Elderly Health Inequality in China and its Determinants: A Geographical Perspective


Abstract
:1. Introduction
2. Methods
2.1. Data
2.1.1. Individual-Level Variables
2.1.2. Provincial-Level Variables
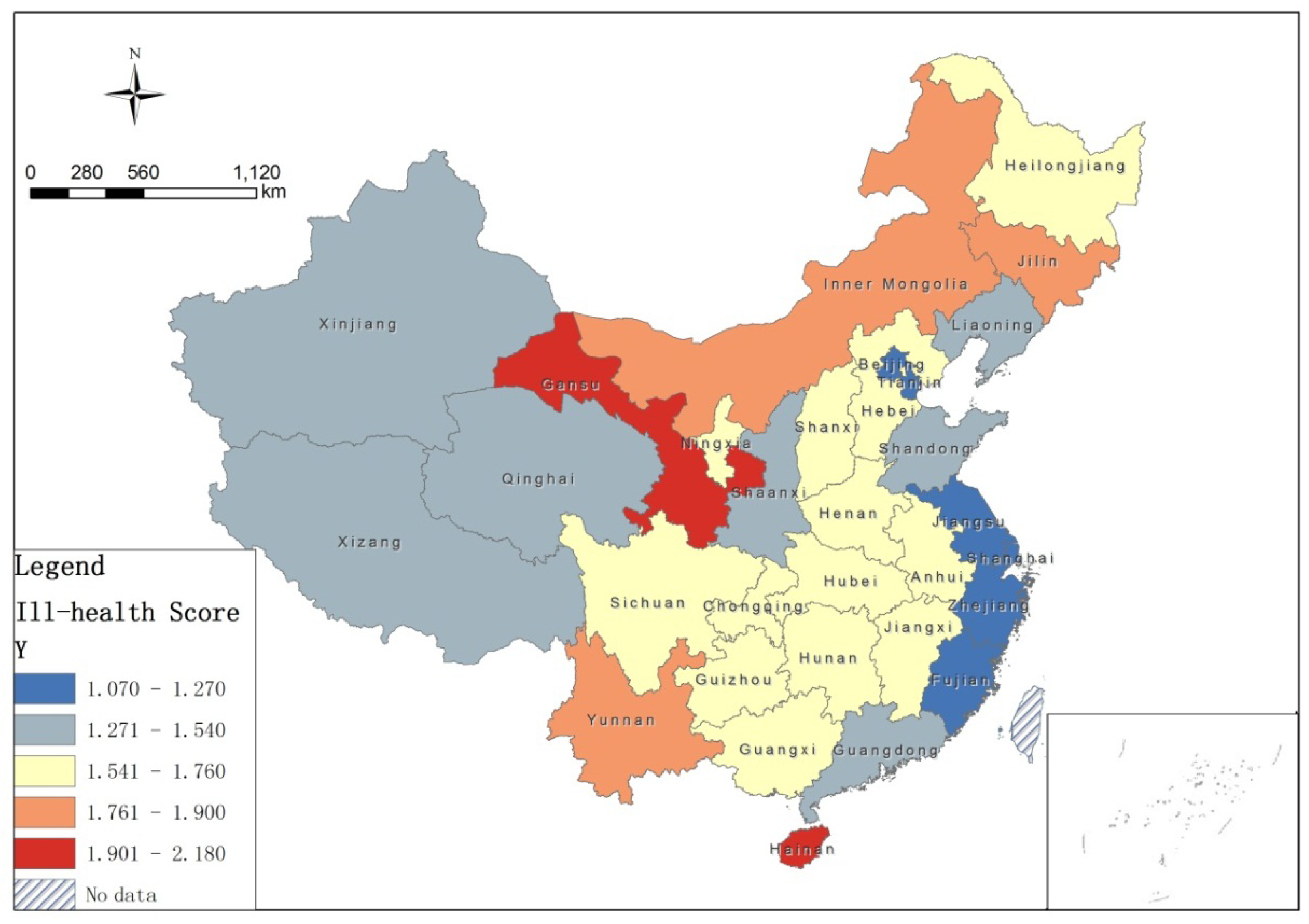
2.2. Ill-Health Score
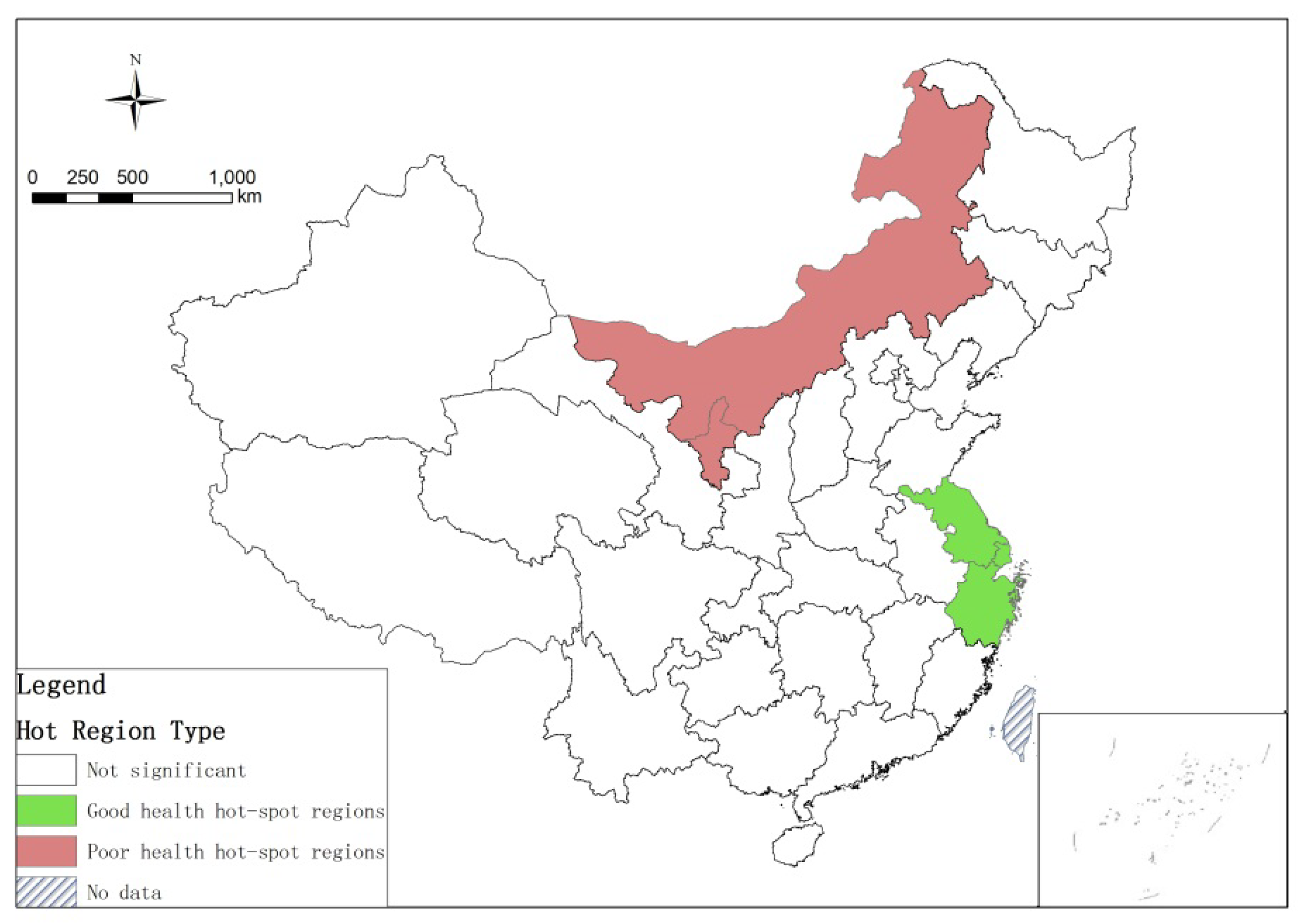
2.3. Spatial Autocorrelation of Elderly Health
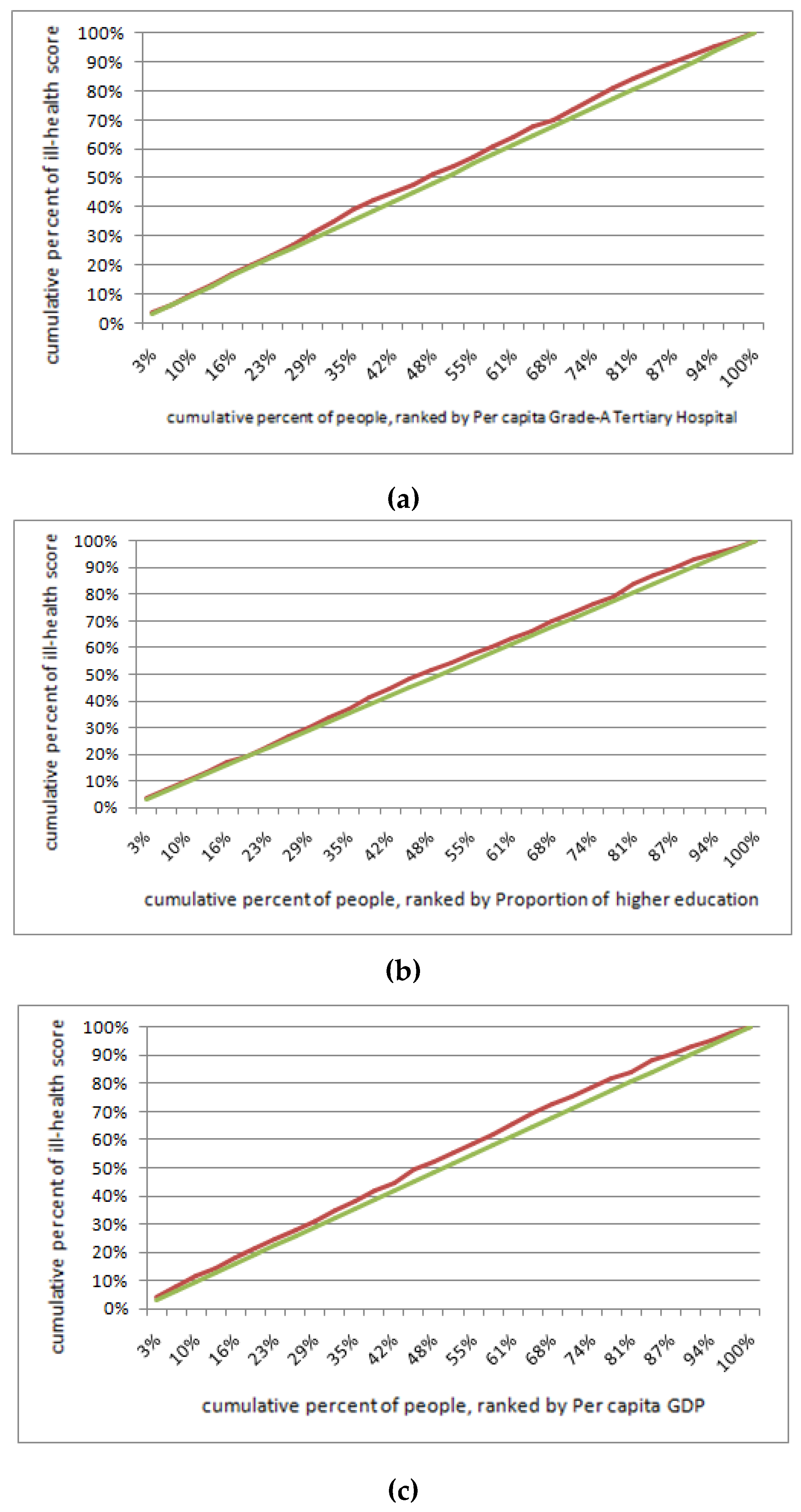
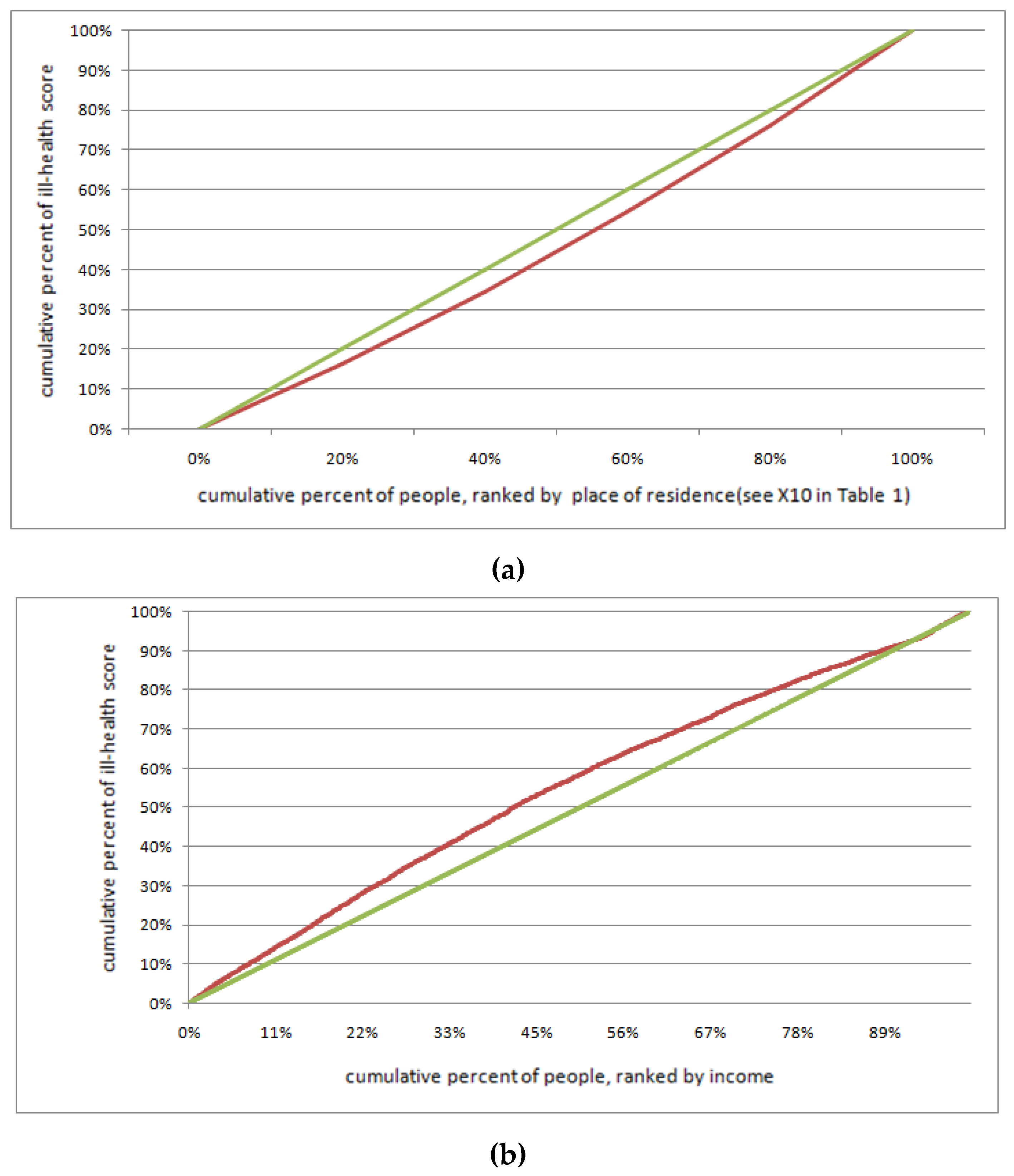
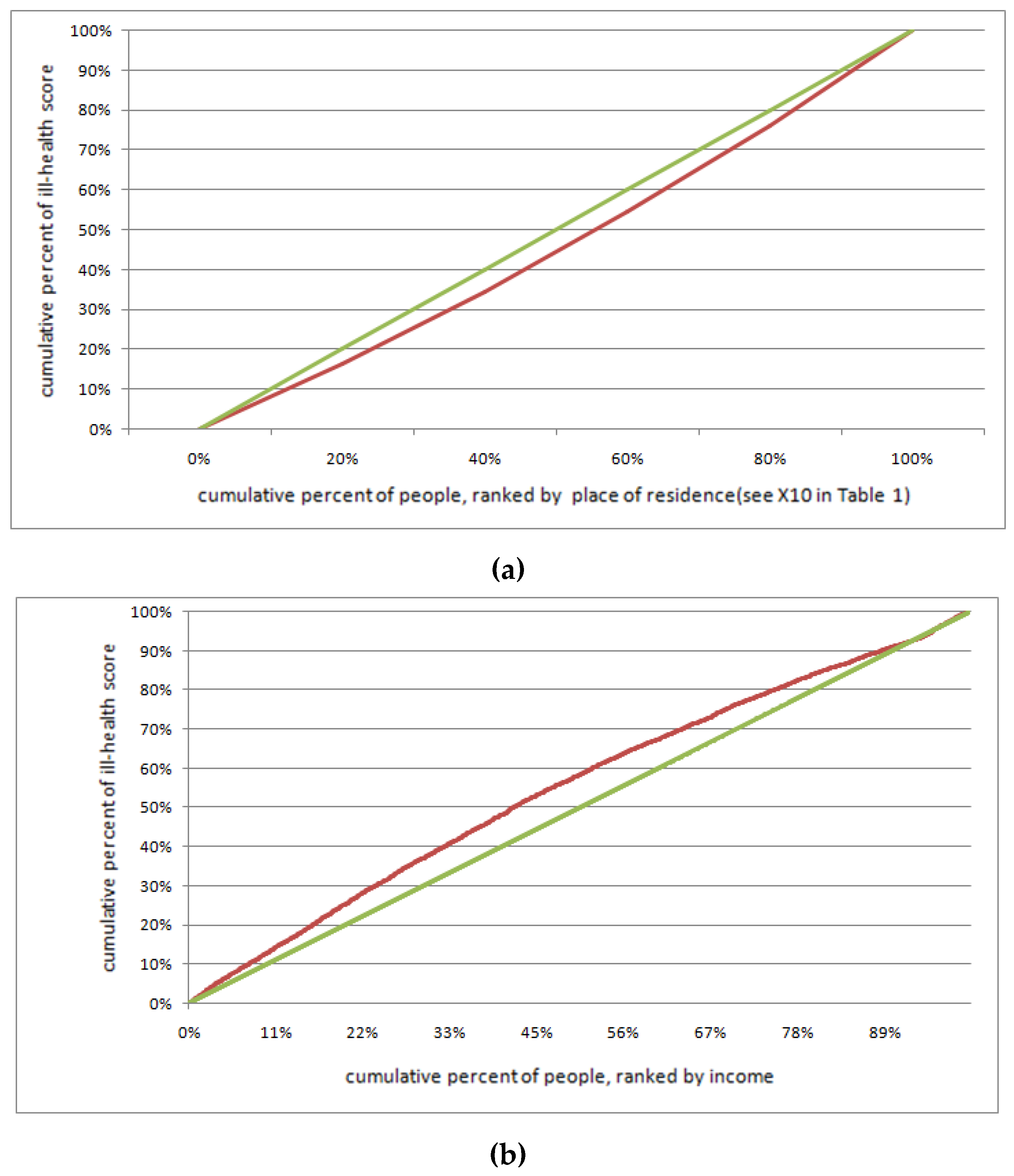
2.4. Health Concentration Curve
2.5. Determinants of Health Inequality
3. Results
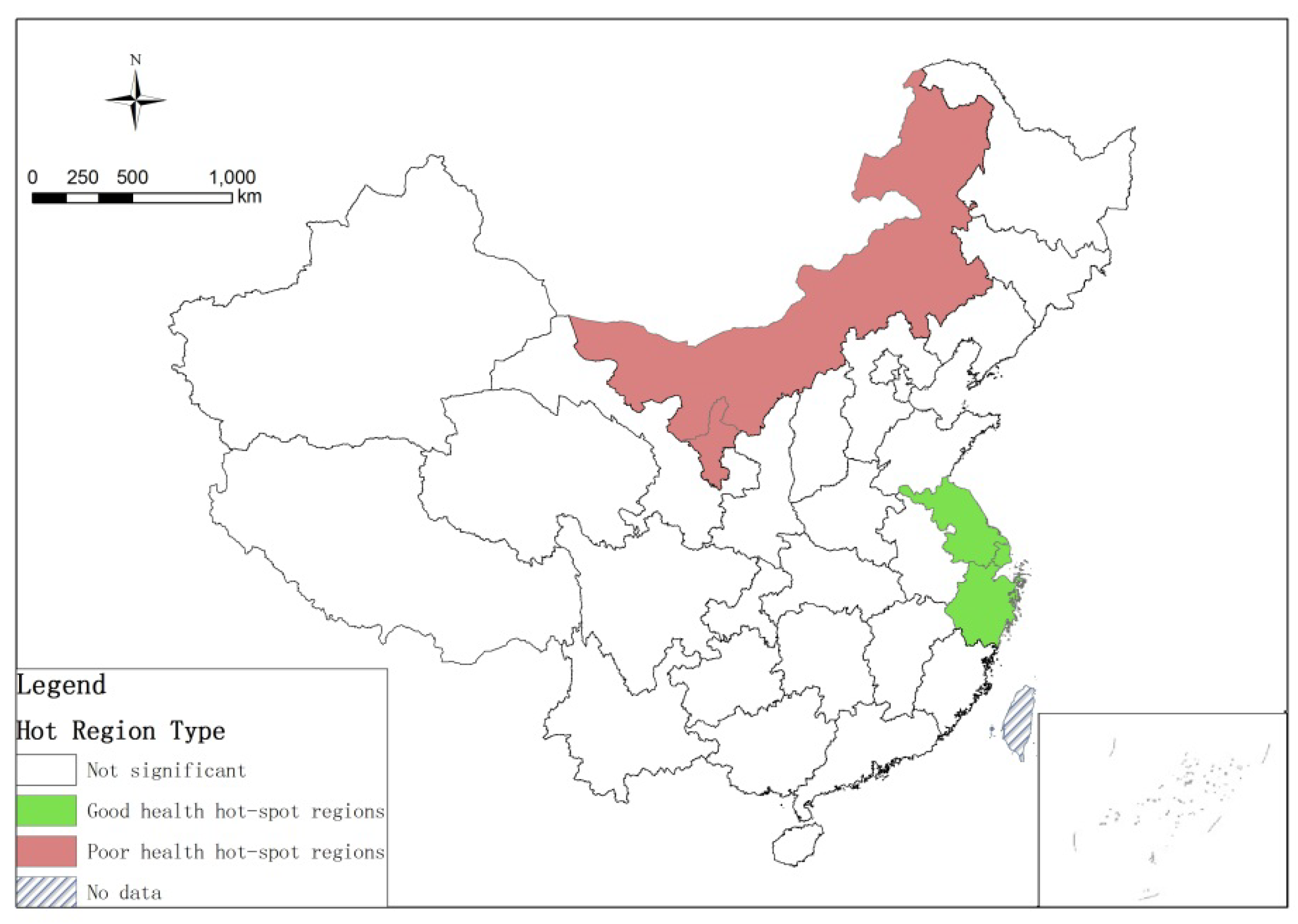
3.1. Spatial Pattern of Elderly Health
3.2. Determinants of Elderly Health Inequality in China
3.2.1. Determinants of Inter-Provincial Health Inequality by Multi-Level Regression
