Social, Environmental and Behavioral Determinants of Asthma Symptoms in Brazilian Middle School Students—A National School Health Survey (Pense 2012)

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Population and Data Collection
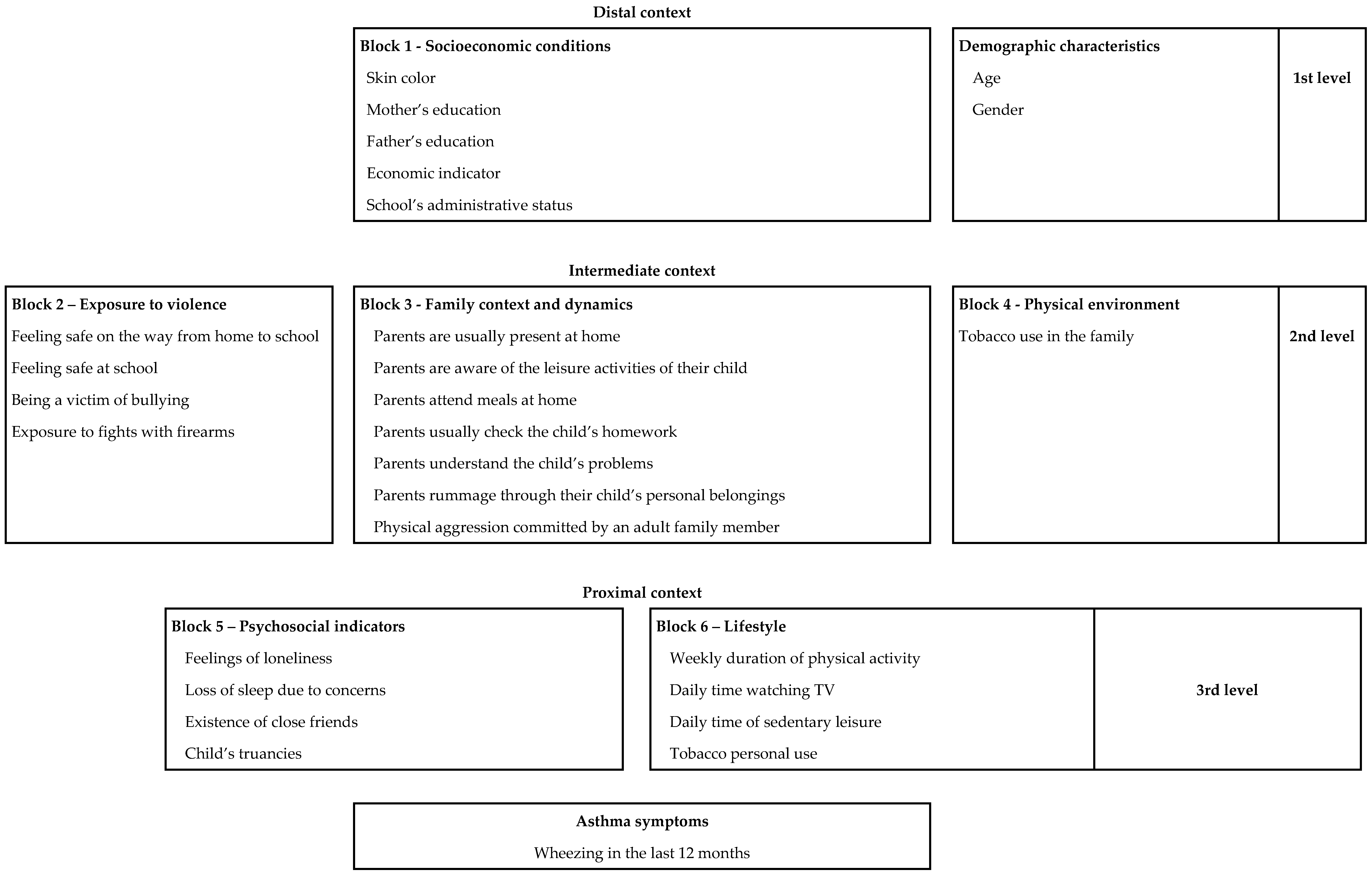
2.2. Measures
2.3. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lemanske, R.F., Jr.; Busse, W.W. Asthma: Clinical expression and molecular mechanisms. J. Allergy Clin. Immunol. 2010, 125 (Suppl. 2), S95–S102. [Google Scholar] [CrossRef]
- The Global Asthma Report 2014. Available online: http://www.globalasthmareport.org/resources/resources.php (accessed on 12 September 2017).
