Bone Mineral Density and Bone Turnover Markers in Postmenopausal Women Subjected to an Aqua Fitness Training Program

 ,
, 
Abstract
1. Introduction
2. Material and Methods
2.1. Participants
2.2. Training Program
2.3. Bone Density Measurements
2.4. Biochemical Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nguyen, V.H. Osteoporosis prevention and osteoporosis exercise in community-based public health programs. Osteoporos. Sarcopenia 2016, 3, 18–31. [Google Scholar] [CrossRef] [PubMed]
- Durden, E.; Pinto, L.; Lopez-Gonzalez, L.; Juneau, P.; Barron, R. Two-year persistence and compliance with osteoporosis therapies among postmenopausal women in a commercially insured population in the United States. Arch. Osteoporos. 2017, 12, 22. [Google Scholar] [CrossRef] [PubMed]
- Kemmler, W.; Klaus, E.; Von Stengel, S. Long-term exercise and bone mineral density changes in postmenopausal women—Are there periods of reduced effectiveness? J. Bone Miner. Res. 2016, 31, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Caputo, E.L.; Costa, M.Z. Influence of physical activity on quality of life in postmenopausal women with osteoporosis. Rev. Bras. Reum. 2014, 54, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Kostka, J.; Kostka, T.; Borowiak, E. Physical Activity in Older Adults in Relation to Place of Residence and Coexistent Chronic Diseases. J. Phys. Act. Health 2017, 14, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Kelley, G.A.; Kelley, K.S.; Kohrt, W.M. Effects of ground and joint reaction force exercise on lumbar spine and femoral neck bone mineral density in postmenopausal women: A meta-analysis of randomized controlled trials. BMC Musculoskelet. Disord. 2012, 13, 177. [Google Scholar] [CrossRef]
- James, M.M.S.; Carroll, S. High-intensity resistance training and postmenopausal bone loss: A meta-analysis. Osteoporos. Int. 2006, 17, 1225–1240. [Google Scholar] [CrossRef]
- Morseth, B.; Emaus, N.; Jørgensen, L. Physical activity and bone: The importance of the various mechanical stimuli for bone mineral density. Rev. Nor. Epidemiologi 2011, 20, 173–178. [Google Scholar] [CrossRef]
- Kohrt, W.M.; Barry, D.W.; Schwartz, R.S. Muscle Forces or Gravity: What Predominates Mechanical Loading on Bone? Med. Sci. Sports Exerc. 2009, 41, 2050–2055. [Google Scholar] [CrossRef]
- Gómez-Bruton, A.; González-Agüero, A.; Gómez-Cabello, A.; Matute-Llorente, A.; Casajús, J.A.; Vicente-Rodríguez, G. The effects of swimming training on bone tissue in adolescence. Scand. J. Med. Sci. Sports 2015, 25, e589–e602. [Google Scholar] [CrossRef]
