Can Between-Session Homework Be Delivered Digitally? A Pilot Randomized Clinical Trial of CBT for Adjustment Disorders

 , ,
, ,
Abstract
1. Introduction
2. Method
2.1. Design
2.2. Participants
2.3. Measures
2.3.1. Diagnostic Instrument
2.3.2. Primary Outcomes
2.3.3. Secondary Outcomes
2.3.4. Treatment Satisfaction
2.4. Treatment
CBT AjD Protocol
- (1)
- In the Traditional condition, the homework component is composed of: (1) reading material in the form of brief manuals as reminders of the different therapeutic contents; (2) writing materials in the form of self-registers and exercises in order to practice the contents seen in the therapy sessions in real life; and (3) therapy session audio recordings in order to practice the elaboration/processing of the stressful event.
- (2)
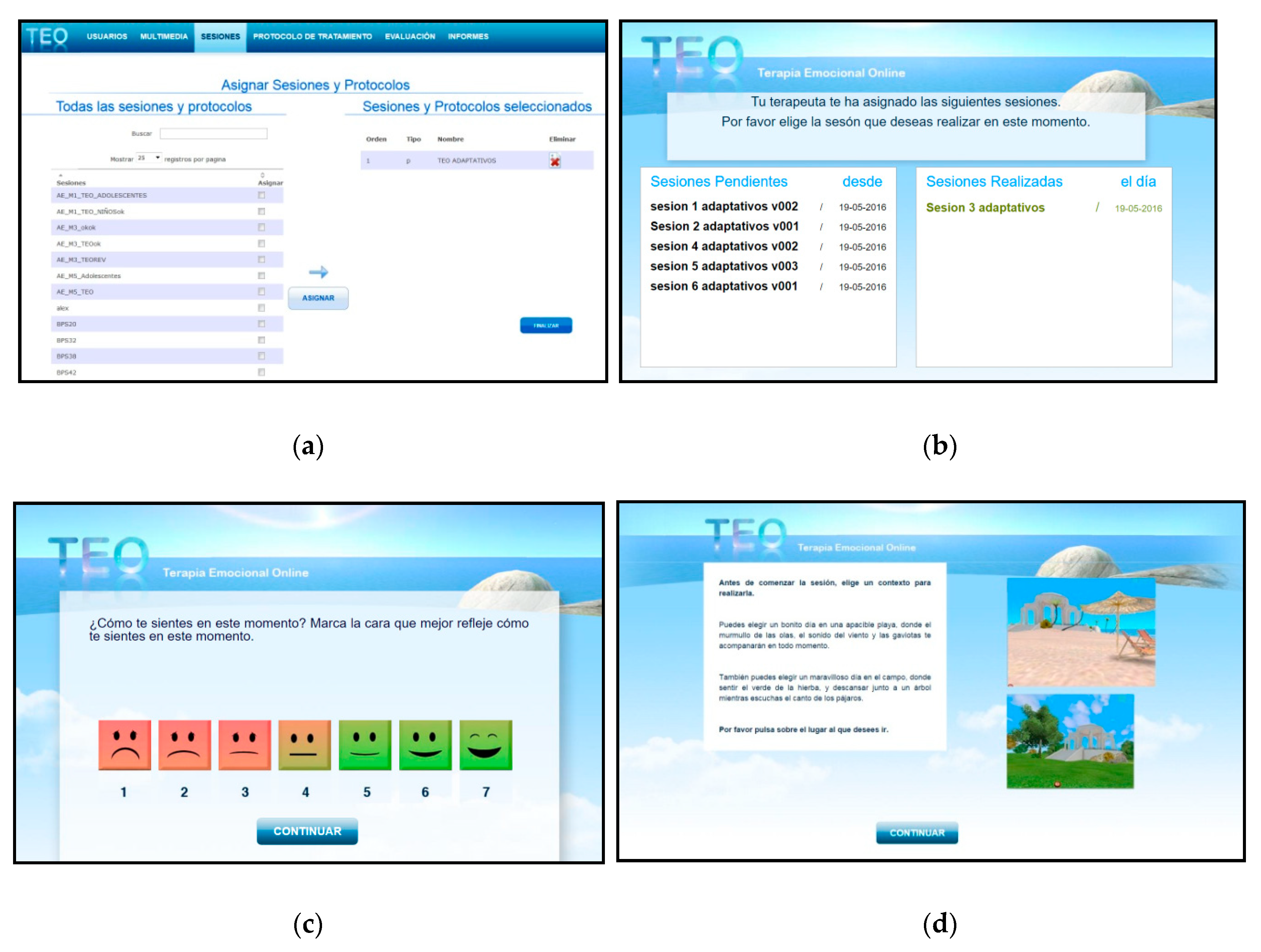
- In the TEO condition, a digital support system was used. TEO is a completely open web-based technology that allows therapists to create and easily send personalized therapeutic material to patients via the Internet (http://www.teo.uji.es). The system has a database with media contents (audio, images, videos, and texts), and the therapists can access these materials and combine them to create homework sessions. TEO is a therapeutic tool developed to complement therapy. In the present study, it is used to administer the homework sessions in the period between the treatment sessions. Therefore, the system is designed to consolidate, support, and improve the therapeutic intervention by assigning homework that can be practiced at home via the Internet. Moreover, through this program, several clinical variables (e.g., mood state or positive and negative emotions) can be assessed before and after each homework session. The therapist can access the reports resulting from a patient’s activity: assessment, content, assigned sessions, completed sessions, dates, etc. The TEO system includes two platforms with different functions:
- Therapist platform: In this platform, the therapist can manage and administer the users and the results of each user’s treatment and create sessions and customize homework protocols using multimedia materials included in the TEO multimedia base (pictures, texts, narratives, music, and videos). These multimedia elements cover the clinical needs of each patient and work on all the therapeutic components included in the AjD protocol. The therapist can view the content created and assign homework sessions (see Figure 2a). Moreover, assessment protocols are assigned to the users and composed of brief questionnaires assessing key clinical variables. The therapist can download the results of these evaluations in order to monitor each patient.
