To contribute to the understanding of the accident causation model, a typical accident, Qingdao “11·22” oil leak and explosion of the Sinopec Donghuang pipelines, was selected as our case study. Additionally, the availability of the accident analysis method will be demonstrated in this section. Through analysis and discussion, readers will not only understand how and why this disaster occurred, but also remember key points in order to avoid similar mistakes within various industries.
3.2. Process Analysis
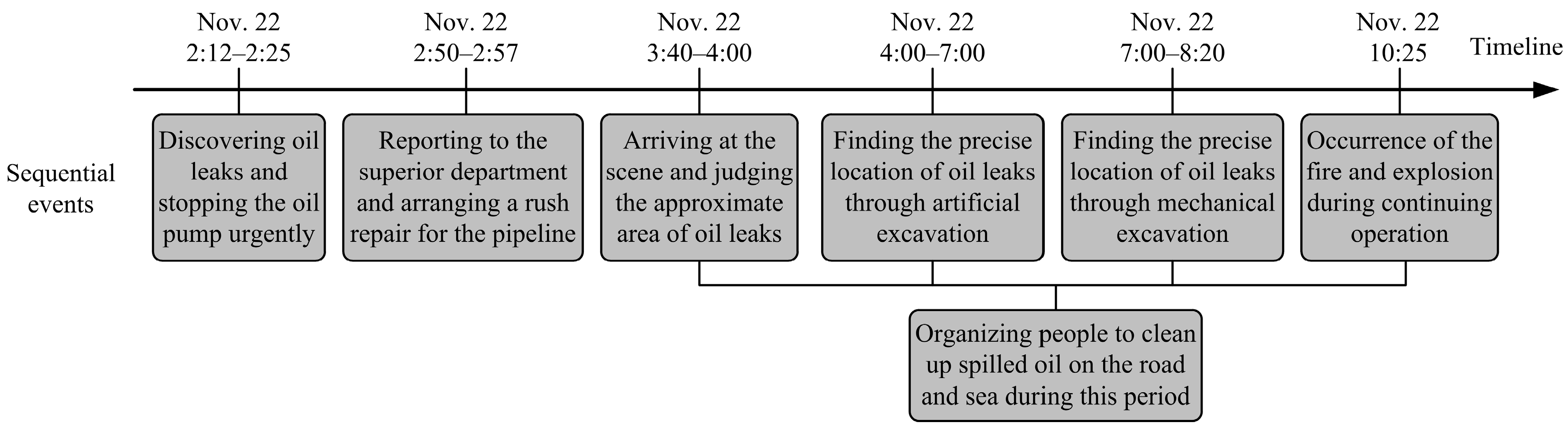
An accident is usually caused by sequential occurrences of multiple adverse events. This disaster began with an oil leak that further evolved into fires and explosions. Several sequential events were identified from the investigation report and are shown in
Figure 3 based on the timeline. The Donghuang oil pipeline is in total about 248.5 km in length, and the accident section was administrated by the Weifang oil transportation agency affiliated with Sinopec. On 22 November 2013, around 2:12 a.m. (local time), an operator on duty in the Weifang oil transportation agency discovered the pipeline leak through the reduction of the oil pressure. In this urgent situation, the manager stopped the oil pump (at 2:25 a.m.) immediately, and meanwhile, reported and arranged a rush repair. Technicians got to the scene at 3:40 a.m. and began to organize people to excavate after judging the approximate area of the underground broken pipeline. In order to improve the efficiency, excavators and hydraulic hammers were further used for digging and drilling. The precise location of the oil leak was eventually determined at about 8:20 a.m. Due to the serious corrosion of pipelines and large amount of oil leaks, the repair work continued for another two h and the explosion occurred during the process of mechanical excavation (at 10:25 a.m.).
