Gender and Body-Fat Status as Predictors of Parental Feeding Styles and Children’s Nutritional Knowledge, Eating Habits and Behaviours

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.2.1. Dietary Knowledge and Habits (DKH)
2.2.2. Children’s Eating Behavior Questionnaire (CEBQ)
2.2.3. Parental Feeding Style Questionnaire (PFSQ)
2.2.4. Body Composition Analyzer
2.3. Statistical Analysis
3. Results
3.1. Children’s Nutritional Knowledge, Eating Habits and Behaviours, Parental Feeding Styles, and Body-Fat percentage (%BF) Descriptive Statistics
3.2. Body-Fat Status of the Five-Year-Old Boys and Girls and Their Parents
3.3. Determination of Body-Fat Status
3.4. Parents’ Body-Fat Status and their Feeding Styles
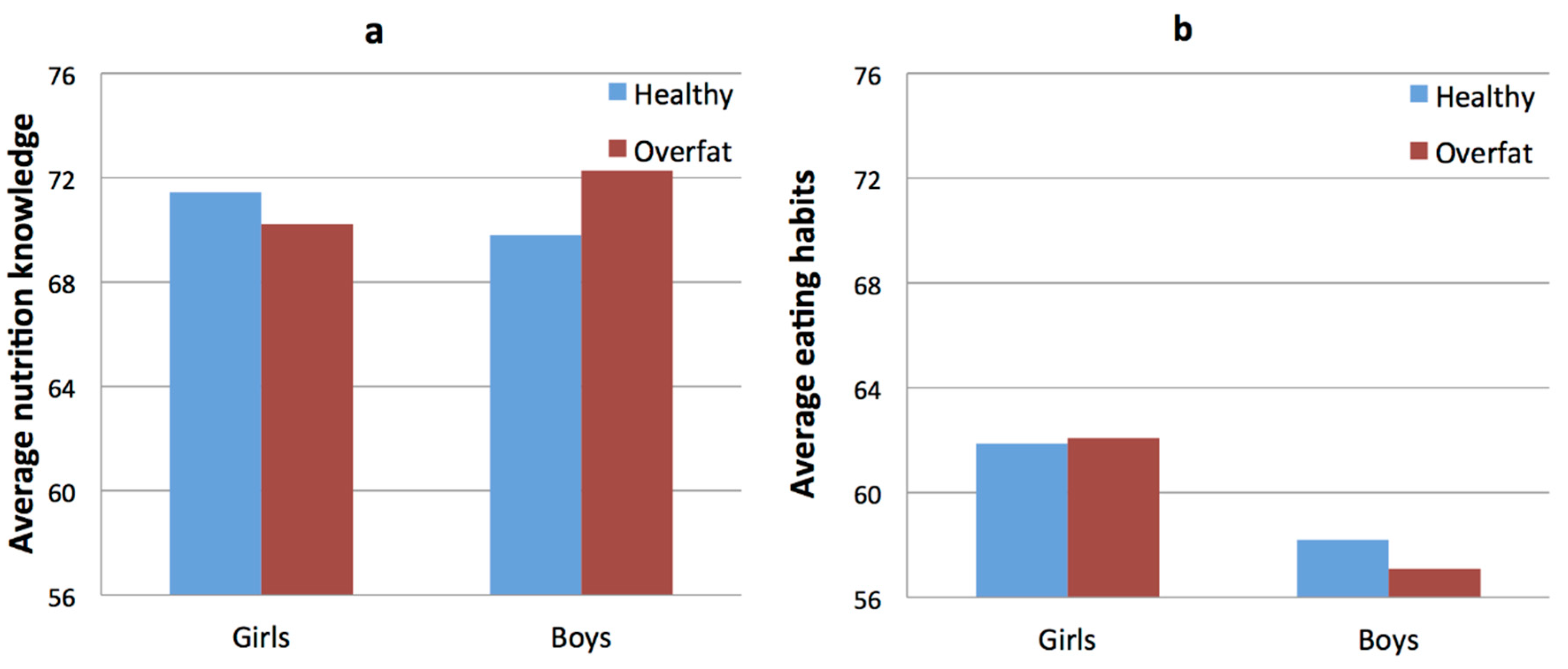
3.5. Children’s Body Fat Status and Their Nutrition Knowledge and Eating Habits
3.6. Children’s Body-Fat Status and Their Parents’ Feeding Styles
3.7. Children’s Body-Fat Status and Their Eating Behaviors
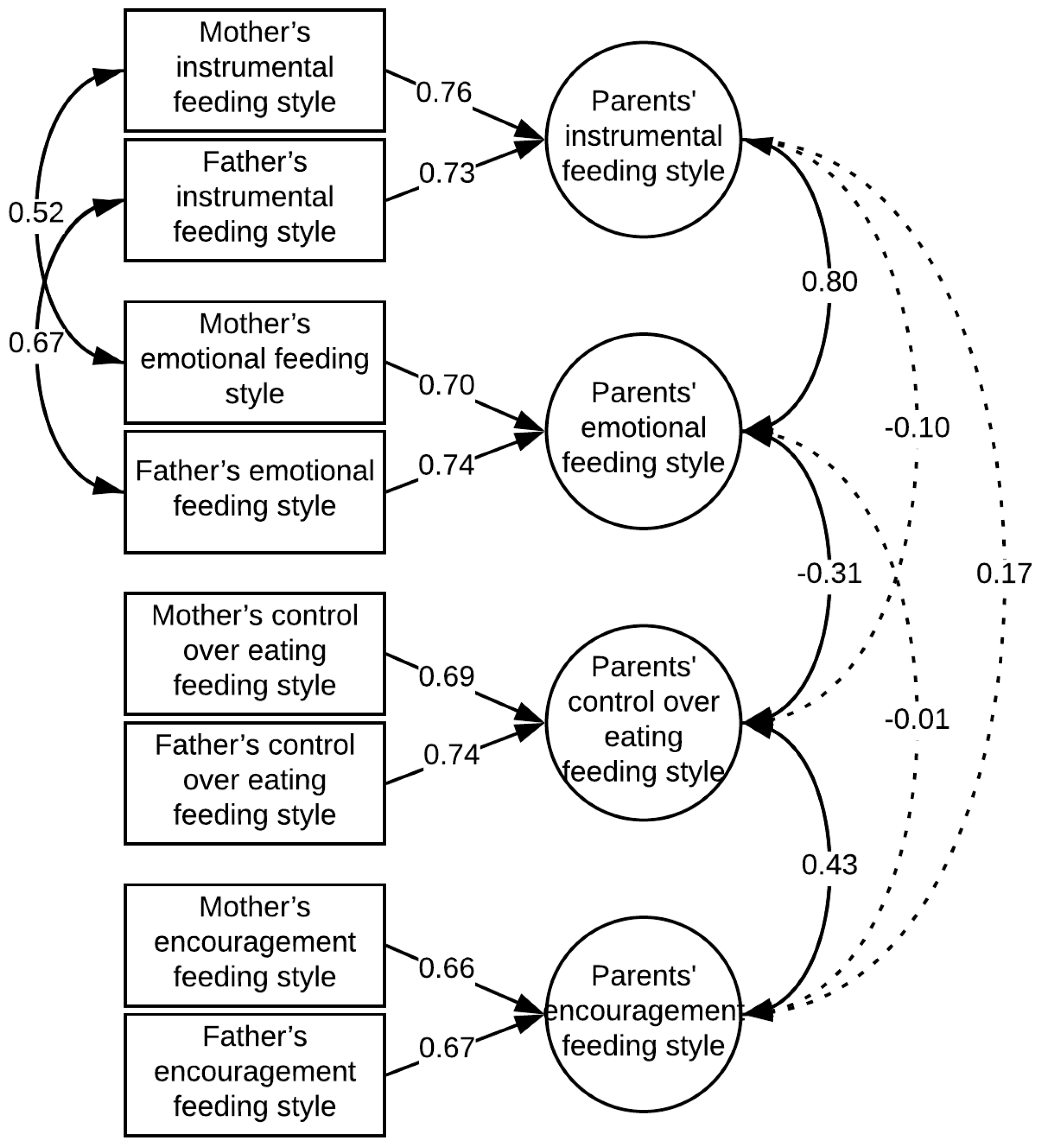
3.8. Parents’ Feeding Styles and Children’s Eating Behaviors
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Scaglioni, S.; Salvioni, M.; Galimberti, C. Influence of parental attitudes in the development of children eating behaviour. Br. J. Nutr. 2008, 99 (Suppl. 1), 22–25. [Google Scholar] [CrossRef] [PubMed]
- Anzman, S.L.; Rollins, B.Y.; Birch, L.L. Parental influence on children’s early eating environments and obesity risk: Implications for prevention. Int. J. Obes. 2010, 34, 1116–1124. [Google Scholar] [CrossRef] [PubMed]
- Butte, N.; Cobb, K.; Dwyer, J.; Graney, L.; Heird, W.; Rickard, K. The Start Healthy Feeding Guidelines for Infants and Toddlers. J. Am. Diet. Assoc. 2004, 104, 442–454. [Google Scholar] [CrossRef] [PubMed]
- Cashdan, E. A sensitive period for learning about food. Hum. Nat. 1994, 5, 279–291. [Google Scholar] [CrossRef] [PubMed]
- Coulthard, H.; Harris, G.; Emmett, P. Delayed introduction of lumpy foods to children during the complementary feeding period affects child’s food acceptance and feeding at 7 years of age. Mater. Child Nutr. 2009, 5, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, C.; Issanchou, S.; Nicklaus, S. Developmental changes in the acceptance of the five basic tastes in the first year of life. Br. J. Nutr. 2009, 102, 1375–1385. [Google Scholar] [CrossRef] [PubMed]
- Ruottinen, S.; Niinikoski, H.; Lagström, H.; Rönnemaa, T.; Hakanen, M.; Viikari, J.; Jokinen, E.; Simell, O. High sucrose intake is associated with poor quality of diet and growth between 13 months and 9 years of age: The special Turku Coronary Risk Factor Intervention Project. Pediatrics 2008, 121, e1676–e1685. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, C.; Scholtens, P.A.M.J.; Lalanne, A.; Weenen, H.; Nicklaus, S. Development of healthy eating habits early in life. Review of recent evidence and selected guidelines. Appetite 2011, 57, 796–807. [Google Scholar] [CrossRef] [PubMed]
