Causes of Delays during Housing Adaptation for Healthy Aging in the UK


Abstract
1. Introduction
2. Research Methods
2.1. Sampling and Participants
2.2. Data Collection
2.3. Data Analysis
2.4. Ethics
3. Results
3.1. Overall Average Waiting Time
3.2. Case Studies
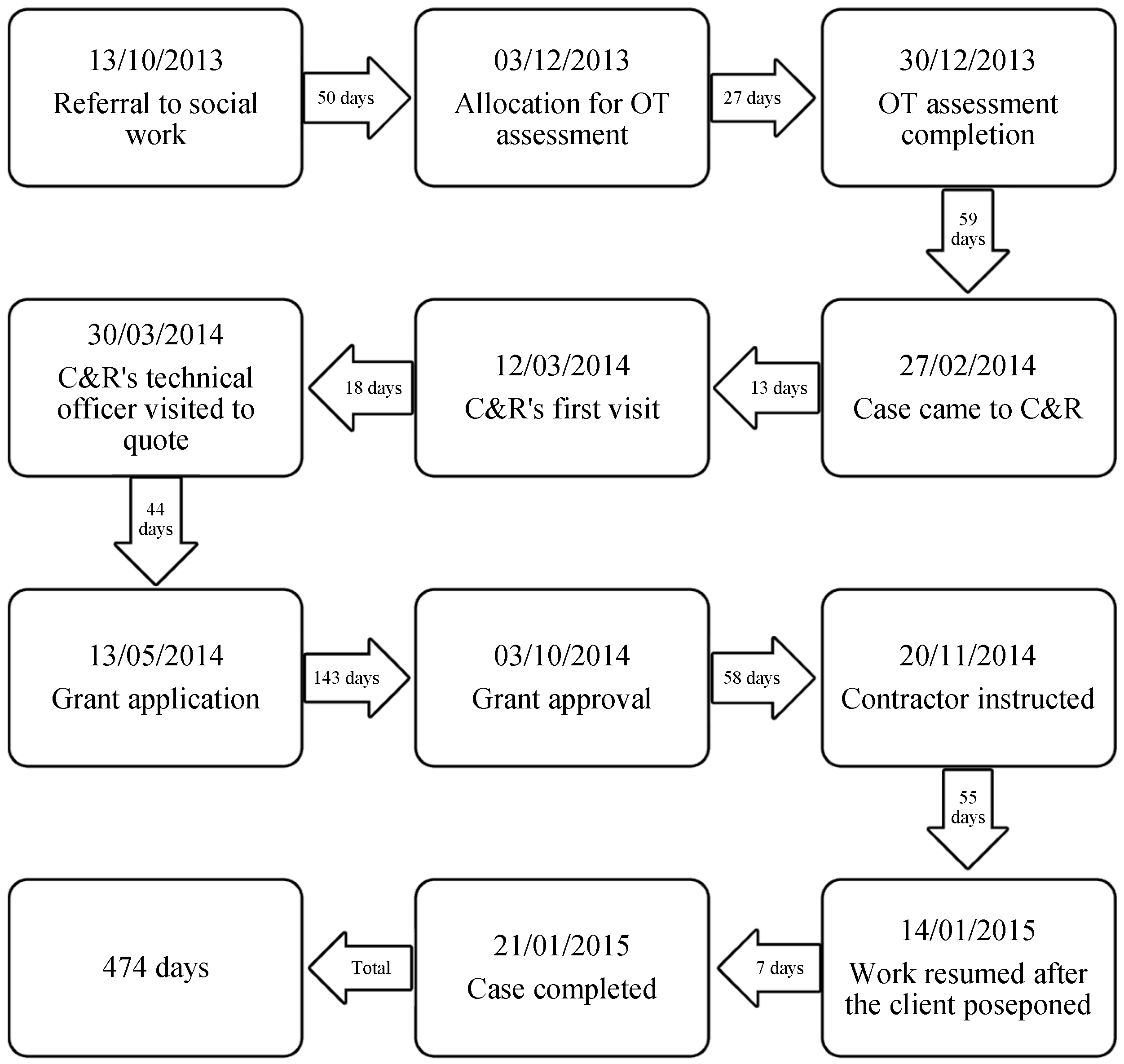
3.2.1. Case One
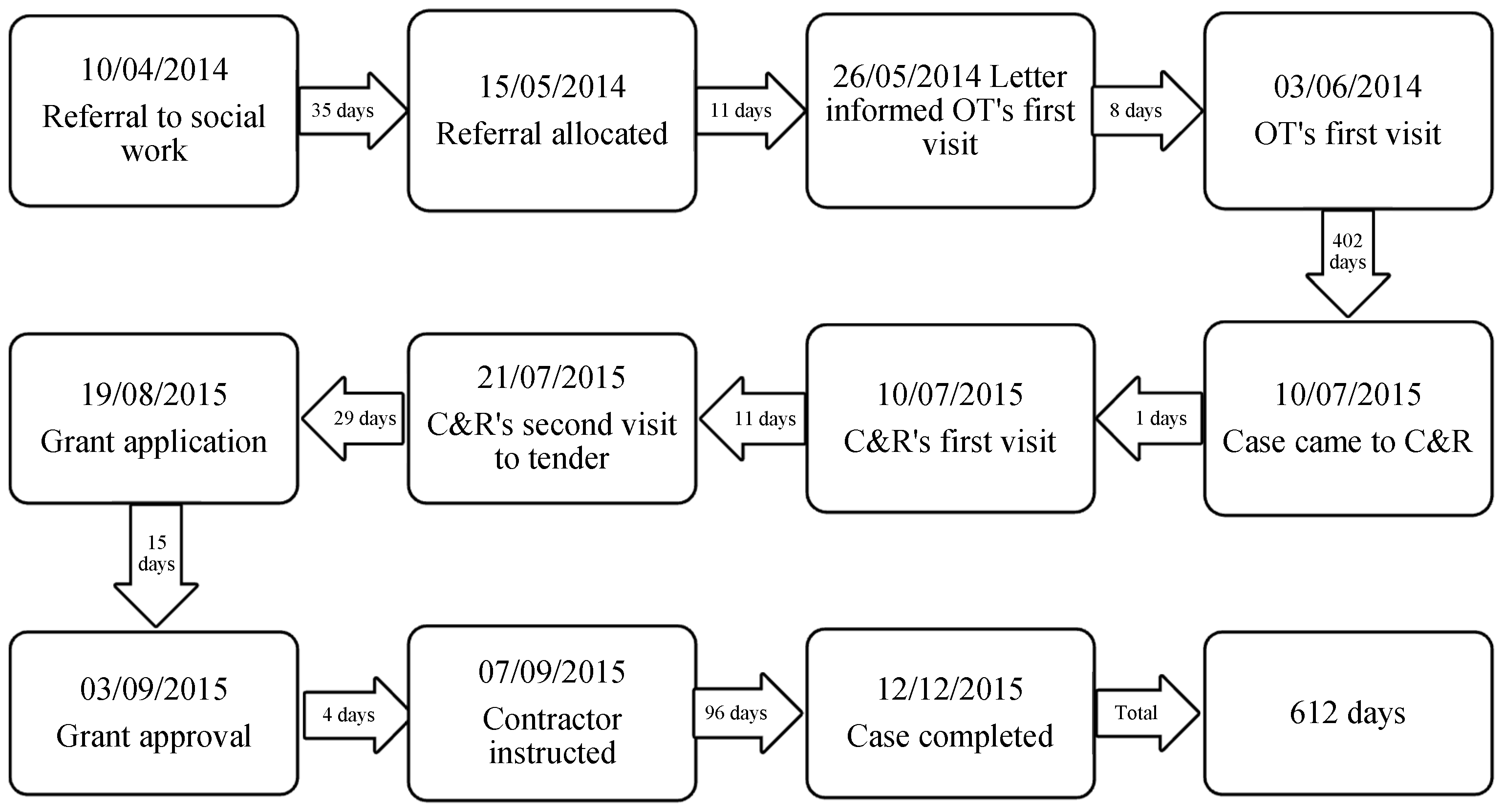
3.2.2. Case Two
3.3. Main Causes of Delays
3.3.1. Insufficient Resources
3.3.2. Lack of Joint Work
3.3.3. Bureaucratic Procedures
3.3.4. Gap between Grant and Cost
3.3.5. Shortage of Reliable Contractors
3.3.6. Clients’ Decisions
4. Discussions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cho, H.Y.; MacLachlan, M.; Clarke, M.; Mannan, H. Accessible home environments for people with functional limitations: A systematic review. Int. J. Environ. Res. Public Health 2016, 13, 826. [Google Scholar] [CrossRef] [PubMed]
- Kylén, M.; Ekström, H.; Haak, M.; Elmståhl, S.; Iwarsson, S. Home and health in the third age—Methodological background and descriptive findings. Int. J. Environ. Res. Public Health 2014, 11, 7060–7080. [Google Scholar] [CrossRef] [PubMed]
- Frank, J.B. The Paradox of Aging in Place in Assisted Living; Bergin & Garvey: Westport, CT, USA, 2002. [Google Scholar]
- Wiles, J. Conceptualizing place in the care of older people: The contributions of geographical gerontology. J. Clin. Nurs. 2005, 14, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Farber, N.; Shinkle, D.; Lynott, J.; Fox-Grage, W.; Harrell, R. Aging in Place: A State Survey of Livability Policies and Practices; AARP Public Policy Institute: Washington, DC, USA, 2011. [Google Scholar]
- Sixsmith, J. The meaning of home: An exploratory study of environmental experience. J. Environ. Psychol. 1986, 6, 281–298. [Google Scholar] [CrossRef]
- Means, R. Safe as houses? Ageing in place and vulnerable older people in the UK. Soc. Policy Adm. 2007, 41, 65–85. [Google Scholar] [CrossRef]
- Pettersson, C.; Slaug, B.; Granbom, M.; Kylberg, M.; Iwarsson, S. Housing accessibility for senior citizens in Sweden: Estimation of the effects of targeted elimination of environmental barriers. Scand. J. Occup. Ther. 2017, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Renaut, S.; Ogg, J.; Petite, S.; Chamahian, A. Home environments and adaptations in the context of ageing. Ageing Soc. 2015, 35, 1278–1303. [Google Scholar] [CrossRef]