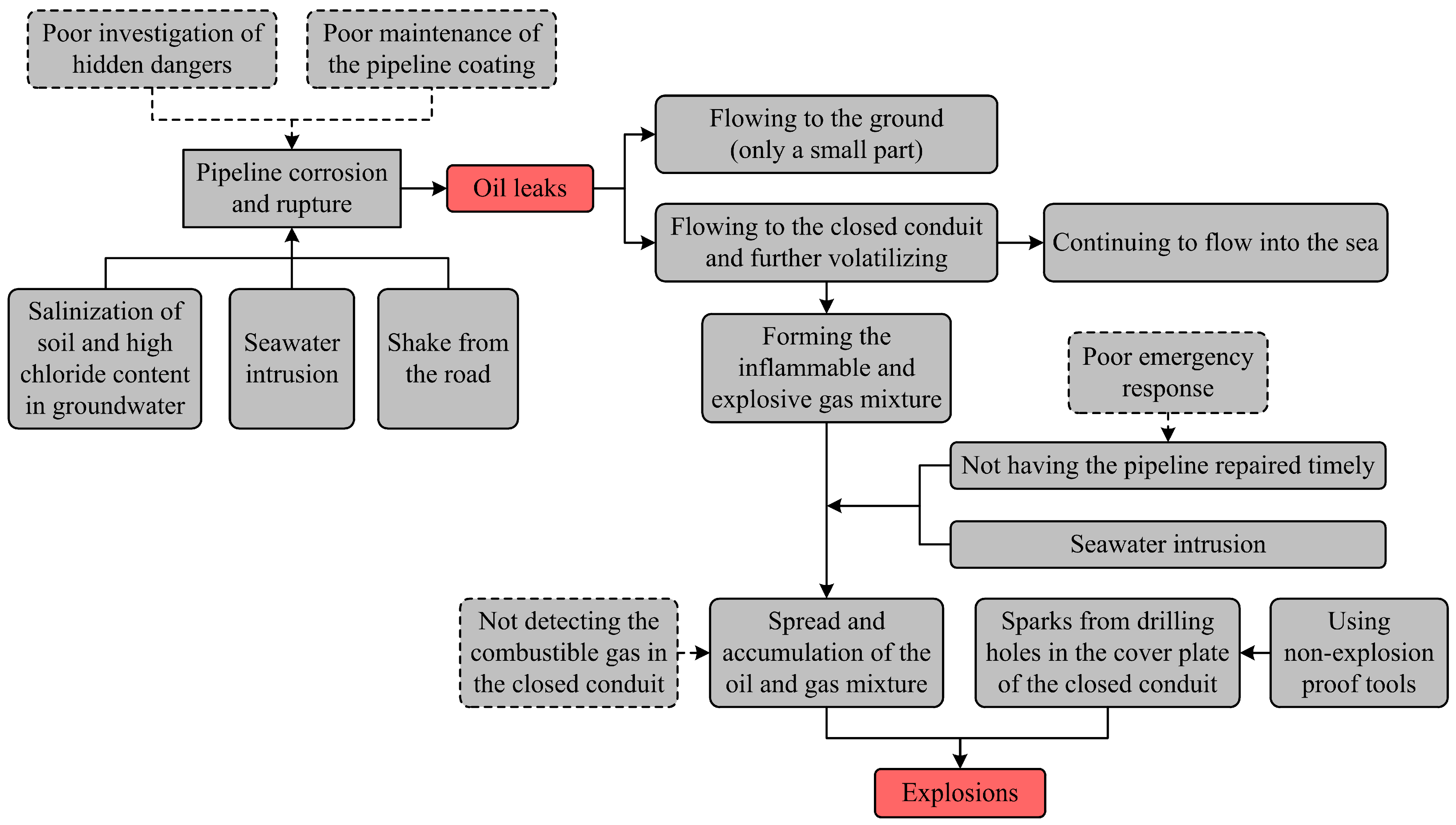
According to the timeline, the entire process of this accident can be divided into two critical events: (1) the oil leaks; (2) the explosion. For the sake of better illustration, an event sequence diagram (ESD) was developed (
Figure 4). The oil leaked out where the underground pipeline and closed conduit crossed. Seawater intrusion often occurs in the closed conduit due to the tide; this formed an alternate dry–wet and salt-spray environment and caused the salinization of soil and high chloride content in the groundwater. It is no wonder that the pipelines’ corrosion and rupture occurred in these conditions. A large amount of spilled oil flowed to the closed conduit and volatilized gradually, thus forming the inflammable and explosive gas mixture. When the rush repair was underway, the oil and gas mixture, affected by the seawater intrusion, spread and accumulated quickly in this space.
It should be noted more than eight h passed after the leaks were discovered, but repair of the broken pipelines was not completed because of poor emergency disposal. According to estimation, the total amount of oil leakage from the ground, closed conduit, and sea was up to 2000 tons during this period. However, people on site were not aware of the risk and still used non-explosion-proof tools to open the cover plate of the closed conduit without taking protective measures. The oil and gas mixture ignited and detonated from the exposed sparks of the mechanical drilling.