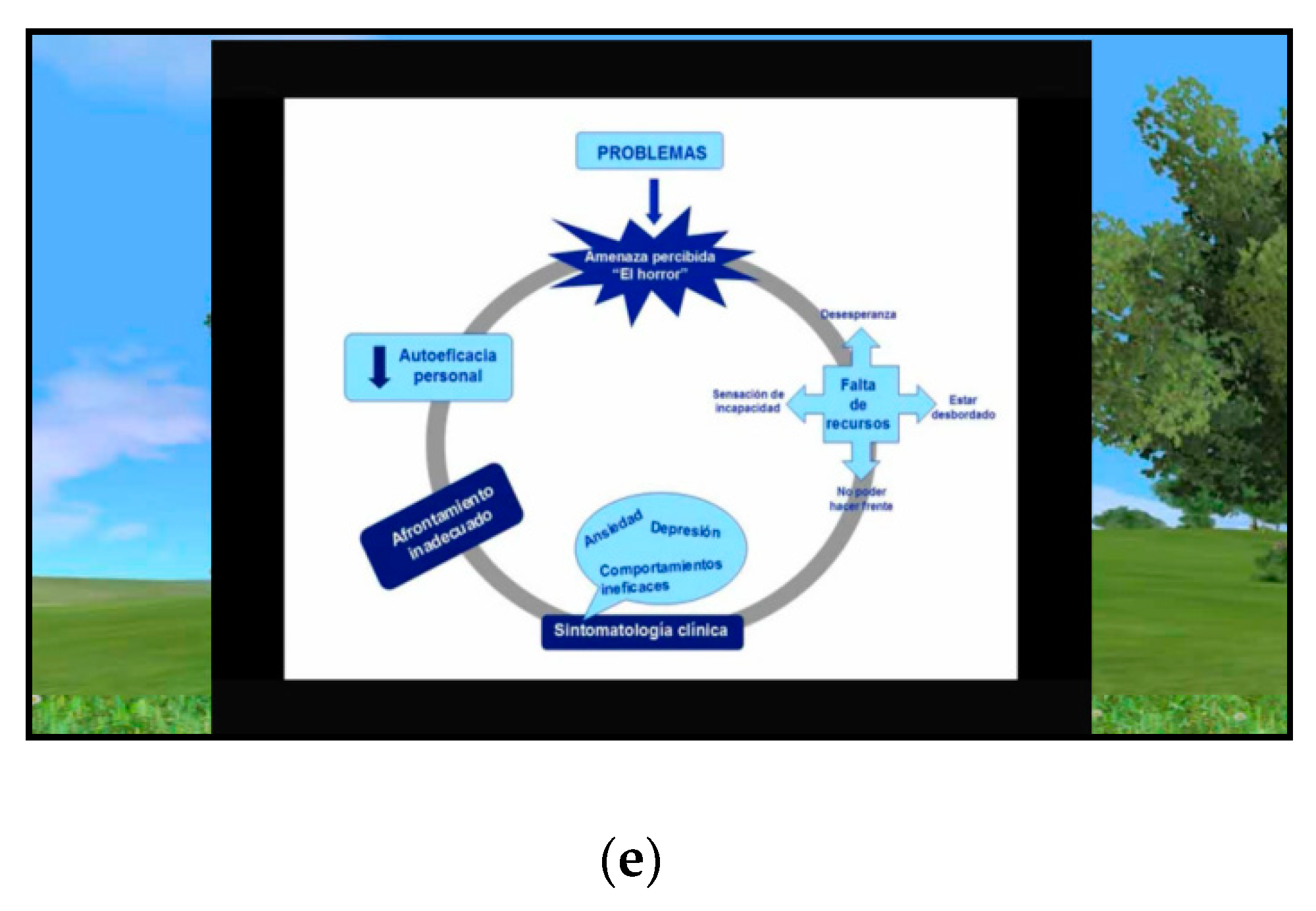
- Patient platform: The main function of the patient platform is to allow the user to receive and view the session assigned and sent by the therapist (see Figure 2b). First, the patients can complete the pre-session assessment protocol (see Figure 2c) and choose a virtual environment (a beach or a forest environment) to go to throughout the homework session (see Figure 2d). This virtual environment also appears at the end of each session, so that the patients can move around to reflect on the session and their experience. Then, they can complete the post-assessment protocol and repeat the session as many times as necessary. In the present study, we used the TEO system to reinforce the treatment components described above. To do so, we designed a homework session component using audios, videos, and images that were available in the TEO system database. Specifically, the TEO system allows access to all the therapeutic material available in EMMA’s world (symbols, audios, and images), with the aim of continuing with the processing/elaboration treatment component from home. Figure 2e presents an example of therapeutic material included in a specific TEO homework session for the treatment of AjD.