- Akgül, S.; Kanbur, N.; Cinemre, Ş.A.; Karabulut, E.; Derman, O. The effect of swimming and type of stroke on bone metabolism in competitive adolescent swimmers: A pilot study. Turk. J. Med. Sci. 2015, 45, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Mattos de, F.; Leite, N.; Pitta, A.; Bento, P.C. Effects of aquatic exercise on muscle strength and functional performance of individuals with osteoarthritis: A systematic review. Rev. Bras. Reum. 2016, 56, 530–542. [Google Scholar] [CrossRef] [PubMed]
- Simas, V.; Hing, W.; Pope, R.; Climstein, M. Effects of water-based exercise on bone health of middle-aged and older adults: A systematic review and meta-analysis. Open Access J. Sports Med. 2017, 8, 39–60. [Google Scholar] [CrossRef] [PubMed]
- Tsukahar, N.; Toda, A.; Goto, J.; Ezawa, I. Cross-sectional and longitudinal studies on the effect of water exercise in controlling bone loss in Japanese postmenopausal women. J. Nutr. Sci. Vitaminol. 1993, 40, 37–47. [Google Scholar] [CrossRef][Green Version]
- Harumia, Y.; Satoru, Y. The relationship between swimming exercise and bone density. A cohort study among middle aged women. Dokkyo J. Med. Sc. 2000, 27, 105–111. [Google Scholar]
- Rotstein, A.; Harush, M.; Vaisman, N. The effect of a water exercise program on bone density of postmenopausal women. J. Sports Med. Phys. Fit. 2008, 48, 352–359. [Google Scholar]
- Balsamo, S.; Da Mota, L.M.; De Santana, F.S.; Nascimento, D.; Bezerra, L.M.; Balsamo, D.O.; Borges, J.L.; De Paula, A.P.; Bottaro, M. Resistance training versus weight-bearing aquatic exercise: A cross-sectional analysis of bone mineral density in postmenopausal women. Rev. Bras. Reum. 2013, 53, 193–198. [Google Scholar] [CrossRef]
- Torres-Ronda, L.; I. del Alcazar, X.S. The properties of water and their applications for training. J. Hum. Kinet. 2014, 44, 237–248. [Google Scholar] [CrossRef]
- Faulkner, K.G.; Wacker, W.K.; Barden, H.S.; Simonelli, C.; Burke, P.K.; Ragi, S.; Del Rio, L. Femur strength index predicts hip fracture independent of bone density and hip axis length. Osteoporos. Int. 2006, 17, 593–599. [Google Scholar] [CrossRef]
- Yoshikawa, T.; Turner, C.H.; Peacock, M.; Slemenda, C.W.; Weaver, C.M.; Teegarden, D.; Markwardt, P.; Burr, D.B. Geometric structure of the femoral neck measured using dual-energy X-ray absorptiometry. J. Bone Miner. Res. 1994, 9, 1053–1064. [Google Scholar] [CrossRef]
