Assessment of Socio-Demographic Factors, Mother and Child Health Status, Water, Sanitation, and Hygienic Conditions Existing in a Hilly Rural Village of Nepal

 , ,
, , 
 and
and 
Abstract
:1. Introduction
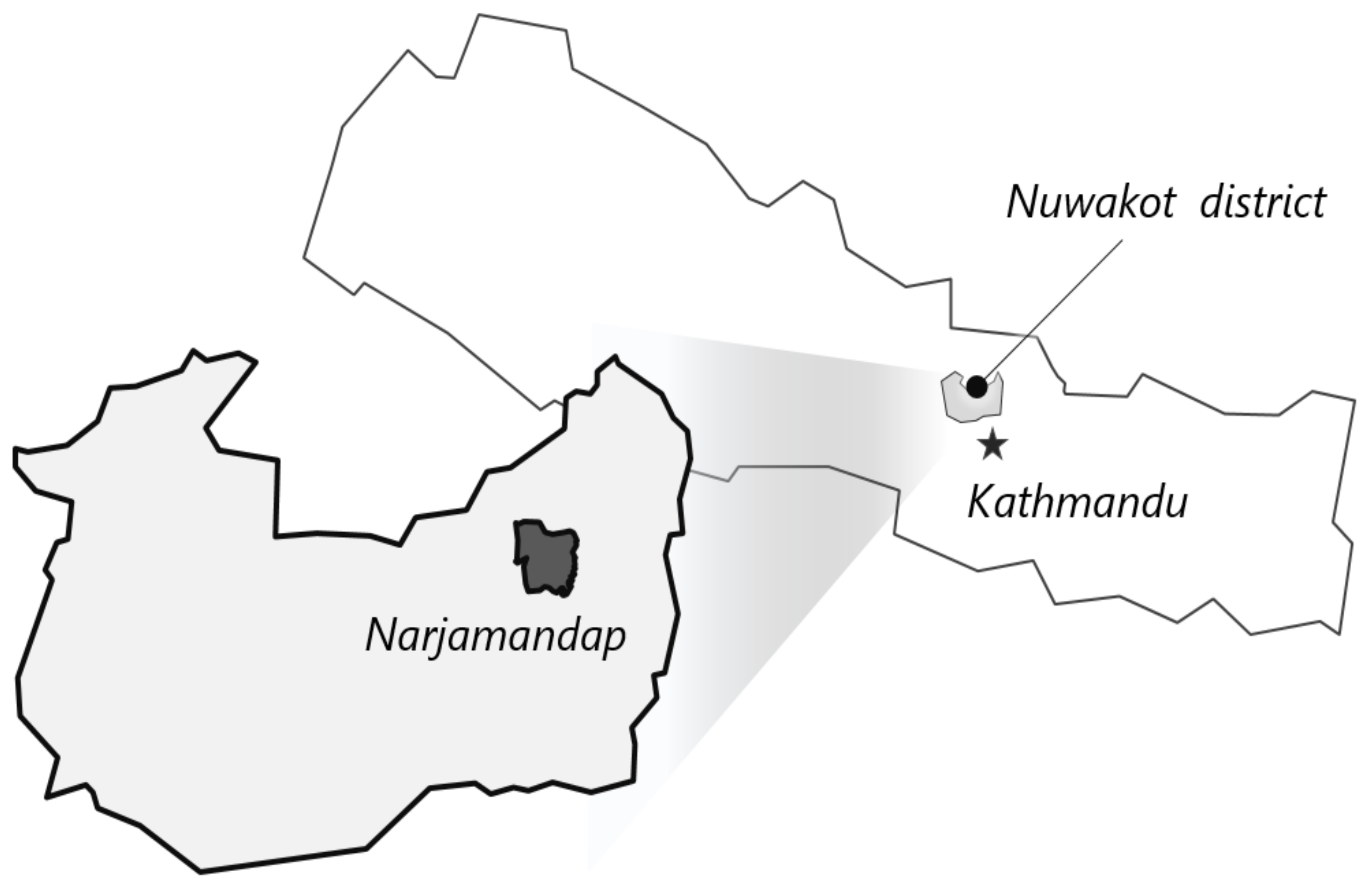
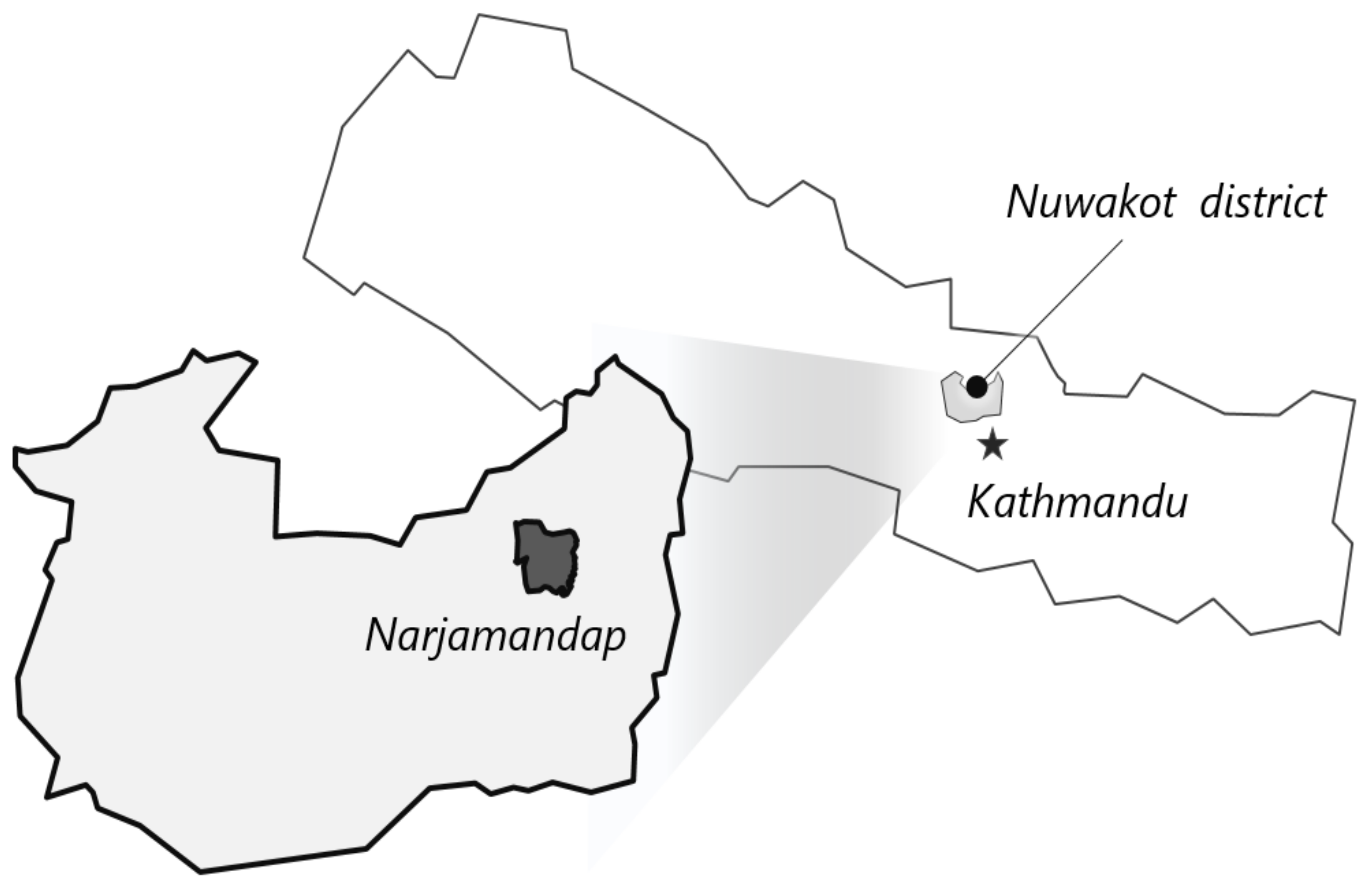
- To describe the demographic and household characteristics in Narjamandap Village.