2.5. Procedure
2.6. Data Analyses
3. Results
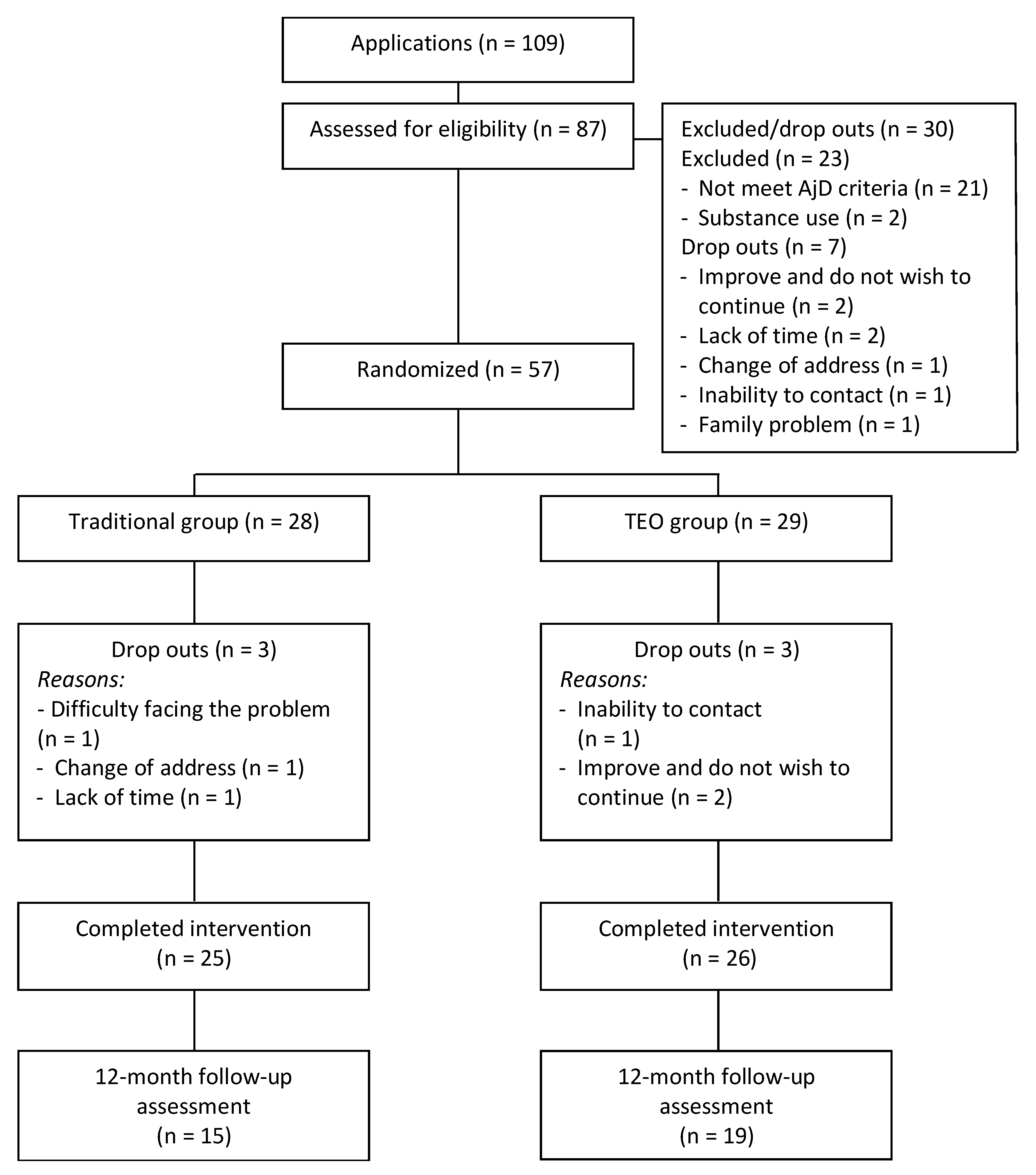
3.1. Participant Flow and Attrition
3.2. Baseline Data and Participants’ Characteristics
3.3. Treatment Efficacy
3.4. Treatment Satisfaction
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Evans, S.C.; Reed, G.M.; Roberts, M.C.; Esparza, P.; Watts, A.D.; Correia, J.M.; Ritchie, P.; Maj, M.; Saxena, S. Psychologists’ perspectives on the diagnostic classification of mental disorders: Results from the WHO-IUPsyS global survey. Int. J. Psychol. 2013, 48, 177–193. [Google Scholar] [CrossRef]
- American Psychological Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; APA: Washington, DC, USA, 2013. [Google Scholar]
- Bachem, R.; Casey, P. Adjustment disorder: A diagnosis whose time has come. J. Affect. Disord. 2018, 227, 243–253. [Google Scholar] [CrossRef] [PubMed]
- Maercker, A.; Forstmeier, S.; Pielmaier, L.; Spangenberg, L.; Brähler, E.; Glaesmer, H. Adjustment disorders: Prevalence in a representative nationwide survey in Germany. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 1745–1752. [Google Scholar] [CrossRef] [PubMed]
- Perkonigg, A.; Lorenz, L.; Maercker, A. Prevalence and correlates of ICD-11 adjustment disorder: Findings from the Zurich adjustment disorder study. Int. J. Clin. Health Psychol. 2018, 18, 209–217. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). International Classification of Diseases for Mortality and Morbidity Statistics, 11th ed.; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- American Psychological Association (APA). Diagnostic and Statistical Manual for Mental Disorders, 4th ed.; APA: Washington, DC, USA, 2000. [Google Scholar]
- World Health Organization (WHO). The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines; WHO: Geneva, Switzerland, 1992. [Google Scholar]
- Yaseen, Y.A. Adjustment disorder: Prevalence, sociodemographic risk factors, and its subtypes in outpatient psychiatric clinic. Asian J. Psychiatr. 2017, 28, 82–85. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.L.; Agathos, J.A.; Metcalf, O.; Gibson, K.; Lau, W. Adjustment disorder: Current developments and future directions. Int. J. Environ. Res. Public Health 2019, 16, 2537. [Google Scholar] [CrossRef] [PubMed]
- Fernández, A.; Mendive, J.M.; Salvador-Carulla, L.; Rubio-Valera, M.; Luciano, J.V.; Pinto-Meza, A.; Haro, J.M.; Palao, D.J.; Bellón, J.A.; Serrano-Blanco, A.; et al. Adjustment disorders in primary care: Prevalence, recognition and use of services. Br. J. Psychiatry 2012, 201, 137–142. [Google Scholar] [CrossRef]
- O’Donnell, M.L.; Alkemade, N.; Creamer, M.; McFarlane, A.C.; Silove, D.; Bryant, R.A.; Felmingham, K.; Steel, Z.; Forbes, D. A longitudinal study of adjustment disorder after trauma exposure. Am. J. Psychiatry 2016, 173, 1231–1238. [Google Scholar] [CrossRef]
- Calvo, E. Duración de la Incapacidad Temporal Asociada a Diferentes Patologías en Trabajadores Españoles; MTIN (Ministerio de Trabajo e Inmigración), Secretaría de Estado de la Seguridad Social: Madrid, Spain, 2010.
- Casey, P.; Jabbar, F.; O’Leary, E.; Doherty, A.M. Suicidal behaviours in adjustment disorder and depressive episode. J. Affect. Disord. 2015, 174, 441–446. [Google Scholar] [CrossRef]
- Kazlauskas, E.; Zelviene, P.; Lorenz, L.; Quero, S.; Maercker, A. A scoping review of ICD-11 adjustment disorder research. Eur. J. Psychotraumatol. 2017, 8, 1421819. [Google Scholar] [CrossRef]
- O’Donnell, M.L.; Metcalf, O.; Watson, L.; Phelps, A.; Varker, T. A systematic review of psychological and pharmacological treatments for adjustment disorder in adults. J. Trauma Stress 2018, 31, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Arends, I.; Bruinvels, D.J.; Rebergen, D.S.; Nieuwenhuijsen, K.; Madan, I.; Neumeyer-Gromen, A.; Bültmann, U.; Verbeek, J.H. Interventions to facilitate return to work in adults with adjustment disorders. Cochrane Database Syst. Rev. 2012, 12. [Google Scholar] [CrossRef] [PubMed]
