Media Health Literacy, eHealth Literacy, and the Role of the Social Environment in Context

{kind=link}
Abstract
1. Introduction
2. The Concepts of Media Health Literacy and eHealth Literacy
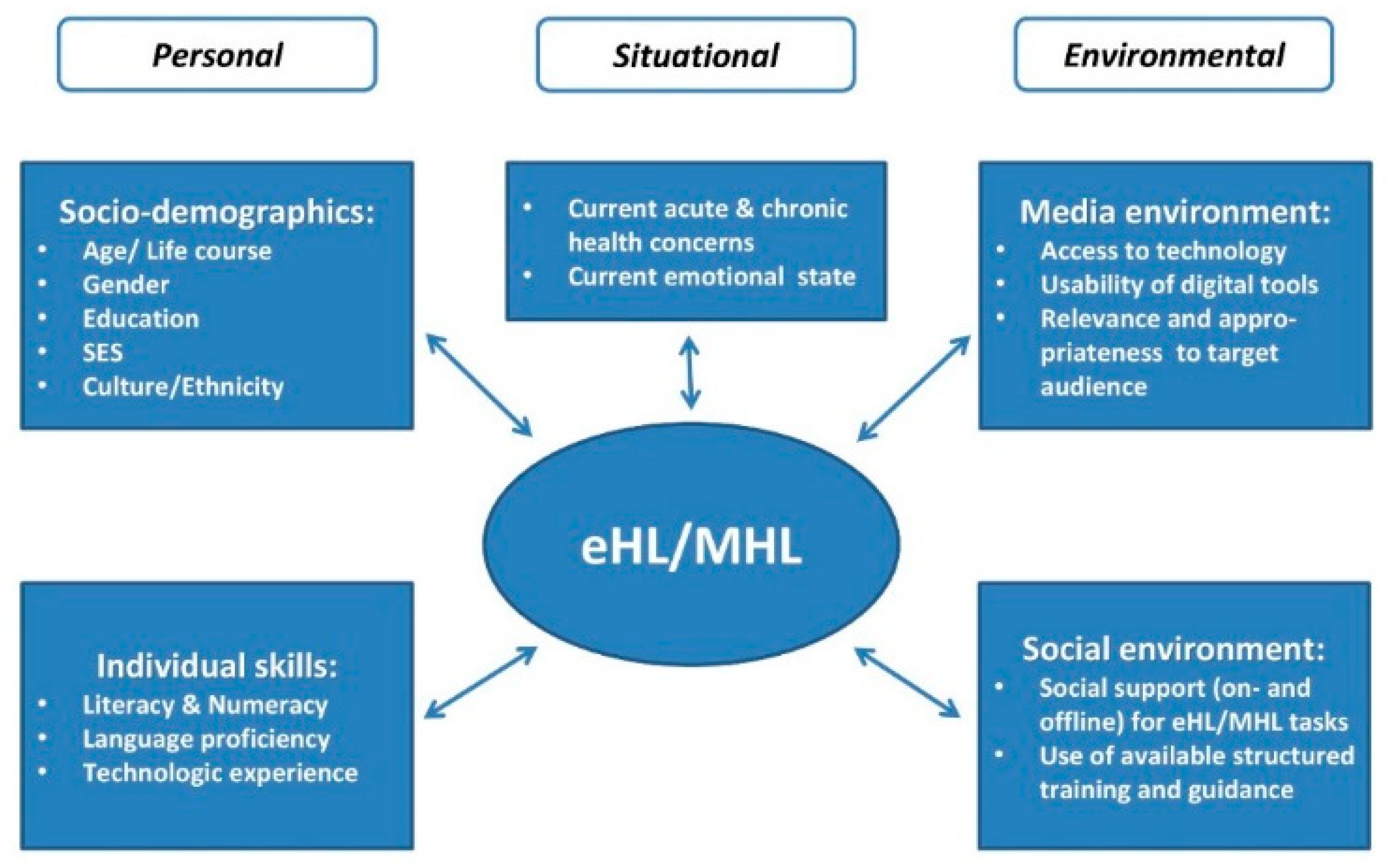
3. Media Health Literacy and eHealth Literacy in Context
3.1. Complexity of Systems and Environments
3.2. The Role of Socio-Demographics
3.3. Social Networks
4. Improving Media Health Literacy and eHealth Literacy
5. Ethical Considerations in Media and eHealth Literacy Practice, Research, and Policy
5.1. Media and eHealth Literacy Ethics in Research
5.2. Media and eHealth Literacy Ethics in Practice and Policy
6. Discussion
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H.; HLS-EU Consortium. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12. [Google Scholar] [CrossRef]
- Kickbusch, I.S. Health literacy: Addressing the health and education divide. Health Promot. Int. 2001, 16, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Levin-Zamir, D.; Lemish, D.; Gofin, R. Media Health Literacy (MHL): Development and measurement of the concept among adolescents. Health Educ. Res. 2011, 26, 323–335. [Google Scholar] [CrossRef] [PubMed]
- Norman, C.D.; Skinner, H.A. eHealth Literacy: Essential skills for consumer health in a networked world. J. Med. Internet Res. 2006, 8, e9. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, S. Developing social media literacy: How children learn to interpret risky opportunities on social network sites. Communications 2014, 39, 283–303. [Google Scholar] [CrossRef]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef]
- McGinnis, J.M.; Berwick, D.M.; Daschle, T.A.; Diaz, A.; Fineberg, H.V.; First, W.H.; Gawande, A.; Halfon, N.; Mourey, R. Systems strategies for better health throughout the life course. In Vital Directions for Health & Health Care; Dzau, V.J., McClellan, M.B., McGinnis, J.M., Finkelman, E.M., Eds.; National Academy of Medicine: Washington, DC, USA, 2017; pp. 43–69. ISBN 978-1-947-10300-9. [Google Scholar]
- Research2Guidance. mHealth App Economics 2017/2018. Current Status and Future Trends in Mobile Health; Research2Guidance: Berlin, Germany, 2017. [Google Scholar]
- Norman, C.D.; Skinner, H.A. eHEALS: The eHealth Literacy Scale. J. Med. Internet Res. 2006, 8, e27. [Google Scholar] [CrossRef] [PubMed]
- Quinn, S.; Bond, R.; Nugent, C. Quantifying health literacy and eHealth literacy using existing instruments and browser-based software for tracking online health information seeking behavior. Comput. Hum. Behav. 2017, 69, 256–267. [Google Scholar] [CrossRef]
- Van der Vaart, R.; van Deursen, A.J.; Drossaert, C.H.; Taal, E.; van Dijk, J.A.; van de Laar, M.A. Does the eHealth Literacy Scale (eHEALS) measure what it intends to measure? Validation of a Dutch version of the eHEALS in two adult populations. J. Med. Internet Res. 2011, 13, e86. [Google Scholar] [CrossRef] [PubMed]
- Norman, C.D. eHealth literacy 2.0: Problems and opportunities with an evolving concept. J. Med. Internet Res. 2011, 13, e125. [Google Scholar] [CrossRef] [PubMed]
