Effectiveness of Interventions to Promote Sustainable Employability: A Systematic Review



Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Methodological Quality Assessment
2.3. Data Extraction
3. Results
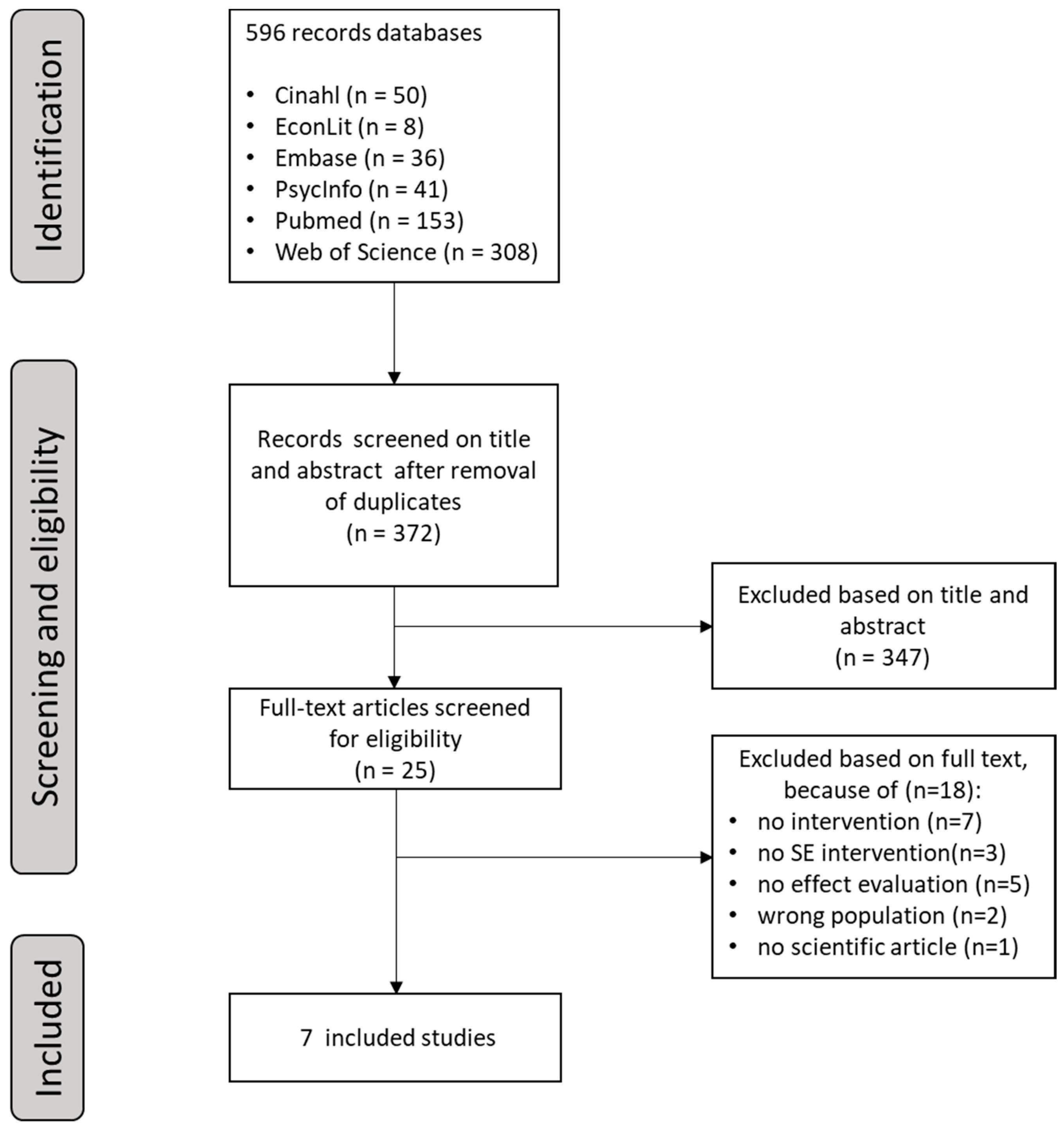
3.1. Selection of Articles
3.2. Methodological Quality of the Studies
3.3. Data Extraction
3.4. Content and Effectiveness of SE Interventions
3.5. Content and Effectiveness of SE Interventions in the Light of the Four SE Core Components
4. Discussion
4.1. Study Strengths and Limitations
4.2. Recommendations for Future Research and Practical Implications
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Detaille, S. Trends en ontwikkelingen op de arbeidsmarkt (Trends and developments on the labour market). In Fit for the Future; Vakmedianet: Alphen aan den Rijn, The Netherlands, 2018; pp. 20–27. [Google Scholar]
- de Jonge, J.; Peeters, M.C.W. The Vital Worker: Towards Sustainable Performance at Work. Int. J. Environ. Res. Public Health 2019, 16, 910. [Google Scholar] [CrossRef] [PubMed]
- Fleuren, B.B.; de Grip, A.; Jansen, N.W.; Kant, I.; Zijlstra, F.R. Critical reflections on the currently leading definition of sustainable employability. Scand. J. Work Environ. Health 2016, 42, 557–560. [Google Scholar] [CrossRef] [PubMed]
- van der Klink, J.J.; Bultmann, U.; Burdorf, A.; Schaufeli, W.B.; Zijlstra, F.R.; Abma, F.I.; Brouwer, S.; van der Wilt, G.J. Sustainable employability—Definition, conceptualization, and implications: A perspective based on the capability approach. Scand. J. Work Environ. Health 2016, 42, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Sen, A.K. The Idea of Justice; Allen Lane: London, UK, 2009. [Google Scholar]
- van der Klink, J.J.; Burdorf, A.; Schaufeli, W.B.; van der Wilt, G.J.; Zijlstra, F.R.H.; Brouwer, S.; Bültmann, U. Duurzaam Inzetbaar: Werk als Waarde (Sustainably Employable: The Value of Work); ZonMw: Den Haag, The Netherlands, 2010. [Google Scholar]