- To describe the mother and child health status particularly related to antenatal care and routine immunization in Narjamandap Village.
- To understand the water, sanitation and hygiene (WASH)status in Narjamandap Village.
- To identify factors associated with MCH status.
- To identify factors associated with the occurrence of diarrheal and febrile disease.
- To assess the usage of smart phones and SNSs by the local population.
- To generate recommendations to improve the existing MCH care in Nepal by identifying the gaps in system, delivery, and care.
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Data Collection
2.4. Data Analysis
3. Results
3.1. Socio-Demographic Characteristics
3.2. Water, Sanitation, and Hygiene Characteristics
3.3. Maternal and Child Health Characteristics
3.4. Factors Associated with Acute Diarrhea and Fever
3.5. Factors Associated with Full Antenatal and Under-Five Child Immunization
4. Discussion
5. Conclusions
- The existing health care delivery system must be strengthened to reach all communities in a timely manner.
- Ways to minimize the time gap between the discovery of symptoms, reporting, and action must be clearly planned. This could be in done economically, technologically, via infrastructure (e.g., use of drones to provide medical supplies for areas that are geographically isolated, or using telemedicine to guide actions, online data entry and disseminating services) or travelling facilities for local level workers.
- In addition, professional health care monitoring teams (experts) must be deployed promptly to further investigate any cases of complications during pregnancy, under-five deaths, missed vaccinations, etc. These must be reported and appropriate actions must be taken promptly.
- Health care delivery for people living in geographically difficult terrains must be strengthened.
- In areas like our study setting, where there is an advantage of having uninterrupted power supply most of the time, the government must allocate resources and personnel for training and using technology to document, report, and monitor the health status of the community.
- Innovative use of mobile technology and social networking sites must be explored to promote the health of the community.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. The Top Ten Causes OF Death. 2017. Available online: http://www.who.int/mediacentre/factsheets/fs310/en/index1.html (accessed on 20 July 2017).
- Fischer Walker, C.L.; Rudan, I.; Liu, L.; Nair, H.; Theodoratou, E.; Bhutta, Z.A.; O’Brien, P.K.; Campbell, P.H.; Black, R.E. Global burden of childhood pneumonia and diarrhoea. Lancet 2013, 381, 1405–1416. [Google Scholar] [CrossRef]
- Ministry of Health; New ERA; ICF. Nepal Demographic and Health Survey 2016; Ministry of Health: Kathmandu, Nepal, 2017. [Google Scholar]
- WCO Nepal. Health System in Nepal: Challenges and Strategic Options. WCO Nepal 2007. Available online: https://apps.who.int/iris/handle/10665/205257 (accessed on 10 October 2019).
- Rural Population. 2017. Available online: http://data.worldbank.org/indicator/SP.RUR.TOTL.ZS (accessed on 20 July 2005).
- World Health Organization. Achieving the health-related MDGs. In It Takes a Workforce; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Bank. Indicators. Available online: http://data.worldbank.org/indicator (accessed on 24 May 2017).
- Mahara, G.; Barr, J.; Thomas, J.; Wang, W.; Guo, X. Maternal health and its affecting factors in Nepal. Fam. Med. Commun. Health 2016, 4, 30–34. [Google Scholar] [CrossRef]
- UNICEF. Nepal. Available online: https://www.unicef.org/infobycountry/nepal_nepal_background.html (accessed on 1 May 2017).