- Van der Vaart, R.; Drossaert, C.H. Development of the digital health literacy instrument: Measuring a broad spectrum of health 1.0 and health 2.0 skills. J. Med. Internet Res. 2017, 19, e27. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.V.; Kaufman, D.R. A framework for characterizing eHealth literacy demands and barriers. J. Med. Internet Res. 2011, 13, e94. [Google Scholar] [CrossRef] [PubMed]
- Parker, R. Measuring health literacy: What? So what? Now what? In Measures of Health Literacy: Workshop Summary; Hernandez, L.M., Ed.; National Academies Press: Washington, DC, USA, 2009; ISBN 978-0-309-13980-9. [Google Scholar]
- Zanchetta, M.S.; Poureslami, I.M. Health literacy within the reality of immigrants’ culture and language. Can. J. Public Health 2006, 97 (Suppl. 2), S26–S30. [Google Scholar] [PubMed]
- Bodie, G.D.; Dutta, M.J. Understanding health literacy for strategic health marketing: eHealth literacy, health disparities, and the digital divide. Health Mark. Q. 2008, 25, 175–203. [Google Scholar] [CrossRef] [PubMed]
- Meppelink, C.S.; van Weert, J.C.M.; Haven, C.J.; Smit, E.G. The effectiveness of health animations in audiences with different health literacy levels: An experimental study. J. Med. Internet Res. 2015, 17, e11. [Google Scholar] [CrossRef] [PubMed]
- Coughlin, S.S.; Hardy, D.; Caplan, L.S. The need for culturally-tailored smartphone applications for weight control. J. Ga. Public Health Assoc. 2016, 5, 228–232. [Google Scholar] [PubMed]
- Vandenbosch, J.; Van den Broucke, S.; Schinckus, L.; Schwarz, P.; Doyle, G.; Pelikan, J.; Muller, I.; Levin-Zamir, D.; Schillinger, D.; Chang, P.; et al. The impact of health literacy on diabetes self-management education. Health Educ. J. 2018, 77, 349–362. [Google Scholar] [CrossRef]
- Choi, N.G.; Dinitto, D.M. The digital divide among low-income homebound older adults: Internet use patterns, eHealth literacy, and attitudes toward computer/Internet use. J. Med. Internet Res. 2013, 15, e93. [Google Scholar] [CrossRef] [PubMed]
- Richtering, S.S.; Hyun, K.; Neubeck, L.; Coorey, G.; Chalmers, J.; Usherwood, T.; Peiris, D.; Chow, C.K.; Redfern, J. eHealth Literacy: Predictors in a population with moderate-to-high cardiovascular risk. JMIR Hum. Factors 2017, 4, e4. [Google Scholar] [CrossRef] [PubMed]
- Guendelman, S.; Broderick, A.; Mlo, H.; Gemmill, A.; Lindeman, D. Listening to communities: Mixed-method study of the engagement of disadvantaged mothers and pregnant women with digital health technologies. J. Med. Internet Res. 2017, 19, e240. [Google Scholar] [CrossRef] [PubMed]
- Tennant, B.; Stellefson, M.; Dodd, V.; Chaney, B.; Chaney, D.; Paige, S.; Alber, J. eHealth literacy and Web 2.0 health information seeking behaviors among baby boomers and older adults. J. Med. Internet Res. 2015, 17, e70. [Google Scholar] [CrossRef] [PubMed]