The explosion seriously destroyed the block and caused extensive marine pollution. The damaged pipelines located in the dangerous section were discontinued and the closed conduit was transformed into an open one for the sightseeing and warning. The compared accident scenes of the present and past can be seen in
Figure 5.
3.3. Causes Analysis
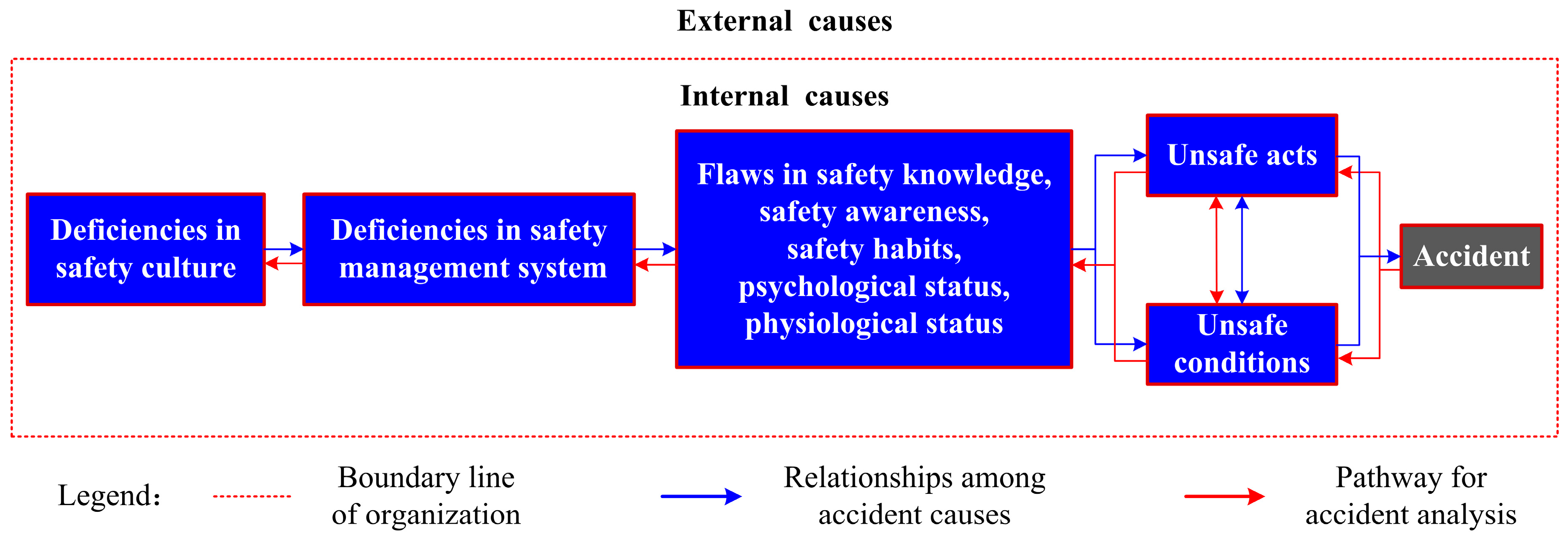
Through the process analysis above, two critical events (i.e., the oil leaks and the explosion) have been identified from this disaster and the cause analysis will be centered on them. There are large differences between the causes of the two events, especially in respect to individual causes; therefore, the analysis results are shown in separate models for the sake of clear and logical illustration.
The accident section of the Donghuang oil pipeline is administrated by Weifang oil transportation agency, and the on-site personnel such as the management, repairmen, excavator operators, etc. are all employed by this unit. Therefore, Weifang oil transportation agency should take full responsibility for the accident. Causes in relation to this organization, usually considered as the internal ones, are of crucial importance. Additionally, this accident involved several local government agencies (e.g., the supervision department of work safety, the planning and design department, the office of emergency management, etc.) whose faults could also have contributed to the oil leaks and explosion. The internal causes illustrated in the improved accident causation model are shown in
Figure 6 and
Figure 7, respectively.