- Maier, A.; Chabanet, C.; Schaal, B.; Leathwood, P.; Issanchou, S. Food-related sensory experience from birth through weaning: Contrasted patterns in two nearby European regions. Appetite 2007, 49, 429–440. [Google Scholar] [CrossRef] [PubMed]
- Havermans, R.C.; Jansen, A. Increasing children’s liking of vegetables through flavour-flavour learning. Appetite 2007, 48, 259–262. [Google Scholar] [CrossRef] [PubMed]
- Cutting, T.M.; Fisher, J.O.; Grimm-Thomas, K.; Birch, L.L. Like mother, like daughter: Familial patterns of overweight are mediated by mothers’ dietary disinhibition. Am. J. Clin. Nutr. 1999, 69, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.L.; Birch, L.L. Parents’ and children’s adiposity and eating style. Pediatrics 1994, 94, 653–661. [Google Scholar] [PubMed]
- Skinner, J.D.; Carruth, B.R.; Bounds, W.; Ziegler, P.; Reidy, K. Do food-related experiences in the first 2 years of life predict dietary variety in school-aged children? J. Nutr. Educ. Behav. 2002, 34, 310–315. [Google Scholar] [CrossRef]
- Gillman, M.W.; Rifas-Shiman, S.L.; Frazier, A.L.; Rockett, H.R.; Camargo, C.A., Jr.; Field, A.E.; Berkey, C.S.; Colditz, G.A. Family dinner and diet quality among older children and adolescents. Arch. Fam. Med. 2000, 9, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L.; Fisher, J.O. Mothers’ child-feeding practices influence daughters’ eating and weight. Am. J. Clin. Nutr. 2000, 71, 1054–1061. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L.; Fisher, J.O.; Grimm-Thomas, K.; Markey, C.N.; Sawyer, R.; Johnson, S.L. Confirmatory factor analysis of the Child Feeding Questionnaire: A measure of parental attitudes, beliefs and practices about child feeding and obesity proneness. Appetite 2001, 36, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.; Duncanson, K.; Burrows, T. A systematic review investigating associations between parenting style and child feeding behaviours. J. Hum. Nutr. Diet. 2014, 27, 557–568. [Google Scholar] [CrossRef] [PubMed]
- Larsen, J.K.; Hermans, R.C.J.; Sleddens, E.F.C.; Engels, R.C.M.E.; Fisher, J.O.; Kremers, S.P.J. How parental dietary behavior and food parenting practices affect children’s dietary behavior. Interacting sources of influence? Appetite 2015, 89, 246–257. [Google Scholar] [CrossRef] [PubMed]
