37, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Hunter, E.; Milroy, H. Aboriginal and Torres Strait Islander suicide in context. Arch. Suicide Res. Off. J. Int. Acad. Suicide Res. 2006, 10, 141–157. [Google Scholar] [CrossRef]
- Klonsky, E.D.; May, A.M.; Glenn, C.R. The relationship between nonsuicidal self-injury and attempted suicide: Converging evidence from four samples. J. Abnorm. Psychol. 2013, 122, 231–237. [Google Scholar] [CrossRef]
- Klonsky, E.D.; Victor, S.E.; Saffer, B.Y. Nonsuicidal self-injury: What we know, and what we need to know. Can. J. Psychiatry 2014, 59, 565–568. [Google Scholar] [CrossRef]
- Klonsky, E.D.; Muehlenkamp, J.J. Self-injury: A research review for the practitioner. J. Clin. Psychol. 2007, 63, 1045–1056. [Google Scholar] [CrossRef]
- Statista. Ethnic Group in Australia. Available online: https://www.statista.com/statistics/260502/ethnic-groups-in-australia/ (accessed on 26 April 2019).
- Pekrun, R.; Goetz, T.; Titz, W.; Perry, R.P. Academic Emotions in Students’ Self-Regulated Learning and Achievement: A Program of Qualitative and Quantitative Research. Educ. Psychol. 2002, 37, 91–105. [Google Scholar] [CrossRef]
- Yeo, S.K.; Lee, W.K. The relationship between adolescents’ academic stress, impulsivity, anxiety, and skin picking behavior. Asian J. Psychiatry 2017, 28, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Olweus, D. School bullying: Development and some important challenges. Annu. Rev. Clin. Psychol. 2013, 9, 751–780. [Google Scholar] [CrossRef] [PubMed]
- Prinstein, M.J.; Boergers, J.; Vernberg, E.M. Overt and relational aggression in adolescents: Social-psychological adjustment of aggressors and victims. J. Clin. Child Psychol. 2001, 30, 479–491. [Google Scholar] [CrossRef] [PubMed]
- Vergara, G.A.; Stewart, J.G.; Cosby, E.A.; Lincoln, S.H.; Auerbach, R.P. Non-Suicidal self-injury and suicide in depressed Adolescents: Impact of peer victimization and bullying. J. Affect. Disord. 2019, 245, 744–749. [Google Scholar] [CrossRef] [PubMed]
- Cluver, L.; Orkin, M.; Boyes, M.E.; Sherr, L. Child and Adolescent Suicide Attempts, Suicidal Behavior, and Adverse Childhood Experiences in South Africa: A Prospective Study. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2015, 57, 52–59. [Google Scholar] [CrossRef]
- Shaikh, M.A.; Lloyd, J.; Acquah, E.; Celedonia, K.L.; Wilson, M.L. Suicide attempts and behavioral correlates among a nationally representative sample of school-attending adolescents in the Republic of Malawi. BMC Public Health 2016, 16, 843. [Google Scholar] [CrossRef]
- Thupayagale-Tshweneagae, G.; Benedict, S. The burden of secrecy among South African adolescents orphaned By HIV and AIDS. Issues Ment. Health Nurs. 2011, 32, 355–358. [Google Scholar] [CrossRef]