3.2.2. Determinants for Health Inequality by Multi-Level Regression at the Individual Level
4. Discussion
4.1. A Significant Geographical Differentiation in Elderly Health in China
4.2. Elderly Health Inequality at the Provincial Level and Its Determinants
4.3. Health Inequality of the Elderly at the Individual Level and Its Determinants
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Yourkavitch, J.; Burgert-Brucker, C.; Assaf, S.; Delgado, S. Using geographical analysis to identify child health inequality in sub-Saharan Africa. PLoS ONE 2018, 13, e0201870. [Google Scholar] [CrossRef]
- Wagstaff, A.; Doorslaer, V.E.; Watanabe, N. On Decomposing the Causes of Health Sector Inequalities with an Application to Malnutrition Inequalities in Vietnam; The World Bank: Washington, DC, USA, 2001. [Google Scholar]
- Liu, H.; Chao, J.X. Income-Related Health Inequality of Urban Residents in China and Influencing Factors. Chin. Gen. Pract. 2009, 12, 1609–1610. (In Chinese) [Google Scholar]
- Hu, L.L. An empirical study on the income-related health inequality in China. Chin. J. Health Policy 2005, 12, 58–62. (In Chinese) [Google Scholar]
- Chen, Y.; Qing, H.M.; Tang, J.X.; Zhou, Y. Income-related Health Inequality and Decomposition. Chin. Health Econ. 2016, 35, 71–73. (In Chinese) [Google Scholar]
- Curtis, S. Health and Inequality: Geographical Perspectives; Sage: Thousand Oaks, CA, USA, 2004. [Google Scholar]
- Ebener, S.; Guerra-Arias, M.; Campbell, J.; Tatem, A.J.; Moran, A.C.; Johnson, F.A.; Porter, R. The geography of maternal and newborn health: The state of the art. International Journal of Health. Geographics 2015, 14, 19. [Google Scholar]
- Johnson, F.A.; Frempong-Ainguah, F.; Matthews, Z.; Harfoot, A.J.; Nyarko, P.; Baschieri, A.; Atkinson, P.M. Evaluating the impact of the community-based health planning and services initiative on uptake of skilled birth care in Ghana. PLoS ONE 2015, 10, e0120556. [Google Scholar] [CrossRef] [PubMed]
- Rosero-Bixby, L. Spatial access to health care in Costa Rica and its equity: A GIS-based study. Soc. Sci. Med. 2004, 58, 1271–1284. [Google Scholar] [CrossRef]
- Li, Z.; Fan, Z.; Shen, S. Urban Green Space Suitability Evaluation Based on the AHP-CV Combined Weight Method: A Case Study of Fuping County, China. Sustainability 2018, 10, 2656. [Google Scholar] [CrossRef]
- WHO. Environmental Health Inequalities in Europe. Available online: http://www.euro.who.int/__data/assets/pdf_file/0010/157969/e96194.pdf (accessed on 13 January 2019).
