Occupational Infection Risk with Multidrug-Resistant Organisms in Health Personnel—A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
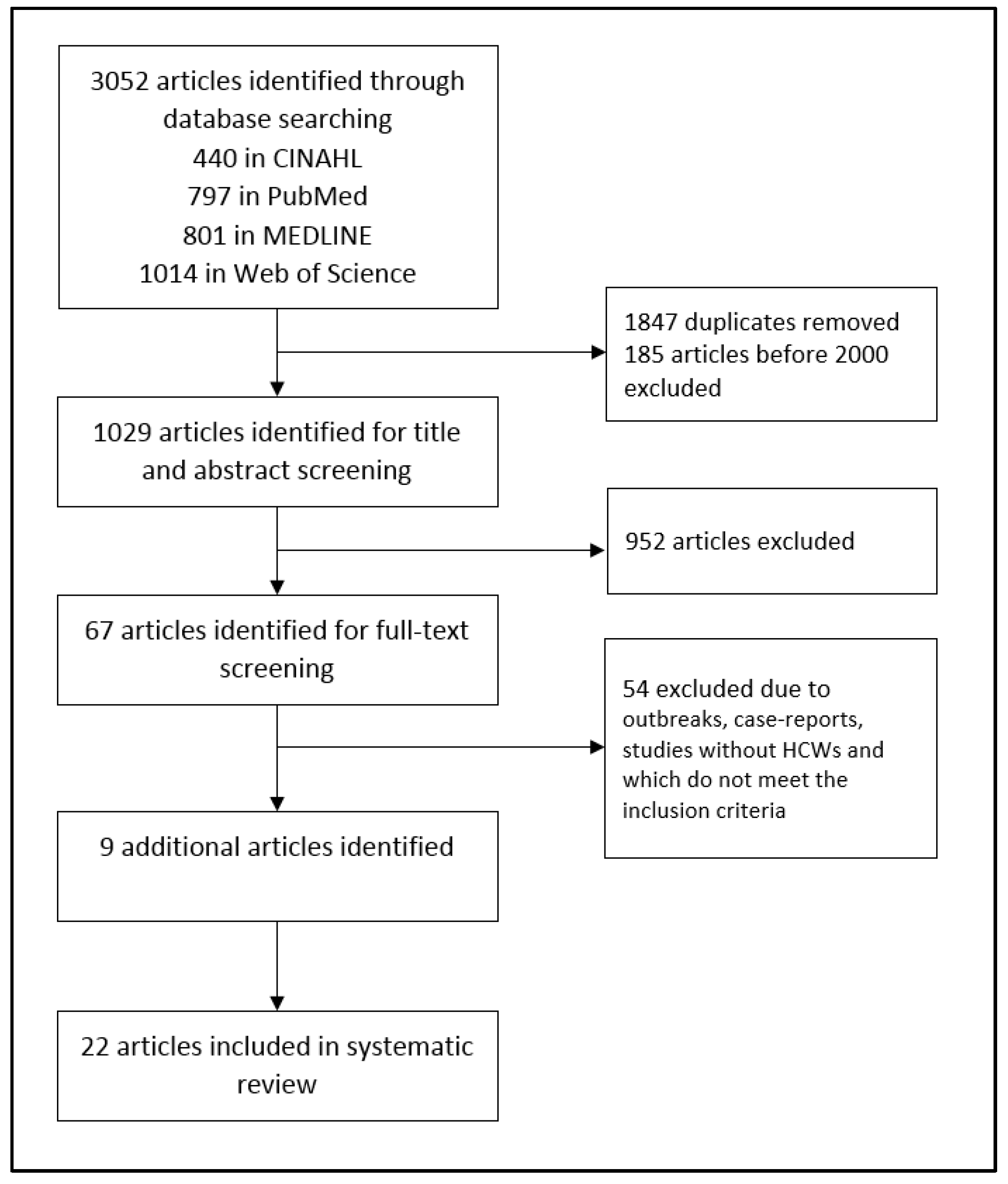
2.2. Database Search
2.3. Study Selection
3. Results
3.1. MDROs
3.2. Study Description
3.2.1. Health Personnel in Hospital Settings
3.2.2. Health Personnel in Geriatric Care Setting
4. Discussion
4.1. MDROs
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Oberdörfer, H.; Hübner, C.; Linder, R.; Fleßa, S. Additional Costs for Care of Patients with Multi-Resistant Pathogens–An Analysis from the Perspective of a Statutory Health Insurance. Gesundheitswesen 2015, 77, 854–860. [Google Scholar] [PubMed]
- Koch, A.M.; Eriksen, H.M.; Elstrom, P.; Aavitsland, P.; Harthug, S. Severe consequences of healthcare-associated infections among residents of nursing homes: A cohort study. J. Hosp. Infect. 2009, 71, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Linder, R.; Thoms, I.; Pfenning, I.; Schadowski, R.; Mows, V. The project HICARE: Cross-sectoral action alliance against multi-resistant pathogens. GMS Krankenhhyg. Interdiszip. 2011, 6, 25. [Google Scholar]
- Noll, I.; Eckmanns, T. Antibiotikaresistenz: Vergleich mit europäischen Daten. Dtsch. Arztebl. 2017, 114, A2209–A2210. [Google Scholar]
- European Centre for Disease Prevention and Control. Surveillance of Antimicrobial Resistance in Europe—Annual Report of the European Antimicrobial Resistance Surveillance Network (EARS-Net) 2017; ECDC: Stockholm, Sweden, 2018. [Google Scholar]
- Remschmidt, C.; Schroder, C.; Behnke, M.; Gastmeier, P.; Geffers, C.; Kramer, T.S. Continuous increase of vancomycin resistance in enterococci causing nosocomial infections in Germany-10 years of surveillance. Antimicrob. Resist. Infect. Control 2018, 7, 54. [Google Scholar] [CrossRef] [PubMed]
- Köck, R.; Werner, P.; Friedrich, A.W.; Fegeler, C.; Becker, K. Persistence of nasal colonization with human pathogenic bacteria and associated antimicrobial resistance in the German general population. New Microbes New Infect. 2016, 9, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Dulon, M.; Haamann, F.; Peters, C.; Schablon, A.; Nienhaus, A. MRSA prevalence in European healthcare settings: A review. BMC Infect. Dis. 2011, 11, 138. [Google Scholar] [CrossRef]