- Forjuoh, S.N.; Zwi, A.B. Violence against children and adolescents. International perspectives. Pediatric Clin. North Am. 1998, 45, 415–426. [Google Scholar] [CrossRef]
- Zhang, M.W.; Ho, R.C. Enabling Psychiatrists to Explore the Full Potential of E-Health. Front. Psychiatry 2015, 6, 177. [Google Scholar] [CrossRef]
- Zhang, M.W.; Ho, R.C. Smartphone application for multi-phasic interventional trials in psychiatry: Technical design of a smart server. Technol. Health Care Off. J. Eur. Soc. Eng. Med. 2017, 25, 373–375. [Google Scholar] [CrossRef]
- Kim, Y.J.; Moon, S.S.; Lee, J.H.; Kim, J.K. Risk Factors and Mediators of Suicidal Ideation Among Korean Adolescents. Crisis 2018, 39, 4–12. [Google Scholar] [CrossRef]
- Offer, D.; Howard, K.I.; Schonert, K.A.; Ostrov, E. To whom do adolescents turn for help? Differences between disturbed and nondisturbed adolescents. J. Am. Acad. Child Adolesc. Psychiatry 1991, 30, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Groholt, B.; Ekeberg, O.; Wichstrom, L.; Haldorsen, T. Suicide among children and younger and older adolescents in Norway: A comparative study. J. Am. Acad. Child Adolesc. Psychiatry 1998, 37, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Vrshek-Schallhorn, S.; Czarlinski, J.; Mineka, S.; Zinbarg, R.E.; Craske, M. Prospective Predictors of Suicidal Ideation during Depressive Episodes among Older Adolescents and Young Adults. Personal. Individ. Differ. 2011, 50, 1202–1207. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rohde, P.; Noell, J.; Ochs, L.; Seeley, J.R. Depression, suicidal ideation and STD-related risk in homeless older adolescents. J. Adolesc. 2001, 24, 447–460. [Google Scholar] [CrossRef]
- Ang, R.P.; Ooi, Y.P. Impact of gender and parents’ marital status on adolescents’ suicidal ideation. Int. J. Soc. Psychiatry 2004, 50, 351–360. [Google Scholar] [CrossRef]
- Ang, R.P.; Chia, B.H.; Fung, D.S. Gender differences in life stressors associated with child and adolescent suicides in Singapore from 1995 to 2003. Int. J. Soc. Psychiatry 2006, 52, 561–570. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Year | Study Location | Sample Size | Mean Age | Proportion of Female Gender | Prevalence of Suicide Attempts | Prevalence of Suicide Plans | Prevalence of Suicide Ideation | Prevalence of Non-Suicidal Self-Injury | Prevalence of Deliberate Self-Harm |
|---|---|---|---|---|---|---|---|---|---|---|
| Abell [33] | 2012 | Jamaica | 2997 | NA | NA | NA | NA | 12M:0.097 | NA | NA |
| Altangerel [34] | 2014 | Mongolian | 5191 | NA | 0.567 | 12M: 0.086 | 12M:0.125 | 12M: 0.196 | NA | NA |
| Asante [35] | 2017 | Ghana | 1984 | NA | 0.458 | 12M: 0.221 | 12M:0.221 | 12M: 0.181 | NA | NA |