- Briggs, D.; Abellan, J.J.; Fecht, D. Environmental inequity in England: Small area associations between socio-economic status and environmental pollution. Soc. Sci. Med. 2008, 67, 1612–1629. [Google Scholar] [CrossRef]
- Yanosky, J.D.; Schwartz, J.; Suh, H.H. Associations between measures of socioeconomic position and chronic nitrogen dioxide exposure in Worcester, Massachusetts. J. Toxicol. Environ. Health Part A 2008, 71, 1593–1602. [Google Scholar] [CrossRef]
- Viel, J.F.; Hägi, M.; Upegui, E.; Laurian, L. Environmental justice in a French industrial region: Are polluting industrial facilities equally distributed? Health Place 2011, 17, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Brochu, P.J.; Yanosky, J.D.; Paciorek, C.J.; Schwartz, J.; Chen, J.T.; Herrick, R.F.; Suh, H.H. Particulate air pollution and socioeconomic position in rural and urban areas of the Northeastern United States. Am. J. Public Health 2011, 101 (Suppl. 1), S224–S230. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.L.; Ebisu, K. Environmental inequality in exposures to airborne particulate matter components in the United States. Environ. Health Perspect. 2012, 120, 1699–1704. [Google Scholar] [CrossRef] [PubMed]
- Laurian, L.; Funderburg, R. Environmental justice in France? A spatio-temporal analysis of incinerator location. J. Environ. Plan. Manag. 2014, 57, 424–446. [Google Scholar] [CrossRef]
- Padilla, C.M.; Kihal-Talantikite, W.; Vieira, V.M.; Rossello, P.; Le Nir, G.; Zmirou-Navier, D.; Deguen, S. Air quality and social deprivation in four French metropolitan areas—A localized spatio-temporal environmental inequality analysis. Environ. Res. 2014, 134, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Pearce, J.; Dorling, D. Increasing geographical inequalities in health in New Zealand, 1980–2001. Int. J. Epidemiol. 2006, 35, 597–603. [Google Scholar] [PubMed]
- Shaw, M.; Dorling, D.; Gordon, D.; Smith, G.D. Putting time, person and place together: The temporal, social and spatial accumulation of health inequality. Crit. Public Health 2001, 11, 289–304. [Google Scholar] [CrossRef]
- Cabrera-Barona, P.; Murphy, T.; Kienberger, S.; Blaschke, T. A multi-criteria spatial deprivation index to support health inequality analyses. Int. J. Health Geogr. 2015, 14, 11. [Google Scholar] [CrossRef]
- Pearce, J.R.; Richardson, E.A.; Mitchell, R.J.; Shortt, N.K. Environmental justice and health: The implications of the socio—Spatial distribution of multiple environmental deprivation for health inequalities in the United Kingdom. Trans. Inst. Br. Geogr. 2010, 35, 522–539. [Google Scholar] [CrossRef]
- Wallace, M.; Crear-Perry, J.; Richardson, L.; Tarver, M.; Theall, K. Separate and unequal: Structural racism and infant mortality in the US. Health Place 2017, 45, 140–144. [Google Scholar] [CrossRef]
- Wang, X.Y. Socioeconomic Status, Healthy Lifestyle, Health Inequality of Chinese Residents. Master Thesis, Xiamen University, Xiamen, China, 2014. (In Chinese). [Google Scholar]
- Yang, G.; Wang, Y.; Zeng, Y.; Gao, G.F.; Liang, X.; Zhou, M.; Vos, T. Rapid health transition in China, 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 381, 1987–2015. [Google Scholar] [CrossRef]
- Zhou, J. The Study on the Province Disparities of Health Inequalities and Health Achievement—An Empirical Analysis Based on CGSS2008 Data. J. Wuhan Text. Univ. 2014, 27, 32–37. (In Chinese) [Google Scholar]
- Lee, M.C.; Jones, A.M. Understanding differences in income-related health inequality between geographic regions in Taiwan using the SF-36. Health Policy 2007, 83, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Deng, Q.H. Health Inequalities in Urban Areas of China and Its Decomposition. J. Grad. Sch. Chin. Acad. Soc. Sci. 2010, 5, 62–68. (In Chinese) [Google Scholar]
- Zhao, Z. Income inequality, unequal health care access, and mortality in China. Popul. Dev. Rev. 2006, 32, 461–483. [Google Scholar] [CrossRef]
- Li, D.; Zhou, Z.; Si, Y.; Xu, Y.; Shen, C.; Wang, Y.; Wang, X. Unequal distribution of health human resource in mainland China: What are the determinants from a comprehensive perspective? Int. J. Equity Health 2018, 17, 29. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Xu, Y.; Ren, J.; Sun, L.; Liu, C. Inequality in the distribution of health resources and health services in China: Hospitals versus primary care institutions. Int. J. Equity Health 2017, 16, 42. [Google Scholar] [CrossRef]
- Liu, X.Z. Research on the elderly health equity. Stud. Ethics 2018, 95, 94–99. (In Chinese) [Google Scholar]
- Guo, Z.Y.; Shi, W.X. The Study on Elderly People’s Health Equity Based on the New Health Conception Index System. Chin. J. Health Stat. 2015, 32, 741–744. (In Chinese) [Google Scholar]