- Albrich, W.C.; Harbarth, S. Health-care workers: Source, vector, or victim of MRSA? Lancet Infect. Dis. 2008, 8, 289–301. [Google Scholar] [CrossRef]
- Hawkins, G.; Stewart, S.; Blatchford, O.; Reilly, J. Should healthcare workers be screened routinely for meticillin-resistant Staphylococcus aureus? A review of the evidence. J. Hosp. Infect. 2011, 77, 285–289. [Google Scholar] [CrossRef]
- Dulon, M.; Peters, C.; Schablon, A.; Nienhaus, A. MRSA carriage among healthcare workers in non-outbreak settings in Europe and the United States: A systematic review. BMC Infect. Dis. 2014, 14, 363. [Google Scholar] [CrossRef]
- Empfehlung der Kommission für Krankenhaushygiene und Infektionsprävention (KRINKO) beim Robert Koch-Institut. Empfehlungen zur Prävention und Kontrolle von Methicillin-resistenten Staphylococcus aureus-Stämmen (MRSA) in medizinischen und pflegerischen Einrichtungen. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2014, 57, 695–732. [Google Scholar] [CrossRef]
- Gruber, I.; Heudorf, U.; Werner, G.; Pfeifer, Y.; Imirzalioglu, C.; Ackermann, H.; Brandt, C.; Besier, S.; Wichelhaus, T.A. Multidrug-resistant bacteria in geriatric clinics, nursing homes, and ambulant care-prevalence and risk factors. Int. J. Med. Microbiol. 2013, 303, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Peters, C.; Dulon, M.; Kleinmüller, O.; Nienhaus, A.; Schablon, A. MRSA Prevalence and Risk Factors among Health Personnel and Residents in Nursing Homes in Hamburg, Germany-A Cross-Sectional Study. PLoS ONE 2017, 12, e0169425. [Google Scholar] [CrossRef]
- Peters, C.; Kleinmüller, O.; Nienhaus, A.; Schablon, A. Prevalence and risk factors of MRSA colonisations: A cross-sectional study among personnel in outpatient care settings in Hamburg, Germany. BMJ Open 2018, 8, e021204. [Google Scholar] [CrossRef] [PubMed]
- Schablon, A.; Kleinmüller, O.; Nienhaus, A.; Peters, C. MRSA prevalence among patient transport staff in Hamburg. GMS Hyg. Infect. Control 2018, 13, Doc3. [Google Scholar]
