Psychosocial and Physiological Health Outcomes of Green Exercise in Children and Adolescents—A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Eligibility Criteria
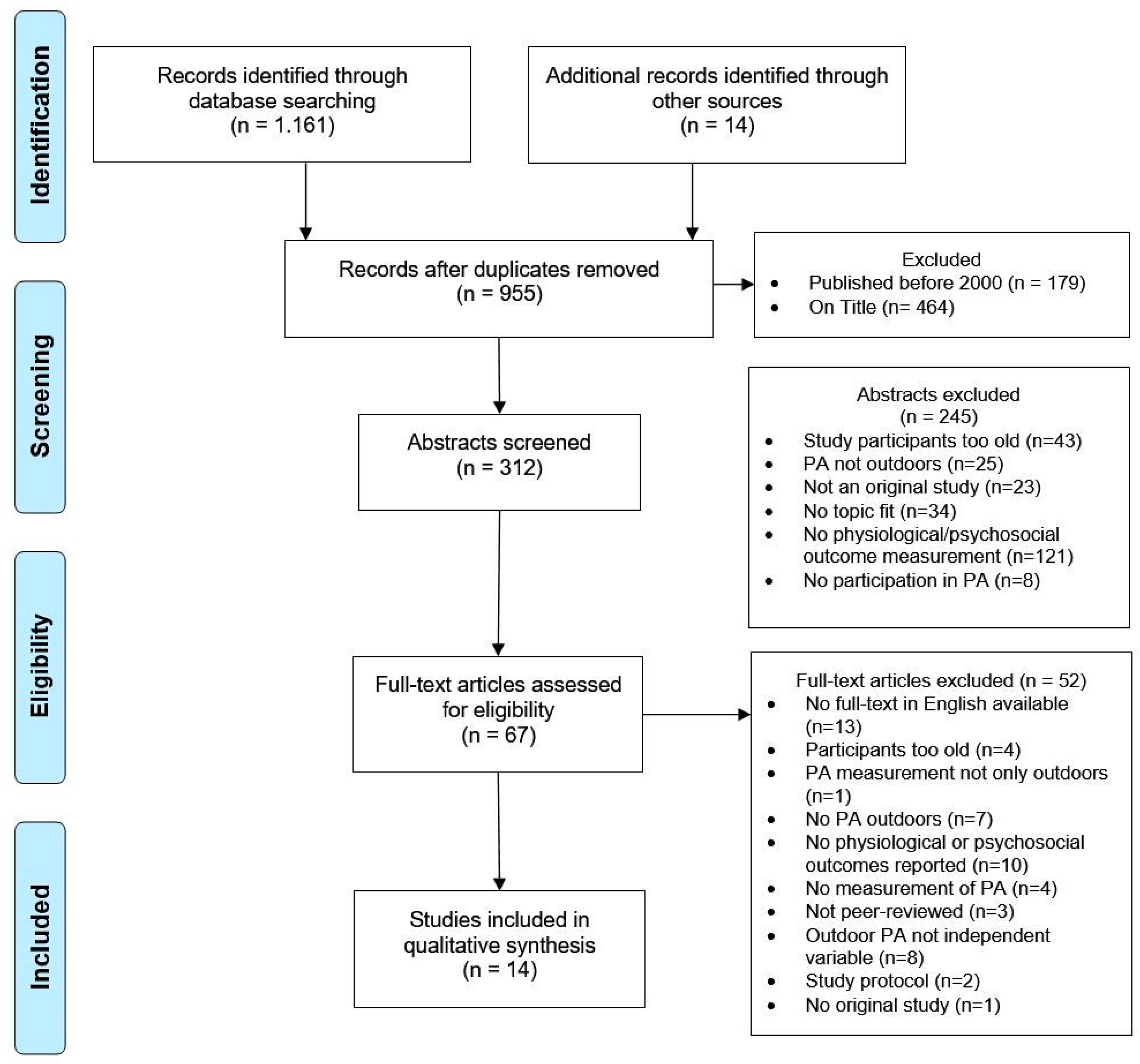
2.2. Screening and Study Selection
3. Results
3.2. Quality of the Evidence
3.3. Evidence Synthesis
3.3.1. Effectiveness of GE
3.3.2. Overview of Psychosocial and Physiological Outcomes
4. Discussion
4.1. Theoretical Background Considerations
4.2. Assessed Outcomes Related to GE
4.3. Conceptual Considerations—What Is “Green”?
4.4. Characteristics of PA Outdoors
4.5. Study Population and Sample Size
4.6. Quality Assessment
4.7. Study Limitations
5. Conclusions and Future Directions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Janssen, I.; Leblanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.Y.; Han, L.H.; Zhang, J.H.; Luo, S.; Hu, J.W.; Sun, K. The influence of physical activity, sedentary behavior on health-related quality of life among the general population of children and adolescents: A systematic review. PLoS ONE 2017, 12, e0187668. [Google Scholar] [CrossRef] [PubMed]
- Fedewa, A.L.; Ahn, S. The Effects of Physical Activity and Physical Fitness on Children’s Achievement and Cognitive Outcomes. Res. Q. Exerc. Sport 2011, 82, 521–535. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Bueno, C.; Pesce, C.; Cavero-Redondo, I.; Sanchez-Lopez, M.; Martinez-Hortelano, J.A.; Martinez-Vizcaino, V. The Effect of Physical Activity Interventions on Children’s Cognition and Metacognition: A Systematic Review and Meta-Analysis. J. Am. Acad. Child Adolesc. Psychiatr. 2017, 56, 729–738. [Google Scholar] [CrossRef]
- McKercher, C.; Sanderson, K.; Schmidt, M.D.; Otahal, P.; Patton, G.C.; Dwyer, T.; Venn, A.J. Physical activity patterns and risk of depression in young adulthood: A 20-year cohort study since childhood. Soc. Psychiatry Psychiatr. Epidemiol. 2014, 49, 1823–1834. [Google Scholar] [CrossRef]
- Fernandes, R.A.; Zanesco, A. Early physical activity promotes lower prevalence of chronic diseases in adulthood. Hypertens. Res. 2010, 33, 926–931. [Google Scholar] [CrossRef]
- McCormick, R. Does Access to Green Space Impact the Mental Well-being of Children: A Systematic Review. J. Pediatr. Nurs. 2017, 37, 3–7. [Google Scholar] [CrossRef]
- Söderström, M.; Boldemann, C.; Sahlin, U.; Martensson, F.; Raustorp, A.; Blennow, M. The quality of the outdoor environment influences childrens health—A cross-sectional study of preschools. Acta Paediatr. 2013, 102, 83–91. [Google Scholar] [CrossRef]
- Maas, J.; Verheij, R.A.; De Vries, S.; Spreeuwenberg, P.; Schellevis, F.G.; Groenewegen, P.P. Morbidity is related to a green living environment. J. Epidemiol. Community Health 2009, 63, 967–973. [Google Scholar] [CrossRef]
- Taylor, A.F.; Kuo, F.E. Could Exposure to Everyday Green Spaces Help Treat ADHD? Evidence from Children’s Play Settings. Appl. Psychol. Health Well Being 2011, 3, 281–303. [Google Scholar] [CrossRef]
- Sharp, J.R.; Maguire, J.L.; Carsley, S.; Abdullah, K.; Chen, Y.; Perrin, E.M.; Parkin, P.C.; Birken, C.S.; Collaboration, T.A.K. Temperament Is Associated With Outdoor Free Play in Young Children: A TARGet Kids! Study. Acad. Pediatr. 2018, 18, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; Nieuwenhuijsen, M.J.; Esnaola, M.; Forns, J.; Basagaña, X.; Alvarez-Pedrerol, M.; Rivas, I.; López-Vicente, M.; De Castro Pascual, M.; Su, J.; et al. Green spaces and cognitive development in primary schoolchildren. Proc. Natl. Acad. Sci. USA 2015, 112, 7937–7942. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-D.; McNeely, E.; Cedeño-Laurent, J.G.; Pan, W.-C.; Adamkiewicz, G.; Dominici, F.; Lung, S.-C.C.; Su, H.-J.; Spengler, J.D. Linking Student Performance in Massachusetts Elementary Schools with the “Greenness” of School Surroundings Using Remote Sensing. PLoS ONE 2014, 9, e108548. [Google Scholar] [CrossRef] [PubMed]