- Sixsmith, J.; Sixsmith, A.; Fänge, A.M.; Naumann, D.; Kucsera, C.; Tomsone, S.; Haak, M.; Dahlin-Ivanoff, S.; Woolrych, R. Healthy ageing and home: The perspectives of very old people in five European countries. Soc. Sci. Med. 2014, 106, 1–9. [Google Scholar] [CrossRef]
- Thordardottir, B.; Chiatti, C.; Ekstam, L.; Fänge, A.M. Heterogeneity of characteristics among housing adaptation clients in Sweden—Relationship to participation and self-rated health. Int. J. Environ. Res. Public Health 2016, 13, 91. [Google Scholar] [CrossRef]
- Haak, M.; Ivanoff, S.D.; Fänge, A.; Sixsmith, J.; Iwarsson, S. Home as the locus and origin for participation: Experiences among very old Swedish people. OTJR 2007, 27, 95–103. [Google Scholar] [CrossRef]
- Pynoos, J.; Nishita, C.; Perelma, L. Advancements in the home modification field: A tribute to M. Powell Lawton. J. Hous. Elder. 2003, 17, 105–116. [Google Scholar] [CrossRef]
- Sanford, J.A. Universal Design as a Rehabilitation Strategy: Design for the Ages; Springer: Salmon Tower Building, NY, USA, 2003. [Google Scholar]
- Chiatti, C.; Iwarsson, S. Evaluation of housing adaptation interventions: Integrating the economic perspective into occupational therapy practice. Scand. J. Occup. Ther. 2014, 21, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Hwang, E.; Cummings, L.; Sixsmith, A.; Sixsmith, J. Impacts of home modifications on ageing-in-place. J. Hous. Elder. 2011, 25, 246–257. [Google Scholar] [CrossRef]
- Stark, S. Home modifications that enable occupational performance. In Using Environments to Enable Occupational Performance; Letts, L., Rigby, P., Eds.; SLACK Incorporated: Thorofare, NJ, USA, 2003; pp. 220–225. [Google Scholar]
- Fänge, A.; Iwarsson, S. Changes in ADL dependence and aspects of usability following housing adaptation—A longitudinal perspective. Am. J. Occup. Ther. 2005, 59, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, L.N. Conducting research on home environments: Lessons learned and new directions. Gerontologist 2003, 43, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Nahemow, L. Ecology and the aging process. In The Psychology of Adult Development and Aging; Eisdorfer, C., Lawton, M.P., Eds.; American Psychological Association: Washington, DC, USA, 1973; pp. 619–674. [Google Scholar]