- Lai, C.; Beasley, R.; Crane, J.; Foliaki, S.; Shah, J.; Weiland, S. Global variation in the prevalence and severity of asthma symptoms: Phase three of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax 2009, 64, 476–483. [Google Scholar] [CrossRef]
- Menezes, A.M.; Wehrmeister, F.C.; Horta, B.; Szwarcwald, C.L.; Vieira, M.L.; Malta, D.C. Prevalence of asthma medical diagnosis among Brazilian adults: National Health Survey, 2013. Revista Brasileira de Epidemiologia 2015, 18 (Suppl. 2), 204–213. [Google Scholar] [CrossRef] [PubMed]
- Kuschnir, F.C.; Gurgel, R.Q.; Solé, D.; Costa, E.; Felix, M.M.; de Oliveira, C.L.; de Vasconcellos, M.T.; Kuschnir, M.C. ERICA: Prevalence of asthma in Brazilian adolescents. Revista de Saude Publica 2016, 50 (Suppl. 1), 13s. [Google Scholar] [CrossRef] [PubMed]
- Barreto, M.L.; Ribeiro-Silva Rde, C.; Malta, D.C.; Oliveira-Campos, M.; Andreazzi, M.A.; Cruz, A.A. Prevalence of asthma symptoms among adolescents in Brazil: National Adolescent School-based Health Survey (PeNSE 2012). Revista Brasileira de Epidemiologia 2014, 17 (Suppl. 1), 106–115. [Google Scholar] [CrossRef]
- Portal da Saúde. Indicadores e Dados Básicos; Ministério de Saúde: Brasília, Brazil, 2008. Available online: http://tabnet.datasus.gov.br (accessed on 12 September 2017).
- Cooper, P.J.; Chico, M.E.; Vaca, M.G.; Rodriguez, A.; Alcântara-Neves, N.M.; Genser, B.; de Carvalho, L.P.; Stein, R.T.; Cruz, A.A.; Rodrigues, L.C.; et al. Risk factors for asthma and allergy associated with urban migration: Background and methodology of a cross-sectional study in Afro-Ecuadorian school children in Northeastern Ecuador (Esmeraldas-SCAALA Study). BMC Pulm. Med. 2006, 6, 24. [Google Scholar] [CrossRef]
- Strina, A.; Barreto, M.L.; Cooper, P.J.; Rodrigues, L.C. Risk factors for non-atopic asthma/wheeze in children and adolescents: A systematic review. Emerg. Themes Epidemiol. 2014, 11, 5. [Google Scholar] [CrossRef] [PubMed]
- Kozyrskyj, A.L.; Kendall, G.E.; Jacoby, P.; Sly, P.D.; Zubrick, S.R. Association between socioeconomic status and the development of asthma: Analyses of income trajectories. Am. J. Public Health 2010, 100, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Silva Rde, C.; Assis, A.M.; Goncalves, M.S.; Fiaccone, R.L.; Matos, S.M.; Barreto, M.L.; Pinto Ede, J.; Silva, L.A.; Rodrigues, L.C.; Alcantara-Neves, N.M. The prevalence of wheezing and its association with body mass index and abdominal obesity in children. J. Asthma 2013, 50, 267–273. [Google Scholar] [CrossRef]
- Ribeiro-Silva Rde, C.; Oliveira-Assis, A.M.; Junqueira, S.B.; Fiaccone, R.L.; Dos Santos, S.M.; Barreto, M.L.; de Jesus Pinto, E.; da Silva, L.A.; Rodrigues, L.C.; Alcantara-Neves, N.M. Food and nutrition insecurity: A marker of vulnerability to asthma symptoms. Public Health Nutr. 2014, 17, 14–19. [Google Scholar] [CrossRef]