| Atlam [36] | 2017 | Turkey | 2973 | NA | 0.548 | NA | LT: 0.248 | NA | NA | LT: 0.154 |
| Baetens [37] | 2011 | Belgium | 1417 | 15.13 | 0.814 | NA | NA | LT: 0.605 | LT: 0.216 | NA |
| Begum [38] | 2017 | Bangladesh | 2476 | NA | NA | NA | NA | LT:0.05 | NA | NA |
| Benjet [39] | 2017 | Mexico | 1071 | NA | 0.57 | NA | NA | NA | LT: 0.186 | NA |
| Borges [40] | 2011 | United States | 1004 | NA | 0.56 | NA | NA | 12M: | NA | 12M: 0.076 |
| Brunner [41] | 2007 | Germany | 5759 | 14.9 | 0.498 | LT: 0.079 | LT: 0.065 | LT: 0.144 | NA | LT: 0.149 |
| Brunner [42] | 2014 | Various European countries | 12073 | 14.9 | 0.556 | NA | NA | NA | NA | LT:0.275 |
| Calvete [43] | 2015 | Spain | 1864 | 15.32 | 0.514 | NA | NA | NA | 12M: 0.536 | NA |
| Carvalho [44] | 2017 | Brazil | 1763 | 16.75 | 0.53 | NA | NA | LT: 0.22 | LT:0296 | NA |
| Cerutti [45] | 2011 | Italy | 234 | 16.47 | 0.5 | NA | NA | NA | NA | LT: 0.419 |
| Chan [46] | 2008 | Hong Kong | 10239 | NA | NA | NA | NA | LT: 0.291 | NA | NA |
| Chan [46] | 2008 | Hong Kong | 5688 | NA | NA | NA | NA | LT: 0.269 | NA | NA |
| Cheung [47] | 2013 | Hong Kong | 2317 | 16.4 | 0.548 | 12M: 0.0967 | NA | 12M: 0.143 | 12M: 0.14 | NA |
| Choquet [48] | 1990 | France | 1519 | 14.7 | 0.45 | NA | NA | 12M:0.18 | NA | NA |
| Chou [49] | 2013 | Taiwan | 2835 | 19.75 | 0.554 | 12M: 0.105 | NA | NA | NA | NA |
| Claes [50] | 2013 | Belgium | 532 | 15.11 | 0.258 | NA | NA | NA | LT: 0.265 | NA |
| Coughlan [51] | 2014 | Ireland | 212 | 11.54 | 0.519 | LT: 0.005 | NA | LT: 0.068 | LT: 0.066 | 0.068 |
| Donald [52] | 2001 | Australia | 3082 | NA | NA | LT: 0.0185 | NA | NA | NA | NA |
| Doyle [53] | 2015 | Ireland | 856 | NA | 0.5 | NA | NA | NA | NA | LT: 0.12 |
| Fleming [54] | 2007 | New Zealand | 9570 | NA | 0.539 | 12M:0.078 | NA | NA | NA | NA |
| Garisch [55] | 2015 | New Zealand | 1162 | 16.35 | 0.615 | NA | NA | NA | LT: 0.696 | NA |
| Ghrayeb [56] | 2014 | Palestine | 720 | 15.4 | 0.496 | NA | 12M: 0.253 | 12M: 0.246 | NA | NA |
| Giletta [57] | 2012 | Italy, Netherlands, United States | 1862 | 15.69 | 0.49 | NA | NA | NA | 12M: 0.24 | NA |
| Gonzalez-Forteza [55] | 2005 | Mexico | 2531 | 16.67 | 0.544 | 0.808 | NA | NA | NA | LT: 0.072 |
| Grunbaum [58] | 2001 | United States | 16262 | 16.16 | NA | 12M: 0.077 | NA | NA | NA | NA |
| Han [59] | 2016 | United States | 135300 | NA | 0.498 | 12M: 0.013 | 12M:0.0214 | 12M: 0.069 | NA | NA |
| Han [60] | 2018 | United States | 17000 | NA | NA | 12M:0.016 | 12M:0.027 | 12M: 0.083 | NA | NA |
| Hawton [61] | 2002 | United Kingdom | 5801 | NA | 0.466 | NA | NA | 12M: 0.149 | NA | 12M: 0.069 |
| Hesketh [62] | 2002 | China | 1576 | NA | NA | LT: 0.090 | NA | LT: 0.160 | NA | NA |