- Heudorf, U.; Bremer, V.; Heuck, D. Methicillin-resistant Staphylococcus aureus in Long-Term Care Facilities for the Aged in Frankfurt am Main, Germany, in 1999. Gesundheitswesen 2001, 63, 447–454. [Google Scholar] [CrossRef]
- Ebrahimi, F.; Mozes, J.; Monostori, J.; Goracz, O.; Fesus, A.; Majoros, L.; Szarka, K.; Kardos, G. Comparison of rates of fecal colonization with extended-spectrum beta-lactamase-producing enterobacteria among patients in different wards, outpatients and medical students. Microbiol. Immunol. 2016, 60, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Maechler, F.; Geffers, C.; Schwab, F.; Peña Diaz, L.A.; Behnke, M.; Gastmeier, P. Entwicklung der Resistenzsituation in Deutschland. Med. Klin. Intensivmed. Notfmed. 2017, 112, 186–191. [Google Scholar] [CrossRef]
- Hogardt, M.; Proba, P.; Mischler, D.; Cuny, C.; Kempf, V.A.; Heudorf, U. Current prevalence of multidrug-resistant organisms in long-term care facilities in the Rhine-Main district, Germany, 2013. Euro Surveill. 2015, 20, 21171. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, N.; Gastmeier, P.; Vonberg, R.P. Effectiveness of healthcare worker screening in hospital outbreaks with gram-negative pathogens: A systematic review. Antimicrob. Resist. Infect. Control 2018, 7, 36. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Khan, K.S.; Kunz, R.; Kleijnen, J.; Antes, G. Systematic Reviews to Support Evidence-Based Medicine: How to Review and Apply Findings of Healthcare Research; Royal Society of Medicine Press: London, UK, 2003. [Google Scholar]
- Schubert, M.; Kampf, D.; Jatzwauk, L.; Kynast, F.; Stein, A.; Strasser, R.; Dulon, M.; Nienhaus, A.; Seidler, A. Prevalence and predictors of MRSA carriage among employees in a non-outbreak setting: A cross-sectional study in an acute care hospital. J. Occup. Med. Toxicol. 2019, 14, 7. [Google Scholar] [CrossRef] [PubMed]
- The Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews. Checklist for Prevalence Studies. Available online: http://joannabriggs.org/research/critical-appraisal-tools.html (accessed on 30 April 2019).