- Feitosa, C.A.; Santos, D.N.; Barreto do Carmo, M.B.; Santos, L.M.; Teles, C.A.; Rodrigues, L.C.; Barreto, M.L. Behavior problems and prevalence of asthma symptoms among Brazilian children. J. Psychosom. Res. 2011, 71, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Moncayo, A.L.; Vaca, M.; Oviedo, G.; Erazo, S.; Quinzo, I.; Fiaccone, R.L.; Chico, M.E.; Barreto, M.L.; Cooper, P.J. Risk factors for atopic and non-atopic asthma in a rural area of Ecuador. Thorax 2010, 65, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Rosas-Salazar, C.; Ramratnam, S.K.; Brehm, J.M.; Han, Y.Y.; Boutaoui, N.; Forno, E.; Acosta-Pérez, E.; Alvarez, M.; Colón-Semidey, A.; Canino, G.; et al. Prematurity, atopy, and childhood asthma in Puerto Ricans. J. Allergy Clin. Immunol. 2014, 133, 357–362. [Google Scholar] [CrossRef]
- Costa, R.D.; Figueiredo, C.A.; Barreto, M.L.; Alcantara-Neves, N.M.; Rodrigues, L.C.; Cruz, A.A.; Vergara, C.; Rafaels, N.; Foster, C.; Potee, J.; et al. Effect of polymorphisms on TGFB1 on allergic asthma and helminth infection in an African admixed population. Ann. Allergy Asthma Immunol. 2017, 118, 483–488.e1. [Google Scholar] [CrossRef] [PubMed]
- Leal, V.N.C.; Genov, I.R.; Mallozi, M.C.; Sole, D.; Pontillo, A. Polymorphisms in inflammasome genes and risk of asthma in Brazilian children. Mol. Immunol. 2018, 93, 64–67. [Google Scholar] [CrossRef]
- Beasley, R.; Semprini, A.; Mitchell, E.A. Risk factors for asthma: Is prevention possible? Lancet 2015, 386, 1075–1085. [Google Scholar] [CrossRef]
- Yonas, M.A.; Lange, N.E.; Celedon, J.C. Psychosocial stress and asthma morbidity. Curr. Opin. Allergy Clin. Immunol. 2012, 12, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Martikainen, P.; Bartley, M.; Lahelma, E. Psychosocial determinants of health in social epidemiology. Int. J. Epidemiol. 2002, 31, 1091–1093. [Google Scholar] [CrossRef]
- Wood, B.L.; Miller, B.D.; Lehman, H.K. Review of family relational stress and pediatric asthma: The value of biopsychosocial systemic models. Fam. Process 2015, 54, 376–389. [Google Scholar] [CrossRef]
- Rosenberg, S.L.; Miller, G.E.; Brehm, J.M.; Celedon, J.C. Stress and asthma: Novel insights on genetic, epigenetic, and immunologic mechanisms. J. Allergy Clin. Immunol. 2014, 134, 1009–1015. [Google Scholar] [CrossRef]
- Brehm, J.M.; Ramratnam, S.K.; Tse, S.M.; Croteau-Chonka, D.C.; Pino-Yanes, M.; Rosas-Salazar, C.; Litonjua, A.A.; Raby, B.A.; Boutaoui, N.; Han, Y.Y.; et al. Stress and Bronchodilator Response in Children with Asthma. Am. J. Respir. Crit. Care Med. 2015, 192, 47–56. [Google Scholar] [CrossRef]
- Brasil. Instituto Brasileiro de Geografia e Estatística. Pesquisa Nacional de Saúde Escolar (PeNSE)—2012. Rio de Janeiro (RJ): IBGE. 2012. Available online: http://portalsaude.saude.gov.br/portalsaude/arquivos/ pdf/2013/Jun/20/pense_2012_arquivo_web.pdf (accessed on 13 October 2017).