- Markevych, I.; Tiesler, C.M.T.; Fuertes, E.; Romanos, M.; Dadvand, P.; Nieuwenhuijsen, M.J.; Berdel, D.; Koletzko, S.; Heinrich, J. Access to urban green spaces and behavioural problems in children: Results from the GINIplus and LISAplus studies. Environ. Int. 2014, 71, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Flouri, E.; Midouhas, E.; Joshi, H. The role of urban neighbourhood green space in children’s emotional and behavioural resilience. J. Environ. Psychol. 2014, 40, 179–186. [Google Scholar] [CrossRef]
- Richardson, E.A.; Pearce, J.; Shortt, N.K.; Mitchell, R. The role of public and private natural space in children’s social, emotional and behavioural development in Scotland: A longitudinal study. Environ. Res. 2017, 158, 729–736. [Google Scholar] [CrossRef]
- Markevych, I.; Thiering, E.; Fuertes, E.; Sugiri, D.; Berdel, D.; Koletzko, S.; von Berg, A.; Bauer, C.P.; Heinrich, J. A cross-sectional analysis of the effects of residential greenness on blood pressure in 10-year old children: Results from the GINIplus and LISAplus studies. BMC Public Health 2014, 14, 11. [Google Scholar] [CrossRef]
- Kelz, C.; Evans, G.W.; Röderer, K. The restorative effects of redesigning the schoolyard: A multi-methodological, quasi-experimental study in rural Austrian middle schools. Environ. Behav. 2015, 47, 119–139. [Google Scholar] [CrossRef]
- Dadvand, P.; Villanueva, C.M.; Font-Ribera, L.; Martinez, D.; Basagana, X.; Belmonte, J.; Vrijheid, M.; Grazuleviciene, R.; Kogevinas, M.; Nieuwenhuijsen, M.J. Risks and Benefits of Green Spaces for Children: A Cross-Sectional Study of Associations with Sedentary Behavior, Obesity, Asthma, and Allergy. Environ. Health Perspect. 2014, 122, 1329–1335. [Google Scholar] [CrossRef]
- Almanza, E.; Jerrett, M.; Dunton, G.; Seto, E.; Ann Pentz, M. A study of community design, greenness, and physical activity in children using satellite, GPS and accelerometer data. Health Place 2012, 18, 46–54. [Google Scholar] [CrossRef]
- Gray, C.; Gibbons, R.; Larouche, R.; Sandseter, E.B.H.; Bienenstock, A.; Brussoni, M.; Chabot, G.; Herrington, S.; Janssen, I.; Pickett, W.; et al. What Is the Relationship between Outdoor Time and Physical Activity, Sedentary Behaviour, and Physical Fitness in Children? A Systematic Review. Int. J. Environ. Res. Public Health 2015, 12, 6455–6474. [Google Scholar] [CrossRef] [PubMed]
- Larouche, R.; Garriguet, D.; Gunnell, K.E.; Goldfield, G.S.; Tremblay, M.S. Outdoor time, physical activity, sedentary time, and health indicators at ages 7 to 14: 2012/2013 Canadian Health Measures Survey. Health Rep. 2016, 27, 3–13. [Google Scholar] [PubMed]
- Larouche, R.; Mire, E.; Belanger, K.; Barreira, T.; Chaput, J.-P.; Fogelholm, M.; Hu, G.; Lambert, E.; Maher, C.; Maia, J.; et al. Relationships between outdoor time, physical activity, sedentary behavior and obesity in children: A 12-country study. Pediatr. Exerc. Sci. 2018, 15, S71–S72. [Google Scholar]
- Larouche, R.; Garriguet, D.; Tremblay, M.S. Outdoor time, physical activity and sedentary time among young children: The 2012–2013 Canadian Health Measures Survey. Can. J. Public Health. 2016, 107, E500–E506. [Google Scholar] [CrossRef] [PubMed]
- Shanahan, D.F.; Franco, L.; Lin, B.B.; Gaston, K.J.; Fuller, R.A. The Benefits of Natural Environments for Physical Activity. Sports Med. 2016, 46, 989–995. [Google Scholar] [CrossRef]