- Gu, H.J.; Liu, Y.P. Income-related Health Inequality of the Elderly and Its Decomposition: An Empirical Research in the Urban and the Rural of China. South China Popul. 2011, 26, 1–9. (In Chinese) [Google Scholar]
- Ruan, Q.G.; Chen, G. Decomposition of Income-Related Inequalities in Health among Chinese Elderly: Based on the Data from Beijing. Popul. Econ. 2017, 5, 84–94. (In Chinese) [Google Scholar]
- Padilla, C.M.; Kihal-Talantikit, W.; Perez, S.; Deguen, S. Use of geographic indicators of healthcare, environment and socioeconomic factors to characterize environmental health disparities. Environ. Health 2016, 15, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, B.F.; Wang, X. Health Inequality among the Chinese Elderly: Changes, Regional Disparities and Determinants. Popul. Res. 2013, 37, 8–90. (In Chinese) [Google Scholar]
- Sun, R.; Gu, D. Air pollution, economic development of communities, and health status among the elderly in urban China. Am. J. Epidemiol. 2008, 168, 1311–1318. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.C.; Maheswaran, R. The health benefits of urban green spaces: A review of the evidence. J. Public Health 2011, 33, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Bowler, D.E.; Buyung-Ali, L.M.; Knight, T.M.; Pullin, A.S. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10, 456. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, B.W.; Ben-Shlomo, Y. Environmental equity, air quality, socioeconomic status, and respiratory health: A linkage analysis of routine data from the Health Survey for England. J. Epidemiol. Community Health 2005, 59, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Yuasa, M.; Ukawa, S.; Ikeno, T.; Kawabata, T. Multilevel, cross-sectional study on social capital with psychogeriatric health among older Japanese people dwelling in rural areas. Australas. J. Ageing 2014, 33, E13–E19. [Google Scholar] [CrossRef] [PubMed]
- Van der Wielen, R.P.; De Groot, L.C.P.G.M.; Van Staveren, W.A.; Löwik, M.R.H.; Van den Berg, H.; Haller, J.; Moreiras, O. Serum vitamin D concentrations among elderly people in Europe. Lancet 1995, 346, 207–210. [Google Scholar] [CrossRef]
- Díaz, J.; Jordán, A.; García, R.; López, C.; Alberdi, J.; Hernández, E.; Otero, A. Heat waves in Madrid 1986–1997: Effects on the health of the elderly. Int. Arch. Occup. Environ. Health 2002, 75, 163–170. [Google Scholar] [CrossRef]
- Bush, K.; Fossani, C.; Li, S.; Mukherjee, B.; Gronlund, C.; O’Neill, M. Extreme precipitation and beach closures in the great lakes region: Evaluating risk among the elderly. Int. J. Environ. Res. Public Health 2014, 11, 2014–2032. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.; Wang, W.W.; Jones, K.; Li, Y. An exploratory multilevel analysis of income, income inequality and self-rated health of the elderly in China. Soc. Sci. Med. 2012, 75, 2481–2492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagstaff, A.; Van Doorslaer, E. Measuring inequalities in health in the presence of multiple-category morbidity indicators. Health Econ. 1994, 3, 281–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anselin, L. Local indicators of spatial association—LISA. Geogr. Anal. 1995, 27, 93–115. [Google Scholar] [CrossRef]
- Yang, Z.; Ding, Q.Y.; Zhou, Q.Y.; Liu, H.M. Differentiation Pattern of Population Health and Its Geographical Influencing Factors in the Middle-Lower Reaches of the Yangtze River. Geogr. Geo Inf. Sci. 2018, 34, 83–90. (In Chinese) [Google Scholar]
- Ni, S.H. Spatial Statistics and Its Application to the Field of Public Health. J. Shantou Univ. 2014, 29, 61–67. (In Chinese) [Google Scholar]
- Zhou, L.; Tian, L.; Gao, Y.; Ling, Y.; Fan, C.; Hou, D.; Zhou, W. How did industrial land supply respond to transitions in state strategy? An analysis of prefecture-level cities in China from 2007 to 2016. Land Use Policy 2019, 87, 104009. [Google Scholar] [CrossRef]
- Thomas, S.L.; Heck, R.H. Analysis of large-scale secondary data in higher education research: Potential perils associated with complex sampling designs. Res. High. Educ. 2001, 42, 517–540. [Google Scholar] [CrossRef]
- Kreft, I.G.; De Leeuw, J. Introducing Multilevel Modeling; Sage: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Xiang, Q.F.; Shi, L. Influence Factors Analysis of Rural Labor Migration in Western Minority Areas- A Study Based on a Multilevel Logistic Models. Appl. Stat. Manag. 2012, 31, 965–974. (In Chinese) [Google Scholar]
- Smyth, F. Medical geography: Understanding health inequalities. Prog. Hum. Geogr. 2008, 32, 119–127. [Google Scholar] [CrossRef]