- Van der Klink, J.J.L.; Blonk, R.W.B.; Schene, A.H.; van Dijk, F.J.H. Reducing long term sickness absence by an activating intervention in adjustment disorders: A cluster randomised controlled design. Occup. Environ. Med. 2003, 60, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Sundquist, J.; Palmér, K.; Johansson, L.M.; Sundquist, K. The effect of mindfulness group therapy on a broad range of psychiatric symptoms: A randomised controlled trial in primary health care. Eur. Psychiatry 2017, 43, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Botella, C.; Baños, R.M.; Guillén, V. Creciendo en la adversidad. Una propuesta de tratamiento para los trastornos adaptativos. In Psicología Positiva Aplicada; DDB: Bilbao, Spain, 2008. [Google Scholar]
- Baños, R.M.; Guillen, V.; Quero, S.; García-Palacios, A.; Alcaniz, M.; Botella, C. A virtual reality system for the treatment of stress-related disorders: A preliminary analysis of efficacy compared to a standard cognitive behavioral program. Int. J. Hum. Comput. Stud. 2011, 69, 602–613. [Google Scholar] [CrossRef]
- Baños, R.M.; Botella, C.; Guillen, V.; García-Palacios, A.; Quero, S.; Bretón-López, J.; Alcañiz, B. An adaptive display to treat stress-related disorders: EMMA’s World. Br. J. Guid. Counc. 2009, 37, 347–356. [Google Scholar] [CrossRef]
- Quero, S.; Molés, M.; Campos, D.; Andreu-Mateu, S.; Baños, R.M.; Botella, C. An adaptive virtual reality system for the treatment of adjustment disorder and complicated grief: 1-year follow-up efficacy data. Clin. Psychol. Psychother. 2019, 26, 204–217. [Google Scholar] [CrossRef]
- Benbow, A.A.; Anderson, P.L. A meta-analytic examination of attrition in virtual reality exposure therapy for anxiety disorders. J. Anxiety Disord. 2019, 1, 18–26. [Google Scholar] [CrossRef]
- Garcia-Palacios, A.; Botella, C.; Hoffman, H.; Fabregat, S. Comparing acceptance and refusal rates of virtual reality exposure vs. in vivo exposure by patients with specific phobias. Cyberpsychol. Behav. 2007, 10, 722–724. [Google Scholar] [CrossRef]
- Guillén, V.; Baños, R.M.; Botella, C. Users’ opinion about a virtual reality system as an adjunct to psychological treatment for stress-related disorders: A quantitative and qualitative mixed-methods study. Front. Psychol. 2018, 9, 1038. [Google Scholar] [CrossRef]
- Callan, J.A.; Kazantzis, N.; Park, S.Y.; Moore, C.G.; Thase, M.E.; Minhajuddin, A.; Kornblith, S.; Siegle, G.J. A propensity score analysis of homework adherence-outcome relations in cognitive behavioral therapy for depression. Behav. Ther. 2019, 50, 285–299. [Google Scholar] [CrossRef] [PubMed]
- Kazantzis, N.; Luong, H.K.; Usatoff, A.S.; Impala, T.; Yew, R.Y.; Hofmann, S.G. The processes of cognitive behavioral therapy: A review of meta-analyses. Cognit. Ther. Res. 2018, 42, 349–357. [Google Scholar] [CrossRef]
- Kazantzis, N.; Whittington, C.; Dattilio, F. Meta-Analysis of homework effects in cognitive and behavioral therapy: A replication and extension. Clin. Psychol. Sci. Pract. 2010, 17, 144–156. [Google Scholar] [CrossRef]
- Beck, A.T. Cognitive Therapy of Depression; Guilford Press: New York, NY, USA, 1979; 425p. [Google Scholar]
- Johansson, O.; Michel, T.; Andersson, G.; Paxling, B. Experiences of non-adherence to Internet-delivered cognitive behavior therapy: A qualitative study. Internet Interv. 2015, 2, 137–142. [Google Scholar] [CrossRef]
- Strain, J.J.; Diefenbacher, A. The adjustment disorders: The conundrums of the diagnoses. Compr. Psychiatry 2008, 49, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Quero, S.; Mor, S.; Molés, M.; Rachyla, I.; Baños, R.; Botella, C. Exploring the assessment of adjustment disorders: Differences between a general and a clinical sample. Psicothema 2019, 31, 17–23. [Google Scholar]