- Rongen, A.; Robroek, S.J.; van Lenthe, F.J.; Burdorf, A. Workplace health promotion: A meta-analysis of effectiveness. Am. J. Prev. Med. 2013, 44, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Burdorf, A. Kennissynthese Werk(en) is Gezond (Knowledge Synthesis Work(ing) is Healthy); Een Studie in Opdracht van ZonMw; ZonMw: Den Haag, The Netherlands, 2016. [Google Scholar]
- Tonnon, S.C.; van der Veen, R.; Westerman, M.J.; Robroek, S.J.; van der Ploeg, H.P.; van der Beek, A.J.; Proper, K.I. The Employer Perspective on Sustainable Employability in the Construction Industry. J. Occup. Environ. Med. 2017, 59, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Oakman, J.; Neupane, S.; Proper, K.I.; Kinsman, N.; Nygard, C.H. Workplace interventions to improve work ability: A systematic review and meta-analysis of their effectiveness. Scand. J. Work Environ. Health 2018, 44, 134–146. [Google Scholar] [CrossRef] [PubMed]
- Cloostermans, L.; Bekkers, M.B.; Uiters, E.; Proper, K.I. The effectiveness of interventions for ageing workers on (early) retirement, work ability and productivity: A systematic review. Int. Arch. Occup. Environ. Health 2015, 88, 521–532. [Google Scholar] [CrossRef] [PubMed]
- Tonnon, S.C.; van der Veen, R.; de Kruif, A.; Robroek, S.J.W.; van der Ploeg, H.P.; Proper, K.I.; van der Beek, A.J. Strategies of employees in the construction industry to increase their sustainable employability. Work 2018, 59, 249–258. [Google Scholar] [CrossRef]
- van Dam, K.; van Vuuren, T.; Kemps, S. Sustainable employment: The importance of intrinsically valuable work and an age-supportive climate. Int. J. Human Resour. Manag. 2017, 28, 2449–2472. [Google Scholar] [CrossRef]
- Effective Public Health Practice Project. Quality Assessment Tool for Quantitative Studies. Available online: https://merst.ca/wp-content/uploads/2018/02/quality-assessment-tool_2010.pdf (accessed on 2 July 2018).