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Decker, B.K.; Lau, A.F.; Dekker, J.P.; Spalding, C.D.; Sinaii, N.; Conlan, S.; Henderson, D.K.; Segre, J.A.; Frank, K.M.; Palmore, T.N. Healthcare personnel intestinal colonization with multidrug-resistant organisms. Clin. Microbiol. Infect. 2018, 24, 82.e1–82.e4. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Fei, C.N.; Zhang, Y.; Liu, G.W.; Liu, J.; Dong, J. Presence, distribution and molecular epidemiology of multi-drug-resistant Gram-negative bacilli from medical personnel of intensive care units in Tianjin, China, 2007–2015. J. Hosp. Infect. 2017, 96, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Aschbacher, R.; Pagani, E.; Confalonieri, M.; Farina, C.; Fazii, P.; Luzzaro, F.; Montanera, P.G.; Piazza, A.; Pagani, L. Review on colonization of residents and staff in Italian long-term care facilities by multidrug-resistant bacteria compared with other European countries. Antimicrob. Resist. Infect. Control 2016, 5, 33. [Google Scholar] [CrossRef] [PubMed][Green Version]
- March, A.; Aschbacher, R.; Dhanji, H.; Livermore, D.M.; Bottcher, A.; Sleghel, F.; Maggi, S.; Noale, M.; Larcher, C.; Woodford, N. Colonization of residents and staff of a long-term-care facility and adjacent acute-care hospital geriatric unit by multiresistant bacteria. Clin. Microbiol. Infect. 2010, 16, 934–944. [Google Scholar] [CrossRef] [PubMed]
- Bassyouni, R.H.; Gaber, S.N.; Wegdan, A.A. Fecal carriage of extended-spectrum beta-lactamase- and AmpC- producing Escherichia coli among healthcare workers. J. Infect. Dev. Ctries. 2015, 9, 304–308. [Google Scholar] [CrossRef]
- Liou, M.L.; Chen, K.H.; Yeh, H.L.; Lai, C.Y.; Chen, C.H. Persistent nasal carriers of Acinetobacter baumannii in long-term-care facilities. Am. J. Infect. Control 2017, 45, 723–727. [Google Scholar] [CrossRef]
- Bayuga, S.; Zeana, C.; Sahni, J.; Della-Latta, P.; el-Sadr, W.; Larson, E. Prevalence and antimicrobial patterns of Acinetobacter baumannii on hands and nares of hospital personnel and patients: The iceberg phenomenon again. Heart Lung 2002, 31, 382–390. [Google Scholar] [CrossRef]
- Baran, J., Jr.; Ramanathan, J.; Riederer, K.M.; Khatib, R. Stool colonization with vancomycin-resistant enterococci in healthcare workers and their households. Infect. Control Hosp. Epidemiol. 2002, 23, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Jozsa, K.; de With, K.; Kern, W.; Reinheimer, C.; Kempf, V.A.J.; Wichelhaus, C.; Wichelhaus, T.A. Intestinal carriage of multidrug-resistant bacteria among healthcare professionals in Germany. GMS Infect. Dis. 2017, 5, Doc07. [Google Scholar] [PubMed]