- Blissett, J. Relationships between parenting style, feeding style and feeding practices and fruit and vegetable consumption in early childhood. Appetite 2011, 57, 826–831. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, T.M.; Hughes, S.O.; Watson, K.B.; Baranowski, T.; Nicklas, T.A.; Fisher, J.O.; Beltran, A.; Baranowski, J.C.; Qu, H.; Shewchuk, R.M. Parenting practices are associated with fruit and vegetable consumption in pre-school children. Public Health Nutr. 2010, 13, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.O.; Patrick, H.; Power, T.G.; Fisher, J.O.; Anderson, C.B.; Nicklas, T.A. The impact of child care providers’ feeding on children’s food consumption. J. Dev. Behav. Pediatr. 2007, 28, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Hennessy, E.; Hughes, S.O.; Goldberg, J.P.; Hyatt, R.R.; Economos, C.D. Permissive parental feeding behavior is associated with an increase in intake of low-nutrient-dense foods among American children living in rural communities. J. Acad. Nutr. Diet. 2012, 112, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Patrick, H.; Nicklas, T.A.; Hughes, S.O.; Morales, M. The benefits of authoritative feeding style: Caregiver feeding styles and children’s food consumption patterns. Appetite 2005, 44, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Moens, E.; Braet, C.; Soetens, B. Observation of Family Functioning at Mealtime: A Comparison between Families of Children with and Without Overweight. J. Pediatr. Psychol. 2007, 32, 52–63. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.J.; Crawford, D.A.; Salmon, J.; Carver, A.; Garnett, S.P.; Baur, L.A. Associations between the home food environment and obesity-promoting eating behaviors in adolescence. Obesity 2007, 15, 719–730. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, R.C. Predicting preschooler obesity at birth: The role of maternal obesity in early pregnancy. Pediatrics 2004, 114, e29–e36. [Google Scholar] [CrossRef] [PubMed]
- Strauss, R.S.; Knight, J. Influence of the home environment on the development of obesity in children. Pediatrics 1999, 103, e85. [Google Scholar] [CrossRef] [PubMed]
- Tschann, J.M.; Gregorich, S.E.; Penilla, C.; Pasch, L.A.; de Groat, C.L.; Flores, E.; Deardorff, J.; Greenspan, L.C.; Butte, N.F. Parental feeding practices in Mexican American families: Initial test of an expanded measure. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 6. [Google Scholar] [CrossRef] [PubMed]
- Francis, L.A.; Hofer, S.M.; Birch, L.L. Predictors of maternal child-feeding style: Maternal and child characteristics. Appetite 2001, 37, 231–243. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, R.F.; Paxton, S.J.; McLean, S.A.; Campbell, K.J.; Wertheim, E.H.; Skouteris, H.; Gibbons, K. Do maternal body dissatisfaction and dietary restraint predict weight gain in young pre-school children? A 1-year follow-up study. Appetite 2013, 67, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Courtenay, W.H. Engendering health: A social constructionist examination of men’s health beliefs and behaviors. Psychol. Men Masc. 2000, 1, 4–15. [Google Scholar] [CrossRef]
