Cost and Affordability of Diets Modelled on Current Eating Patterns and on Dietary Guidelines, for New Zealand Total Population, Māori and Pacific Households

 ,
,
Abstract
1. Introduction
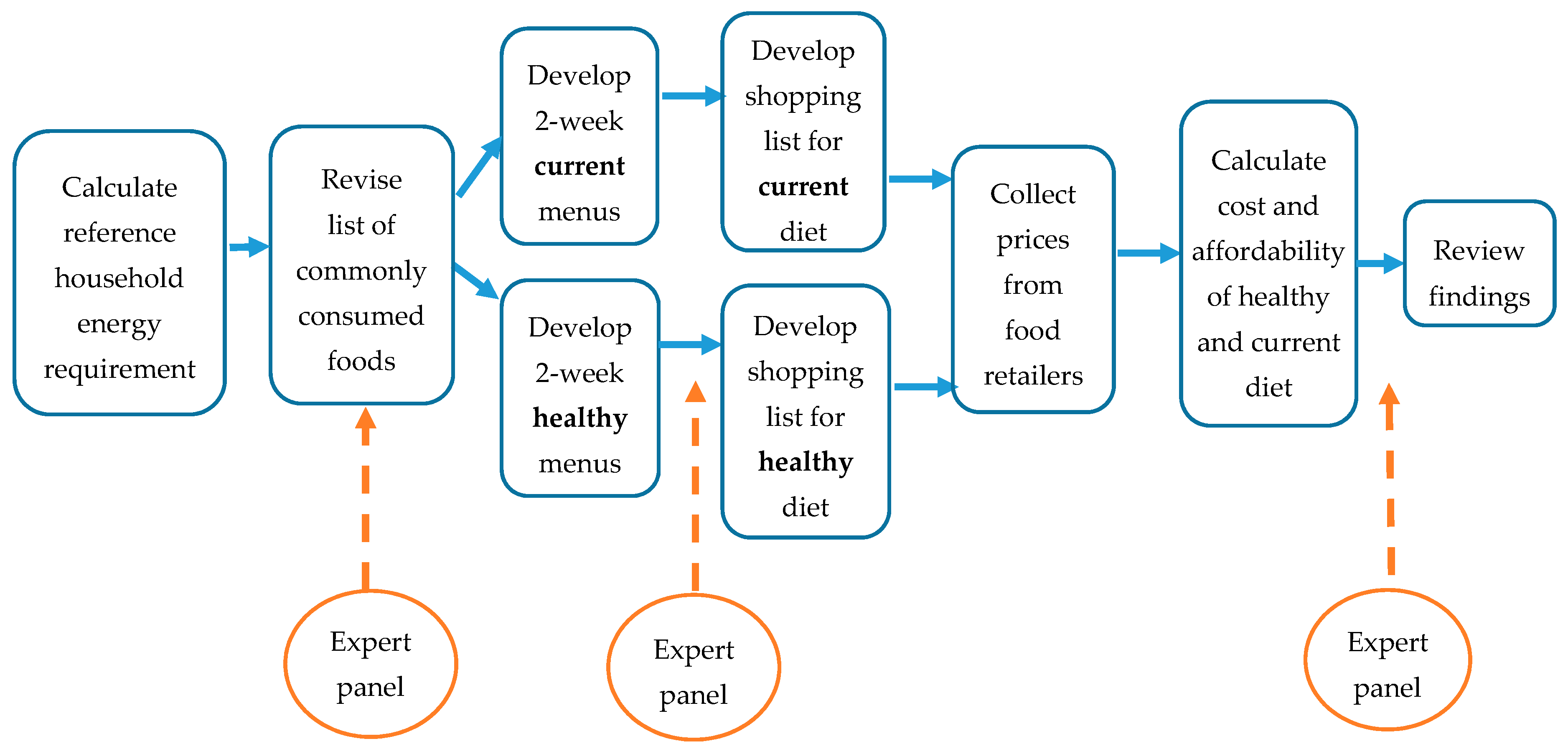
2. Materials and Methods
2.1. Expert Panels
2.2. Common Foods
2.3. Household Energy Requirements
2.4. Diet Constraints
2.5. Gifting and Gathering of Food
2.6. Menu Development
2.7. Price Collection
2.8. Analysis
3. Results
3.1. Energy Requirements
3.2. Cost of Diets
3.3. Affordability of Diets
3.4. Cost Scenarios
4. Discussion
4.1. Strengths
4.2. Limitations
4.3. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- GBD 2016 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters or risks, 1990–2015: A systematic analysis for the Global Burden of Diseases Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar]
- University of Otago and Ministry of Health. A Focus on Nutrition: Key Findings of the 2008/09 New Zealand Adult Nutrition Survey; Ministry of Health: Wellington, New Zealand, 2011.