- Dawson, P.; Pradhan, Y.V.; Houston, R.; Karki, S.; Poudel, D.; Hodgins, S. From research to national expansion: 20 Years’ experience of community-based management of childhood pneumonia in Nepal. Bull. World Health Organ. 2008, 86, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, R. Child Healthcare in Nepal: Progress and Direction. Am. J. Public Health Res. 2015, 3, 74–80. [Google Scholar] [CrossRef] [Green Version]
- Hughes, M.M.; Katz, J.; Englund, J.A.; Khatry, S.K.; Shrestha, L.; LeClerq, S.C.; Steinhoff, M.; Tielsch, J.M. Infant vaccination timing: Beyond traditional coverage metrics for maximizing impact of vaccine programs, an example from southern Nepal. Vaccine 2016, 34, 933–941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrestha, R. Maternal Mortality in Nepal: Addressing the Issue. Inq. J. 2012, 4, 1–4. [Google Scholar]
- Karkee, R.; Comfort, J. NGOs, Foreign Aid, and Development in Nepal. Front. Public Health 2016, 4, 177. [Google Scholar] [CrossRef] [PubMed]
- Laranjo, L.; Arguel, A.; Neves, A.L.; Gallagher, A.M.; Kaplan, R.; Mortimer, N.; Lau, A.Y.S. The influence of social networking sites on health behavior change: A systematic review and meta-analysis. J. Am. Med. Inf. Assoc. 2014, 22, 243–256. [Google Scholar] [CrossRef] [PubMed]
- Rayamajhi, R.B.; Budhathoki, S.S.; Ghimire, A.; Niraula, S.R.; Khanal, V.K.; Neupane, B.; Shakya, P.P. Original Research Article a Study on Sanitary and Hygiene Practices. J. Chitwan Med. Coll. 2014, 4, 20–24. [Google Scholar] [CrossRef]
- Ogunsola, F.; Balogun, M.; Aigbefo, S.; Oduyebo, O. Perception and practice of hand washing in Kuramo Community, Lagos, Nigeria. Int. J. Infect. Control 2013, 9, 1–8. [Google Scholar] [CrossRef]
- Karn, R.R.; Bhandari, B.; Jha, N. A Study on Personal Hygiene and Sanitary Practices in a Rural Village of Mornag District of Nepal. J. Nobel Med. Coll. 2011, 1, 39–44. [Google Scholar] [CrossRef]
- Schwarz, D.; Sharma, R.; Bashyal, C.; Schwarz, R.; Baruwal, A.; Karelas, G.; Basnet, B.; Khadka, N.; Brady, J.; Silver, Z.; et al. Strengthening Nepal’s Female Community Health Volunteer network: A qualitative study of experiences at two years. BMC Health Serv. Res. 2014, 14, 473. [Google Scholar] [CrossRef] [PubMed]
- Khatri, R.B.; Mishra, S.R.; Khanal, V. Female Community Health Volunteers in Community-Based Health Programs of Nepal: Future Perspective. Front. Public Health 2017, 5, 181. [Google Scholar] [CrossRef] [PubMed]
- Budhathoki, S.S.; Bhattachan, M.; Yadav, A.K.; Upadhyaya, P.; Pokharel, P.K. Eco-social and behavioural determinants of diarrhoea in under-five children of Nepal: A framework analysis of the existing literature. Trop. Med. Health 2016, 44, 7. [Google Scholar] [CrossRef] [PubMed]
- Anteneh, Z.A.; Andargie, K.; Tarekegn, M. Prevalence and determinants of acute diarrhea among children younger than five years old in Jabithennan District, Northwest Ethiopia, 2014. BMC Public Health 2017, 17, 99. [Google Scholar] [CrossRef] [PubMed]
- Woldu, W.; Bitew, B.D.; Gizaw, Z. Socioeconomic factors associated with diarrheal diseases among under-five children of the nomadic population in northeast Ethiopia. Trop. Med. Health 2016, 44, 40. [Google Scholar] [CrossRef] [PubMed]