- Organização Mundial da Saúde. Social determinants of health and well-being among young people. In Health behaviour in School-Aged Children (HBSC) Study: International Report from the 2009/2010 Survey; WHO: Copenhagen, Denmark, 2012. [Google Scholar]
- Victora, C.G.; Huttly, S.R.; Fuchs, S.C.; Olinto, M.T. The role of conceptual frameworks in epidemiological analysis: A hierarchical approach. Int. J. Epidemiol. 1997, 26, 224–227. [Google Scholar] [CrossRef] [PubMed]
- Chong Neto, H.J.; Rosario, N.A.; Sole, D.; Latin American, I.G. Asthma and Rhinitis in South America: How Different They Are from Other Parts of the World. Allergy Asthma Immunol. Res. 2012, 4, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Cooper, P.J.; Rodrigues, L.C.; Barreto, M.L. Influence of poverty and infection on asthma in Latin America. Curr. Opin. Allergy Clin. Immunol. 2012, 12, 171–178. [Google Scholar] [CrossRef]
- Mejias, S.G.; Ramphul, K. Prevalence and Associated Risk Factors of Bronchial Asthma in Children in Santo Domingo, Dominican Republic. Cureus 2018, 10, E2211. [Google Scholar] [CrossRef] [PubMed]
- Ramratnam, S.K.; Han, Y.Y.; Rosas-Salazar, C.; Forno, E.; Brehm, J.M.; Rosser, F.; Marsland, A.L.; Colón-Semidey, A.; Alvarez, M.; Miller, G.E.; et al. Exposure to gun violence and asthma among children in Puerto Rico. Respir. Med. 2015, 109, 975–981. [Google Scholar] [CrossRef]
- Sternthal, M.J.; Jun, H.J.; Earls, F.; Wright, R.J. Community violence and urban childhood asthma: A multilevel analysis. Eur. Respir. J. 2010, 36, 1400–1409. [Google Scholar] [CrossRef]
- Alves Gda, C.; Santos, D.N.; Feitosa, C.A.; Barreto, M.L. Community violence and childhood asthma prevalence in peripheral neighborhoods in Salvador, Bahia State, Brazil. Cadernos de Saude Publica 2012, 28, 86–94. [Google Scholar] [CrossRef]
- Walker, J.; Lewis-Land, C.; Kub, J.; Tsoukleris, M.; Butz, A. The effect of violence on asthma: Are our children facing a double-edged sword? J. Community Health 2008, 33, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Priftis, K.N.; Chrousos, G.P. Neuroimmunomodulation in asthma: Focus on the hypothalamic-pituitary-adrenal axis. Neuroimmunomodulation 2009, 16, 263–264. [Google Scholar] [CrossRef] [PubMed]
- Jesenak, M.; Zelieskova, M.; Babusikova, E. Oxidative Stress and Bronchial Asthma in Children-Causes or Consequences? Front. Pediatr. 2017, 5, 162. [Google Scholar] [CrossRef] [PubMed]
- Wright, R.J.; Mitchell, H.; Visness, C.M.; Cohen, S.; Stout, J.; Evans, R.; Gold, D.R. Community violence and asthma morbidity: The Inner-City Asthma Study. Am. J. Public Health 2004, 94, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Apter, A.J.; Garcia, L.A.; Boyd, R.C.; Wang, X.; Bogen, D.K.; Ten Have, T. Exposure to community violence is associated with asthma hospitalizations and emergency department visits. J. Allergy Clin. Immunol. 2010, 126, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Arif, A.A.; Korgaonkar, P. The association of childhood asthma with mental health and developmental comorbidities in low-income families. J. Asthma 2016, 53, 277–281. [Google Scholar] [CrossRef]
- Alati, R.; O’Callaghan, M.; Najman, J.M.; Williams, G.M.; Bor, W.; Lawlor, D.A. Asthma and internalizing behavior problems in adolescence: A longitudinal study. Psychosom. Med. 2005, 67, 462–470. [Google Scholar] [CrossRef] [PubMed]