- Pretty, J.; Griffin, M.; Sellens, M.; Pretty, C. Green Exercise: Complementary Roles of Nature, Exercise and Diet in Physical and Emotional Well-Being and Implications for Public Health Policy. CES Occasional Paper 2003, 1, 1–39. [Google Scholar]
- Pretty, J. How nature contributes to mental and physical health. Spiritual. Health Int. 2004, 5, 68–78. [Google Scholar] [CrossRef]
- Lahart, I.; Darcy, P.; Gidlow, C.; Calogiuri, G. The Effects of Green Exercise on Physical and Mental Wellbeing: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 1352. [Google Scholar] [CrossRef]
- Calogiuri, G.; Nordtug, H.; Weydahl, A. The Potential of Using Exercise in Nature as an Intervention to Enhance Exercise Behavior: Results from a Pilot Study. Percept. Mot. Skills 2015, 121, 350–370. [Google Scholar] [CrossRef]
- Brown, D.K.; Barton, J.L.; Pretty, J.; Gladwell, V.F. Walks4Work: Assessing the role of the natural environment in a workplace physical activity intervention. Scand. J. Work. Environ. Health 2014, 390–399. [Google Scholar] [CrossRef]
- Mackay, G.J.; Neill, J.T. The effect of “green exercise” on state anxiety and the role of exercise duration, intensity, and greenness: A quasi-experimental study. J. Sport Exerc. Psychol. 2010, 11, 238–245. [Google Scholar] [CrossRef]
- Pretty, J.; Peacock, J.; Hine, R.; Sellens, M.; South, N.; Griffin, M. Green exercise in the UK countryside: Effects on health and psychological well-being, and implications for policy and planning. J. Environ. Plann. Man. 2007, 50, 211–231. [Google Scholar] [CrossRef]
- Wooller, J.J.; Rogerson, M.; Barton, J.; Micklewright, D.; Gladwell, V. Can Simulated Green Exercise Improve Recovery From Acute Mental Stress? Front. Psychol. 2018, 9. [Google Scholar] [CrossRef]
- Thompson Coon, J.; Boddy, K.; Stein, K.; Whear, R.; Barton, J.; Depledge, M.H. Does Participating in Physical Activity in Outdoor Natural Environments Have a Greater Effect on Physical and Mental Wellbeing than Physical Activity Indoors? A Systematic Review. Environ. Sci. Technol. 2011, 45, 1761–1772. [Google Scholar] [CrossRef] [PubMed]
- Manferdelli, G.; La Torre, A.; Codella, R. Outdoor physical activity bears multiple benefits to health and society. J. Sports Med. Phys. Fitness 2019. [Google Scholar] [CrossRef] [PubMed]
- Eigenschenk, B.; Thomann, A.; McClure, M.; Davies, L.; Gregory, M.; Dettweiler, U.; Ingles, E. Benefits of Outdoor Sports for Society. A Systematic Literature Review and Reflections on Evidence. Int. J. Environ. Res. Public Health 2019, 16, 937. [Google Scholar] [CrossRef] [PubMed]
- Moher, D. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Peacock, R. Effectiveness and efficiency of search methods in systematic reviews of complex evidence: Audit of primary sources. BMJ 2005, 331, 1064–1065. [Google Scholar] [CrossRef]
- de Oliveira, A.M.; Buchain, P.C.; Vizzotto, A.D.B.; Elkis, H.; Cordeiro, Q. Psychosocial Impact. In Encyclopedia of Behavioral Medicine; Gellman, M.D., Ed.; Springer: New York, NY, USA, 2013; pp. 1583–1584. [Google Scholar]
- Vizzotto, A.D.B.; de Oliveira, A.M.; Elkis, H.; Cordeiro, Q.; Buchain, P.C. Psychosocial Characteristics. In Encyclopedia of Behavioral Medicine; Gellman, M.D., Ed.; Springer: New York, NY, USA, 2013; pp. 1578–1580. [Google Scholar]
- Salomon, K. Physiological Reactivity. In Encyclopedia of Behavioral Medicine; Gellmann, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 1493–1494. [Google Scholar]
- Thomas, B.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological research. J. Eval. Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef]