- Ghaddar, S.F.; Valerio, M.A.; Garcia, C.M.; Hansen, L. Adolescent health literacy: The importance of credible sources for online health information. J. Sch. Health 2012, 82, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Chang, F.-C.; Chiu, C.-H.; Chen, P.-H.; Miao, N.-F.; Lee, C.-M.; Chiang, J.-T.; Pan, Y.-C. Relationship between parental and adolescent eHealth Literacy and online health information seeking in Taiwan. Cyberpsychol. Behav. Soc. Netw. 2015, 18, 618–624. [Google Scholar] [CrossRef] [PubMed]
- Borzekowski, D.L.G. Considering children and health literacy: A theoretical approach. Pediatrics 2009, 124 (Suppl. 3), S282–S288. [Google Scholar] [CrossRef] [PubMed]
- Fox, S. Online Health Search 2006; PEW Internet & American Life Project: Washington, DC, USA, 2006. [Google Scholar]
- European Commission. European Citizens’ Digital Health Literacy; European Union: Brussels, Belgium, 2014. [Google Scholar]
- Rennis, L.; McNamara, G.; Seidel, E.; Shneyderman, Y. Google it!: Urban community college students’ use of the Internet to obtain self-care and personal health information. Coll. Stud. J. 2015, 49, 414–426. [Google Scholar]
- Kontos, E.; Blake, K.D.; Chou, W.-Y.S.; Prestin, A. Predictors of eHealth usage: Insights on the digital divide from the Health Information National Trends Survey 2012. J. Med. Internet Res. 2014, 16, e172. [Google Scholar] [CrossRef] [PubMed]
- Nölke, L.; Mensing, M.; Krämer, A.; Hornberg, C. Sociodemographic and health-(care-)related characteristics of online health information seekers: A cross-sectional German study. BMC Public Health 2015, 15, 31. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.; Mosadeghi, S.; Almario, C.V. Persistent digital divide in access to and use of the Internet as a resource for health information: Results from a California population-based study. Int. J. Med. Inform. 2017, 103, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Baumann, E.; Czerwinski, F.; Reifegerste, D. Gender-specific determinants and patterns of online health information seeking: Results from a representative German health survey. J. Med. Internet Res. 2017, 19, e92. [Google Scholar] [CrossRef] [PubMed]
- Carroll, J.K.; Moorhead, A.; Bond, R.; LeBlanc, W.G.; Petrella, R.J.; Fiscella, K. Who uses mobile phone health apps and does use matter? A secondary data analytics approach. J. Med. Internet Res. 2017, 19, e125. [Google Scholar] [CrossRef] [PubMed]
- Levin-Zamir, D.; Leung, A.Y.M.; Dodson, S.; Rowlands, G. Health literacy in selected populations: Individuals, families, and communities from the international and cultural perspective. Inf. Serv. Use 2017, 37, 131–151. [Google Scholar] [CrossRef]
- Neter, E.; Brainin, E. eHealth literacy: Extending the digital divide to the realm of health information. J. Med. Internet Res. 2012, 14, e19. [Google Scholar] [CrossRef] [PubMed]
- Knapp, C.; Madden, V.; Wang, H.; Sloyer, P.; Shenkman, E. Internet use and eHealth literacy of low-income parents whose children have special health care needs. J. Med. Internet Res. 2011, 13, e75. [Google Scholar] [CrossRef] [PubMed]