- Rachyla, I.; Botella, C.; Mor, S.; Tur, C.; López-Montoyo, A.; Quero, S. Diagnostic interview for adjustment disorders: Reliability and validity. submitted.
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J.B.W. Structured Clinical Interview for DSM-IV Axis I Disorders; Clinician Version (SCID-CV); American Psychiatric Press: Washington, DC, USA, 1996. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Sanz, J.; Navarro, M.; Vázquez, C. Adaptación española del inventario para la depresión de Beck-II (BDI-II): 1. Propiedades psicométricas en estudiantes universitarios. Análisis Modif. Conduct. 2003, 29, 239–288. [Google Scholar]
- Prigerson, H.G.; Maciejewski, P.K.; Reynolds, C.F.; Bierhals, A.J.; Newsom, J.T.; Fasiczka, A.; Frank, E.; Doman, J.; Miler, M. Inventory of complicated grief: A scale to measure maladaptive symptoms of loss. Psychiatry Res. 1995, 59, 65–79. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Sandín, B.; Chorot, P.; Lostao, L.; Joiner, T.; Santed, M.A.; Valiente, R.M. Escalas PANAS de afecto positivo y negativo: Validación factorial y convergencia transcultural. Psicothema 1999, 11, 37–51. [Google Scholar]
- Borkovec, T.D.; Nau, S.D. Credibility of analogue therapy rationales. J. Behav. Ther. Exp. Psychiatry 1972, 3, 257–260. [Google Scholar] [CrossRef]
- Botella, C.; Gallego, M.J.; Garcia-Palacios, A.; Baños, R.M.; Quero, S.; Alcañiz, M. The acceptability of an Internet-based self-help treatment for fear of public speaking. Br. J. Guid. Counc. 2009, 37, 297–311. [Google Scholar] [CrossRef]
- Botella, C.; Mira, A.; Moragrega, I.; García-Palacios, A.; Bretón-López, J.; Castilla, D.; Riera López del Amo, A.; Soler, C.; Molinari, G.; Quero, S.; et al. An Internet-based program for depression using activity and physiological sensors: Efficacy, expectations, satisfaction, and ease of use. Neuropsychiatr. Dis. Treat. 2016, 12, 393–406. [Google Scholar] [CrossRef]
- Quero, S.; Pérez-Ara, M.Á.; Bretón-López, J.; García-Palacios, A.; Baños, R.M.; Botella, C. Acceptability of virtual reality interoceptive exposure for the treatment of panic disorder with agoraphobia. Br. J. Guid. Counc. 2014, 42, 123–137. [Google Scholar] [CrossRef]
- Neimeyer, R.A. Lessons of Loss; Center for the Study of Loss and Transition: Keystone Heights, FL, USA, 2000. [Google Scholar]
- Botella, C.; Baños, R.; Rey, B.; Alcañiz, M.; Guillen, V.; Quero, S.; García-Palacios, A. Using an Adaptive Display for the Treatment of Emotional Disorders. In Proceedings of the CHI 2006, Conference on Human Factors in Computing Systems, Montréal, QU, Canada, 24–27 April 2006; pp. 586–591. [Google Scholar]
- Botella, C.; Quero, S.; Lasso de la Vega, N.; Baños, R.M.; Guillén, V.; García Palacios, A.; Castilla, D. Clinical issues in the application of virtual reality to treatment of PTSD. In Novel Approaches to the Diagnosis and Treatment of Posttraumatic Stress Disorder; IOS Press: Amsterdam, The Netherlands, 2006; pp. 183–195. [Google Scholar]
- Popper, K. La Responsabilidad de Vivir; Paidós: Barcelona, Spain, 1995. [Google Scholar]
- Peterson, C.; Seligman, M.E.P. Character Strengths and Virtues: A Handbook and Classification; American Psychological Association: Washington, DC, USA, 2004; 800p. [Google Scholar]
- Salim, A.; Mackinnon, A.; Christensen, H.; Griffiths, K. Comparison of data analysis strategies for intent-to-treat analysis in pre-test–post-test designs with substantial dropout rates. Psychiatry Res. 2008, 160, 335–345. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: New York, NY, USA, 1988. [Google Scholar]