- Bourne, J.E.; Sauchelli, S.; Perry, R.; Page, A.; Leary, S.; England, C.; Cooper, A.R. Health benefits of electrically-assisted cycling: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 116. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.; Dinnes, J.; D’Amico, R.; Sowden, A.; Sakarovitch, C.; Song, F.; Petticrew, M.; Altman, D. Evaluating non-randomised intervention studies. Health Technol. Assess. 2003, 7, iii–x, 1–173. [Google Scholar] [CrossRef] [PubMed]
- Gopinath, B.; Baur, L.A.; Wang, J.J.; Hardy, L.L.; Teber, E.; Kifley, A.; Wong, T.Y.; Mitchell, P. Influence of Physical Activity and Screen Time on the Retinal Microvasculature in Young Children. Arterioscler. Thromb. Vasc. Biol. 2011, 31, 1233–1239. [Google Scholar] [CrossRef] [PubMed]
- Gopinath, B.; Hardy, L.L.; Baur, L.A.; Burlutsky, G.; Mitchell, P. Physical activity and sedentary behaviors and health-related quality of life in adolescents. Pediatrics 2012, 130, e167–e174. [Google Scholar] [CrossRef]
- Gopinath, B.; Hardy, L.L.; Teber, E.; Mitchell, P. Association between physical activity and blood pressure in prepubertal children. Hypertens. Res. 2011, 34, 851–855. [Google Scholar] [CrossRef] [PubMed]
- Parsons, A.A.; Ollberding, N.J.; Smith, L.; Copeland, K.A. Sleep matters: The association of race, bedtime, outdoor time, and physical activity with preschoolers’ sleep. Prev. Med. 2018, 12, 54–59. [Google Scholar] [CrossRef]
- Duncan, M.J.; Clarke, N.D.; Birch, S.L.; Tallis, J.; Hankey, J.; Bryant, E.; Eyre, E.L.J. The Effect of Green Exercise on Blood Pressure, Heart Rate and Mood State in Primary School Children. Int. J. Environ. Res. Public Health 2014, 11, 3678–3688. [Google Scholar] [CrossRef]
- Faber Taylor, A.; Kuo, F.E. Children With Attention Deficits Concentrate Better After Walk in the Park. J. Atten. Disord. 2009, 12, 402–409. [Google Scholar] [CrossRef]
- Reed, K.; Wood, C.; Barton, J.; Pretty, J.N.; Cohen, D.; Sandercock, G.R. A repeated measures experiment of green exercise to improve self-esteem in UK school children. PLoS ONE 2013, 8, e69176. [Google Scholar] [CrossRef]
- Wood, C.; Angus, C.; Pretty, J.; Sandercock, G.; Barton, J. A randomised control trial of physical activity in a perceived environment on self-esteem and mood in UK adolescents. Int. J. Environ. Health Res. 2013, 23, 311–320. [Google Scholar] [CrossRef]
- Wood, C.; Sandercock, G.; Barton, J. Interactions between physical activity and the environment to improve adolescent self-esteem: A randomised controlled trial. Int. J. Environ. Health 2014, 7, 144–155. [Google Scholar] [CrossRef]
- Barton, J.; Sandercock, G.; Pretty, J.; Wood, C. The effect of playground- and nature-based playtime interventions on physical activity and self-esteem in UK school children. Int. J. Environ. Health Res. 2015, 25, 196–206. [Google Scholar] [CrossRef] [PubMed]
- Flynn, J.I.; Bassett, D.R.; Fouts, H.N.; Thompson, D.L.; Coe, D.P. Active Families in the Great Outdoors: A program to promote family outdoor physical activity. J. Adventure Educ. Outdoor Learn. 2017, 17, 227–238. [Google Scholar] [CrossRef]
- Raney, M.A.; Hendry, C.F.; Yee, S.A. Physical activity and social behaviors of urban children in green playgrounds. Am. J. Prev. Med. 2019, 56, 522–529. [Google Scholar] [CrossRef]
- Hammond, D.E.; McFarland, A.L.; Zajicek, J.M.; Waliczek, T.M. Growing Minds: The Relationship Between Parental Attitudes Toward Their Child’s Outdoor Recreation and Their Child’s Health. Horttechnology 2011, 21, 217–224. [Google Scholar] [CrossRef]
- Liu, J.; Sekine, M.; Tatsuse, T.; Fujimura, Y.; Hamanishi, S.; Lu, F.; Zheng, X. Outdoor physical activity and its relation with self-reported health in Japanese children: Results from the Toyama birth cohort study. Child Care Health Dev. 2015, 41, 920–927. [Google Scholar] [CrossRef]
- Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Ulrich, R.S. Aesthetic and affective response to natural environment. In Behavior and the Natural Environment; Plenum Press: New York, NY, USA, 1983; pp. 85–125. [Google Scholar]
- Barton, J.; Pretty, J. What is the Best Dose of Nature and Green Exercise for Improving Mental Health? A Multi-Study Analysis. Environ. Sci. Technol. 2010, 44, 3947–3955. [Google Scholar] [CrossRef]
- Rogerson, M.; Barton, J. Effects of the Visual Exercise Environments on Cognitive Directed Attention, Energy Expenditure and Perceived Exertion. Int. J. Environ. Res. Public Health 2015, 12, 7321–7336. [Google Scholar] [CrossRef]
- Araújo, D.; Brymer, E.; Brito, H.; Withagen, R.; Davids, K. The empowering variability of affordances of nature: Why do exercisers feel better after performing the same exercise in natural environments than in indoor environments? J. Sport Exerc. Psychol. 2019, 42, 138–145. [Google Scholar] [CrossRef]
- Heitzler, C.D.; Martin, S.L.; Duke, J.; Huhman, M. Correlates of physical activity in a national sample of children aged 9–13 years. Prev. Med. 2006, 42, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Van Dyck, D.; De Meester, F.; Cardon, G.; Deforche, B.; De Bourdeaudhuij, I. Physical Environmental Attributes and Active Transportation in Belgium: What about Adults and Adolescents Living in the Same Neighborhoods? Am. J. Health Promot. 2013, 27, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.C. The relationship between nature-based tourism and autonomic nervous system function among older adults. J. Travel Med. 2014, 21, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Gladwell, V.; Kuoppa, P.; Tarvainen, M.; Rogerson, M. A Lunchtime Walk in Nature Enhances Restoration of Autonomic Control during Night-Time Sleep: Results from a Preliminary Study. Int. J. Environ. Res. Public Health 2016, 13, 280. [Google Scholar] [CrossRef] [PubMed]
- Rogerson, M.; Gladwell, V.; Gallagher, D.; Barton, J. Influences of Green Outdoors versus Indoors Environmental Settings on Psychological and Social Outcomes of Controlled Exercise. Int. J. Environ. Res. Public Health 2016, 13, 363. [Google Scholar] [CrossRef]
- Börnhorst, C.; Wijnhoven, T.M.; Kunešová, M.; Yngve, A.; Rito, A.I.; Lissner, L.; Duleva, V.; Petrauskiene, A.; Breda, J. WHO European Childhood Obesity Surveillance Initiative: Associations between sleep duration, screen time and food consumption frequencies. BMC Public Health 2015, 15. [Google Scholar] [CrossRef]
- Rey-López, J.P.; Vicente-Rodriguez, G.; Ortega, F.B.; Ruiz, J.R.; Martinez-Gómez, D.; De Henauw, S.; Manios, Y.; Molnar, D.; Polito, A.; Verloigne, M.; et al. Sedentary patterns and media availability in European adolescents: The HELENA study. Prev. Med. 2010, 51, 50–55. [Google Scholar] [CrossRef]
- Mutz, M.; Müller, J. Mental health benefits of outdoor adventures: Results from two pilot studies. J. Adolesc. 2016, 49, 105–114. [Google Scholar] [CrossRef]
- Truelove, S.; Bruijns, B.A.; Vanderloo, L.M.; O’Brien, K.T.; Johnson, A.M.; Tucker, P. Physical activity and sedentary time during childcare outdoor play sessions: A systematic review and meta-analysis. Prev. Med. 2018, 108, 74–85. [Google Scholar] [CrossRef]
- Jankowska, M.M.; Schipperijn, J.; Kerr, J. A Framework for Using GPS Data in Physical Activity and Sedentary Behavior Studies. Exerc. Sport Sci. Rev. 2015, 43, 48–56. [Google Scholar] [CrossRef]
- Klinker, C.D.; Schipperijn, J.; Christian, H.; Kerr, J.; Ersbøll, A.K.; Troelsen, J. Using accelerometers and global positioning system devices to assess gender and age differences in children’s school, transport, leisure and home based physical activity. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 8. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: New York, NY, USA, 2013. [Google Scholar]