- Vartanian, L.R.; Herman, C.P.; Polivy, J. Consumption stereotypes and impression management: How you are what you eat. Appetite 2007, 48, 265–277. [Google Scholar] [CrossRef] [PubMed]
- Sparks, P.; Conner, M.; James, R.; Shepherd, R.; Povey, R. Ambivalence about health-related behaviours: An exploration in the domain of food choice. Br. J. Health Psychol. 2001, 6 Pt 1, 53–68. [Google Scholar] [CrossRef] [PubMed]
- Lipowska, M.; Lipowski, M. Children’s Awareness of Healthy Behaviours—Validity of Beauty & Health and Dietary Knowledge & Habits Scales. Health Psychol. Rep. 2018, 6. [Google Scholar]
- Wardle, J.; Guthrie, C.A.; Sanderson, S.; Rapoport, L. Development of the Children’s Eating Behaviour Questionnaire. J. Child Psychol. Psychiatry Allied Discip. 2001, 42, 963. [Google Scholar] [CrossRef]
- Carnell, S.; Wardle, J. Measuring behavioural susceptibility to obesity: Validation of the Child Eating Behaviour Questionnaire. Appetite 2007, 48, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Sanderson, S.; Guthrie, C.A.; Rapoport, L.; Plomin, R. Parental feeding style and the inter-generational transmission of obesity risk. Obes. Res. 2002, 10, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Maffetone, P.B.; Rivera-Dominguez, I.; Laursen, P.B. Overfat and Underfat: New Terms and Definitions Long Overdue. Front. Public Health 2016, 4, 279. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, H.D.; Cole, T.J.; Fry, T.; Jebb, S.A.; Prentice, A.M. Body fat reference curves for children. Int. J. Obes. 2006, 30, 598–602. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, D.; Heymsfield, S.B.; Heo, M.; Jebb, S.A.; Murgatroyd, P.R.; Sakamoto, Y. Healthy percentage body fat ranges: An approach for developing guidelines based on body mass index. Am. J. Clin. Nutr. 2000, 72, 694–701. [Google Scholar] [CrossRef] [PubMed]
- Rosseel, Y. Lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef]
- Lipowska, M.; Lipowski, M.; Pawlicka, P. “Daughter and son: A completely different story”? Gender as a moderator of the relationship between sexism and parental attitudes. Health Psychol. Rep. 2016, 4, 224–236. [Google Scholar] [CrossRef]
- Gibson, L.Y.; Byrne, S.M.; Davis, E.A.; Blair, E.; Jacoby, P.; Zubrick, S.R. The role of family and maternal factors in childhood obesity. Med. J. Aust. 2007, 186, 591–595. [Google Scholar] [PubMed]
- Muthuri, S.K.; Onywera, V.O.; Tremblay, M.S.; Broyles, S.T.; Chaput, J.P.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; Lambert, E.V.; et al. Relationships between Parental Education and Overweight with Childhood Overweight and Physical Activity in 9–11 Year Old Children: Results from a 12-Country Study. PLoS ONE 2016, 11, e0147746. [Google Scholar] [CrossRef] [PubMed]