- Jacobson, N.S.; Truax, P. Clinical significance: A statistical approach to denning meaningful change in psychotherapy research. J. Consult. Clin. Psychol. 1991, 59, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W.; Tetzlaff, J.M.; Gotzsche, P.C.; Altman, D.G.; Mann, H.; Berlin, J.A.; Dickersin, K.; Hróbjartsson, A.; Schulz, K.F.; Parulekar, W.R.; et al. SPIRIT 2013 explanation and elaboration: Guidance for protocols of clinical trials. BMJ 2013, 346, e7586. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jerić, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. SPIRIT 2013 Statement: Defining standard protocol items for clinical trials. Ann. Intern. Med. 2013, 158, 200. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G.; Consolidated Standards of Reporting Trials Group. CONSORT 2010 Explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. J. Clin. Epidemiol. 2010, 63, e1–e37. [Google Scholar] [CrossRef] [PubMed]
- Botella, C.; Serrano, B.; Baños, R.M.; Garcia-Palacios, A. Virtual reality exposure-based therapy for the treatment of post-traumatic stress disorder: A review of its efficacy, the adequacy of the treatment protocol, and its acceptability. Neuropsychiatr. Dis. Treat. 2015, 11, 2533–2545. [Google Scholar] [CrossRef]
- Gonçalves, R.; Pedrozo, A.L.; Coutinho, E.S.F.; Figueira, I.; Ventura, P. Efficacy of virtual reality exposure therapy in the treatment of PTSD: A systematic review. PLoS ONE 2012, 7, e48469. [Google Scholar] [CrossRef] [PubMed]
- Motraghi, T.E.; Seim, R.W.; Meyer, E.C.; Morissette, S.B. Virtual reality exposure therapy for the treatment of posttraumatic stress disorder: A methodological review using CONSORT guidelines. J. Clin. Psychol. 2014, 70, 197–208. [Google Scholar] [CrossRef] [PubMed]
- Botella, C.; García-Palacios, A.; Villa, H.; Baños, R.M.; Quero, S.; Alcañiz, M.; Riva, G. Virtual reality exposure in the treatment of panic disorder and agoraphobia: A controlled study. Clin. Psychol. Psychother. 2007, 14, 164–175. [Google Scholar] [CrossRef]
- Beck, S.; Tompkins, M. Handbook of Homework Assignment in Psychoyherapy; Springer: New York, NY, USA, 2007. [Google Scholar]
- Baños, R.M.; Etchemendy, E.; Mira, A.; Riva, G.; Gaggioli, A.; Botella, C. Online positive interventions to promote well-being and resilience in the adolescent population: A narrative review. Front. Psychiatry 2017, 8, 10. [Google Scholar] [CrossRef] [PubMed]
- Kazdin, A.E. Evidence-based psychotherapies II: Changes in models of treatment and treatment delivery. S. Afr. J. Psychol. 2014, 45, 3–21. [Google Scholar] [CrossRef]
- Kazdin, A.E.; Blase, S.L. Rebooting psychotherapy research and practice to reduce the burden of mental illness. Perspect. Psychol. Sci. 2011, 6, 21–37. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.; Vella-Brodrick, D.; Klein, B. Positive psychology and the internet: A mental health opportunity. Electron. J. Appl. Psychol. 2010, 6, 30–41. [Google Scholar] [CrossRef]
- Rachyla, I.; Quero, S.; Pérez-Ara, M.; Campos, D.; Mira, A. Web-based, self-help intervention for adjustment disorders: Acceptance and usability. Annu. Rev. CyberTherapy Telemed. 2017, 15, 207–210. [Google Scholar]
- Eimontas, J.; Rimsaite, Z.; Gegieckaite, G.; Zelviene, P.; Kazlauskas, E. Internet-Based self-help intervention for ICD-11 adjustment disorder: Preliminary findings. Psychiatr. Q. 2018, 89, 451–460. [Google Scholar] [CrossRef]
- Kazdin, A.E. Addressing the treatment gap: A key challenge for extending evidence-based psychosocial interventions. Behav. Res. Ther. 2017, 88, 7–18. [Google Scholar] [CrossRef]
- Casey, P. Adjustment disorder. CNS Drugs 2009, 23, 927–938. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Traditional Group (N = 28) | TEO Group (N = 29) | |
|---|---|---|
| Age, mean (SD) | 31.71 (11.27) | 28.48 (9.55) |