- Wood, L.; Egger, M.; Gluud, L.L.; Schulz, K.F.; Jüni, P.; Altman, D.G.; Gluud, C.; Martin, R.M.; Wood, A.J.G.; Sterne, J.A.C. Empirical evidence of bias in treatment effect estimates in controlled trials with different interventions and outcomes: Meta-epidemiological study. BMJ 2008, 336, 601–605. [Google Scholar] [CrossRef] [PubMed]
- Glaser, B.; Strauss, A. Grounded theory: The discovery of grounded theory. Sociol. J. Br. Sociol. Assoc. 1967, 12, 27–49. [Google Scholar]
- Fahrenberg, J.; Myrtek, M.; Pawlik, K.; Perrez, M. Ambulatory assessment—Monitoring behavior in daily life settings: A behavioral-scientific challenge for psychology. Eur. J. Psychol. Assess. 2007, 23, 206–213. [Google Scholar] [CrossRef]
- Trull, T.J.; Ebner-Priemer, U. Ambulatory assessment. Annu. Rev. Clin. Psychol. 2013, 9, 151–176. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| PICOS | Eligibility Criteria |
|---|---|
| Population |
|
| Intervention |
|
| Comparison |
|
| Outcomes |
|
| Study Design |
|
| Author/Year | Study Design | Participants and Country | Type of Green Exercise and Procedures | Outcome Variable(s) | Measurement Instrument(s) | Results | Quality Assessment |
|---|---|---|---|---|---|---|---|
| Barton et al. (2015) [55] | Crossover RCT | 52 boys and girls Mean age: 9 years UK | Intervention and control condition in both urban and rural school, available during lunch time break (55 min) at both schools Intervention: five days of nature-based orienteering (NBO) Control: five days provision of playground sports equipment (PSE) on not-green playground during recess | Self-esteem (SE) | Accelerometer Rosenberg SE scale | ○ = SE | Weak SB: 3, SD: 2, C: 2, B: 3, DCM: 3, WD: 3 |
| Duncan et al. (2014) [50] | Crossover RCT | 14 children (50% female) Mean age: 10 years UK | Two 15 min bouts of cycling at in two lab conditions Intervention: green condition (viewing a film of cycling in a forest) Control condition: viewing a black screen | Blood pressure (BP) Heart rateMood state response | Automated oscillometric device Heart rate monitor Fatigue, tension and vigor subscales of Brunel Mood State Inventory | ↓↓ systolic BP 15 min post-exercise ○ = systolic BP or diastolic BP immediately post-exercise ↑ = HR immediately and 15 min. post-exercise ↑ fatigue score ↓ = vigor score ○ = tension | Weak SB: 3, SD: 1, C: 1, B: 3, DCM: 1, WD: 1 |
| Faber Taylor & Kuo (2009) [51] | Crossover RCT | 17 children with (12% female) attention deficit hyperactivity disorder (ADHD) Mean age: 9 years USA | 20 min guided walk in three different settings Intervention: park (green area) Control 1: residential area Control 2: downtown area | Attention Child’s rating of settings | Digit Span Backwards (DSB) three-point scale for children to rate walk as fun, relaxing, interesting, scary, boring, weird, and/or uncomfortable | ↑↑ Digit Span Backwards score post-intervention ↑↑ fun rating = ratings for relaxing, interesting, scary, boring, weird, and/or uncomfortable | Moderate SB: 3, SD: 1, C: 1, B: 1, DCM: 1, WD: 2 |
| Flynn et al. (2017) [56] | One group pre-post | 27 children in 16 families (51.9% female) Mean age: 11 years USA | Four-week outdoor PA family intervention | PA self-efficacy PA enjoyment PA social support | Weekly PA activity logs (filled in by parents) Self-administered survey for children on PA enjoyment, SE, and social support | ○ PA enjoyment and self-efficacy ↑ PA social support | Weak SB: 3, SD: 2, C: 1, B: 3, DCM: 2, WD: 3 |