- McQuaid, E.L.; Kopel, S.J.; Nassau, J.H. Behavioral adjustment in children with asthma: A meta-analysis. J. Dev. Behav. Pediatr. 2001, 22, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Wright, R.J.; Rodriguez, M.; Cohen, S. Review of psychosocial stress and asthma: An integrated biopsychosocial approach. Thorax 1998, 53, 1066–1074. [Google Scholar] [CrossRef]
- Weil, C.M.; Wade, S.L.; Bauman, L.J.; Lynn, H.; Mitchell, H.; Lavigne, J. The relationship between psychosocial factors and asthma morbidity in inner-city children with asthma. Pediatrics 1999, 104, 1274–1280. [Google Scholar] [CrossRef]
- Vanker, A.; Gie, R.P.; Zar, H.J. The association between environmental tobacco smoke exposure and childhood respiratory disease: A review. Expert Rev. Respir. Med. 2017, 11, 661–673. [Google Scholar] [CrossRef]
- Gibbs, K.; Collaco, J.M.; McGrath-Morrow, S.A. Impact of Tobacco Smoke and Nicotine Exposure on Lung Development. Chest 2016, 149, 552–561. [Google Scholar] [CrossRef]
- Perret, J.L.; Bonevski, B.; McDonald, C.F.; Abramson, M.J. Smoking cessation strategies for patients with asthma: Improving patient outcomes. J. Asthma Allergy 2016, 9, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Sandberg, S.; Paton, J.Y.; Ahola, S.; McCann, D.C.; McGuinness, D.; Hillary, C.R.; Oja, H. The role of acute and chronic stress in asthma attacks in children. Lancet 2000, 356, 982–987. [Google Scholar] [CrossRef]
- Wandalsen, N.F.; Gonzalez, C.; Wandalsen, G.F.; Solé, D. Avaliação de critérios para o diagnóstico de asma através de um questionário epidemiológico. Jornal Brasileiro de Pneumologia 2009, 35, 199–205. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | n | % | Asthma Symptoms | |||||
|---|---|---|---|---|---|---|---|---|
| n | % 1 | 95% CI | PR 2 | 95% CI | p-Value | |||
| 109,104 | 25,038 | 22.7 | 21.5–23.9 | |||||
| DEMOGRAPHIC CHARACTERISTICS | ||||||||
| Gender | ||||||||
| Boys | 52,015 | 47.7 | 11,062 | 20.7 | 18.9–22.7 | |||
| Girls | 57,089 | 52.3 | 13976 | 24.4 | 23.3–25.4 | 1.17 | 1.08–1.27 | <0.001 |
| Age | ||||||||
| <14 years old | 22,443 | 20.6 | 5174 | 23.3 | 21.9–24.9 | |||
| 14 years | 50,900 | 46.7 | 11,834 | 23.1 | 21.9–24.4 | 1.00 | 0.96–1.04 | 0.10 |
| 15 years | 21,105 | 19.3 | 4769 | 22.2 | 20.9–23.6 | 0.97 | 0.93–1.01 | |
| 16 years or older | 14,656 | 13.4 | 3261 | 21.0 | 20.0–22.0 | 0.92 | 0.85–1.00 | |
| SOCIOECONOMIC CONDITIONS | ||||||||
| Self-referred skin color | ||||||||
| White | 37,674 | 34.6 | 8699 | 23.0 | 21.4–24.6 | |||
| Black | 14,513 | 13.3 | 3259 | 21.8 | 19.4–24.4 | 0.97 | 0.89–1.05 | 0.61 |
| Brown | 48,237 | 44.2 | 10,976 | 22.6 | 21.9–23.2 | 0.98 | 0.93–1.03 | |
| Others | 8611 | 7.9 | 2104 | 23.4 | 20.8–26.1 | 1.02 | 0.95–1.08 | |
| Mother’s education | ||||||||
| No education or primary education unfinished | 33,322 | 36.8 | 7522 | 22.4 | 21.7–23.2 | |||
| Primary education, or intermediate education unfinished | 15,975 | 17.6 | 3682 | 23.0 | 21.2–24.9 | 1.02 | 0.98–1.07 | <0.001 |
| Intermediate education, or higher education unfinished | 28,244 | 31.2 | 6769 | 23.7 | 22.3–25.2 | 1.09 | 1.05–1.13 | |
| Higher education | 13,036 | 14.4 | 3255 | 25.5 | 24.2–26.9 | 1.17 | 1.10 –1.25 | |
| Father’s education | ||||||||