- Sinmegn, M.T.; Asres, A.G.; Shimeka, T.A. Determinants of childhood diarrhea among underfive children in Benishangul Gumuz Regional State, North West Ethiopia. BMC Pediatr. 2014, 14, 102. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, B.; Lee, K.T.; Chu, W.S.; Lee, C.S.; Song, C.K.; Bhandari, P.; Ahn, S.H. Socio-economic impact of renewable energy-based power system in mountainous villages of Nepal. Int. J. Precis. Eng. Manuf. Green Technol. 2017, 4, 37–44. [Google Scholar] [CrossRef]

{kind=link}
| Variables | N | n (%) | Mean (SD) |
|---|---|---|---|
| Age | 25.44 (5.93) | ||
| Ethnic group | 301 | ||
| Dalit | 22 (7.3) | ||
| Tamang/Lama/Gurung | 171 (56.8) | ||
| Brahmin/Chettri | 105 (34.9) | ||
| Newar | 3 (1) | ||
| Occupation | 315 | ||
| Housewife | 70 (22.2) | ||
| Farmer | 47 (14.9) | ||
| Shopkeeper | 3 (1.0) | ||
| Teacher | 3 (1.0) | ||
| Tailor | 2 (0.6) | ||
| Housewife & part time income generating worker * | 187 ((59.7) | ||
| Farmer & other part time work | 3 ( (0.9) | ||
| Ability to read & write | 308 | ||
| Yes | 239 (77.6) | ||
| No | 69 (22.4) | ||
| Highest level of education | 256 | ||
| Informal education | 50 (19.5) | ||
| Primary school (Grade 1–5) | 62 (24.2) | ||
| Middle school (Grades 6–8) | 55 (21.5) | ||
| Secondary (Grades 9 & 10) | 51 (19.9) | ||
| High school(Grades 11 & 12) | 38 (14.8) | ||
| Fuel used for cooking | 287 | ||
| Firewood | 240 (83.6) | ||
| Biogas | 1 (0.3) | ||
| Firewood & other sources (kerosene, biogas, electricity) | 46 (16) | ||
| Daily source of lighting | 293 | ||
| Electricity | 260 (88.7) | ||
| Kerosene | 2 (0.7) | ||
| Electricity & kerosene/candle | 31 (10.6) |
| Variables | N | n (%) |
|---|---|---|
| Sick with acute diarrhea in past 4 weeks | 315 | |
| Yes | 68 (21.6) | |
| No | 247 (78.4) | |
| Sick with fever in past 4 weeks | 315 | |
| Yes | 111 (35.2) | |
| No | 204 ( 64.8) | |
| Main source of drinking water * | 293 | |
| Improved sources | 268 (91.5) | |
| Unimproved sources | 25 (8.5) | |
| Water treatment | 315 | |
| Yes | 10 (3.2) | |
| No | 305 (96.8) | |
| Type of water treatment | 10 | |
| Boil | 6 (60) | |
| Add chlorine | 2 (20) | |
| Water filter | 2 (20) | |
| Toilet facility | 315 | |
| Yes | 191 (60.6) | |
| No | 124 (39.4) | |
| Type of toilet | 187 | |
| Flush toilet with public sewerage | 30 (16) | |
| Flush toilet with septic tank | 76 (406) | |
| Outdoor pit latrine | 81 (43.3) | |
| Hand washing practice before handling food | 293 | |
| Soap & water | 159 (54.3) | |
| Water only | 102 (34.8) | |
| Mud/Ash/Sand | 1 (0.3) | |
| Both Soap & water & water only | 18 (6.1) | |
| Water only & mud/ash/sand | 6 (2.0) | |
| Soap & water, water only & mud/ash/sand | 1 (0.3) | |
| Hand washing practice before eating | 293 | |
| Soap & water | 175 (59.7) | |
| Water only | 101 (34.5) | |
| Mud/ash/sand | 2 (0.7) | |
| Soap & water & water only | 9 (3.1) | |
| Soap & water & mud/ash/sand | 6 (2.0) | |
| Hand washing practice after visiting toilet | 293 | |
| Soap & water | 254 (86.7) | |
| Water only | 11 (3.8) | |
| Mud/ash/sand | 12 (4.1) | |
| Soap & water & water only | 7 (2.4) | |
| Soap & water & mud/ash/sand | 9 (3.1) |
| Variables | N | n (%) | Mean (SD) |
|---|---|---|---|
| Age at marriage | 278 | 19.04 (3.45) | |
| Age at first childbirth | 278 | 20.74 (3.44) | |