| Gopinath, Baur et al.; Gopinath, Hardy et al. (2011) [46,48] | Cross-sectional | 1765 children (48.3% female) [48], 1492 children (49.3% female) [46] Mean age: 7 years Australia | Comparison of children Exposure: low, middle and high tertile of outdoor PA Control: low, middle and high tertile of indoor PA Linear associations between BP and indoor/outdoor PA | Retinal Arteriolar and venular Diameter Systolic BP Diastolic BP Mean arterial BP | Questionnaire on PA (proxy-report through parents) Retinal photography Automated sphygmomanometer | = retinal arteriolar and venular diameter = systolic and diastolic BP Linear association between indoor PA and ↓ diastolic BP and ↓ mean arterial BP, ○ systolic BP ○ outdoor PA and BP outcome | Weak SB: 2, SD: 3, C: N/A, B: N/A, DCM: 3, WD: 1 |
| Gopinath et al. (2012) [47] | Prospective cohort study | Cross-sectional: 1094 adolescents (56.1 % female) longitudinal: 775 children and adolescents Mean age: 12 years at basline, 17 years at follow-up Australia | five-year cohort study. Comparison of children cross-sectionally (at follow-up) and longitudinally. QoL was only measured at follow-up. Comparison of children Exposure: low, moderate and high tertile of outdoor PA Control: low and moderate-high tertile of indoor PA | Health related quality of life (QoL) | Questionnaire on PA Pediatric Quality of Life Inventory 4.0 | ↑ QoL in control group in low tertiles ↑↑ QoL comparing high and moderate-high tertiles | Weak SB: 2, SD: 2, C: N/A, B: N/A, DCM: 3, WD: 3 |
| Hammond et al. (2011) [58] | Cross-sectional | 140 parents (84% female) of children between 6 and 13 years USA | One-time questionnaire accessed through parents (proxy-reporting) to report about children’s health problems and PA in two settings Exposure: PA outdoors Control: PA indoors | Health problems | Health inventory Questions on outdoor and indoor organized activities and sports | ○ = health problems (body pain/discomfort, trouble sleeping, repeated upset stomach, feeling tired/having low energy) | Weak SB: 3, SD: 3, C: N/A, B: N/A, DCM: 3, WD: 1 |
| Liu et al. (2015) [59] | Prospectivecohort study | 5238 children (52.2% female) Mean age: 6 years at baseline, 12 years at follow-up Japan | six-year cohort study (baseline at age 6). Questionnaire on frequency of outdoor PA and self-reported health at baseline and follow-up. Exposure: frequent outdoor PA Control: infrequent outdoor PA | Self-reported health | Self-report questionnaire about outdoor PA Dartmouth Primary Care Cooperative project Charts (Self-report instrument about health) | ↑↑ self-reported health at baseline and follow-up | Weak SB: 2, SD: 2, C: N/A, B: N/A, DCM: 3, WD: 3 |
| Parsons et al. (2018) [49] | Cross-sectional study | 447 children (51.5% female) Mean age: 4 yearsUSA | Data collection on sleep and PA indoors and outdoors in child-care centers Exposure: outdoors Control: indoors | Sleep duration | Sleep diary filled in by parents and child care center staff Accelerometer Observation of outdoor and indoor PA through child care center staff | ○ = sleep duration | Weak SB: 2, SD: 3, C: N/A, B: N/A, DCM: 3, WD: 1 |
| Raney et al. (2019) [57] | Nonrandomized controlled trial | 437 children (51.1% female) 5th grade students USA | Outdoor PA in school playgrounds during 20 min recess Intervention: playground greening at one school Control: no greening | Antisocial interactions | Accelerometers System for Observing Play and Leisure Activity in Youth (SOPLAY) System for Observing Children’s Activity and Relationships During Play (SOCARP) | ↓↓ of physical and verbal conflicts after four months ↓ of minutes spent alone and ↑ increase of minutes spent in small groups in intervention group | Weak SB: 3, SD: 1, C: 3, B: 3, DCM: 1, WD: 3 |