| No education or primary education unfinished | 35,174 | 41.9 | 7982 | 22.4 | 21.1–23.8 | |||
| Primary education, or intermediate education unfinished | 14,114 | 16.8 | 3300 | 23.4 | 21.7–25.2 | 1.01 | 0.94–1.08 | <0.001 |
| Intermediate education, or higher education unfinished | 22,617 | 26.9 | 5366 | 23.4 | 21.3–25.7 | 1.06 | 0.96–1.16 | |
| Higher education | 12,119 | 14.4 | 3049 | 25.9 | 24.7–27.1 | 1.17 | 1.12–1.23 | |
| SES indicator | ||||||||
| 1st tertile + 2nd tertile (D + C class) | 50,430 | 64.4 | 5867 | 24.0 | 23.1–24.9 | |||
| 3rd tertile (B class) | 27,868 | 35.6 | 7048 | 25.1 | 23.2–27.1 | 1.16 | 1.10–1.23 | <0.001 |
| School’s administrative status | ||||||||
| Public | 86,599 | 79.4 | 19,495 | 22.3 | 21.1–23.5 | |||
| Private | 22,504 | 20.6 | 5543 | 25.0 | 24.1–26.0 | 1.12 | 1.05–1.19 | <0.001 |
| EXPOSURE TO VIOLENCE | ||||||||
| Feeling safe on the way from home to school | ||||||||
| Yes | 99,497 | 91.6 | 21,899 | 21.7 | 20.4–23.0 | |||
| No | 9150 | 8.4 | 3113 | 33.1 | 31.0–35.4 | 1.55 | 1.49–1.62 | <0.001 |
| Feeling safe at school | ||||||||
| Yes | 100,126 | 92.4 | 22,004 | 21.5 | 20.4–22.7 | |||
| No | 8187 | 7.6 | 2924 | 35.6 | 32.7–38.7 | 1.69 | 1.60–1.78 | <0.001 |
| Being victim of bullying | ||||||||
| Rarely/never | 101,310 | 93.4 | 22,612 | 21.9 | 20.7–23.2 | |||
| Frequently | 7193 | 6.6 | 2350 | 32.8 | 31.3–34.3 | 1.51 | 1.42–1.61 | <0.001 |
| Exposure to fights with firearms | ||||||||
| No | 96,771 | 89.3 | 20,912 | 21.2 | 20.0–22.5 | |||
| Yes | 11,648 | 10.7 | 4053 | 35.6 | 34.3–36.9 | 1.76 | 1.69–1.85 | <0.001 |
| FAMILY CONTEXT AND DYNAMICS | ||||||||
| Parents are frequently present at home | ||||||||
| Presence of mother and/or father | 101,845 | 93.5 | 23,221 | 22.5 | 21.2–23.8 | |||
| Absence of mother and father | 7065 | 6.5 | 1775 | 25.4 | 24.3–26.5 | 1.13 | 1.04–1.23 | 0.004 |
| Parents are aware of the leisure activities of their child | ||||||||
| Frequently | 63,916 | 58.9 | 13,815 | 21.3 | 20.3–22.4 | |||
| Rarely/never | 44,656 | 41.1 | 11,168 | 24.5 | 23.0–26.1 | 1.17 | 1.14–1.20 | <0.001 |
| Parents are present during meals | ||||||||
| Frequently | 76,929 | 70.7 | 16,790 | 21.4 | 20.3–22.5 | |||
| Rarely/never | 31,959 | 29.3 | 8237 | 25.9 | 24.3–27.6 | 1.20 | 1.15–1.25 | <0.001 |
| Parents check the child’s homework | ||||||||
| Frequently | 33,500 | 31.0 | 6661 | 19.4 | 18.0–20.9 | |||
| Rarely/never | 74,756 | 69.0 | 18,256 | 24.3 | 23.2–25.5 | 1.25 | 1.19–1.30 | <0.001 |
| Parents are understanding of the child’s problems | ||||||||
| Frequently | 47,895 | 44.1 | 9495 | 19.4 | 18.0–20.9 | |||
| Rarely/never | 60,674 | 55.9 | 15,492 | 25.4 | 24.4–26.5 | 1.31 | 1.26–1.36 | <0.001 |
| Main carers rummaging without permission through their child’s personal belongings | ||||||||
| Rarely/never | 91,579 | 84.4 | 20,569 | 22.1 | 20.9–23.3 | |||
| Frequently | 16,868 | 15.6 | 4393 | 25.9 | 24.3–27.6 | 1.18 | 1.13–1.22 | <0.001 |
| Physical aggression committed by an adult in the family | ||||||||
| No | 97,010 | 89.4 | 20,740 | 21.0 | 19.8–22.3 | |||
| Yes | 11,470 | 10.6 | 4233 | 36.8 | 34.9–38.7 | 1.73 | 1.67–1.80 | <0.001 |
| PHYSICAL ENVIRONMENT | ||||||||
| Tobacco use in the family | ||||||||
| None of the parents/guardians | 76,809 | 72.5 | 16,989 | 21.8 | 20.4–23.3 | |||