- Deeks, J.; Dinnes, J.; D’Amico, R.; Sowden, A.; Sakarovitch, C. Evaluating non-randomised intervention studies. Health Technol. Assess. 2003, 7, 27. [Google Scholar] [CrossRef]
- Thomas, B.H.; Ciliska, D.; Dobbins, M.; Micucci, S. A Process for Systematically Reviewing the Literature: Providing the Research Evidence for Public Health Nursing Interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Oude Hengel, K.M.; Blatter, B.M.; Joling, C.I.; van der Beek, A.J.; Bongers, P.M. Effectiveness of an intervention at construction worksites on work engagement, social support, physical workload, and need for recovery: Results from a cluster randomized controlled trial. BMC Public Health 2012, 12, 1008. [Google Scholar] [CrossRef] [PubMed]
- Oude Hengel, K.M.; Blatter, B.M.; van der Molen, H.F.; Bongers, P.M.; van der Beek, A.J. The effectiveness of a construction worksite prevention program on work ability, health, and sick leave: Results from a cluster randomized controlled trial. Scand. J. Work Environ. Health 2013, 39, 456–467. [Google Scholar] [CrossRef] [PubMed]
- Koolhaas, W.; Groothoff, J.W.; de Boer, M.R.; van der Klink, J.J.; Brouwer, S. Effectiveness of a problem-solving based intervention to prolong the working life of ageing workers. BMC Public Health 2015, 15, 76. [Google Scholar] [CrossRef] [PubMed]
- van Holland, B.J.; Reneman, M.F.; Soer, R.; Brouwer, S.; de Boer, M.R. Effectiveness and Cost-benefit Evaluation of a Comprehensive Workers’ Health Surveillance Program for Sustainable Employability of Meat Processing Workers. J. Occup. Rehabil. 2018, 28, 107–120. [Google Scholar] [CrossRef] [PubMed]
- van der Meer, L.; Leijten, F.R.; Heuvel, S.G.; Ybema, J.F.; de Wind, A.; Burdorf, A.; Geuskens, G.A. Company Policies on Working Hours and Night Work in Relation to Older Workers’ Work Ability and Work Engagement: Results from a Dutch Longitudinal Study with 2 Year Follow-Up. J. Occup. Rehabil. 2016, 26, 173–181. [Google Scholar] [CrossRef]
- Van Scheppingen, A.R.; de Vroome, E.M.; Ten Have, K.C.; Bos, E.H.; Zwetsloot, G.I.; van Mechelen, W. Inducing a health-promoting change process within an organization: The effectiveness of a large-scale intervention on social capital, openness, and autonomous motivation toward health. J. Occup. Environ. Med. 2014, 56, 1128–1136. [Google Scholar] [CrossRef]
- Weiss, M.D. Leveraging Best Practices to Promote Health, Safety, Sustainability, and Stewardship. Workplace Health Saf. 2013, 61, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Koolhaas, W. Sustainable Employability of Ageing Workers—The Development of An Intervention. Ph.D. Thesis, University of Groningen, Groningen, The Netherlands, 2014. [Google Scholar]
- Montano, D.; Hoven, H.; Siegrist, J. Effects of organisational-level interventions at work on employees’ health: A systematic review. BMC Public Health 2014, 14, 135. [Google Scholar] [CrossRef]
- Nielsen, K.; Fredslund, H.; Christensen, K.B.; Albertsen, K. Success or failure? Interpreting and understanding the impact of interventions in four similar worksites. Work Stress 2006, 20, 272–287. [Google Scholar] [CrossRef]
- Oude Hengel, K.M.; Blatter, B.M.; van der Molen, H.F.; Joling, C.I.; Proper, K.I.; Bongers, P.M.; van der Beek, A.J. Meeting the Challenges of Implementing an Intervention to Promote Work Ability and Health-Related Quality of Life at Construction Worksites: A Process Evaluation. J. Occup. Environ. Med. 2011, 53, 1483–1491. [Google Scholar] [CrossRef] [PubMed]
- Van Holland, B.J.; Brouwer, S.; de Boer, M.R.; Reneman, M.F.; Soer, R. Process Evaluation of a Workers’ Health Surveillance Program for Meat Processing Workers. J. Occup. Rehabil. 2017, 27, 307–318. [Google Scholar] [CrossRef] [PubMed]
- Westgaard, R.H. RCTs of ergonomic interventions. Occup. Environ. Med. 2010, 67, 217–218. [Google Scholar] [CrossRef] [PubMed]
- Pruijt, H.; Derogee, P. Employability and Job Security, Friends or Foes? The Paradoxical Reception of Employacurity in the Netherlands. Socio-Econ. Rev. 2010, 8, 437–460. [Google Scholar] [CrossRef][Green Version]
- Olsen, O.; Albertsen, K.; Nielsen, M.L.; Poulsen, K.B.; Gron, S.M.F.; Brunnberg, H.L. Workplace restructurings in intervention studies—A challenge for design, analysis and interpretation. BMC Med. Res. Methodol. 2008, 8, 39. [Google Scholar] [CrossRef] [PubMed]