| Kądziela-Olech [63] | 2015 | Poland | 2220 | 16.7 | 0.463 | NA | NA | NA | 12M:0.048 | 12M:0.083 |
| Kang [64] | 2015 | South Korea | 72623 | NA | NA | 12M: 0.049 | 12M: 0.191 | 12M:0.191 | NA | NA |
| Kataoka [65] | 2014 | Japan | 9778 | NA | 0.486 | NA | NA | 12M: 0.05 | NA | NA |
| Kidger [66] | 2012 | England | 4855 | 16.67 | 0.589 | NA | NA | NA | NA | LT: 0.186 |
| Kvernmo [67] | 2009 | Norway | 447 | 14.7 | 0.526 | NA | NA | 12M:0.161 | NA | LT: 0.136 |
| Kirmayer [68] | 1996 | Canada | 99 | 19.4 | 0.516 | LT: 0.341 | NA | LT: 0.429 | NA | NA |
| Larsson [69] | 2008 | Norway | 2464 | 13.7 | 0.508 | LT: 0.030 | NA | LT: 0.040 | LT: 0.029 | NA |
| Laskyte [70] | 2009 | Lithuania | 3848 | NA | 0.572 | NA | NA | NA | NA | LT:0.07 |
| Law [13] | 2013 | Hong Kong | 2579 | 12 | 0.5 | 12M: 0.039 | NA | 12M:0.046 | NA | 12M:0.233 |
| Laukkanen [71] | 2009 | Finland | 4205 | 15.58 | 0.536 | NA | NA | NA | NA | LT: 0.217 |
| Le [72] | 2011 | Vietnam | 7584 | NA | 0.560 | LT: 0.005 | NA | LT: 0.034 | NA | LT: 0.028 |
| Lee [73] | 2008 | South Korea | 368 | NA | 0.389 | LT: 0.033 | NA | TW: 0.098 | NA | NA |
| Lee [74] | 2013 | South Korea | 74698 | NA | 0.472 | 12M:0.0597 | NA | 12M:0.238 | NA | NA |
| Lewinsohn [75] | 1996 | USA | 1709 | NA | NA | LT: 0.071 | LT: 0.083 | LT: 0.129 | NA | NA |
| Lin [76] | 2017 | Taiwan | 2170 | 15.83 | 0.511 | NA | NA | NA | 12M:0.2 | NA |
| Liu [77] | 2018 | China | 11831 | 14.97 | 0.49 | LT: 0.040 | LT: 0.098 | LT: 0.205 | NA | NA |
| Lucassen [78] | 2011 | New Zealand | 9107 | NA | 0.46 | 12M: 0.042 | NA | 12M:0.125 | NA | 12M:0.184 |
| Madu [79] | 2003 | South America | 435 | 17.25 | 0.559 | LT: 0.209 | LT: 0.161 | LT: 0.371 | NA | NA |
| Mahfoud [80] | 2011 | Lebanon | 5109 | 13.8 | 0.543 | NA | NA | 12M: 0.157 | NA | NA |
| Madge [5] | 2008 | Australia/Belgium/ England/Hungary/ Ireland/The Netherlands/ Norway. | 30427 | 15.6 | 0.49 | NA | NA | NA | NA | LT: 0.089 |
| Matsumoto [81] | 2008 | Japan | 1726 | 14.5 | 0.51 | NA | NA | LT: 0.398 | NA | LT: 0.099 |
| McCann [82] | 2010 | Ireland | 3178 | NA | 0.59 | NA | NA | NA | NA | LT: 0.105 |
| Meehan [83] | 1992 | United States | 694 | NA | NA | LT: 0.104 | NA | LT 0.539 | NA | NA |
| Mohl [84] | 2011 | Denmark | 2864 | 17 | 0.608 | NA | NA | LT: 0.215 | NA | NA |
| Mojs [85] | 2012 | Poland | 1065 | NA | 0.72 | NA | NA | LT: 0.015 | NA | NA |
| Morey [86] | 2008 | Ireland | 3646 | 16.01 | 0.53 | NA | NA | LT: 0.056 | NA | LT: 0.091 |
| Morey [87] | 2017 | England | 2000 | 15.6 | 0.52 | NA | NA | NA | NA | LT: 0.155 |
| Muehlenkamp [88] | 2009 | United States | 1375 | 15.48 | 0.561 | LT: 0.065 | NA | NA | LT: 0.214 | NA |
| Muehlenkamp [89] | 2011 | United States | 390 | 16.27 | 0.549 | LT: 0.056 | NA | NA | LT 0.159 | NA |