- Zibrik, L.; Khan, S.; Bangar, N.; Stacy, E.; Novak Lauscher, H.; Ho, K. Patient and community centered eHealth: Exploring eHealth barriers and facilitators for chronic disease self-management within British Columbia’s immigrant Chinese and Punjabi seniors. Health Policy Technol. 2015, 4, 348–356. [Google Scholar] [CrossRef]
- Chung, S.; Park, B.K.; Nahm, E.-S. The Korean eHealth Literacy Scale (K-eHEALS): Reliability and validity testing in younger adults recruited online. J. Med. Internet Res. 2018, 20, e138. [Google Scholar] [CrossRef] [PubMed]
- Diviani, N.; Dima, A.L.; Schulz, P.J. A psychometric analysis of the Italian version of the eHealth Literacy Scale using item response and classical test theory methods. J. Med. Internet Res. 2017, 19, e114. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-Y.D.; Arozullah, A.M.; Cho, Y.I. Health literacy, social support, and health: A research agenda. Soc. Sci. Med. 2004, 58, 1309–1321. [Google Scholar] [CrossRef]
- Hernán-García, M.; Botello-Díaz, B.; Marcos-Marcos, J.; Toro-Cárdenas, S.; Gil-García, E. Understanding children: A qualitative study on health assets of the Internet in Spain. Int. J. Public Health 2015, 60, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Aponte, J.; Nokes, K.M. Electronic health literacy of older Hispanics with diabetes. Health Promot. Int. 2017, 32, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, L.; Gavier, M.; Helleso, R. Latina breast cancer survivors informational needs: Information partners. Stud. Health Technol. Inform. 2009, 146, 727. [Google Scholar] [PubMed]
- Hayat, T.Z.; Brainin, E.; Neter, E. With some help from my network: Supplementing eHealth Literacy with social ties. J. Med. Internet Res. 2017, 19, e98. [Google Scholar] [CrossRef] [PubMed]
- Wharf Higgins, J.; Begoray, D. Exploring the borderlands between media and health: Conceptualizing “Critical Media Health Literacy”. J. Media Lit. Educ. 2012, 4, 136–148. [Google Scholar]
- Gordon, C.S.; Jones, S.C.; Kervin, L.; Lee, J.K. Empowering students to respond to alcohol advertisements: Results from a pilot study of an Australian media literacy intervention. Aust. N. Z. J. Public Health 2016, 40, 231–232. [Google Scholar] [CrossRef] [PubMed]
- Zoellner, J.M.; Hedrick, V.E.; You, W.; Chen, Y.; Davy, B.M.; Porter, K.J.; Bailey, A.; Lane, H.; Alexander, R.; Estabrooks, P.A. Effects of a behavioral and health literacy intervention to reduce sugar-sweetened beverages: A randomized-controlled trial. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 38. [Google Scholar] [CrossRef] [PubMed]
- Lopes, F.; Araújo, R. Power to health reporters: Health literacy as a tool to avoid pressures from news sources. Port. J. Public Health 2018, 35, 193–201. [Google Scholar] [CrossRef]
- Stellefson, M.; Hanik, B.; Chaney, B.; Chaney, D.; Tennant, B.; Chavarria, E.A. eHealth literacy among college students: A systematic review with implications for eHealth education. J. Med. Internet Res. 2011, 13, e102. [Google Scholar] [CrossRef] [PubMed]