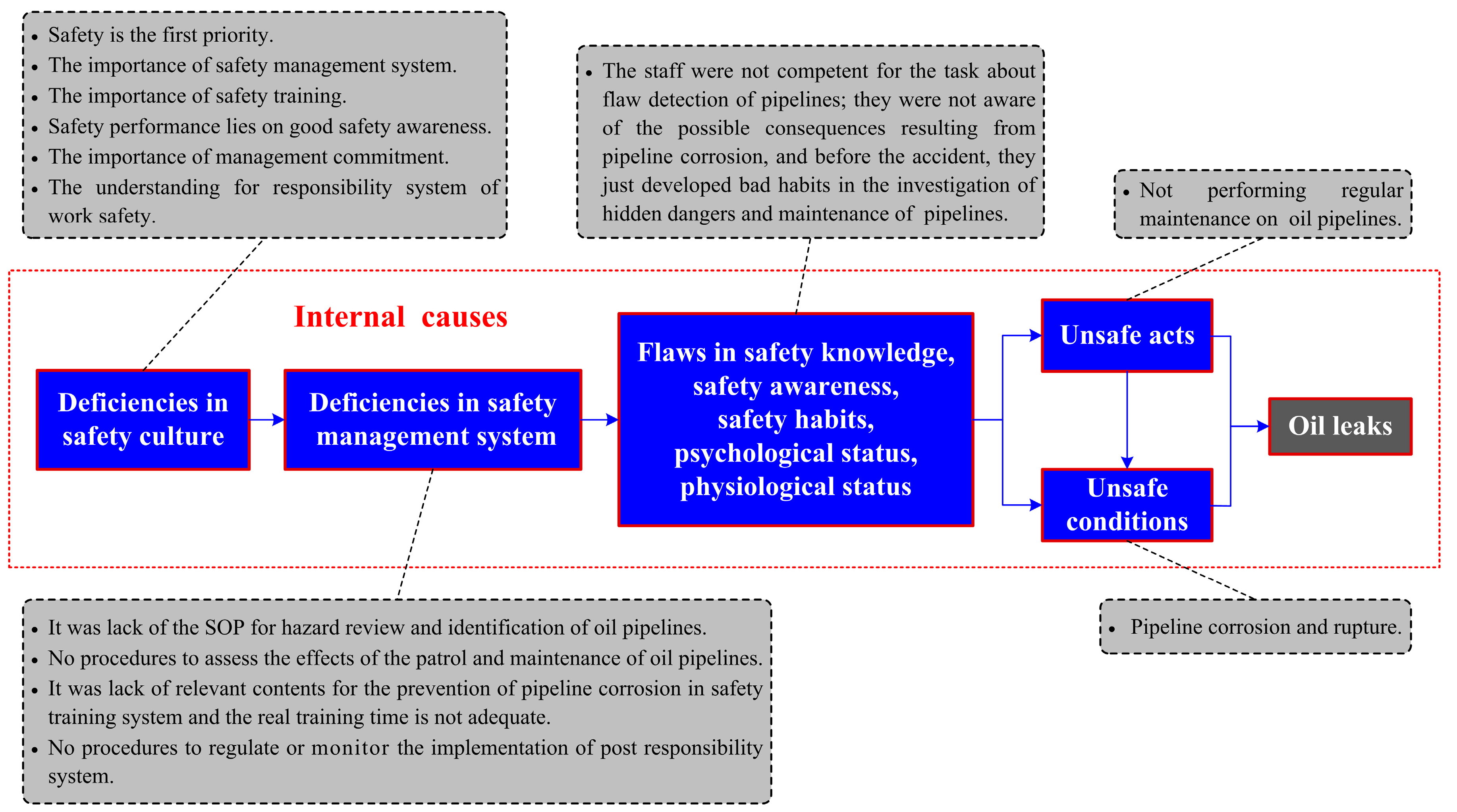
3.3.1. The Oil Leaks
The corrosion and rupture of the pipeline, which was considered to be the unsafe condition cause, directly led to the oil leaks. The pipelines corroded easily due to the effect of bad local hydrogeological conditions such as the salt-spray environment, salinization of soil, and high content of chloride in the groundwater. The Oil and Gas Pipelines Protection Law of the People’s Republic of China (PRC) (article 23) stipulates that pipeline enterprises shall conduct regular detection and maintenance of pipelines to ensure that they are in good condition; the sections and sites with high risks shall be monitored in a critical manner, and effective measures shall be taken to prevent pipeline accidents. However, employees in the Weifang oil transportation agency did not do this work well according to the rules, and the coating overhaul for the Donghuang oil pipelines that began in 2011 had not yet been finished before the incident. The organization’s nonfeasance caused the corrosion and rupture to exist for a long time, and we believe it caused the unsafe condition indirectly. Thus, this also provides an effective way to prevent some unsafe conditions, namely by turning to the elimination of corresponding unsafe acts.