| Nada-Raja [90] | 2004 | New Zealand | 966 | NA | 0.489 | LT: 0.092 | NA | LT: 0.090 | NA | LT: 0.135 |
| Nath [91] | 2012 | India | 1817 | 19.11 | NA | LT: 0.040 | NA | LT: 0.116 | NA | NA |
| Nixon [92] | 2008 | Canada | 568 | 15.2 | 0.537 | NA | NA | NA | LT: 0.169 | NA |
| Nobakht [93] | 2017 | Iran | 200 | NA | 0.5 | NA | NA | NA | NA | LT: 0.405 |
| Nock [94] | 2013 | USA | 6483 | NA | 0.482 | LT: 0.040 | LT: 0.040 | LT: 0.121 | NA | NA |
| O’Connor [95] | 2009 | Scotland | 1967 | NA | 0.534 | NA | NA | NA | NA | LT: 0.138 |
| Omigbodun [96] | 2008 | Nigeria | 1429 | 14.4 | 0.491 | 12M: 0.117 | NA | 12M: 0.229 | NA | NA |
| Patton [97] | 1997 | Australia | 1699 | NA | NA | 12M: 0.002 | NA | NA | NA | 12M: 0.051 |
| Pawlowska [98] | 2016 | Poland | 5685 | 17.18 | 0.3 | LT: 0.044 | LT: 0.150 | LT: 0.243 | NA | LT: 0.137 |
| Pérez-Amezcua [99] | 2010 | Mexico | 12424 | NA | 0.55 | LT: 0.088 | NA | LT: 0.466 | NA | NA |
| Plener [100] | 2009 | USA | 665 | 14.8 | 0.571 | LT: 0.065 | NA | LT: 0.359 | LT: 0.256 | NA |
| Portzky [101] | 2008 | Netherlands/Belgium | 8889 | 15.48 | 0.51 | NA | NA | NA | NA | LT: 0.072 |
| Rey Gex [102] | 1998 | Switzerland | 9268 | 17.46 | 0.431 | LT: 0.030 | NA | 12M: 0.172 | NA | NA |
| Rudatsikira [103] | 2007 | Guyana | 1197 | NA | 0.579 | NA | NA | 12M: 0.184 | NA | NA |
| Rudd [104] | 1989 | United States | 737 | NA | 0.61 | 12M: 0.056 | NA | 12M:0.437 | NA | NA |
| Sampasa-Kanyinga [105] | 2017 | Canada | 1922 | 14.4 | 0.54 | 12M: 0.029 | NA | 12M: 0.105 | NA | NA |
| Sarno [106] | 2010 | Italy | 578 | NA | 0.825 | NA | NA | NA | LT: 0.206 | NA |
| Shaikh [107] | 2014 | India | 5184 | NA | 0.248 | NA | 12M:0.076 | 12M: 0.033 | NA | NA |
| Shek [108] | 2012 | Hong Kong | 3328 | 12.59 | 0.472 | NA | 12M:0.0475 | 12M: 0.134 | NA | 12M: 0.327 |
| Sidhartha [109] | 2006 | India | 1205 | 14.73 | 0.4 | LT: 0.080 | NA | LT: 0.217 | NA | LT: 0.180 |
| Silviken [110] | 2007 | Norway | 2691 | 16.9 | 0.521 | LT: 0.095 | NA | SM: 0.151 | NA | NA |
| Soares [111] | 2015 | Brazil | 549 | NA | 0.801 | LT:0.027 | NA | LT: 0.118 | NA | NA |
| Somer [112] | 2015 | Turkey | 1656 | 16.8 | 0.55 | NA | NA | NA | LT: 0.313 | NA |
| Sornberger [113] | 2012 | Canada | 1744 | 14.92 | 0.508 | NA | NA | NA | LT: 0.245 | NA |
| Straub [114] | 2015 | Germany | 1117 | 14.83 | 0.527 | LT:0.056 | NA | LT: 0.317 | NA | NA |
| Tang [115] | 2011 | Hong Kong | 2013 | 15.6 | 0.453 | 12M: 0.0348 | NA | 12M:0.088 | 12M: 0.155 | NA |
| Tang [116] | 2018 | China | 15623 | 15.2 | 0.485 | 12M: 0.0443 | 12M:0.08 | 12M: 0.159 | 12M: 0.292 | NA |
| Teo [117] | 2011 | Australia | 207 | NA | NA | NA | NA | NA | NA | LT: 0.14 |