- Katz-Wise, S.L.; Budge, S.L.; Lindberg, S.M.; Hyde, J.S. Individuation or Identification? Self-Objectification and the Mother-Adolescent Relationship. Psychol. Women Q. 2013, 37, 366–380. [Google Scholar] [CrossRef] [PubMed]
- Johannsen, D.L.; Johannsen, N.M.; Specker, B.L. Influence of parents’ eating behaviors and child feeding practices on children’s weight status. Obesity 2006, 14, 431–439. [Google Scholar] [CrossRef] [PubMed]
- Lo, K.; Cheung, C.; Lee, A.; Tam, W.W.S.; Keung, V. Associations between Parental Feeding Styles and Childhood Eating Habits: A Survey of Hong Kong Pre-School Children. PLoS ONE 2015, 10, e0124753. [Google Scholar] [CrossRef] [PubMed]
- Sleddens, E.F.C.; Kremers, S.P.J.; De Vries, N.K.; Thijs, C. Relationship between parental feeding styles and eating behaviours of Dutch children aged 6–7. Appetite 2010, 54, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Rodenburg, G.; Kremers, S.P.J.; Oenema, A.; van de Mheen, D. Associations of parental feeding styles with child snacking behaviour and weight in the context of general parenting. Public Health Nutr. 2014, 17, 960–969. [Google Scholar] [CrossRef] [PubMed]
- Kosakowska-Berezecka, N.; Korzeniewska, L.; Kaczorowska, M. Sharing housework can be healthy: Cultural and psychological factors influencing men’s involvement in household maintenance. Health Psychol. Rep. 2016, 4, 189–201. [Google Scholar] [CrossRef]
- Birch, L.L.; Fisher, J.O. Development of Eating Behaviors among Children and Adolescents. Pediatrics 1998, 101 (Suppl. 2), 539–549. [Google Scholar] [PubMed]
- Birch, L.L. Development of food preferences. Annu. Rev. Nutr. 1999, 19, 41–62. [Google Scholar] [CrossRef] [PubMed]
- Bellisle, F.; Rolland-Cachera, M.F. Three consecutive (1993, 1995, 1997) surveys of food intake, nutritional attitudes and knowledge, and lifestyle in 1000 French children, aged 9–11 years. J. Hum. Nutr. Diet. 2007, 20, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Mantzios, M.; Egan, H. An exploratory examination of mindfulness, self-compassion, and mindful eating in relation to motivations to eat palatable foods and BMI. Health Psychol. Rep. 2018, 6. [Google Scholar] [CrossRef]
- Drewnowski, A. Taste preferences and food intake. Annu. Rev. Nutr. 1997, 17, 237–253. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.; Hackett, A.F. Eating habits of 11–14-year-old schoolchildren living in less affluent areas of Liverpool, UK. J. Hum. Nutr. Diet. 1997, 10, 135–144. [Google Scholar] [CrossRef]
- Wardle, J. Eating behaviour and obesity. Obes. Rev. 2007, 8 (Suppl. 1), 73–75. [Google Scholar] [CrossRef] [PubMed]
- Carnell, S.; Benson, L.; Driggin, E.; Kolbe, L. Parent feeding behavior and child appetite: Associations depend on feeding style. Int. J. Eat. Disord. 2014, 47, 705–709. [Google Scholar] [CrossRef] [PubMed]