The flaws in individuals’ safety knowledge, safety awareness, and safety habits resulted in the unsafe acts directly. As the investigation noted, Weifang oil transportation carried out a total of three flaw detections on the Donghuang oil pipelines during 2009–2013, but the staff in charge of the work failed to find the pipeline’s corrosion and rupture during their inspections; therefore they might not be qualified for the technical task because of their lack of knowledge and experience. All members in the organization should attach importance to their job responsibilities, especially managers, whose poor inspection and supervision remain very important factors for the occurrence of unsafe acts. However, people who were in charge of the regular maintenance of equipment and facilities did not abide by the rules and neglected the overhaul of the pipelines in production. Based on this, we can deduce that the staff were neither aware of the adverse consequences resulting from pipeline corrosion nor had good habits to carry out the regular maintenance of the pipeline.
The roots of an accident lie in the errors of an organization; moreover, individual behaviors are largely affected by organizational factors [
8]. Therefore, the deficiencies in an organizational safety management system and safety culture could be inferred according to the above analysis on individual flaws.
According to the Safety Specification for Crude Oil and Natural Gas Pipelines (article 8), several deficient elements, such as hazard identification, safety training and education, safety accountability, and equipment management (i.e., the maintenance and detection for oil pipelines), were identified from the safety management system of the Weifang oil transportation agency. The lack of a standard operating procedure (SOP) for hazard identification led to the staff’s inadequate training and insufficient knowledge. This made them fail to identify the pipeline’s hidden dangers in the process of past flaw detections (a total of three times in 2009, 2011, and 2013). Before this accident, the on-site staff had already performed regular patrol and maintenance for the oil pipelines, but the corrosion and rupture were not prevented effectively because there was no procedure or process in the safety management system to assess the effect of the implementation of engineering standards. Safety training, as one of the most important means for accident prevention, was not well conducted in the Weifang oil transportation agency. There were no adequate theoretical contents about the prevention of pipeline corrosion in the training document. Some operating skills about the pipelines’ detection were not trained well in accordance with engineering standards; moreover, the specified training time for employed front-line workers was not sufficient. The flawed organizational roles caused the ambiguous assignment of responsibilities for the protection of operational safety within the Weifang oil transportation agency. The violation of regulations reflected that the post responsibility system was not valued by the operators and managers, and the organization did not establish processes to monitor its daily implementation either.
The deficient safety management system indicated that members in the organization did not reach an agreement on safety beliefs such as “safety is the first priority”, “the importance of safety management system”, “the importance of safety training”, “the importance of laws and engineering standards” or “safety performance depends on good safety awareness”. Good leadership can contribute to a good safety climate. The key role for leaders and managers is to develop and drive a culture for safety management within the organization. The staff in the Weifang oil transportation agency ignored that safety should be put first in daily work and they did not pay much attention to the roles of safety awareness and the responsibility system for accident prevention. Moreover, the top management failed to demonstrate their commitment to support the implementation and audit of the safety management system. Collectively, managers and leaders should provide the organizational systems and drive the organizational culture that determines not only what people in the organization do, but more importantly, how they do it.
In addition, there were several external factors related to the occurrence of the oil leaks. The local supervision department of work safety who is the lead unit for the protection of underground pipelines failed to perform its supervision duties well because the coating overhaul for the Donghuang oil pipelines was not finished within two years. Moreover, it failed to urge the pipeline enterprise to carry out the hazard identification and regular maintenance for oil pipelines and did not realize the closed-loop management of the safety inspection through the form of “reviewing”. There was also some irrationality in the layout of the oil pipelines approved by the local planning and design department, which had a great impact on the occurrence of the oil leaks. As mentioned above, the oil pipeline around the accident site was installed in a closed conduit, which posed a higher risk when the leaked oil easily flowed into the conduit and caused inconvenience for the maintenance and rush repair of the installation. In view of this, the damaged pipelines located in the dangerous section are now out of use.
3.3.2. The Explosions
Another two unsafe acts made the oil leaks further evolve into multiple explosions and large-scale fires. During the rush repair, the closed conduit was full of inflammable and explosive mixtures of oil and gas due to the seawater intrusion, thus causing another dangerous condition. According to the Oil and Gas Pipelines Protection Law of the PRC (article 30), it is forbidden to use mechanical tools for excavation and construction within five meters on both sides of the center line of the pipeline. The spark, a requirement for this accidental event, was just generated from drilling holes in the cover plate with a non-explosion-proof hydraulic hammer. If on-site staff performed effective gas detection for the closed conduit in accordance with the operating procedures stipulated in Safety Specification for Crude Oil and Natural Gas Pipelines (article 8.4) before the excavation, this explosion could have been avoided. Indeed, this disaster was classified as an “accountability accident” by the SAWS and almost all unsafe acts violated regulations or engineering standards; therefore, identifying and eliminating those specific unsafe acts is of crucial importance for the prevention of such similar mistakes.