- Leao-Vasconcelos, L.; Lima, A.B.M.; Costa, D.D.; Rocha-Vilefort, L.O.; de Oliveira, A.C.A.; Goncalves, N.F.; Vieira, J.D.G.; Prado-Palos, M.A. Enterobacteriaceae isolates from the oral cavity of workers in a Brazilian oncology hospital. Rev. Inst. Med. Trop. Sao Paulo 2015, 57, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Ake, J.; Scott, P.; Wortmann, G.; Huang, X.Z.; Barber, M.; Wang, Z.N.; Nikolich, M.; Van Echo, D.; Weintrob, A.; Lesho, E. Gram-Negative Multidrug-Resistant Organism Colonization in a US Military Healthcare Facility in Iraq. Infect. Control Hosp. Epidemiol. 2011, 32, 545–552. [Google Scholar] [CrossRef]
- Adler, A.; Baraniak, A.; Izdebski, R.; Fiett, J.; Salvia, A.; Samso, J.V.; Lawrence, C.; Solomon, J.; Paul, M.; Lerman, Y.; et al. A multinational study of colonization with extended spectrum beta-lactamase-producing Enterobacteriaceae in healthcare personnel and family members of carrier patients hospitalized in rehabilitation centres. Clin. Microbiol. Infect. 2014, 20, O516–O523. [Google Scholar] [CrossRef]
- Angelin, M.; Forsell, J.; Granlund, M.; Evengard, B.; Palmgren, H.; Johansson, A. Risk factors for colonization with extended-spectrum beta-lactamase producing Enterobacteriaceae in healthcare students on clinical assignment abroad: A prospective study. Travel Med. Infect. Dis. 2015, 13, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Moraes, R.B.; Della Giustina, A.; Farenzena, E.M.V.; Milman, L.D.; Fedrizzi, R.S. Microbiologic profile of hospitalized healthcare workers. Rev. Assoc. Med. Bras. 2014, 60, 473–478. [Google Scholar] [CrossRef]
- Kocak Tufan, Z.; Arslan, S.; Cesur, S.; Bulut, C.; Irmak, H.; Kinikli, S.; Ergin, F.; Celik, A.K.; Demiroz, A.P. Absence of vancomycin-resistant enterococci (VRE) despite the presence of risk factors: A survey of rectal carriage of VRE. Turk. J. Med. Sci. 2010, 40, 623–628. [Google Scholar]
- Andriatahina, T.; Randrianirina, F.; Hariniana, E.R.; Talarmin, A.; Raobijaona, H.; Buisson, Y.; Richard, V. High prevalence of fecal carriage of extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae in a pediatric unit in Madagascar. BMC Infect. Dis. 2010, 10, 204. [Google Scholar] [CrossRef]
- Agostinho, A.; Renzi, G.; Haustein, T.; Jourdan, G.; Bonfillon, C.; Rougemont, M.; Hoffmeyer, P.; Harbarth, S.; Uckay, I. Epidemiology and acquisition of extended-spectrum beta-lactamase-producing Enterobacteriaceae in a septic orthopedic ward. Springerplus 2013, 2, 91. [Google Scholar] [CrossRef]