- Webber, L.; Hill, C.; Saxton, J.; Van Jaarsveld, C.H.M.; Wardle, J. Eating Behaviour and Weight in Children. Int. J. Obes. 2009, 33, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Viana, V.; Sinde, S.; Saxton, J.C. Children’s Eating Behaviour Questionnaire: Associations with BMI in Portuguese children. Br. J. Nutr. 2008, 100, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Carnell, S.; Wardle, J. Appetite and adiposity in children: Evidence for a behavioral susceptibility theory of obesity. Am. J. Clin. Nutr. 2008, 88, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Cooke, L.J.; Wardle, J. Age and gender differences in children’s food preferences. Br. J. Nutr. 2005, 93, 741–746. [Google Scholar] [CrossRef] [PubMed]
- Le Bigot Macaux, A. Eat to live or live to eat? Do parents and children agree? Public Health Nutr. 2001, 4, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Lien, N.; Lytle, L.A.; Klepp, K.I. Stability in consumption of fruit, vegetables, and sugary foods in a cohort from age 14 to age 21. Prev. Med. 2001, 33, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Haase, A.M.; Steptoe, A.; Nillapun, M.; Jonwutiwes, K.; Bellisle, F. Gender differences in food choice: The contribution of health beliefs and dieting. Ann. Behav. Med. 2004, 27, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Kulik, L. Like-Sex Versus Opposite-Sex Effects in Transmission of Gender Role Ideology from Parents to Adolescents in Israel. J. Youth Adolesc. 2002, 31, 451–457. [Google Scholar] [CrossRef]
- Flannery-Schroeder, E.C.; Chrisler, J.C. Body esteem, eating attitudes, and gender-role orientation in three age groups of children. Curr. Psychol. 1996, 15, 235–248. [Google Scholar] [CrossRef]
- Reinehr, T.; Kersting, M.; Chahda, C.; Andler, W. Nutritional knowledge of obese compared to non obese children. Nutr. Res. 2003, 23, 645–649. [Google Scholar] [CrossRef]
- Colavito, E.A.; Guthrie, J.F.; Hertzler, A.A.; Webb, R.E. Relationship of Diet-Health Attitudes and Nutrition Knowledge of Household Meal Planners to the Fat and Fiber Intakes of Meal Planners and Preschoolers. J. Nutr. Educ. 1996, 28, 321–328. [Google Scholar] [CrossRef]
- Shepherd, R.; Towler, G. Nutrition knowledge, attitudes and fat intake: Application of the theory of reasoned action. J. Hum. Nutr. Diet. 2007, 20, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Epstein, L.H.; Roemmich, J.N.; Raynor, H.A. Behavioral therapy in the treatment of pediatric obesity. Pediatr. Clin. N. Am. 2001, 48, 981–993. [Google Scholar] [CrossRef]
- Janssen, I.; Katzmarzyk, P.T.; Ross, R. Waist circumference and not body mass index explains obesity-related health risk. Am. J. Clin. Nutr. 2004, 79, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Tomiyama, A.J.; Hunger, J.M.; Nguyen-Cuu, J.; Wells, C. Misclassification of cardiometabolic health when using body mass index categories in NHANES 2005–2012. Int. J. Obes. 2016, 40, 883–886. [Google Scholar] [CrossRef] [PubMed]