- Lien, L.L.; Steggell, C.D.; Iwarsson, S. Adaptive strategies and person-environment fit among functionally limited older adults aging in place: A mixed methods approach. Int. J. Environ. Res. Public Health 2005, 12, 11954–11974. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P. The elderly in context: Perspectives from environmental psychology and gerontology. Environ. Behav. 1985, 17, 501–519. [Google Scholar] [CrossRef]
- Wahl, H.W.; Iwarsson, S.; Oswald, F. Aging well and the environment: Toward an integrative model and research agenda for the future. Gerontologist 2012, 52, 306–316. [Google Scholar] [CrossRef]
- Mandelstam, M. Home Adaptations: The Care Act 2014 and Related Provision across the United Kingdom; College of Occupational Therapists Ltd.: London, UK, 2016. [Google Scholar]
- Morgan, D.J.; Boniface, G.E.; Reagon, C. The effects of adapting their home on the meaning of home for families with a disabled child. Disabil. Soc. 2016, 31, 481–496. [Google Scholar] [CrossRef]
- Ramsay, M. Adapting for a Lifetime: The Key Role of Home Improvement Agencies in Adaptations Delivery; Foundations: Derbyshire, UK, 2010. [Google Scholar]
- Zhou, W.; Oyegoke, A.S.; Sun, M. Service planning and delivery outcomes of home adaptations for ageing in the UK. J. Hous. Built Environ. 2017, 1–19. [Google Scholar] [CrossRef]
- Bradford, I. The adaptation process. In Housing Options for Disabled People; Bull, R., Ed.; Jessica Kingsley: London, UK, 1998; pp. 78–114. [Google Scholar]
- Hall, E.; Scottish Work Services Inspectorate. Equipment and Adaptation Services in Scotland: A Survey of Waiting Times for Social Work Provision; Scottish Executive Central Research Unit: Edinburgh, UK, 2001. [Google Scholar]
- Clayton, V.; Silke, D. Evaluation of the Housing Adaptation Grant Schemes for Older People and People with a Disability; Housing Agency: Dublin, UK, 2010. [Google Scholar]
- Jones, C. Review of Housing Adaptations Including Disabled Facilities Grants—Wales; Welsh Government: Cardiff, UK, 2005. [Google Scholar]
- Mackintosh, S.; Leather, P. The Disabled Facilities Grant: Before and after the Introduction of the Better Care Fund; Foundations: Derbyshire, UK, 2016. [Google Scholar]
- Adaptation Working Group. Adapting for Change; Scottish Government: Edinburgh, UK, 2012.
- Department for Communities and Local Government. Lifetime Homes, Lifetime Neighbourhoods; DCLG Publications: London, UK, 2008.