| Thaku [118] | 2015 | India | 705 | NA | 0.488 | NA | NA | 12M: 0.309 | NA | NA |
| Toprak [119] | 2010 | Turkey | 636 | 19.36 | 0.539 | LT:0.072 | NA | LT: 0.126 | NA | LT: 0.171 |
| Tresno [120] | 2012 | Indonesia | 207 | 19.78 | NA | LT:0.121 | NA | NA | LT: 0.565 | NA |
| Valdez-Santiago [121] | 2017 | Mexico | 21509 | 15.4 | NA | LT: 0.027 | NA | NA | NA | NA |
| Vawda [122] | 2013 | South Africa | 222 | 13.3 | 0.482 | LT: 0.054 | LT: 0.059 | LT 0.225 | NA | NA |
| Ventura-Junca [123] | 2010 | Chile | 1567 | 16.2 | 0.459 | LT: 0.190 | NA | LT: 0.620 | NA | NA |
| Wan [124] | 2011 | China | 17622 | 16.1 | 0.512 | NA | NA | NA | NA | 12M: 0.17 |
| Whitlock [125] | 2011 | United States | 11529 | NA | 0.576 | NA | NA | NA | LT:0.154 | NA |
| Xin [126] | 2017 | China | 11880 | 14.62 | 0.505 | 12M: 0.0491 | 12M:0.11 | 12M: 0.209 | NA | 12M: 0.30 |
| Zetterqvist [127] | 2013 | Sweden | 3060 | NA | 0.505 | NA | NA | NA | 12M:0.356 | NA |
| Zubrick [128] | 2016 | Australia | 2563 | NA | 0.692 | 12M: 0.0241 | 12M: 0.052 | 12M: 0.075 | 12M:0.08 | NA |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, K.-S.; Wong, C.H.; McIntyre, R.S.; Wang, J.; Zhang, Z.; Tran, B.X.; Tan, W.; Ho, C.S.; Ho, R.C. Global Lifetime and 12-Month Prevalence of Suicidal Behavior, Deliberate Self-Harm and Non-Suicidal Self-Injury in Children and Adolescents between 1989 and 2018: A Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 4581. https://doi.org/10.3390/ijerph16224581
Lim K-S, Wong CH, McIntyre RS, Wang J, Zhang Z, Tran BX, Tan W, Ho CS, Ho RC. Global Lifetime and 12-Month Prevalence of Suicidal Behavior, Deliberate Self-Harm and Non-Suicidal Self-Injury in Children and Adolescents between 1989 and 2018: A Meta-Analysis. International Journal of Environmental Research and Public Health. 2019; 16(22):4581. https://doi.org/10.3390/ijerph16224581
Chicago/Turabian StyleLim, Kim-San, Celine H. Wong, Roger S. McIntyre, Jiayun Wang, Zhisong Zhang, Bach X. Tran, Wanqiu Tan, Cyrus S. Ho, and Roger C. Ho. 2019. "Global Lifetime and 12-Month Prevalence of Suicidal Behavior, Deliberate Self-Harm and Non-Suicidal Self-Injury in Children and Adolescents between 1989 and 2018: A Meta-Analysis" International Journal of Environmental Research and Public Health 16, no. 22: 4581. https://doi.org/10.3390/ijerph16224581
APA StyleLim, K.-S., Wong, C. H., McIntyre, R. S., Wang, J., Zhang, Z., Tran, B. X., Tan, W., Ho, C. S., & Ho, R. C. (2019). Global Lifetime and 12-Month Prevalence of Suicidal Behavior, Deliberate Self-Harm and Non-Suicidal Self-Injury in Children and Adolescents between 1989 and 2018: A Meta-Analysis. International Journal of Environmental Research and Public Health, 16(22), 4581. https://doi.org/10.3390/ijerph16224581