| Gender, n (%) | ||
| Male | 6 (21.4%) | 8 (27.6%) |
| Female | 22 (78.6%) | 21 (72.4%) |
| Education, n (%) | ||
| Elementary or secondary | 10 (35.7%) | 5 (17.2%) |
| University | 18 (64.3%) | 24 (82.8%) |
| Marital status, n (%) | ||
| Single | 16 (57.1%) | 25 (86.2%) |
| Married/partnered | 8 (28.6%) | 2 (6.9%) |
| Widowed/divorced | 4 (14.3%) | 2 (6.9%) |
| Medication, n (%) | ||
| Yes | 7 (25.9%) | 3 (10.7%) |
| No | 20 (74.1%) | 25 (89.3%) |
| Months since symptom onset, mean (SD) | 29.00 (44.23) | 20.03 (31.41) |
| Homework | |
|---|---|
| 1 | Treatment explanation |
| The impact of stressful events | |
| Cognitive Model of AjD (part I) | |
| Logic of using the Book of Life and EMMA’s world | |
| 2 | Explanation if the exposure and elaboration techniques |
| Breathing exercises (optional) | |
| Elaboration of stressful event practice | |
| Self-exposure tasks to the first item in the exposure hierarchy | |
| 3 | Elaboration practice |
| “Positive” meaning of problems (Part I) | |
| Breathing exercises (optional) | |
| Self-exposure tasks | |
| 4 | Elaboration practices |
| “Positive” meaning of problems (Part II) | |
| Self-exposure tasks | |
| 5 | Elaboration practices |
| Cognitive Model of AjD (Part II) | |
| “Letter to my future self” | |
| 6 | Practice of a new “metaphorical description” of the stressful event in EMMA’s world |
| Choose of search for a heuristic/proverb to apply in everyday situations |
| BL Mean (SD) | Post Mean (SD) | Baseline vs. Post-Treatment | ||||
|---|---|---|---|---|---|---|
| Within-Group d [95% CI] | Within-Group Comparison | Between-Group d [95% CI] | Between-Group Comparison | |||
| BDI | ||||||
| Traditional group | 24.18 (8.91) (n = 28) | 4.91 (3.93) (n = 24) | 2.09 [1.34; 2.85] | F1, 50.61 = 119.80, ρ = 0.000 ** | 0.36 [−0.92; 0.20] | F1, 91.39 = 0.52, ρ = 0.473 |
| TEO group | 22.48 (10.86) (n = 29) | 7.19 (7.68) (n = 26) | 1.37 [0.81; 1.92] | F1, 49.75 = 86.82, ρ = 0.000 ** | ||
| SLI | ||||||
| Traditional group | 35.38 (11.97) (n = 28) | 15.87 (11.18) (n = 24) | 1.58 [0.95; 2.20] | F1, 49.75 = 75.07, ρ = 0.000 ** | 0.11 [−0.67; 0.44] | F1, 85.79 = 0.03, ρ = 0.862 |
| TEO group | 37.22 (10.58) (n = 29) | 17.15 (11.43) (n = 26) | 1.84 [1.18; 2.50] | F1, 49.02 = 102.87, ρ = 0.000 ** | ||
| PANAS + | ||||||
| Traditional group | 22.64 (6.95) (n = 28) | 32.68 (7.34) (n = 25) | 1.40 [−1.97; −0.82] | F1, 49.84 = 41.04, ρ = 0.000 ** | 0.30 [-0.25; 0.86] | F1, 90.08 = 0.84, ρ = 0.362 |
| TEO group | 21.91 (8.45) (n = 29) | 30.20 (8.63) (n = 25) | 0.95 [−1.44; −0.46] | F1, 50.49 = 31.50, ρ = 0.000 ** | ||
| PANAS - | ||||||
| Traditional group | 27.30 (7.69) (n = 28) | 16.84 (5.96) (n = 25) | 1.32 [0.76; 1.88] | F1, 47.44 = 43.76, ρ = 0.000 ** | 0.11 [−0.66; 0.45] | F1, 93.73 = 0.01, ρ = 0.909 |
| TEO group | 25.86 (8.33) (n = 29) | 17.48 (5.75) (n = 25) | 0.97 [0.48; 1.47] | F1, 48.18 = 30.93, ρ = 0.000 ** | ||
| 9 | Post Mean (SD) | Fup Mean (SD) | Post-Treatment vs. Follow-Up | |||
|---|---|---|---|---|---|---|
| Within-Group d [95% CI] | Within-Group Comparison | Between-Group d [95% CI] | Between-Group Comparison | |||
| BDI | ||||||
| Traditional group | 4.91 (3.93) (n = 24) | 2.00 (2.17) (n = 15) | 0.70 [0.11; 1.29] | F1, 34.22 = 3.91, ρ = 0.056 | 0.44 [−1.13; 0.24] | F1, 78.26 = 1.38, ρ = 0.244 |
| TEO group | 7.19 (7.68) (n = 26) | 4.05 (5.69) (n = 19) | 0.39 [−0.09; 0.87] | F1, 32.25 = 5.07, ρ = 0.031 * | ||
| SLI | ||||||
| Traditional group | 15.87 (11.18) (n = 24) | 5.33 (4.17) (n = 15) | 0.89 [0.26; 1.52] | F1, 31.14 = 19.28, ρ = 0.000 ** | 0.43 [−1.12; 0.25] | F1, 76.17 = 1.18, ρ = 0.282 |
| TEO group | 17.15 (11.43) (n = 26) | 8.09 (7.49) (n = 19) | 0.76 [0.23; 1.29] | F1, 29.59 = 14.37, ρ = 0.001 ** | ||
| PANAS + | ||||||