- Dellve, L.; Eriksson, A. Health-Promoting Managerial Work: A Theoretical Framework for a Leadership Program that Supports Knowledge and Capability to Craft Sustainable Work Practices in Daily Practice and During Organizational Change. Societies 2017, 7, 12. [Google Scholar] [CrossRef]
- Brouwer, S.; de Lange, A.; van der Mei, S.; Wessels, M.; Koolhaas, W.; Bültmann, U.; van der Heijden, B.; van der Klink, J.J.L. Duurzame Inzetbaarheid van de Oudere Werknemer: Stand van Zaken (Sustainable Employability of the Ageing Worker: The Situation); UMC: Groningen, The Netherlands, 2012. [Google Scholar]
- SER. Een Kwestie van Gezond Verstand: Breed Preventiebeleid Binnen Arbeidsorganisaties (Samenvatting) (A Matter of Common Sense: Broad Prevention Policy within Work Organisations); Sociaal Economische Raad (SER): Den Haag, The Netherlands, 2009. [Google Scholar]
- Van Vuuren, T. Vitaliteitsmanagement: Je hoeft niet ziek te zijn om beter te worden! (Vitality Management: You Do Not Need to Be Ill, to Get Better!); Inaugural Speech; Open Universiteit: Heerlen, The Netherlands, 2011. [Google Scholar]
- Van Vuuren, T. Vitaliteitsmanagement: Je hoeft niet ziek te zijn om beter te worden! (Vitality Management: You do not need to be ill, to get better!) Gedrag Organ. 2012, 25, 400–418. [Google Scholar]


{kind=link}
| SE Core Component | Intervention Content | Outcome Measures |
|---|---|---|
| Health | Intervention focuses on health aspects, such as well-being, quality of working life, vitality, lifestyle, or mental and physical health. | E.g., well-being, quality of working life, vitality, lifestyle, or mental and physical health. |
| Productivity | Intervention focuses on productivity aspects, such as work ability, productivity, or work engagement. | E.g., work ability, productivity, or work engagement. |
| Valuable work | Intervention focuses on valuable work aspects, such as perceived positive attitude, job motivation, having the right competences to perform the job, and development of skills and knowledge. | E.g., perceived positive attitude, job motivation, having the right competences to perform the job, and development of skills and knowledge. |
| Long-term perspective | Intervention focuses on all work ages. Intervention explicitly aimed at long-term effects. | Use of a follow-up period (at least 1 year) with repeated measures not only assessing short-term effects. |
| Study | Selection Bias (Baseline) | Study Design | Confounders b | Blinding | Data Collection | Withdrawals and Dropout | Data Analysis | Overall Quality c |
|---|---|---|---|---|---|---|---|---|
| Oude Hengel a [17] | Strong | Strong | Strong | Weak | Moderate | Moderate | Yes | Moderate |
| Oude Hengel a [18] | Strong | Strong | Strong | Weak | Strong | Moderate | Yes | Moderate |
| Koolhaas [19] | Moderate | Moderate | Strong | Weak | Strong | Moderate | Yes | Moderate |
| Van Holland [20] | Weak | Moderate | Strong | Weak | Strong | Weak | Yes | Weak |
| Van der Meer [21] | Weak | Moderate | Strong | Moderate | Moderate | Weak | Yes | Weak |
| Van Scheppingen [22] | Weak | Moderate | Strong | Weak | Strong | Weak | Yes | Weak |
| Weiss [23] | Weak | Moderate | Weak | Weak | Weak | Weak | No | Weak |
| Study | Study Population | Follow-Up | Intervention Content | SE Core Components in Content | Outcome Measures | SE Core Components in Outcome Measures | Effectiveness b |
|---|---|---|---|---|---|---|---|
| Oude Hengel a [17] Moderate overall quality | Construction workers (N = 293) Mean age = 41.8 years intervention group and 44.2 years control group Education level: Intervention group: Low (74%); Medium-high (26%). Control group: Low (84%); Medium-high (15%). | 3,6,12 months |
| Health | Physical workload | Health | Negative effect (in intervention group 6 months of follow-up |
| Need for recovery | Health | No effect | |||||
| Work engagement | Productivity | No effect | |||||
| Social support at work | Valuable work | No effect | |||||
| Health Long-term perspective | ||||||
| Valuable work | ||||||
| Oude Hengel a [18] Moderate overall quality | Construction workers (N = 293) Mean age = 41.8 years intervention group and 44.2 years control group Education level: Intervention group: Low (74%); Medium-high (26%). Control group: Low (84%); Medium-high (15%). | 3,6,12 months |
| Health | Sick leave | Health | No effect |