- Tarrant, S.M.; Hardy, B.M.; Byth, P.L.; Brown, T.L.; Attia, J.; Balogh, Z.J. Preventable mortality in geriatric hip fracture inpatients. Bone Jt. J. 2014, 96, 1178–1184. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gómez-Bruton, A.; Montero-Marín, J.; González-Agüero, A.; Gómez-Cabello, A.; García-Campayo, J.; Moreno, L.A.; Casajús, J.A.; Vicente-Rodríguez, G. Swimming and peak bone mineral density: A systematic review and meta-analysis. J. Sports Sci. 2018, 36, 365–377. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Bruton, A.; Gonzalez-Aguero, A.; Gomez-Cabello, A.; Casajus, J.A.; Vicente-Rodriguez, G. Is Bone Tissue Really Affected by Swimming? A Systematic Review. PLoS ONE 2013, 8, e70119. [Google Scholar] [CrossRef] [PubMed]
- Murtezani, A.; Nevzati, A.; Ibraimi, Z.; Sllamniku, S.; Meka, V.S.; Abazi, N. The effect of land versus aquatic exercise program on bone mineral density and physical function in postmenopausal women with osteoporosis: A randomized controlled trial. Ortop. Traumatol. Rehabil. 2014, 16, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Friedman, A. Important determinants of bone strength: Beyond bone mineral density. J. Clin. Rheumatol. 2006, 12, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Parimi, N.; Orwoll, E.S.; Black, D.M.; Schousboe, J.T.; Eastell, R. Association of incident hip fracture with the estimated femoral strength by finite element analysis of DXA scans in the Osteoporotic Fractures in Men (MrOS) study. Osteoporos. Int. 2017, 29, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Palermo, L.; Black, D.M.; Eastell, R. Prediction of incident hip fracture with the estimated femoral strength by finite element analysis of DXA Scans in the Study of Osteoporotic Fractures. J. Bone Miner. Res. 2014, 29, 2594–2600. [Google Scholar] [CrossRef] [PubMed]
- Wendlova, J. Femur strength index versus bone mineral density: New findings (slovak epidemiological study). Vnitr. Lek. 2010, 56, 764–770. [Google Scholar]
- Greenblatt, M.B.; Tsai, J.N.; Wein, M.N. Bone turnover markers in the diagnosis and monitoring of metabolic bone disease. Clin. Chem. 2017, 63, 464–474. [Google Scholar] [CrossRef]
- Zoch, M.L.; Clemens, T.L.; Riddle, R.C. New insights into the biology of osteocalcin. Bone 2016, 82, 42–49. [Google Scholar] [CrossRef]