| Traditional group | 32.68 (7.34) (n = 25) | 39.13 (8.40) (n = 15) | 0.83 [−1.45; −0.21] | F1, 41.46 = 7.67, ρ = 0.008 ** | 0.40 [−0.28; 1.09] | F1, 79.68 = 1.96, ρ = 0.165 |
| TEO group | 30.20 (8.63) (n = 25) | 35.47 (9.25) (n = 19) | 0.58 [−1.09; −0.08] | F1, 37.36 = 5.40, ρ = 0.026 * | ||
| PANAS - | ||||||
| Traditional group | 16.84 (5.96) (n = 25) | 13.73 (2.89) (n = 15) | 0.49 [−0.06; 1.05] | F1, 36.48 = 4.23, ρ = 0.047 * | 0.45 [−1.14; 0.23] | F1, 79.34 = 1.21, ρ = 0.276 |
| TEO group | 17.48 (5.75) (n = 25) | 15.63 (4.83) (n = 19) | 0.31 [−0.16; 0.78] | F1, 32.78 = 1.56, ρ = 0.220 | ||
| Post M (SD) | Fup M (SD) | |||
|---|---|---|---|---|
| Traditional Group | TEO Group | Traditional Group | TEO Group | |
| Treatment was logical | 8.80 (0.82) | 8.96 (1.00) | 9.00 (1.16) | 9.00 (0.91) |
| Treatment was satisfactory | 9.24 (0.78) | 9.13 (1.15) | 9.46 (0.97) | 9.11 (1.18) |
| Would recommend the treatment | 9.44 (0.71) | 9.33 (0.87) | 9.31 (0.86) | 9.39 (0.85) |
| Treatment was useful for the problem | 9.28 (0.68) | 9.00 (1.14) | 9.54 (0.97) | 9.00 (1.33) |
| Treatment was useful for other problems | 8.56 (1.12) | 8.71 (1.12) | 8.77 (1.01) | 8.89 (1.37) |
| Treatment Satisfaction at Post-Treatment | Treatment Satisfaction at 12-Month Follow-Up | |||||||
|---|---|---|---|---|---|---|---|---|
| R2 | β | t | ρ | R2 | β | t | ρ | |
| BDI | ||||||||
| Traditional group | 0.19 | −0.47 | −2.50 | 0.021 * | 0.20 | −0.51 | −1.98 | 0.074 |
| TEO group | 0.08 | −0.35 | −1.73 | 0.099 | 0.00 | −0.25 | −1.03 | 0.319 |
| Total | 0.12 | −0.37 | −2.72 | 0.009 ** | 0.08 | −0.34 | −1.92 | 0.065 |
| SLI | ||||||||
| Traditional group | −0.05 | −0.03 | −0.14 | 0.892 | 0.39 | −0.67 | −2.97 | 0.013 * |
| TEO group | 0.22 | −0.50 | −2.72 | 0.013 * | 0.08 | −0.37 | −1.57 | 0.136 |
| Total | 0.10 | −0.34 | −2.45 | 0.018 * | 0.20 | −0.48 | −2.92 | 0.007 ** |
| PANAS+ | ||||||||
| Traditional group | 0.11 | 0.38 | 1.99 | 0.059 | 0.47 | 0.72 | 3.42 | 0.006 ** |
| TEO group | 0.11 | 0.39 | 1.97 | 0.062 | −0.01 | 0.22 | 0.90 | 0.380 |
| Total | 0.12 | 0.37 | 2.73 | 0.009 ** | 0.14 | 0.41 | 2.42 | 0.022 * |
| PANAS- | ||||||||
| Traditional group | −0.04 | −0.02 | −0.08 | 0.938 | 0.05 | −0.36 | −1.29 | 0.225 |
| TEO group | 0.21 | −0.49 | −2.64 | 0.015 * | 0.03 | −0.30 | −1.25 | 0.230 |
| Total | 0.05 | −0.26 | −1.82 | 0.075 | 0.07 | −0.32 | −1.81 | 0.080 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quero, S.; Rachyla, I.; Molés, M.; Mor, S.; Tur, C.; Cuijpers, P.; López-Montoyo, A.; Botella, C. Can Between-Session Homework Be Delivered Digitally? A Pilot Randomized Clinical Trial of CBT for Adjustment Disorders. Int. J. Environ. Res. Public Health 2019, 16, 3842. https://doi.org/10.3390/ijerph16203842
Quero S, Rachyla I, Molés M, Mor S, Tur C, Cuijpers P, López-Montoyo A, Botella C. Can Between-Session Homework Be Delivered Digitally? A Pilot Randomized Clinical Trial of CBT for Adjustment Disorders. International Journal of Environmental Research and Public Health. 2019; 16(20):3842. https://doi.org/10.3390/ijerph16203842
Chicago/Turabian StyleQuero, Soledad, Iryna Rachyla, Mar Molés, Sonia Mor, Cintia Tur, Pim Cuijpers, Alba López-Montoyo, and Cristina Botella. 2019. "Can Between-Session Homework Be Delivered Digitally? A Pilot Randomized Clinical Trial of CBT for Adjustment Disorders" International Journal of Environmental Research and Public Health 16, no. 20: 3842. https://doi.org/10.3390/ijerph16203842
APA StyleQuero, S., Rachyla, I., Molés, M., Mor, S., Tur, C., Cuijpers, P., López-Montoyo, A., & Botella, C. (2019). Can Between-Session Homework Be Delivered Digitally? A Pilot Randomized Clinical Trial of CBT for Adjustment Disorders. International Journal of Environmental Research and Public Health, 16(20), 3842. https://doi.org/10.3390/ijerph16203842