- Ministry of Health. New Zealand Health Survey 2016/17. Available online: https://www.health.govt.nz/nz-health-statistics/national-collections-and-surveys/surveys/current-recent-surveys/new-zealand-health-survey#published (accessed on 20 November 2017).
- Swinburn, B.; Egger, G.; Raza, F. Dissecting obesogenic environments: The development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev. Med. 1999, 29, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.; Sacks, G.; Vandevijvere, S.; Kumanyika, S.; Lobstein, T.; Neal, B.; Barquera, S.; Friel, S.; Hawkes, C.; Kelly, B.; et al. INFORMAS (International Network for Food and Obesity/non-communicable diseases Research, Monitoring and Action Support): Overview and key principles. Obes. Rev. 2013, 14 (Suppl. 1), 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kumanyika, S.K. Environmental influences on childhood obesity: Ethnic and cultural influences in context. Physiol. Behav. 2008, 94, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health; Kahukura, T. Māori Health Chart Book 2015, 3rd ed.; Ministry of Health: Wellington, New Zealand, 2015.
- Berghan, G.; Came, H.; Coupe, N.; Doole, C.; Fay, J.; McCreanor, T.; Simpson, T. Tiriti-Based Health Promotion Practice. STIR: Stop Institutional Racism. 2017. Available online: https://trc.org.nz/treaty-waitangi-based-practice-health-promotion (accessed on 7 February 2018).
- Sorensen, D.; Jensen, S.; Rigamoto, M.; Pritchard, M. Pacific People in New Zealand: How Are We doing? Pasifika Futures Ltd.: Auckland, New Zealand, 2015. [Google Scholar]
- Lee, A.; Ni Mhurchu, C.; Sacks, G.; Swinburn, B.; Snowdon, W.; Vandevijvere, S.; Hawkes, C.; L’Abbé, M.; Rayner, M.; Sanders, D.; et al. Monitoring the price and affordability of foods and diets globally. Obes. Rev. 2013, 14 (Suppl. 1), 82–95. [Google Scholar] [CrossRef] [PubMed]
- Ni Mhurchu, C.; Eyles, H.; Dixon, R.; Matoe, L.; Teevale, T.; Meagher-Lundberg, P. Economic incentives to promote healthier food purchases: Exploring acceptability and key factors for success. Health Promot. Int. 2012, 27, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, S.; Lawton, J.; Caraher, M.; Singh, G.; Horsley, K.; Mussa, F. A tale of two localities: Healthy eating on a restricted income. Health Educ. J. 2011, 70, 48–56. [Google Scholar] [CrossRef]
- Bowyer, S.; Caraher, M.; Eilbert, K.; Carr-Hill, R. Shopping for food: Lessons from a London borough. Br. Food J. 2009, 111, 452–474. [Google Scholar] [CrossRef]
- Goedemé, T.; Storms, B.; Van den Bosch, K. Pilot Project: Developing a Common Methodology on Reference Budgets in Europe; European Commission: Brussels, Belgium, 2015. [Google Scholar]
- Rao, M.; Afshin, A.; Singh, G.; Mozaffarian, D. Do healthier foods and diet patterns cost more than less healthy options? A systematic review and meta-analysis. BMJ Open 2013, 3, e004277. [Google Scholar] [CrossRef] [PubMed]
- Kettings, C.; Sinclair, A.; Voevodin, M. A healthy diet consistent with Australian health recommendations is too expensive for welfare-dependent families. Aust. N. Z. J. Public Health 2009, 33, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Nathoo, T.; Shoveller, J. Do healthy food baskets assess food security? Chronic Dis. Can. 2003, 24, 65–69. [Google Scholar] [PubMed]
- Statistics New Zealand. Adult National Nutrition Survey 2008/09 Confidentialised unit Record Files; Statistics New Zealand: Wellington, New Zealand, 2011.