| At least one | 29,160 | 27.5 | 7317 | 24.6 | 23.7–25.4 | 1.12 | 1.07–1.18 | <0.001 |
| PSYCHOSOCIAL INDICATORS | ||||||||
| Feeling of loneliness | ||||||||
| Rarely/never | 90,204 | 83.2 | 19,051 | 20.7 | 19.6–21.9 | |||
| Frequently | 18,254 | 16.8 | 5972 | 32.4 | 30.6–34.3 | 1.53 | 1.48–1.59 | <0.001 |
| Loss of sleep due to concerns | ||||||||
| Rarely/never | 97,873 | 90.4 | 21,303 | 21.4 | 20.2–22.6 | |||
| Frequently | 10,447 | 9.6 | 3683 | 34.7 | 33.0–36.3 | 1.59 | 1.55–1.64 | <0.001 |
| Existence of close friends | ||||||||
| 3 or more friends | 87,401 | 80.6 | 19,304 | 21.7 | 20.4–23.0 | |||
| Less than 3 friends | 20,983 | 19.4 | 5707 | 26.8 | 25.5–28.2 | 1.23 | 1.18–1.28 | <0.001 |
| Child’s truancies | ||||||||
| Rarely/never | 105,722 | 97.2 | 23,961 | 22.3 | 21.1–23.6 | |||
| Frequently | 3092 | 2.8 | 1070 | 34.4 | 32.6–36.2 | 1.56 | 1.45–1.68 | <0.001 |
| LIFESTYLE | ||||||||
| Daily time of sedentary leisure | ||||||||
| ≤4 h a day | 67,733 | 62.3 | 14,427 | 20.9 | 19.6–22.1 | |||
| >4 h a day | 40,966 | 37.7 | 10,558 | 25.8 | 24.3–27.4 | 1.22 | 1.17–1.27 | <0.001 |
| TV watching | ||||||||
| ≤2 h a day | 41,120 | 37.8 | 8832 | 21.0 | 19.5–22.6 | |||
| >2 h a day | 67,672 | 62.2 | 16,178 | 23.6 | 22.5–24.8 | 1.11 | 1.06–1.16 | <0.001 |
| Tobacco use (ever in life, even one or two puffs) | ||||||||
| No | 86,113 | 79.1 | 17,979 | 20.6 | 19.3–21.9 | |||
| Yes | 22,784 | 20.9 | 7056 | 31.3 | 30.6–32.0 | 1.56 | 1.47–1.64 | <0.001 |
| n: Total 108,350, with Asthma Symptoms 25,038, 23.1% (Weighted % 22.7, 21.5–23.9) | PR 1 | 95% CI | p-Value | PR 2 | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| DEMOGRAPHIC CHARACTERISTICS | ||||||
| Gender | ||||||
| Boys | ||||||
| Girls | 1.17 | 1.08–1.27 | <0.001 | |||
| Age | ||||||
| <14 years | ||||||
| 14 years | 1.00 | 0.96–1.04 | 0.10 | |||
| 15 years | 0.97 | 0.93–1.01 | ||||
| >15 years | 0.92 | 0.85–1.00 | ||||
| SOCIOECONOMIC CONDITIONS 3 | ||||||
| SES indicator | ||||||
| 1st tertile + 2nd tertile (D + C class) | ||||||
| 3rd tertile (B class) | 1.15 | 1.09–1.22 | <0.001 | 1.15 | 1.09–1.22 | <0.001 |
| School’s administrative status | ||||||
| Public | ||||||
| Private | 1.07 | 1.00–1.13 | 0.037 | 1.07 | 1.00–1.13 | 0.037 |
| EXPOSURE TO VIOLENCE | ||||||
| Feeling safe on the way from home to school | ||||||
| Yes | ||||||
| No | 1.19 | 1.14–1.25 | <0.001 | 1.15 | 1.05–1.17 | <0.001 |
| Feeling safe at school | ||||||
| Yes | ||||||
| No | 1.37 | 1.30–1.45 | <0.001 | 1.29 | 1.18–1.30 | <0.001 |
| Being victim of bullying | ||||||
| Rarely/never | ||||||
| Frequently | 1.36 | 1.29–1.44 | <0.001 | 1.29 | 1.10–1.24 | <0.001 |
| Exposure to fights with firearms | ||||||
| No | ||||||
| Yes | 1.63 | 1.55–1.70 | <0.001 | 1.48 | 0.71–1.75 | <0.001 |
| FAMILY CONTEXT AND DYNAMICS | ||||||
| Parents are frequently present at home | ||||||
| Presence of mother and/or father | ||||||
| Absence of mother and father | 1.09 | 1.00–1.18 | 0.05 | |||
| Parents are aware of the leisure activities of their child | ||||||
| Frequently | ||||||
| Rarely/never | 1.04 | 1.00–1.09 | 0.05 | |||
| Parents are present during meals | ||||||
| Frequently | ||||||
| Rarely/never | 1.11 | 1.06–1.51 | <0.001 | 1.09 | 1.05–1.14 | <0.001 |
| Parents check the child’s homework | ||||||
| Frequently | ||||||