| Reed et al. (2013) [52] | Crossover RCT | 86 boys and girls Age: 11–12 years UK | Running over 1.5 miles in two settings; participants engaged in both conditions Intervention: green setting Control: urban nongreen setting | SE Exercise enjoyment Perceived exertion | PA questionnaire for adolescents Fitnessgram Pacer Test Rosenberg SE Scale Ratings of Perceived Exertion Scale | ↑ = SE = ratings of perceived exertion and enjoyment | Weak SB: 3, SD: 3, C: N/A, B: N/A, DCM: 3, WD: 1 |
| Wood et al. (2013) [53] | Crossover RCT | 25 children (56% female) Age: 11–12 years UK | Laboratory condition: All participants engaged in two constant load tests on a cycle ergometer (10 min) whilst viewing two types of picture series Intervention: natural environment pictures Control: built environment pictures | SE Mood | Rosenberg SE scale Adolescent Profile of Mood States Questionnaire (PMSQ) | ↑ = SE and fatigue ↓ = tension ○ = depression, anger, vigor and confusion | Weak SB: 3, SD: 1, C: 1, B: 2, DCM: 3, WD: 1 |
| Wood et al. (2014) [54] | Crossover RCT | 60 children (50% female) Mean age: 13 years UK | Participants engaged in two orienteering courses (20 min, respectively) Intervention: natural environment Control: built environment | SE | Accelerometer Rosenberg SE scale | ↑ = SE | Weak SB: 3, SD: 1, C: 1, B: 3, DCM: 2, WD: 3 |
| Psychosocial Outcome | Stronger/only Effect Intervention/Exposure Group | Effect both in Intervention and Control Group | No Effect neither in Intervention or Control Group/ No Differences between Exposure and Control Group | Stronger/Only Effect in Control Group |
|---|---|---|---|---|
| Self-esteem | ↑ [52,53,54] | [55] | ||
| Fatigue | ↑ [50,53] | |||
| Vigor | ↓ [50] | [53] | ||
| Tension | ↓ [53] | [50] | ||
| Anger | [53] | |||
| Depression | [53] | |||
| Confusion | [53] | |||
| Attention | ↑ [51] | |||
| Setting rating | [51] | |||
| PAself-efficacy | [56] | |||
| PA enjoyment | [52,56] | |||
| Social support | ↑ [56] | |||
| Health-related quality of life | ↑ [47] | ↑ [47] | ||
| Self-reported health | ↑ [59] | [58] | ||
| Antisocialinteractions | ↓ [57] |
| Physiological Outcome | Stronger/only Effect Intervention/Exposure Group | Effect both in Intervention and Control Group | No effect neither in Intervention or Control Group/ No Differences between Exposure and Control Group | Stronger/Only Effect in Control Group |
|---|---|---|---|---|
| Systolic BP | ↓ [50] | [48] | ||
| Diastolic BP | [48,50] | ↓ [48] | ||
| Mean arterial BP | ↓ [48] | |||
| Heart rate | ↑ [50] | |||
| Retinal diameter | [46] | |||
| Sleep duration | [49] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mnich, C.; Weyland, S.; Jekauc, D.; Schipperijn, J. Psychosocial and Physiological Health Outcomes of Green Exercise in Children and Adolescents—A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 4266. https://doi.org/10.3390/ijerph16214266
Mnich C, Weyland S, Jekauc D, Schipperijn J. Psychosocial and Physiological Health Outcomes of Green Exercise in Children and Adolescents—A Systematic Review. International Journal of Environmental Research and Public Health. 2019; 16(21):4266. https://doi.org/10.3390/ijerph16214266
Chicago/Turabian StyleMnich, Carina, Susanne Weyland, Darko Jekauc, and Jasper Schipperijn. 2019. "Psychosocial and Physiological Health Outcomes of Green Exercise in Children and Adolescents—A Systematic Review" International Journal of Environmental Research and Public Health 16, no. 21: 4266. https://doi.org/10.3390/ijerph16214266
APA StyleMnich, C., Weyland, S., Jekauc, D., & Schipperijn, J. (2019). Psychosocial and Physiological Health Outcomes of Green Exercise in Children and Adolescents—A Systematic Review. International Journal of Environmental Research and Public Health, 16(21), 4266. https://doi.org/10.3390/ijerph16214266