- Sempolska, K.; Stupnicki, R. Relative fat content in young women with normal BMI but differing in the degree of physical activity. Rocz. Panstwowego Zakładu Hig. 2007, 58, 333–338. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Score Range | Min. | Max. | M | SD |
|---|---|---|---|---|---|
| Child’s % body fat | – | 13.10 | 51.60 | 22.11 | 4.94 |
| Mother’s % body fat | – | 8.40 | 61.40 | 31.46 | 8.94 |
| Father’s % body fat | – | 4.20 | 61.70 | 22.59 | 8.36 |
| Mother’s instrumental feeding style | 1–6 | 1.00 | 5.50 | 2.32 | 0.83 |
| Mother’s control over eating feeding style | 1–6 | 2.10 | 5.40 | 3.82 | 0.56 |
| Mother’s emotional feeding style | 1–6 | 1.00 | 5.60 | 2.11 | 0.86 |
| Mother’s encouragement feeding style | 1–6 | 1.38 | 6.00 | 4.26 | 0.57 |
| Father’s instrumental feeding style | 1–6 | 1.00 | 5.50 | 2.43 | 0.88 |
| Father’s control over eating feeding style | 1–6 | 1.50 | 6.00 | 3.72 | 0.59 |
| Father’s emotional feeding style | 1–6 | 1.00 | 5.00 | 2.20 | 0.79 |
| Father’s encouragement feeding style | 1–6 | 1.00 | 5.63 | 4.12 | 0.68 |
| Child’s nutrition knowledge | 0–90 | 36.67 | 85.17 | 71.03 | 9.27 |
| Child’s eating habits | 0–90 | 27.00 | 90.00 | 59.58 | 11.15 |
| Food responsiveness | 5–30 | 5.00 | 30.00 | 11.65 | 3.89 |
| Emotional overeating | 4–24 | 4.00 | 20.00 | 9.23 | 2.59 |
| Enjoyment of food | 4–24 | 4.00 | 24.00 | 14.03 | 3.44 |
| Desire to drink | 3–18 | 3.00 | 18.00 | 9.94 | 3.25 |
| Satiety responsiveness | 5–30 | 6.00 | 27.00 | 17.24 | 3.32 |
| Slowness in eating | 4–24 | 4.00 | 24.00 | 13.92 | 3.55 |
| Emotional undereating | 4–24 | 4.00 | 23.00 | 12.58 | 3.22 |
| Food fussiness | 6–36 | 8.00 | 36.00 | 22.36 | 5.82 |
| Participants | Healthy | Overfat | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | Min. | Max. | M | SD | n | Min. | Max. | M | SD | |
| Girls | 101 | 16.10 | 22.90 | 20.96 | 1.40 | 73 | 23.00 | 51.60 | 27.55 | 5.33 |
| Boys | 100 | 13.10 | 19.90 | 17.29 | 1.84 | 113 | 20.00 | 39.90 | 23.90 | 4.07 |
| Mothers | 190 | 8.40 | 32.40 | 25.50 | 5.20 | 125 | 33.00 | 61.60 | 40.27 | 5.60 |
| Fathers | 109 | 4.20 | 21.90 | 14.75 | 4.35 | 167 | 20.20 | 61.70 | 27.72 | 6.02 |
| Predictor | Unstandardized Coefficients | Standardized Coefficients (Beta) | t | p-Value | |
|---|---|---|---|---|---|
| B | Standard Error | ||||
| Girls | |||||
| Food responsiveness | 0.29 | 0.09 | 0.26 | 3.34 | 0.01 |
| Satiety responsiveness | −0.18 | 0.11 | −0.13 | −1.66 | 0.10 |
| Boys | |||||
| Emotional overeating | 0.32 | 0.14 | 0.17 | 2.34 | 0.02 |
| Emotional undereating | −0.23 | 0.11 | −0.15 | −2.06 | 0.04 |
| Child’s Sex | Child’s Body Fat Status | Parents’ Feeding Style | FR | EO | EF | DD | SR | SE | EU | FF |
|---|---|---|---|---|---|---|---|---|---|---|