- Scottish Government. Age, Home and Community: A Strategy for Housing for Scotland’s Older People: 2012–2021; Scottish Government: Edinburgh, UK, 2011.
- Welsh Government. The Strategy for Older People in Wales 2013–2023—Living Longer, Aging Well; Welsh Government Publications: Cardiff, UK, 2013.
- Boniface, G.; Mason, M.; Macintyre, J.; Synan, C.; Riley, J. The effectiveness of local authority social services’ occupational therapy for older people in Great Britain: A critical literature review. Br. J. Occup. Ther. 2013, 76, 538–547. [Google Scholar] [CrossRef]
- Bibbings, J.; Boniface, G.; Campbell, J.; Findlay, G.; Reeves-McAll, E.; Zhang, M.; Zhou, P. A Review of Independent Living Adaptations; Welsh Government: Cardiff, UK, 2015. [Google Scholar]
- Kempton, O.; Warby, A. Measuring the Social Return on Investment of Stage 3 Adaptations and Very Sheltered Housing in Scotland; Envoy Partnership: London, UK, 2012. [Google Scholar]
- Creswell, J.W. Research Design. Qualitative, Quantitative, and Mixed Methods Approaches, 2nd ed.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2003. [Google Scholar]
- Pettersson, C.; Löfqvist, C.; Malmgren Fänge, A. Clients’ experiences of housing adaptations: A longitudinal mixed-methods study. Disabil. Rehabil. 2012, 34, 1706–1715. [Google Scholar] [CrossRef] [PubMed]
- Schwingel, A.; Gálvez, P.; Linares, D.; Sebastião, E. Using a mixed-methods re-aim framework to evaluate community health programs for older Latinas. J. Aging Health 2016, 4, 551–593. [Google Scholar] [CrossRef] [PubMed]
- Teddlie, C.; Yu, F. Mixed methods sampling: A typology with examples. J. Mix. Methods Res. 2007, 1, 77–100. [Google Scholar] [CrossRef]
- Connell, J.; Page, S.J.; Bentley, T. Towards sustainable tourism planning in New Zealand: Monitoring local government planning under the Resource Management Act. Tour. Manag. 2009, 30, 867–877. [Google Scholar] [CrossRef]
- Davies, K.; Bullock, M.; Brandon, A.; Wainman, K.; Craig, L.; Fletcher, P.; Duncan, A. A Study of the Housing and Support Needs of Older People in Herefordshire; Peter Fletcher Associates Ltd.: Northumberland, UK, 2012. [Google Scholar]
- Heywood, F.; Gangoli, G.; Langan, J.; Marsh, A.; Moyers, S.; Smith, R.; Sutton, E.; Hodges, M.; Hamilton, J. Reviewing the Disabled Facilities Grant Programme; Office of the Deputy Prime Minister: London, UK, 2005.