- Zeka, A.; Zanobetti, A.; Schwartz, J. Individual-level modifiers of the effects of particulate matter on daily mortality. Am. J. Epidemiol. 2006, 163, 849–859. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.D.; Krieger, N. Tackling health inequities. Br. Med J. 2008, 337, 529–530. [Google Scholar] [CrossRef]
- Pearce, J.; Dorling, D. Tackling global health inequalities: Closing the health gap in a generation. Environ. Plan. A 2009, 41, 1–6. [Google Scholar] [CrossRef]
- Szeto, W.Y.; Yang, L.; Wong, R.C.P.; Li, Y.C.; Wong, S.C. Spatio-temporal travel characteristics of the elderly in an ageing society. Travel Behav. Soc. 2017, 9, 10–20. [Google Scholar] [CrossRef] [Green Version]
- Liu, G.Q.; Li, N.X.; Mao, L.P. Health Values and Health-related Behaviors in Ethnic Minority Groups in Guizhou Province. J. Sichuan Univ. 2007, 38, 475–479. (In Chinese) [Google Scholar]
- Van de Poel, E.; O’Donnell, O.; Van Doorslaer, E. Is there a health penalty of China’s rapid urbanization? Health Econ. 2012, 21, 367–385. [Google Scholar] [CrossRef] [PubMed]
- Qin, W.; Xu, L.; Li, J.; Sun, L.; Ding, G.; Shao, H.; Xu, N. Estimating benefit equity of government health subsidy in healthcare Services in Shandong Province, China: A cross-sectional study. Int. J. Equity Health 2018, 17, 61. [Google Scholar] [CrossRef] [PubMed]
- Si, L.; Chen, M.; Palmer, A.J. Has equity in government subsidy on healthcare improved in China? Evidence from the China’s National Health Services Survey. Int. J. Equity Health 2017, 16, 6. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Level | Type | Code | Variable name | Expected effects on ill-health1 | Calculation method | |
|---|---|---|---|---|---|---|
| Dependent variable | Y | Ill- health score | Ill-health score [47] (see 2.2) | |||
| Level 2: provincial-level | Explanatory variables | Medical resources [30,31] | S1 | Grade-A tertiary hospital Per capita | - | Urban Statistical Yearbook of China |
| Education [23] | S2 | Proportion of higher education population to total population | - | The Sixth Population Census Data | ||
| Economic | S3 | GDP Per capita | - | Urban Statistical Yearbook of China | ||
| Environment [36,41] | S4 | Annual average air pollution index in 2010 | + | Datacenter in Ministry of Environmental Protection of China | ||
| S5 | Average daily precipitation | ? | Urban Statistical Yearbook of China, Unit: mm | |||
| S6 | Average daily temperature | + | Urban Statistical Yearbook of China, Unit: 0.1 °C | |||
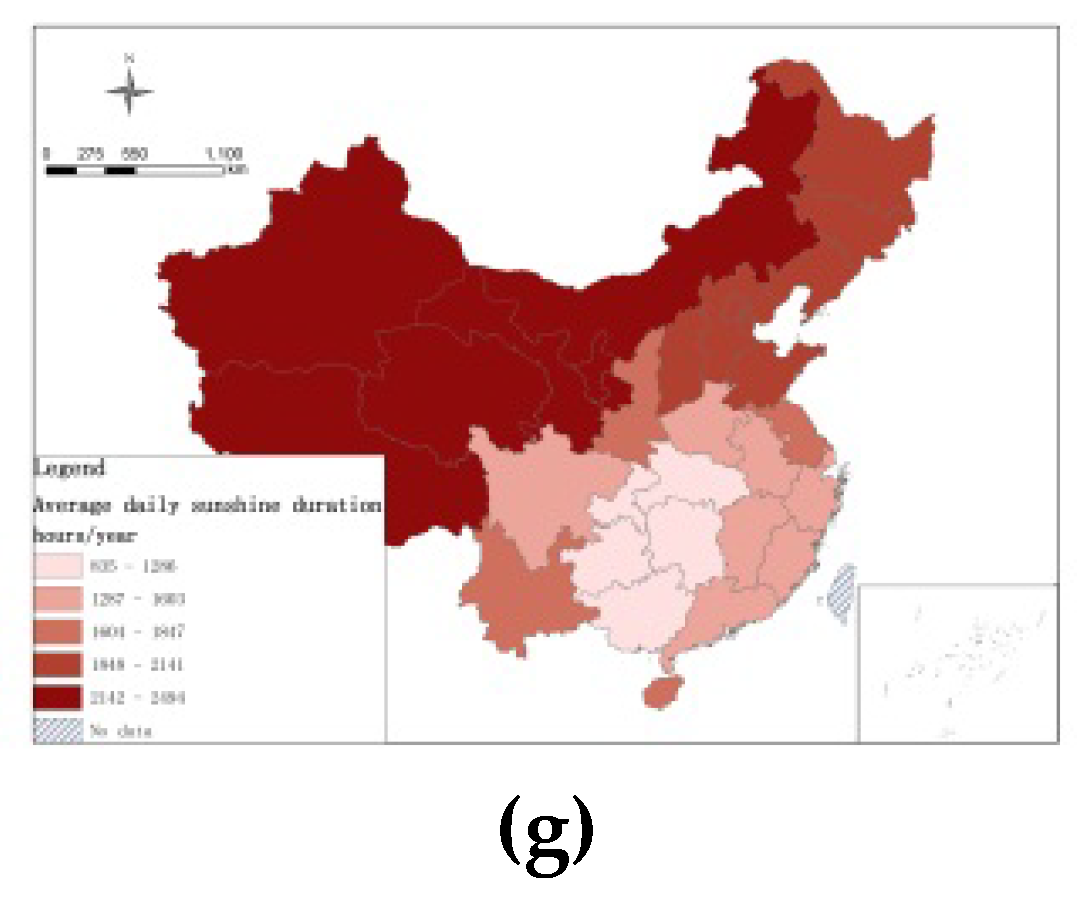
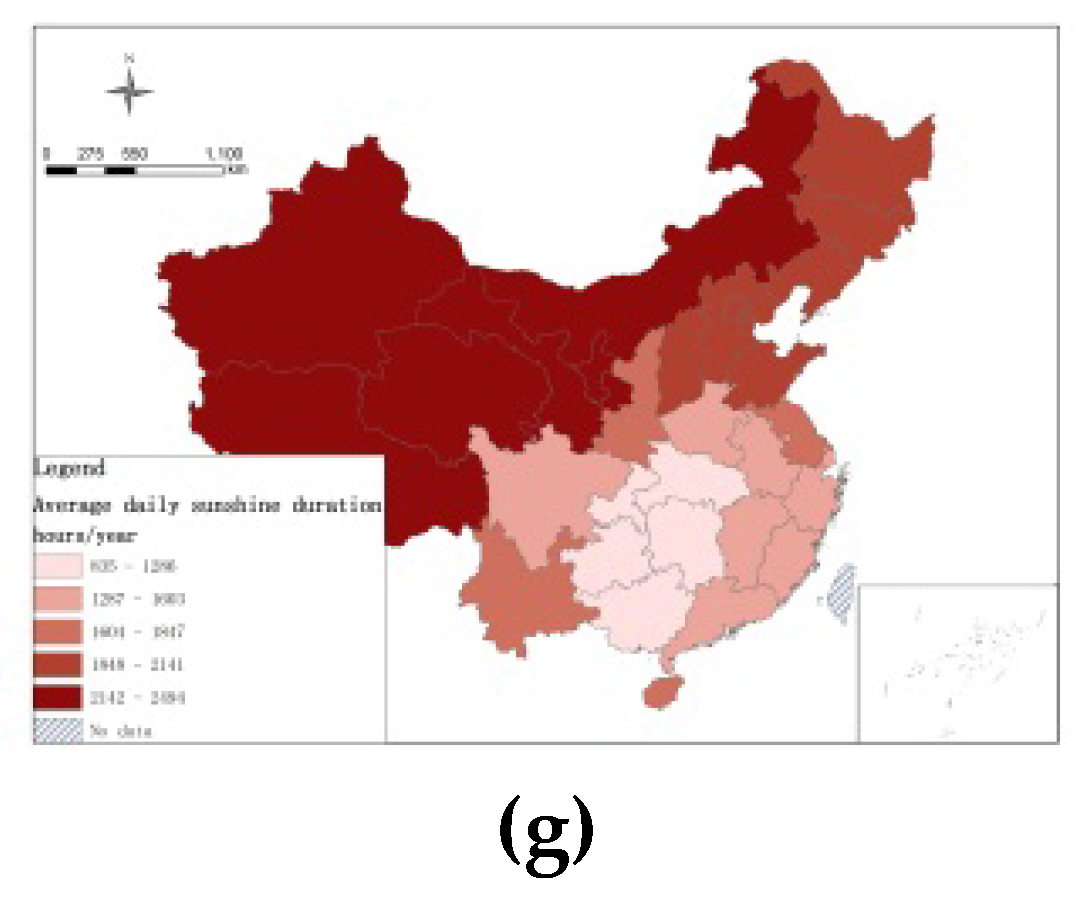
| S7 | Average daily sunshine duration | - | Urban Statistical Yearbook of China, Unit: hours/year | |||
| Level 1: Individual-level | Control variables | Individual characteristics | X1 | Age | + | |
| X2 | Gender | - | Male = 0, female = 1 | |||
| X3 | Educational level | - | Uneducated = 1 Elementary school = 2 Junior high school = 3 High school/Technical secondary school/ Vocational high school = 4 College degree = 5 Bachelor degree or above = 6 | |||
| X4 | Marital Status | - | Spouse is alive = 1Other = 0 | |||
| X5 | Ethnicity | - | Han = 0, Other = 1 | |||
| X6 | Exercise frequency | - | 1 = No exercise 2 = Less than once in a week 3 = One to two times 4 = Three to Five Times 5 = Six times and above | |||
| Social interaction | X7 | Loneliness | - | Often = 1 Sometimes = 2 Never = 3 | ||
| X8 | Social responsibility | - | Maintain community social security/Help mediate Neighborhood Disputes/Maintain Community Environment/Help Neighbors/Care For The Next Generation/ Participate In Cultural And Scientific Promotion Activities = 1 Do not participate = 0 | |||
| X9 | Social activity | - | Watching movies / Dancing, Croquet/ Table tennis/ Badminton, Playing mahjong/Playing poker/Playing chess, Fishing/Calligraphy/ Photography/ Collection = 1 Do not participate = 0 | |||
| Explanatory variables | Built -environment | X10 | Place of residence | + | Urban = 0, Urban-Rural area = 1, Town = 2, Town-Rural area = 3, Village = 4 | |
| X11 | House Type | + | Block = 1, Bungalow = 2, Mud house and other = 3 | |||
| X12 | House quality | + | Property rights = 1 Lease and other = 2 | |||
| Personal economic situation | X13 | Annual income | - | Ten thousand Yuan (Ln) | ||
| X14 | Social insurance | - | No social insurance = 0, else = 1 | |||
| X15 | Commercial insurance | - | No commercial insurance = 0, else = 1 | |||
| Variables | N | Min | Max | Average | Std. | |
|---|---|---|---|---|---|---|
| Y | Ill-health score | 221,518 | 0.14 | 7.61 | 1.5522 | 1.66329 |
| S1 | Grade-A tertiary hospital per capita | 31 | 0.01 | 0.04 | 0.011 | 0.006 |
| S2 | Proportion of higher education population to total population | 31 | 5.29 | 31.5 | 9.00 | 3.82 |
| S3 | GDP per capita | 31 | 2.62 | 10.9 | 5.34 | 2.03 |