- Papadakis, G.; Keramidas, I.; Kakava, K.; Pappa, T.; Villiotou, V.; Triantafillou, E.; Drosou, A.; Tertipi, A.; Kaltzidou, V.; Pappas, A. Seasonal variation of serum vitamin D among Greek female patients with osteoporosis. In Vivo 2015, 29, 409–413. [Google Scholar]
- Kasprzak, Z.; Pilaczyńska-Szcześniak, Ł. Effects of regular physical exercises in the water on the metabolic profile of women with abdominal obesity. J. Hum. Kinet. 2014, 41, 71–79. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameters | Assessment at Baseline | Assessment at 6 Months | |
|---|---|---|---|
| Body mass (kg) | T | 71.16 (11.10); 71.50 (65.80–73.70) | 71.34 (11.90); 68.30 (64.70–74.30) |
| C | 77.06 (13.85); 78.70 (66.10–86.10) | 77.26 (13.95); 78.70 (65.10–87.00) | |
| BMI (kg/m2) | T | 27.49 (3.48); 28.28 (24.24–28.60) | 27.72 (3.92); 27.00 (25.10–29.00) |
| C | 28.54 (4.39); 28.08 (24.73–32.55) | 28.78 (4.51); 29.00 (25.10–32.50) | |
| Total fat (%) | T | 41.07 (5.97); 40.10 (39.30–45.60) | 40.46 (6.29); 39.60 (38.50–45.10) |
| C | 41.28 (6.68); 44.50 (35.80–47.50) | 41.29 (6.57); 44.20 (36.00–46.30) | |
| Lean body mass (kg) | T | 39.71 (4.42); 40.46 (37.71–41.36) | 40.18 (3.89); 40.60 (37.38–41.90) |
| C | 42.65 (4.14); 41.41 (40.45–45.61) | 42.82 (4.35); 41.34 (40.156–44.00) | |
| Total fat (kg) | T | 28.30 (7.98); 27.50 (24.39–30.74) | 28.10 (8.88); 26.96 (24.49–29.83) |
| C | 31.22 (10.13); 36.12 (22.32–37.68) | 31.31 (10.04); 36.70 (22.06–38.12) | |
| Android fat tissue (%) | T | 45.17 (8.14); 45.70 (42.70–51.80) | 43.83 (9.41); 44.00 (42.10–50.00) |
| C | 46.34 (8.16); 44.80 (39.70–54.20) | 45.90 (7.72); 45.70 (40.20–53.10) | |
| Gynoid fat tissue (%) | T | 48.09 (5.08); 50.10 (44.90–52.00) | 46.79 (4.96); 47.70 (43.40–50.50) |
| C | 45.96 (6.48); 47.30 (42.10–51.30) | 45.88 (5.66); 45.90 (43.70–50.20) |
| Parameters | Assessment at Baseline | Assessment at 6 Month | |
|---|---|---|---|
| Total BMD (g/cm2) | T | 1.12 (0.13); 1.09 (1.05–1.21) | 1.11 (0.11); 1.09 (1.07–1.19) |
| C | 1.13 (0.08); 1.14 (1.11–1.16) | 1.13 (0.08); 1.14 (1.13–1.14) | |
| BMD L1–L4 (g/cm2) | T | 1.05 (0.21); 1.02 (0.91–1.21) | 1.04 (0.20); 1.00 (0.87–1.18) |
| C | 1.11 (0.09); 1.11 (1.08–1.19) | 1.11 (0.10); 1.13 (1.05–1.17) | |
| BMD total femur (g/cm2) | T | 0.95 (0.16); 0.93 (0.83–1.11) | 0.94 (0.16); 0.91 (0.83–1.12) |
| C | 0.94 (0.09); 0.95 (0.90–0.96) | 0.94 (0.10); 0.94 (0.89–0.96) | |
| BMD femoral neck (g/cm2) | T | 0.90 (0.16); 0.88 (0.76–1.08) | 0.90 (0.16); 0.88 (0.77–1.06) |
| C | 0.90 (0.09); 0.92 (0.85–0.98) | 0.90 (0.09); 0.93 (0.83–0.97) | |