- Perry, F.C. Adaptation Works: How Disabled Facilities Grants Are the Overlooked Solution to the Accessible Housing Shortage and Associated Costs; Disability United: Warwickshire, UK, 2015. [Google Scholar]
- Scottish Executive. Equipped for Inclusion: Report of the Strategy Forum: Equipment and Adaptations; Scottish Executive: Edinburgh, UK, 2003.
- Audit Commission. Home Alone: The Role of Housing in Community Care; Audit Commission: London, UK, 1998.
- Keeble, U. Aids and Adaptations; Bedford Square Press: London, UK, 1979. [Google Scholar]
- Home Adaptations Consortium. Home Adaptations for Disabled People: A Detailed Guide to Related Legislation, Guidance and Good Practice; Care & Repair England: Nottingham, UK, 2013.
- Audit Scotland. Adapting to the Future—Management of Community Equipment and Adaptations; Audit Scotland: Edinburgh, UK, 2004.



{kind=link}
{kind=link}
| The Adaptation Process | Minimum | Average | Maximum | Median | |
|---|---|---|---|---|---|
| Stages | (day) | ||||
| Category I | |||||
| 1 | Referral | 1 | 41 | 189 | 28 |
| 2 | Case allocation | 1 | 21 | 103 | 7 |
| 3 | Assessment | 2 | 46 | 233 | 21 |
| 4 | Funding approval | 3 | 85 | 233 | 60 |
| 5 | Installation | 14 | 54 | 90 | 56 |
| Total | 60 | 193 | 360 | 166 | |
| Category II | |||||
| 1–3 | Referral to assessment | 28 | 121 | 573 | 85 |
| 4 | Funding approval | 23 | 118 | 630 | 67 |
| 5 | Installation | 30 | 93 | 226 | 77 |
| Total | 90 | 243 | 474 | 236 | |
| Category III | |||||
| 4 | Funding approval | 7 | 112 | 385 | 92 |
| 5 | Installation | 7 | 115 | 356 | 96 |
| Total | 84 | 227 | 522 | 188 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, W.; Oyegoke, A.S.; Sun, M. Causes of Delays during Housing Adaptation for Healthy Aging in the UK. Int. J. Environ. Res. Public Health 2019, 16, 192. https://doi.org/10.3390/ijerph16020192
Zhou W, Oyegoke AS, Sun M. Causes of Delays during Housing Adaptation for Healthy Aging in the UK. International Journal of Environmental Research and Public Health. 2019; 16(2):192. https://doi.org/10.3390/ijerph16020192
Chicago/Turabian StyleZhou, Wusi, Adekunle Sabitu Oyegoke, and Ming Sun. 2019. "Causes of Delays during Housing Adaptation for Healthy Aging in the UK" International Journal of Environmental Research and Public Health 16, no. 2: 192. https://doi.org/10.3390/ijerph16020192
APA StyleZhou, W., Oyegoke, A. S., & Sun, M. (2019). Causes of Delays during Housing Adaptation for Healthy Aging in the UK. International Journal of Environmental Research and Public Health, 16(2), 192. https://doi.org/10.3390/ijerph16020192