- National Institute of Diabetes and Digestive and Kidney Diseases. Body Weight Planner. Available online: https://www.niddk.nih.gov/health-information/weight-management/body-weight-planner (accessed on 6 April 2017).
- Ministry of Health. Annual Update of Key Results 2013/14: New Zealand Health Survey. Available online: https://www.health.govt.nz/publication/annual-update-key-results-2013-14-new-zealand-health-survey (accessed on 20 November 2017).
- FAO; WHO; UNU. Report on Human Energy Requirements; Food and Agricultural Organization; World Health Organization; United Nations University Expert Consultation: Rome, Italy, 2004. [Google Scholar]
- CDC Growth Charts 2010. Available online: http://www.cdc.gov/growthcharts/index.htm (accessed on 11 January 2016).
- Clinical Trials Research Unit and Synovate. A National Survey of Children and Young People’s Physical Activity and Dietary Behaviours in New Zealand: 2008/09: Key Findings; Ministry of Health: Wellington, New Zealand, 2010.
- Hall, K.; Butte, N.; Swinburn, B.; Chow, C. Dynamics of childhood growth and obesity: Development and validation of a quantitative mathematical model. Lancet Diabetes Endocrinol. 2013, 10, 97–105. [Google Scholar] [CrossRef]
- Ministry of Health. NZ Food NZ Children: Key Results of the 2002 National Children’s Nutrition Survey; Ministry of Health: Wellington, New Zealand, 2003.
- Skeaff, S.; McLean, R.; Mann, J.; Williams, S. The Impact of Mandatory Fortification of Bread with Iodine; MPI Technical Paper No: 2013/025; Ministry of Primary Industries: Wellington, New Zealand, 2013.
- Ministry of Health. Eating and Activity Guidelines for New Zealand Adults. 2015. Available online: https://www.health.govt.nz/publication/eating-and-activity-guidelines-new-zealand-adults (accessed on 20 November 2017).
- NHMRC. Nutrient Reference Values for Australia and New Zealand; National Health and Medical Research Council: Canberra, Australia, 2006.
- Xyris Software (Australia) Pty Ltd. FoodWorks 7 Professional [computer program]; Xyris Software (Australia) Pty Ltd.: Brisbane, Australia, 2012. [Google Scholar]
- Dignan, C.; Burlingame, B.; Kumar, S.; Aalbersberg, W. The Pacific Island Food Composition Tables; Food and Agriculture Organization of the United Nations: Rome, Italy, 2004. [Google Scholar]
- New Zealand Institute of Plant and Food Research. FOODfiles 2013; The New Zealand Institute of Plant and Food Research and the New Zealand Ministry of Health: Palmerston North, New Zealand, 2013.
- Mackay, S.; Vandevijvere, S.; Xie, P.; Lee, A.; Swinburn, B. Paying for convenience: Comparing the cost of takeaway meals with their healthier home-cooked counterparts in New Zealand. Public Health Nutr. 2017, 20, 2269–2276. [Google Scholar] [CrossRef] [PubMed]
- OECD Income Distribution and Poverty. 2016. Available online: http://stats.oecd.org/Index.aspx?DataSetCode=IDD (accessed on 30 May 2016).