- Bitterman, R.; Geffen, Y.; Rabino, G.; Eluk, O.; Warman, S.; Greenblatt, A.S.; Neuberger, A.; Reisner, S.A.; Hussein, K.; Paul, M. Rate of colonization of health care workers by carbapenem-resistant Enterobacteriaceae in an endemic hospital: A prospective study. Am. J. Infect. Control 2016, 44, 1053–1054. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Fei, C.N.; Liu, J.; Ji, X.Y.; Song, J. Investigation on the status of multidrug-resistant gram-negative bacteria induced by occupational exposure among medical staff in ICU. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi/Chin. J. Ind. Hyg. Occup. Dis. 2018, 36, 734–737. [Google Scholar]
- March, A.; Aschbacher, R.; Pagani, E.; Sleghel, F.; Soelva, G.; Hopkins, K.L.; Doumith, M.; Innocenti, P.; Burth, J.; Piazzani, F.; et al. Changes in colonization of residents and staff of a long-term care facility and an adjacent acute-care hospital geriatric unit by multidrug-resistant bacteria over a four-year period. Scand. J. Infect. Dis. 2014, 46, 114–122. [Google Scholar] [CrossRef] [PubMed]
- March, A.; Aschbacher, R.; Sleghel, F.; Soelva, G.; Kaczor, M.; Migliavacca, R.; Piazza, A.; Mattioni Marchetti, V.; Pagani, L.; Scalzo, K.; et al. Colonization of residents and staff of an Italian long-term care facility and an adjacent acute care hospital geriatric unit by multidrug-resistant bacteria. New Microbiol. 2017, 40, 258–263. [Google Scholar] [PubMed]
- Valenza, G.; Nickel, S.; Pfeifer, Y.; Eller, C.; Krupa, E.; Lehner-Reindl, V.; Höller, C. Extended-Spectrum-ß-Lactamase-Producing Escherichia coli as Intestinal Colonizers in the German Community. Antimicrob. Agents Chemother. 2014, 58, 1228–1230. [Google Scholar] [CrossRef]
- Meyer, E.; Gastmeier, P.; Kola, A.; Schwab, F. Pet animals and foreign travel are risk factors for colonisation with extended-spectrum beta-lactamase-producing Escherichia coli. Infection 2012, 40, 685–687. [Google Scholar] [CrossRef] [PubMed]
- Woerther, P.L.; Andremont, A.; Kantele, A. Travel-acquired ESBL-producing Enterobacteriaceae: Impact of colonization at individual and community level. J. Travel Med. 2017, 24, S29–S34. [Google Scholar] [CrossRef]
- Karanika, S.; Karantanos, T.; Arvanitis, M.; Grigoras, C.; Mylonakis, E. Fecal Colonization With Extended-spectrum Beta-lactamase-Producing Enterobacteriaceae and Risk Factors Among Healthy Individuals: A Systematic Review and Metaanalysis. Clin. Infect. Dis. 2016, 63, 310–318. [Google Scholar] [CrossRef]
- Royden, A.; Ormandy, E.; Pinchbeck, G.; Pascoe, B.; Hitchings, M.D.; Sheppard, S.K.; Williams, N.J. Prevalence of faecal carriage of extended-spectrum beta-lactamase (ESBL)-producing Escherichia coli in veterinary hospital staff and students. Vet. Rec. Open 2019, 6, e000307. [Google Scholar] [CrossRef]