| Girls | Healthy (n = 96) | Instrumental | 0.46 ** | 0.45 ** | 0.22 * | 0.14 | 0.01 | −0.03 | 0.08 | 0.03 |
| Control over eating | 0.47 ** | 0.46 ** | 0.27 ** | 0.04 | −0.12 | −0.05 | 0.04 | −0.14 | ||
| Emotional | −0.06 | −0.09 | −0.11 | −0.03 | 0.09 | 0.01 | −0.04 | 0.17 | ||
| Encouragement | 0.09 | 0.03 | 0.12 | 0.17 | 0.16 | 0.08 | 0.01 | 0.02 | ||
| Overfat (n = 65) | Instrumental | 0.10 | 0.13 | −0.07 | 0.17 | 0.16 | 0.09 | 0.33 ** | 0.21 | |
| Control over eating | 0.19 | 0.21 | −0.04 | 0.34 ** | 0.15 | 0.03 | 0.31 * | 0.16 | ||
| Emotional | −0.03 | −0.06 | 0.17 | −0.22 | −0.12 | −0.02 | 0.08 | 0.04 | ||
| Encouragement | −0.06 | −0.03 | 0.03 | 0.01 | 0.01 | 0.13 | 0.27 * | −0.07 | ||
| Boys | Healthy (n = 90) | Instrumental | 0.11 | 0.33 ** | −0.06 | 0.18 | 0.08 | 0.08 | 0.16 | 0.25 * |
| Control over eating | 0.17 | 0.32 ** | −0.02 | 0.34 ** | 0.07 | 0.09 | 0.10 | 0.28 ** | ||
| Emotional | 0.02 | −0.12 | −0.09 | −0.31 ** | 0.09 | 0.07 | 0.09 | 0.01 | ||
| Encouragement | −0.15 | −0.10 | −0.08 | −0.15 | 0.01 | 0.14 | 0.07 | 0.06 | ||
| Overfat (n = 105) | Instrumental | 0.24 * | 0.44 ** | 0.03 | 0.17 | 0.08 | 0.18 | 0.35 ** | 0.01 | |
| Control over eating | 0.25 ** | 0.46 ** | −0.01 | 0.16 | 0.02 | 0.13 | 0.28 ** | −0.05 | ||
| Emotional | −0.04 | −0.25 * | 0.01 | −0.02 | −0.02 | 0.02 | −0.19 | 0.06 | ||
| Encouragement | −0.08 | −0.11 | 0.15 | 0.10 | 0.03 | 0.07 | 0.20 * | −0.09 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lipowska, M.; Lipowski, M.; Jurek, P.; Jankowska, A.M.; Pawlicka, P. Gender and Body-Fat Status as Predictors of Parental Feeding Styles and Children’s Nutritional Knowledge, Eating Habits and Behaviours. Int. J. Environ. Res. Public Health 2018, 15, 852. https://doi.org/10.3390/ijerph15050852
Lipowska M, Lipowski M, Jurek P, Jankowska AM, Pawlicka P. Gender and Body-Fat Status as Predictors of Parental Feeding Styles and Children’s Nutritional Knowledge, Eating Habits and Behaviours. International Journal of Environmental Research and Public Health. 2018; 15(5):852. https://doi.org/10.3390/ijerph15050852
Chicago/Turabian StyleLipowska, Małgorzata, Mariusz Lipowski, Paweł Jurek, Anna M. Jankowska, and Paulina Pawlicka. 2018. "Gender and Body-Fat Status as Predictors of Parental Feeding Styles and Children’s Nutritional Knowledge, Eating Habits and Behaviours" International Journal of Environmental Research and Public Health 15, no. 5: 852. https://doi.org/10.3390/ijerph15050852
APA StyleLipowska, M., Lipowski, M., Jurek, P., Jankowska, A. M., & Pawlicka, P. (2018). Gender and Body-Fat Status as Predictors of Parental Feeding Styles and Children’s Nutritional Knowledge, Eating Habits and Behaviours. International Journal of Environmental Research and Public Health, 15(5), 852. https://doi.org/10.3390/ijerph15050852