Safe acts or unsafe acts, by the accident causation model, are directly determined by individuals’ habitual behaviors such as competence, awareness, thought, habit, etc. The two unsafe acts above were produced by the staff involved in the oil pipeline’s rush repair. As the investigation report noted, the management and employed front-line workers at the scene were not trained adequately and lacked the experience to rush repair the underground pipelines. They did not know how inflammable and explosive gases formed, nor did they understand why the mixture spread and accumulated in the closed conduit. According to the survey, most people did not even have the theoretical knowledge about the chemical property of crude oil and did not think that it could be easily detonated like refined oil (e.g., gasoline, diesel oil, etc.). Also, the staff was not aware of the consequences of using non-explosion-proof tools and developed bad habits in the process of daily operations since accidental events had not occurred in the past. It is therefore no wonder that unsafe acts appeared in this event.
The poor disposal of the oil leak indicates that there are also lots of flaws in some elements of the Weifang oil transportation agency’s safety management system, such as equipment management (i.e., the regulation for repair), risk assessment and mitigation, safety training and education, emergency response planning, etc. The repair of underground oil pipelines is a high-risk task and the organization must establish a comprehensive SOP in the management system according to related engineering standards for managers and operators. The personnel allocation (operators and supervisors), tools selection, job steps, and protective measures should be detailed in this procedure. However, the Weifang oil transportation agency was not aware of the risks in the repair of leaked oil pipelines and neglected the importance of safety procedures. This also caused deficiencies in other systems or plans. Some contents about the SOP, especially the danger of using non-explosion-proof tools in the repair of oil pipelines, were not given in the safety training system, and the occurrence of the explosions also had a lot to do with peoples’ lack of knowledge and bad treatment in the rush repair. As we know, the leaks of oil pipelines can easily trigger domino events once disposed improperly. According to the survey, there was no procedure or process in the safety management system to assess the risk of the area where the pipeline leaked, and protective measures were not taken by the organization, either. Additionally, emergency plans about the pipeline leaks need to be mastered and exercised by all concerned but the management failed to ensure that emergency training was provided as intended. According to the investigation, the regular exercise for pipeline leaks was actually carried out by the Weifang oil transportation agency, but there was no procedure or process in the safety management system to assess the effect of its implementation and the emergency response plan was not performed and audited all the time.
There are no significant differences in the deficiencies of organizational safety culture elements between the analyses of the two critical events; thus, analyses in this section will be simplified. The occurrence of explosions indicated that the members’ inadequate consensus on safety beliefs such as “safety is the first priority”, “the importance of safety management system”, “the importance of safety training”, “safety performance lies on good safety awareness”, “the importance of laws and engineering standards”, etc. could be inferred as poor safety culture. The quality of leadership and commitment to safety can drive or limit the safety culture of an organization. However, the leaders and managers in the Weifang oil transportation agency failed to deeply understand the process safety management (PSM) program—its importance for maintaining both safe operations and compliance, its key roles and responsibilities, as well as current issues and challenges the organization faced in its implementation. As mentioned above, improper disposal of the oil leaks triggered the multiple explosions; clearly, Weifang oil transportation agency neglected the importance of emergency management for the PSM. The management should promote all staff to master the emergency plan and supervise its implementation and regular audit.
In addition, there were several external factors contributing to the explosion and serious casualties. The local administration committee of the development zone failed to fully understand the severity of the crude oil leakage and initially classified it as a general emergency (total four levels: particularly serious, serious, major, and general) based only on the report of the pipeline enterprise. This led to a poor command and coordination for the emergency: warning and road closure measures were not taken on the site; the nearby masses were not notified and evacuated in a timely manner; and problems such as violations of regulations from on-site emergency personnel were not found and stopped. Moreover, the local office of emergency management did not organize experts to carry out the research and assessment on the development trend of the oil leaks and thus failed to raise the level of the emergency response timely. Therefore, it was not surprising that the multiple explosions occurred, and the casualties and property losses were so severe.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}