- Jackson, S.S.; Harris, A.D.; Magder, L.S.; Stafford, K.A.; Johnson, J.K.; Miller, L.G.; Calfee, D.P.; Thom, K.A. Bacterial burden is associated with increased transmission to health care workers from patients colonized with vancomycin-resistant Enterococcus. Am. J. Infect. Control 2019, 47, 13–17. [Google Scholar] [CrossRef]
- Montoya, A.; Schildhouse, R.; Goyal, A.; Mann, J.D.; Snyder, A.; Chopra, V.; Mody, L. How often are health care personnel hands colonized with multidrug- resistant organisms? A systematic review and meta-analysis. Am. J. Infect. Control 2018, 10. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Country | Study Design | Study Period | Setting | Sample Type | Sample Size | MDRO Prevalence | Quality Assessment | |
|---|---|---|---|---|---|---|---|---|
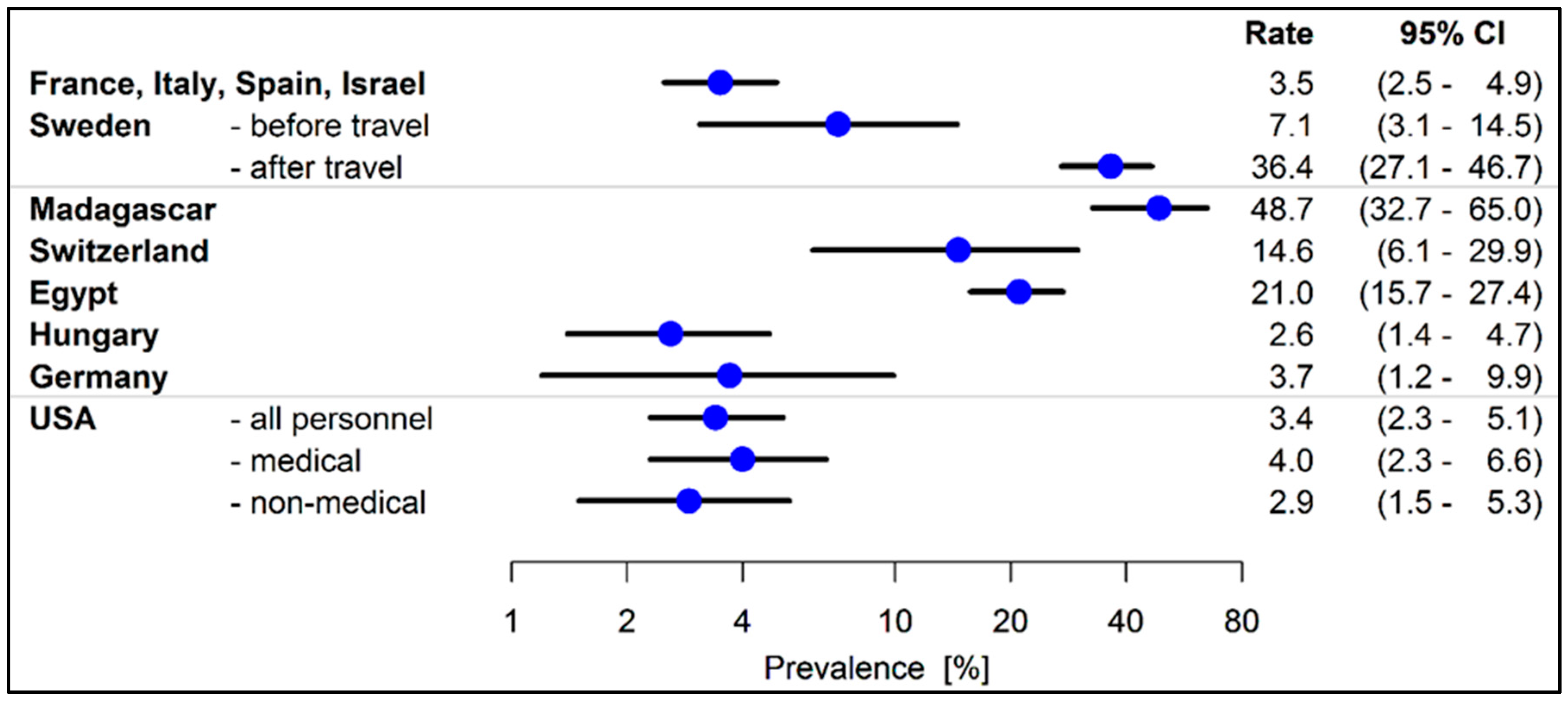
| Adler 2014 [38] | France (F), Italy (I), Spain (E), Israel (IL) | prospective | 2008–11 | rehabilitation units | rectal | 1001 F 147 I 439 E 47 IL 368 | ESBL 35 (3.5%) 3 (2.0%) 12 (2.7%) 5 (10.6%) 15 (4.1%) | ++ |
| Angelin 2015 [39] | Sweden | prospective | 2010–14 | abroad clinical assignment | faecal | 99 | ESBL before 7 (7.1%) ESBL after 36 (36.4%) CPO 0% | ++ |
| Moraes 2014 [40] | Brazil | retrospective | 2005–12 | hospital | different samples | 105 | MDRO 0% | ++ |
| Baran 2002 [34] | USA | cross-sectional | 1998 | hospital | stool | 52 MP 40 NMP | VRE 5 (9.6%) MP VRE 0% NMP | ++ |
| Bayuga 2002 [33] | USA | cross-sectional | 2000–01 | hospital | nasal, hand | 184 | Acinetobacte baumannii 1 (0.5%) | ++ |
| Kocak Tufan 2010 [41] | Turkey | cross-sectional | 2005 | hospital | stool | 221 | VRE 0% | ++ |
| Andriatahina 2010 [42] | Madagascar | (cohort study) cross-sectional | 2008 | hospital | rectal | 39 | ESBL 19 (48.7%) | + |
| Agostinho 2013 [43] | Switzerland | cross-sectional | 2010–11 | hospital | anal | 41 | ESBL 6 (14.6%) | + |
| Bassyouni 2015 [31] | Egypt | cross-sectional | 2013 | hospital | stool | 200 | ESBL 42 (21.0%) AmpC 6 (3.0%) | + |
| Leao-Vasconelos 2015 [36] | Brazil | cross-sectional | 2009–10 | hospital | saliva | 294 | MDRO 27 (9.2%) | + |
| Ebrahimi 2016 [18] | Hungary | cross-sectional | 2010–13 | hospital | faecal | 424 | ESBL 11 (2.6%) | + |
| Bitterman 2016 [44] | Israel | cross-sectional | 2015 | hospital | rectal | 177 | CPO 0% | ++ |
| Jozsa 2017 [35] | Germany | cross-sectional | 2013–14 | unspecified | rectal | 107 | ESBL 4 (3.7%) MRSA 0% VRE 0% | + |
| Liu 2017 [28] | China | cross-sectional | 2007–15 | hospital | nasal, hand | 1185 MP 133 NMP | MDR-GNB 104 (8.8) MP MDR-GNB 20 (15.0) NMP MRSA 11 (0.9%) MP VRE 1 (0.1%) MP | +++ |