| Rarely/never | 1.13 | 1.08–1.19 | <0.001 | 1.13 | 1.08–1.18 | <0.001 |
| Parents are understanding of the child’s problems | ||||||
| Frequently | ||||||
| Rarely/never | 1.19 | 1.13–1.25 | <0.001 | 1.18 | 1.13–1.23 | <0.001 |
| Main carers rummaging without permission through their child’s personal belongings | ||||||
| Rarely/never | ||||||
| Frequently | 1.18 | 1.13–1.24 | <0.001 | 1.14 | 1.09–1.19 | <0.001 |
| Physical aggression committed by an adult in the family | ||||||
| No | ||||||
| Yes | 1.61 | 1.56–1.67 | <0.001 | 1.38 | 1.33–1.43 | <0.001 |
| PHYSICAL ENVIRONMENT | ||||||
| Tobacco use in family | ||||||
| No | ||||||
| Yes | 1.12 | 1.07–1.18 | <0.001 | 1.09 | 1.04–1.15 | 0.001 |
| PSYCHOLOGICAL ASPECTS | ||||||
| Feeling of loneliness | ||||||
| Rarely/never | ||||||
| Frequently | 1.38 | 1.33–1.43 | <0.001 | 1.23 | 1.18–1.27 | <0.001 |
| Loss of sleep due to concerns | ||||||
| Rarely/never | ||||||
| Frequently | 1.37 | 1.33–1.41 | <0.001 | 1.20 | 1.16–1.24 | <0.001 |
| Existence of close friends | ||||||
| 3 or more friends | ||||||
| Less than 3 friends | 1.15 | 1.10–1.19 | <0.001 | 1.09 | 1.05–1.13 | <0.001 |
| Child’s truancies | ||||||
| Rarely/never | ||||||
| Frequently | 1.45 | 1.34–1.57 | <0.001 | 1.09 | 1.02–1.18 | 0.009 |
| LIFESTYLE | ||||||
| Daily time of sedentary leisure | ||||||
| ≤4 h sitting watching TV etc./day | ||||||
| > 4 h sitting watching TV etc./day | 1.17 | 1.13–1.21 | <0.001 | 1.08 | 1.05–1.11 | <0.001 |
| Daily time of TV watching | ||||||
| ≤2 h/day | ||||||
| > 2 h/day | 1.04 | 1.00–1.08 | 0.048 | 1.04 | 1.01–1.08 | 0.015 |
| Tobacco personal use | ||||||
| No | ||||||
| Yes | 1.53 | 1.45–1.61 | <0.001 | 1.27 | 1.22–1.33 | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ribeiro-Silva, R.C.; Malta, D.C.; Rodrigues, L.C.; Ramos, D.O.; Fiaccone, R.L.; Machado, D.B.; Barreto, M.L. Social, Environmental and Behavioral Determinants of Asthma Symptoms in Brazilian Middle School Students—A National School Health Survey (Pense 2012). Int. J. Environ. Res. Public Health 2018, 15, 2904. https://doi.org/10.3390/ijerph15122904
Ribeiro-Silva RC, Malta DC, Rodrigues LC, Ramos DO, Fiaccone RL, Machado DB, Barreto ML. Social, Environmental and Behavioral Determinants of Asthma Symptoms in Brazilian Middle School Students—A National School Health Survey (Pense 2012). International Journal of Environmental Research and Public Health. 2018; 15(12):2904. https://doi.org/10.3390/ijerph15122904
Chicago/Turabian StyleRibeiro-Silva, Rita C., Deborah C. Malta, Laura C. Rodrigues, Dandara O. Ramos, Rosemeire L. Fiaccone, Daiane B. Machado, and Maurício L. Barreto. 2018. "Social, Environmental and Behavioral Determinants of Asthma Symptoms in Brazilian Middle School Students—A National School Health Survey (Pense 2012)" International Journal of Environmental Research and Public Health 15, no. 12: 2904. https://doi.org/10.3390/ijerph15122904
APA StyleRibeiro-Silva, R. C., Malta, D. C., Rodrigues, L. C., Ramos, D. O., Fiaccone, R. L., Machado, D. B., & Barreto, M. L. (2018). Social, Environmental and Behavioral Determinants of Asthma Symptoms in Brazilian Middle School Students—A National School Health Survey (Pense 2012). International Journal of Environmental Research and Public Health, 15(12), 2904. https://doi.org/10.3390/ijerph15122904