| S4 | Annual Average air pollution index (AQI) in 2010 | 31 | 37.86 | 108.91 | 69.12 | 9.48 |
| S5 | Average daily precipitation | 31 | 100.20 | 1555.36 | 828.26 | 355.89 |
| S6 | Average daily temperature | 31 | 15.78 | 247.84 | 144.59 | 44.23 |
| S7 | Average daily sunshine duration | 31 | 834.63 | 2493.64 | 1676.14 | 363.49 |
| Valid N | 31 | |||||
| X1 | Age | 222,179 | 60 | 109 | 69.731 | 7.84458 |
| X2 | Gender | 222,179 | 0 | 1 | 0.4777 | 0.4995 |
| X3 | Educational level | 221,445 | 1 | 6 | 2.1401 | 1.0509 |
| X4 | Marital Status | 218,772 | 1 | 2 | 1.2791 | 0.44856 |
| X5 | Ethnicity | 222,179 | 1 | 5 | 3.8798 | 1.75637 |
| X6 | Exercise frequency | 220,903 | 1 | 5 | 2.5233 | 1.66817 |
| X7 | Loneliness | 219,094 | 1 | 3 | 2.571 | 0.60939 |
| X8 | Social responsibility | 215,366 | 0 | 1 | 0.46 | 0.498 |
| X9 | Social activity | 215,706 | 0 | 1 | 0.92 | 0.27 |
| X10 | Place of residence | 222179 | 1 | 5 | 3.5357 | 1.66677 |
| X11 | House Type | 222179 | 1 | 2 | 1.0505 | 0.21896 |
| X12 | House quality | 220777 | 1 | 3 | 1.6342 | 0.71889 |
| X13 | Annual income | 218760 | −5.3 | 12.21 | 0.8541 | 1.20279 |
| X14 | Social insurance | 215395 | 0 | 1 | 0.0092 | 0.09541 |
| X15 | Commercial insurance | 218067 | 0 | 1 | 0.038 | 0.19126 |
| Valid N | 210488 | |||||
| Variables name | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | Model 6 | Model 7 | Model 8 | |
|---|---|---|---|---|---|---|---|---|---|
| Intercept | 1.829 *** | 1.788 *** | 1.996 *** | ||||||
| S1 | Grade-A tertiary hospital per capita | −0.027 ** | |||||||
| S2 | Proportion of higher education population to total population | −17.391 ** | |||||||
| S3 | GDP per capita | −0.803 *** | -- | ||||||
| S4 | Annual average AQI | -- | -- | ||||||
| S3× S4 | GDP per capita× Annual average AQI | -- | |||||||
| S5 | Average daily precipitation | -- | |||||||
| S6 | Average daily temperature | -- | |||||||
| S7 | Average daily sunshine duration | -- | |||||||
| Variables name | Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | ||
|---|---|---|---|---|---|---|---|
| Intercept | 0.173 | 3.000 *** | 2.738 *** | 2.683 *** | 2.972 *** | ||
| Determinants for health inequality at the provincial level | S1 | Grade-A tertiary hospital per capita | −0.911 * | −0.411 * | −0.330 * | −1.118 * | −0.551 * |
| S2 | Proportion of higher education population to total population | −0.131 * | −0.013 * | −0.013 * | −0.017 *** | −0.014 * | |
| S3 | GDP per capita | −0.411 *** | −0.050 *** | −0.049 *** | −0.060 *** | −0.052 *** | |
| Individual characteristics at the individual level(Control variable) | X1 | Age | 0.030 *** | 0.023 *** | 0.030 *** | 0.023 *** | 0.023 *** |
| X2 | Gender | −0.166 *** | −0.174 *** | −0.182 *** | −0.182 *** | −0.173 *** | |
| X3 | Educational level | −0.071 *** | −0.029 *** | −0.057 *** | −0.020 *** | −0.030 *** | |
| X4 | Marital status | −0.013 * | −0.302 *** | −0.013 | −0.303 *** | −0.303 *** | |
| X5 | Ethnicity | 0.050 *** | 0.037 *** | 0.014 ** | 0.009 * | 0.033 *** | |
| X6 | Exercise frequency | −0.156 *** | −0.109 *** | −0.107 *** | −0.105 *** | −0.109 *** | |
| Social interaction at the individual level (Control variable) | X7 | Loneliness | −0.542 *** | −0.525 *** | −0.532 *** | −0.523 *** | |
| X8 | Social responsibility | −0.211 *** | −0.206 *** | −0.214 *** | −0.201 *** | ||
| X9 | Social activity | −0.730 *** | −0.776 *** | −0.729 *** | −0.773 *** | ||
| Living Environment at the individual level | X10 | Place of residence | 0.022 *** | 0.047 *** | |||
| X11 | House type | 0.086 *** | 0.098 *** | ||||
| X12 | House quality | 0.060 *** | 0.062 *** | ||||
| X10×S3 | Place of residence×GDP per capita | −0.004 *** | |||||
| Economy at the individual level | X13 | Annual income | −0.027 *** | ||||
| X14 | Social insurance | −0.207 *** | |||||
| X15 | Commercial insurance | −0.088 *** | |||||
| AIC | 823615.9 | 767524.1 | 760488.6 | 762080.3 | 739731 | ||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan, C.; Ouyang, W.; Tian, L.; Song, Y.; Miao, W. Elderly Health Inequality in China and its Determinants: A Geographical Perspective. Int. J. Environ. Res. Public Health 2019, 16, 2953. https://doi.org/10.3390/ijerph16162953
Fan C, Ouyang W, Tian L, Song Y, Miao W. Elderly Health Inequality in China and its Determinants: A Geographical Perspective. International Journal of Environmental Research and Public Health. 2019; 16(16):2953. https://doi.org/10.3390/ijerph16162953
Chicago/Turabian StyleFan, Chenjing, Wei Ouyang, Li Tian, Yan Song, and Wensheng Miao. 2019. "Elderly Health Inequality in China and its Determinants: A Geographical Perspective" International Journal of Environmental Research and Public Health 16, no. 16: 2953. https://doi.org/10.3390/ijerph16162953