| Decker 2017 [27] | USA | cross-sectional | 2013–15 | hospital | perirectal | 379 MP 376 NMP | VRE 0% MP+ staff ESBL 15 (4.0%) MP ESBL 11 (2.9%) NMP CPO 0% MP CPO 1 (0.3%) NMP | +++ |
| Ake 2011 [37] | USA/Iraq | surveillance | 2007 | hospital | groin, axillar | 80 | MDRO 3 (3.8%) | ++ |
| Country | Study Design | Study Period | Setting | Sample Type | Sample Size | MDRO Prevalence | Quality Assessment | |
|---|---|---|---|---|---|---|---|---|
| Aschbacher 2016 [29] | Italy | review | 2000–16 | LTCF | nasal, rectal, inguinal, oro-pharyngeal, urine | MRSA 5.8–14.5% ESBL 5.2–7.0% CPO 0–1.5% VRE 0% | not applicable | |
| March 2010 [30] | Italy | cross-sectional | 2008 | LTCF, geriatric unit | nasal, rectal, inguinal, oropharyngeal, urine | 69 | MRSA 10 (14.5%) ESBL 10 (14.5%) VRE 0% MBL 1 (1.5%) AmpC 1 (1.5%) | + |
| March 2014 [46] | Italy | cross-sectional | 2012 | LTCF, geriatric unit | nasal, rectal, inguinal, oropharyngeal, urine | 57 | MRSA 4 (7.0%) ESBL 3 (5.3%) MBL 0% | + |
| March 2017 [47] | Italy | cross-sectional | 2016 | LTCF, geriatric unit | nasal, rectal, inguinal, oropharyngeal, urine | 67 | MRSA 5 (7.4%) ESBL 8 (11.9%) VRE 0% MBL 0% | + |
| Gruber 2013 [13] | Germany | cross-sectional | 2006–07 | nursing homes, geriatric clinics | nasal, throat, rectal | 64 | MRSA 2 (3.1%) ESBL 2 (3.1%) VRE 1 (1.6%) | ++ |
| Liou 2017 [32] | Taiwan | (prospective) cross-sectional | 2014–16 | LTFCs, hospital | nasal | 13 | A. baumannii 0% | + |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peters, C.; Dulon, M.; Nienhaus, A.; Schablon, A. Occupational Infection Risk with Multidrug-Resistant Organisms in Health Personnel—A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 1983. https://doi.org/10.3390/ijerph16111983
Peters C, Dulon M, Nienhaus A, Schablon A. Occupational Infection Risk with Multidrug-Resistant Organisms in Health Personnel—A Systematic Review. International Journal of Environmental Research and Public Health. 2019; 16(11):1983. https://doi.org/10.3390/ijerph16111983
Chicago/Turabian StylePeters, Claudia, Madeleine Dulon, Albert Nienhaus, and Anja Schablon. 2019. "Occupational Infection Risk with Multidrug-Resistant Organisms in Health Personnel—A Systematic Review" International Journal of Environmental Research and Public Health 16, no. 11: 1983. https://doi.org/10.3390/ijerph16111983
APA StylePeters, C., Dulon, M., Nienhaus, A., & Schablon, A. (2019). Occupational Infection Risk with Multidrug-Resistant Organisms in Health Personnel—A Systematic Review. International Journal of Environmental Research and Public Health, 16(11), 1983. https://doi.org/10.3390/ijerph16111983