| Total surviving children | 293 | 1.58 (1.28) | |
| TT vaccine for recent pregnancy | 315 | ||
| Yes | 257 (81.6) | ||
| No | 58 (18.4) | ||
| TT vaccine dose | 254 | ||
| One dose | 3 (1.2) | ||
| Two doses | 251 (98.8) | ||
| Missing data | 61 | ||
| Antenatal care during pregnancy | 315 | ||
| Regular | 250 (79.4) | ||
| Less than three visits | 39 (12.4) | ||
| None | 26 (8.3) | ||
| Type of delivery | |||
| Normal vaginal delivery | 315 | 298 (94.6) | |
| Assisted delivery (vacuum cup/forceps) | 1 (0.3) | ||
| Caesarean section | 16 (5.1) | ||
| Place of delivery | 315 | ||
| Home | 164 (52.1) | ||
| Health post | 66 (21.0) | ||
| Private clinic | 7 (2.2) | ||
| Hospital | 78 (24.8) | ||
| Immunization card | 290 | ||
| Yes | 137 (47.2) | ||
| No | 153 (52.8) | ||
| BCG | 206 | ||
| Yes | 199 (96.6) | ||
| No | 7 (3.4) | ||
| BCG scar | 277 | ||
| Yes | 233 (84.1) | ||
| No | 44 (15.1) | ||
| Place of immunization | 230 | ||
| Health post | 133 (57.8) | ||
| Booth | 93 (40.4) | ||
| Private clinic | 4 (1.7) |
| Variables | Odd Ratio Estimate | 95% Wald Confidence Limits | P Value |
|---|---|---|---|
| Education Primary education | 1 | ||
| Illiterate | 0.53 | 0.27–1.06 | 0.07 |
| Secondary Education | 0.55 | 0.31–0.97 | 0.04 |
| High School | 0.21 | 0.08–0.56 | 0.001 |
| Housewife | 1.67 | 0.87–3.20 | 0.12 |
| Shopkeeper | 0.27 | 0.08–0.83 | 0.02 |
| Source of drinking water Improved Vs. Unimproved | 3.07 | 1.38–6.81 | 0.005 |
| Toilet facility | 0.49 | 0.28–85 | 0.01 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhandari, P.; Bak, J.; Lee, K.-S.; Chon, Y.; Bhattachan, A.; Rimal, P.; Shrestha, B.R.; Bhandari, B.; Moon, J.-O.; Wu, N.; et al. Assessment of Socio-Demographic Factors, Mother and Child Health Status, Water, Sanitation, and Hygienic Conditions Existing in a Hilly Rural Village of Nepal. Int. J. Environ. Res. Public Health 2019, 16, 3965. https://doi.org/10.3390/ijerph16203965
Bhandari P, Bak J, Lee K-S, Chon Y, Bhattachan A, Rimal P, Shrestha BR, Bhandari B, Moon J-O, Wu N, et al. Assessment of Socio-Demographic Factors, Mother and Child Health Status, Water, Sanitation, and Hygienic Conditions Existing in a Hilly Rural Village of Nepal. International Journal of Environmental Research and Public Health. 2019; 16(20):3965. https://doi.org/10.3390/ijerph16203965
Chicago/Turabian StyleBhandari, Pratibha, JeongEun Bak, Kang-Sung Lee, Yun Chon, Anuj Bhattachan, Pradip Rimal, Biswo Ram Shrestha, Binayak Bhandari, Jeong-Ook Moon, Namkyu Wu, and et al. 2019. "Assessment of Socio-Demographic Factors, Mother and Child Health Status, Water, Sanitation, and Hygienic Conditions Existing in a Hilly Rural Village of Nepal" International Journal of Environmental Research and Public Health 16, no. 20: 3965. https://doi.org/10.3390/ijerph16203965
APA StyleBhandari, P., Bak, J., Lee, K.-S., Chon, Y., Bhattachan, A., Rimal, P., Shrestha, B. R., Bhandari, B., Moon, J.-O., Wu, N., Chu, W.-S., Song, C.-K., Lee, C. S., Mogasale, V., & Ahn, S.-H. (2019). Assessment of Socio-Demographic Factors, Mother and Child Health Status, Water, Sanitation, and Hygienic Conditions Existing in a Hilly Rural Village of Nepal. International Journal of Environmental Research and Public Health, 16(20), 3965. https://doi.org/10.3390/ijerph16203965