- Paek, H.-J.; Hove, T. Social cognitive factors and perceived social influences that improve adolescent eHealth literacy. Health Commun. 2012, 27, 727–737. [Google Scholar] [CrossRef] [PubMed]
- Xie, B. Effects of an eHealth literacy intervention for older adults. J. Med. Internet Res. 2011, 13, e90. [Google Scholar] [CrossRef] [PubMed]
- Xie, B. Older adults, e-health literacy, and collaborative learning: An experimental study. J. Am. Soc. Inf. Sci. 2011, 62, 933–946. [Google Scholar] [CrossRef]
- Xie, B. Experimenting on the impact of learning methods and information presentation channels on older adults’ e-health literacy. J. Am. Soc. Inf. Sci. 2011, 62, 1797–1807. [Google Scholar] [CrossRef]
- Watkins, I.; Xie, B. eHealth literacy interventions for older adults: A systematic review of the literature. J. Med. Internet Res. 2014, 16, e225. [Google Scholar] [CrossRef] [PubMed]
- Vayena, E.; Dzenowagis, J.; Brownstein, J.S.; Sheikh, A. Policy implications of Big Data in the health sector. Bull. World Health Organ. 2018, 96, 66–68. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- Paasche-Orlow, M.K.; Parker, R.M.; Gazmararian, J.A.; Nielsen-Bohlman, L.T.; Rudd, R.E. The prevalence of limited health literacy. J. Gen. Intern. Med. 2005, 20, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Paakkari, L.; Paakkari, O. Health literacy as a learning outcome in schools. Health Educ. 2012, 112, 133–152. [Google Scholar] [CrossRef]
- Bandura, A. Social Learning Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1977; ISBN 978-0-138-16744-8. [Google Scholar]
- De Wit, L.; Fenenga, C.; Giammarchi, C.; di Furia, L.; Hutter, I.; de Winter, A.; Meijering, L. Community-based initiatives improving critical health literacy: A systematic review and meta-synthesis of qualitative evidence. BMC Public Health 2017, 18, 40. [Google Scholar] [CrossRef] [PubMed]
- Rudd, R.E.; Rosenfeld, L.; Simonds, V.W. Health literacy: A new area of research with links to communication. Atl. J. Commun. 2012, 20, 16–30. [Google Scholar] [CrossRef]

© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Levin-Zamir, D.; Bertschi, I. Media Health Literacy, eHealth Literacy, and the Role of the Social Environment in Context. Int. J. Environ. Res. Public Health 2018, 15, 1643. https://doi.org/10.3390/ijerph15081643
Levin-Zamir D, Bertschi I. Media Health Literacy, eHealth Literacy, and the Role of the Social Environment in Context. International Journal of Environmental Research and Public Health. 2018; 15(8):1643. https://doi.org/10.3390/ijerph15081643
Chicago/Turabian StyleLevin-Zamir, Diane, and Isabella Bertschi. 2018. "Media Health Literacy, eHealth Literacy, and the Role of the Social Environment in Context" International Journal of Environmental Research and Public Health 15, no. 8: 1643. https://doi.org/10.3390/ijerph15081643
APA StyleLevin-Zamir, D., & Bertschi, I. (2018). Media Health Literacy, eHealth Literacy, and the Role of the Social Environment in Context. International Journal of Environmental Research and Public Health, 15(8), 1643. https://doi.org/10.3390/ijerph15081643