| Musculoskeletal symptoms | Health | No effect | |||||
| Health Long-term perspective | Mental and physical health status | Health | No effect | |||
| Work ability | Productivity | No effect | |||||
| Valuable work | ||||||
| Koolhaas [19] Moderate overall quality | Aging workers (Age >45 years) (N = 125) Education level: Low (17%) Medium (40%) High (43%) | 1 year |
| Health Valuable work | Perceived fatigue | Health | No effect |
| Vitality | Health | Negative effect | |||||
| Valuable work | Work ability | Productivity | Negative effect | |||
| Productivity | Productivity | No effect | |||||
| Work engagement | Productivity | No effect | |||||
| Long term perspective | Job content (skills discretion) | Valuable work | Positive effect | |||
| Perceived work attitude | Valuable work | Positive effect | |||||
| Self-efficacy | Valuable work | Positive effect | |||||
| Van Holland [20] Weak overall quality | Workers of Dutch meat processing company (N = 305) mean age = 50.6 years Education level: No-low (64%); Medium-high (32%) | 3 years |
| Health Productivity | Sickness absence | Health | Negative effect |
| Health | Health | No effect | |||||
| Vitality | Health | No effect | |||||
| Valuable work | Work ability | Productivity | Negative effect | |||
| Productivity | Productivity | Negative effect | |||||
| Psychosocial variable: meaning of work | Valuable work | Positive effect | |||||
| Van der Meer [21] Weak overall quality | Workers, including self-employed and people without paid job (45–64 years) (N = 6922) Mean age = 53.7 years | 2 years | Create awareness and knowledge of aging employees on the availability and the use of two company policies to support:
| Health Valuable work Productivity | Work engagement | Productivity | Positive effect (by starting to use the policy ‘exemption from evening/night work’) |
| Work ability | Productivity | Negative effect: (by starting to use the policy ‘reduced working hours’) | |||||
| Van Scheppingen [22] Weak overall quality | Workers in Dutch dairy company (N = 324) Age: <30 = 14.8% 30–45 = 37.3% >45 = 47.8% Educational level: Primary = 22.2% Secondary = 42.0% Higher = 35.8% | 18 months |
| Health Valuable work | An improvement of employees’ lifestyle:
| Health | Positive effect (smoking and healthy eating; component 1) |
| Health | Positive effect (healthy eating; component 2) | |||||
| Health | Health and vitality at work:
| Health Long-term perspective | Positive effect (sustainable employability; component 1) | |||
| Autonomous motivation toward a healthy lifestyle | Valuable work | Positive effect (component 3) | |||||
| Bonding social capital | Valuable work | Positive effect (component 1) | |||||
| Openness toward health and vitality at work | Valuable work | Positive effect (component 1) | |||||
| Positive effect (component 3) | |||||||
| Weiss [23] Weak overall quality | Several companies with 100 or more employees No further information on demographics | 4 years |
| Health Valuable work Health Valuable work | Six core components: Consistency Stability Confidence Trust (self-efficacy) Dedication Attachment | Valuable work Long-term perspective | No effect: high level of self-efficacy No effect: High levels of attachment |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hazelzet, E.; Picco, E.; Houkes, I.; Bosma, H.; de Rijk, A. Effectiveness of Interventions to Promote Sustainable Employability: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 1985. https://doi.org/10.3390/ijerph16111985
Hazelzet E, Picco E, Houkes I, Bosma H, de Rijk A. Effectiveness of Interventions to Promote Sustainable Employability: A Systematic Review. International Journal of Environmental Research and Public Health. 2019; 16(11):1985. https://doi.org/10.3390/ijerph16111985
Chicago/Turabian StyleHazelzet, Emmelie, Eleonora Picco, Inge Houkes, Hans Bosma, and Angelique de Rijk. 2019. "Effectiveness of Interventions to Promote Sustainable Employability: A Systematic Review" International Journal of Environmental Research and Public Health 16, no. 11: 1985. https://doi.org/10.3390/ijerph16111985
APA StyleHazelzet, E., Picco, E., Houkes, I., Bosma, H., & de Rijk, A. (2019). Effectiveness of Interventions to Promote Sustainable Employability: A Systematic Review. International Journal of Environmental Research and Public Health, 16(11), 1985. https://doi.org/10.3390/ijerph16111985