- Ministry of Social Development. Benefit Rates at 1 April 2016. Available online: http://www.workandincome.govt.nz/products/benefit-rates/benefit-rates-april-2016.html#null (accessed on 4 May 2016).
- Inland Revenue. Estimate Your Working for Families Tax Credits 2016. Available online: http://www.ird.govt.nz/calculators/keyword/wff-tax-credits/calculator-wfftc-estimate-2016.html (accessed on 30 May 2016).
- Employment New Zealand. The Minimum Wage. 1 April 2016. Available online: https://www.employment.govt.nz/hours-and-wages/pay/minimum-wage/ (accessed on 30 May 2016).
- Lee, A.J.; Kane, S.; Ramsey, R.; Good, E.; Dick, M. Testing the price and affordability of healthy and current (unhealthy) diets and the potential impacts of policy change in Australia. BMC Public Health 2016, 16, 315. [Google Scholar] [CrossRef] [PubMed]
- Department of Human Nutrition. Information Package for Users of the New Zealand Estimated Food Costs 2016; University of Otago: Dunedin, New Zealand, 2016. [Google Scholar]
- Landrigan, T.; Kerr, D.; Dhaliwal, S.; Savage, V.; Pollard, C. Removing the Australian tax exemption on healthy food adds food stress to families vulnerable to poor nutrition. Aust NZ J Public Health 2017. [Google Scholar] [CrossRef] [PubMed]
- New Zealand Legislation. Goods and Services Tax Act 1985. Available online: http://www.legislation.govt.nz/act/public/1985/0141/latest/DLM81035.html (accessed on 30 August 2016).
- Poslusna, K.; Ruprich, J.; de Vries, J.; Jakubikova, M.; van’t Veer, P. Misreporting of energy and micronutrient intake estimated by food records and 24 h recalls, control and adjustment methods in practice. Br. Nutr. 2009, 101 (Suppl. 2), S73–S85. [Google Scholar] [CrossRef] [PubMed]
- Statistics New Zealand. Food Price Index: July 2017. Available online: http://www.stats.govt.nz/browse_for_stats/economic_indicators/prices_indexes/FoodPriceIndex_HOTPJul17.aspx (accessed on 10 October 2017).
- Andajani-Sutjahjo, S.; Ball, K.; Warren, N.; Inglis, V.; Crawford, D. Perceived personal, social and environmental barriers to weight maintenance among young women: A community survey. Int. J. Behav. Nutr. Phys. Act. 2004, 1, 15. [Google Scholar] [CrossRef] [PubMed]
- Funaki-Tahifote, M.; Fung, M.; Timaloa, Y.; Langi, T.; Lafuloa, S.; Manuopangai, V.; Johnston, O. Better Quality and Reduced Quantity in Food/Drinks in Pacific Settings; Health Promotion Agency: Wellington, New Zealand, 2016.
- Statistics New Zealand. Food Price Index Selected Monthly Weighted Average Prices for New Zealand. 2017. Available online: http://www.stats.govt.nz/infoshare/SelectVariables.aspx?pxID=e3632d54-64c5-45c0-80f5-721bc77c2bca (accessed on 30 May 2017).