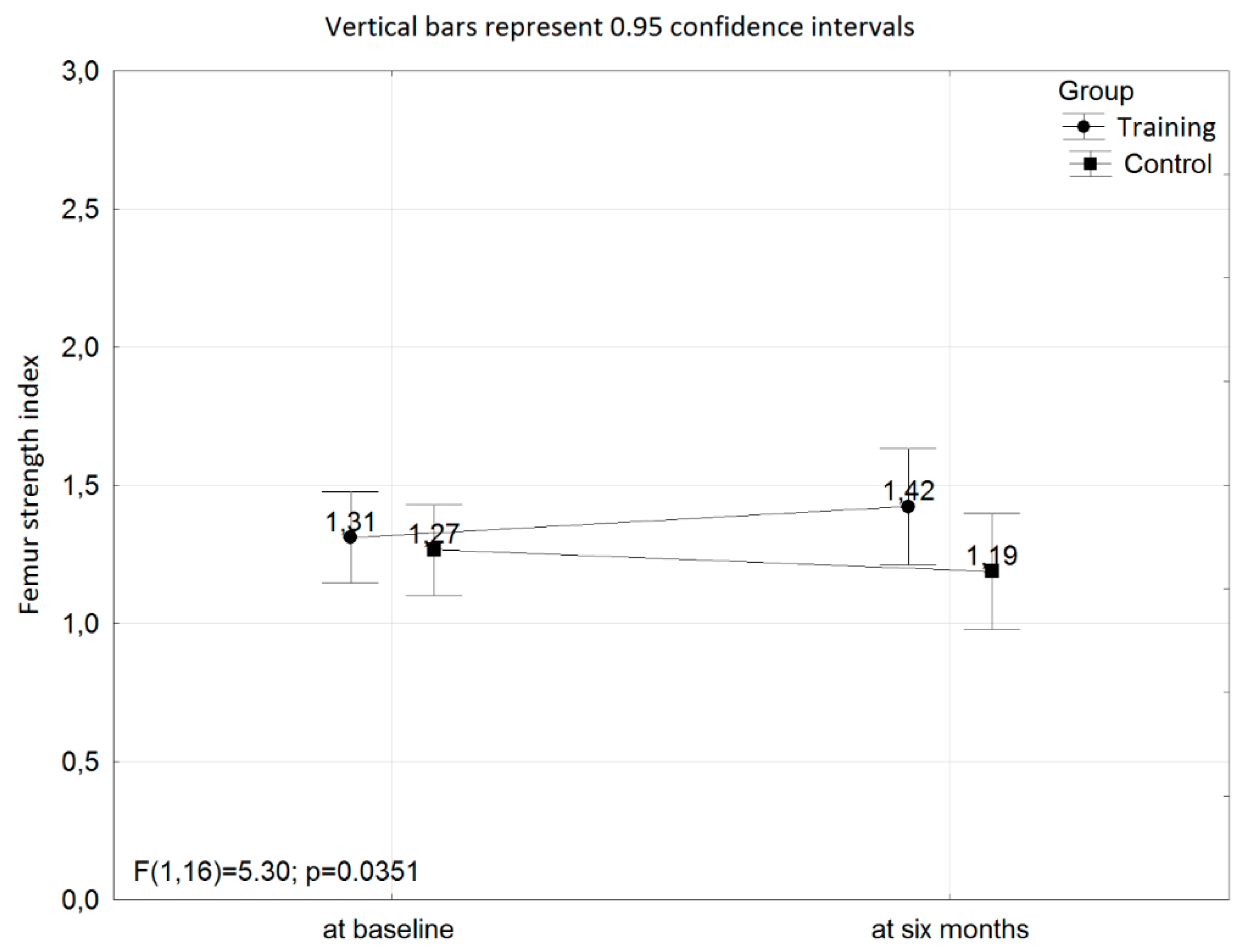
| Femur strength index (N) | T | 1.31 (0.28); 1.30 (1.20–1.50) | 1.42 (0.34); 1.40 (1.20–1.70) * |
| C | 1.27 (0.18); 1.30 (1.20–1.40) | 1.19 (0.24); 1.10 (1.10–1.40) | |
| T–score L1–L4 | T | −1.06 (1.73); −1.30 (−2.20–0.20) | −1.19 (1.69); −1.50 (−2.6–0.00) |
| C | −0.57 (0.77); −0.60 (−0.90–0.10) | −0.60 (0.81); −0.50 (−1.10–−0.10) | |
| T–score total femur | T | −0.48 (1.28); −0.70 (−1.40–0.80) | −0.52 (1.28); −0.80 (−1.50–0.90) |
| C | −0.50 (0.70); −0.50 (−0.90–−0.40) | −0.52 (0.82); −0.50 (−0.90–−0.40) | |
| T–score femoral neck | T | −1.00 (1.18); −1.20 (−2.00–0.30) | −1.01 (1.16); −1.10 (−2.00–0.20) |
| C | −1.01 (0.65); −0.90 (−1.40–−0.40) | −1.00 (0.65); −0.70 (−1.50–−0.50) | |
| OC (ng/mL) | T | 1.47 (0.67); 1.39 (1.17–1.92) | 1.78 (1.00); 1.53 (1.20–2.37) |
| C | 1.70 (0.70); 1.84 (1.04–2.17) | 1.69 (0.80); 1.73 (0.94–2.30) | |
| CTX (ng/mL) | T | 0.36 (0.10); 0.30 (0.29–0.37) | 0.38 (0.11); 0.35 (0.32–0.42) |
| C | 0.53 (0.37); 0.44 (0.27–0.66) | 0.56 (0.22); 0.61 (0.34–0.73) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wochna, K.; Nowak, A.; Huta-Osiecka, A.; Sobczak, K.; Kasprzak, Z.; Leszczyński, P. Bone Mineral Density and Bone Turnover Markers in Postmenopausal Women Subjected to an Aqua Fitness Training Program. Int. J. Environ. Res. Public Health 2019, 16, 2505. https://doi.org/10.3390/ijerph16142505
Wochna K, Nowak A, Huta-Osiecka A, Sobczak K, Kasprzak Z, Leszczyński P. Bone Mineral Density and Bone Turnover Markers in Postmenopausal Women Subjected to an Aqua Fitness Training Program. International Journal of Environmental Research and Public Health. 2019; 16(14):2505. https://doi.org/10.3390/ijerph16142505
Chicago/Turabian StyleWochna, Krystian, Alicja Nowak, Anna Huta-Osiecka, Katarzyna Sobczak, Zbigniew Kasprzak, and Piotr Leszczyński. 2019. "Bone Mineral Density and Bone Turnover Markers in Postmenopausal Women Subjected to an Aqua Fitness Training Program" International Journal of Environmental Research and Public Health 16, no. 14: 2505. https://doi.org/10.3390/ijerph16142505
APA StyleWochna, K., Nowak, A., Huta-Osiecka, A., Sobczak, K., Kasprzak, Z., & Leszczyński, P. (2019). Bone Mineral Density and Bone Turnover Markers in Postmenopausal Women Subjected to an Aqua Fitness Training Program. International Journal of Environmental Research and Public Health, 16(14), 2505. https://doi.org/10.3390/ijerph16142505