{kind=link}
| Food Group | Healthy Diet | Current Diet | Healthy Diet | Current Diet | Healthy Diet | Current Diet |
|---|---|---|---|---|---|---|
| All | All | Māori | Māori | Pacific | Pacific | |
| Fruits | 18.1% | 9.4% | 13.6% | 8.0% | 14.1% | 7.0% |
| Vegetables | 17.6% | 11.8% | 20.8% | 10.4% | 25.2% | 12.9% |
| Grains | 13.8% | 6.9% | 14.0% | 5.5% | 15.4% | 6.8% |
| Dairy | 11.0% | 5.5% | 11.2% | 6.8% | 12.4% | 5.2% |
| Protein | 37.9% | 31.4% | 37.9% | 22.0% | 30.1% | 26.6% |
| Fats and Oils | 1.5% | 1.3% | 0.7% | 1.4% | 1.50% | 0.9% |
| Sauces and Spreads | 0 | 2.0% | 1.6% | 2.3% | 0 | 3.0% |
| Snacks, sweets | 0 | 6.9% | 0 | 11.5% | 0 | 8.0% |
| Processed meats | 0 | 4.4% | 0 | 5.3% | 0 | 5.2% |
| Beverages | 0 | 3.3% | 0 | 5.2% | 0 | 3.8% |
| Takeaway | 0 | 10.8% | 0 | 15.9% | 0 | 14.9% |
| Alcohol | 0 | 6.4% | 0 | 5.7% | 0 | 5.8% |
| Proportion less healthy food | 0 | 35.5% | 1.6% | 45.9% | 0 | 40.7% |
| Total cost | $649.06 | $671.69 | $558.50 | $561.68 | $526.92 | $550.52 |
| Standard Diet | GST off Core Foods | |||
|---|---|---|---|---|
| Healthy Diet % Income | Current Diet % Income | Healthy Diet % Income | Current Diet % Income | |
| Median Household income ($1733 per week) | ||||
| Total population | 18.7% | 19.4% | 16.3% | 17.7% |
| Māori | 16.1% | 16.2% | 14.0% | 15.1% |
| Pacific | 15.2% | 15.9% | 13.2% | 15.2% |
| Minimum Wage ($1115 per week) | ||||
| Total population | 32.8% | 33.9% | 28.5% | 31.0% |
| Māori | 28.2% | 28.3% | 24.5% | 26.3% |
| Pacific | 26.6% | 27.8% | 23.1% | 26.6% |
| Income support ($636 per week) | ||||
| Total population | 51.0% | 52.8% | 44.4% | 48.2% |
| Māori | 43.9% | 44.2% | 38.2% | 41.0% |
| Pacific | 41.4% | 43.3% | 36.0% | 41.4% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mackay, S.; Buch, T.; Vandevijvere, S.; Goodwin, R.; Korohina, E.; Funaki-Tahifote, M.; Lee, A.; Swinburn, B. Cost and Affordability of Diets Modelled on Current Eating Patterns and on Dietary Guidelines, for New Zealand Total Population, Māori and Pacific Households. Int. J. Environ. Res. Public Health 2018, 15, 1255. https://doi.org/10.3390/ijerph15061255
Mackay S, Buch T, Vandevijvere S, Goodwin R, Korohina E, Funaki-Tahifote M, Lee A, Swinburn B. Cost and Affordability of Diets Modelled on Current Eating Patterns and on Dietary Guidelines, for New Zealand Total Population, Māori and Pacific Households. International Journal of Environmental Research and Public Health. 2018; 15(6):1255. https://doi.org/10.3390/ijerph15061255
Chicago/Turabian StyleMackay, Sally, Tina Buch, Stefanie Vandevijvere, Rawinia Goodwin, Erina Korohina, Mafi Funaki-Tahifote, Amanda Lee, and Boyd Swinburn. 2018. "Cost and Affordability of Diets Modelled on Current Eating Patterns and on Dietary Guidelines, for New Zealand Total Population, Māori and Pacific Households" International Journal of Environmental Research and Public Health 15, no. 6: 1255. https://doi.org/10.3390/ijerph15061255
APA StyleMackay, S., Buch, T., Vandevijvere, S., Goodwin, R., Korohina, E., Funaki-Tahifote, M., Lee, A., & Swinburn, B. (2018). Cost and Affordability of Diets Modelled on Current Eating Patterns and on Dietary Guidelines, for New Zealand Total Population, Māori and Pacific Households. International Journal of Environmental Research and Public Health, 15(6), 1255. https://doi.org/10.3390/ijerph15061255