
Development of Activity and Participation Norms among General Adult Populations in Taiwan



 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Sampling Design and Participants
2.2. The Measurement of Activity and Participation Functioning
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Samples
3.2. Functioning Scores of the Weighted Sample
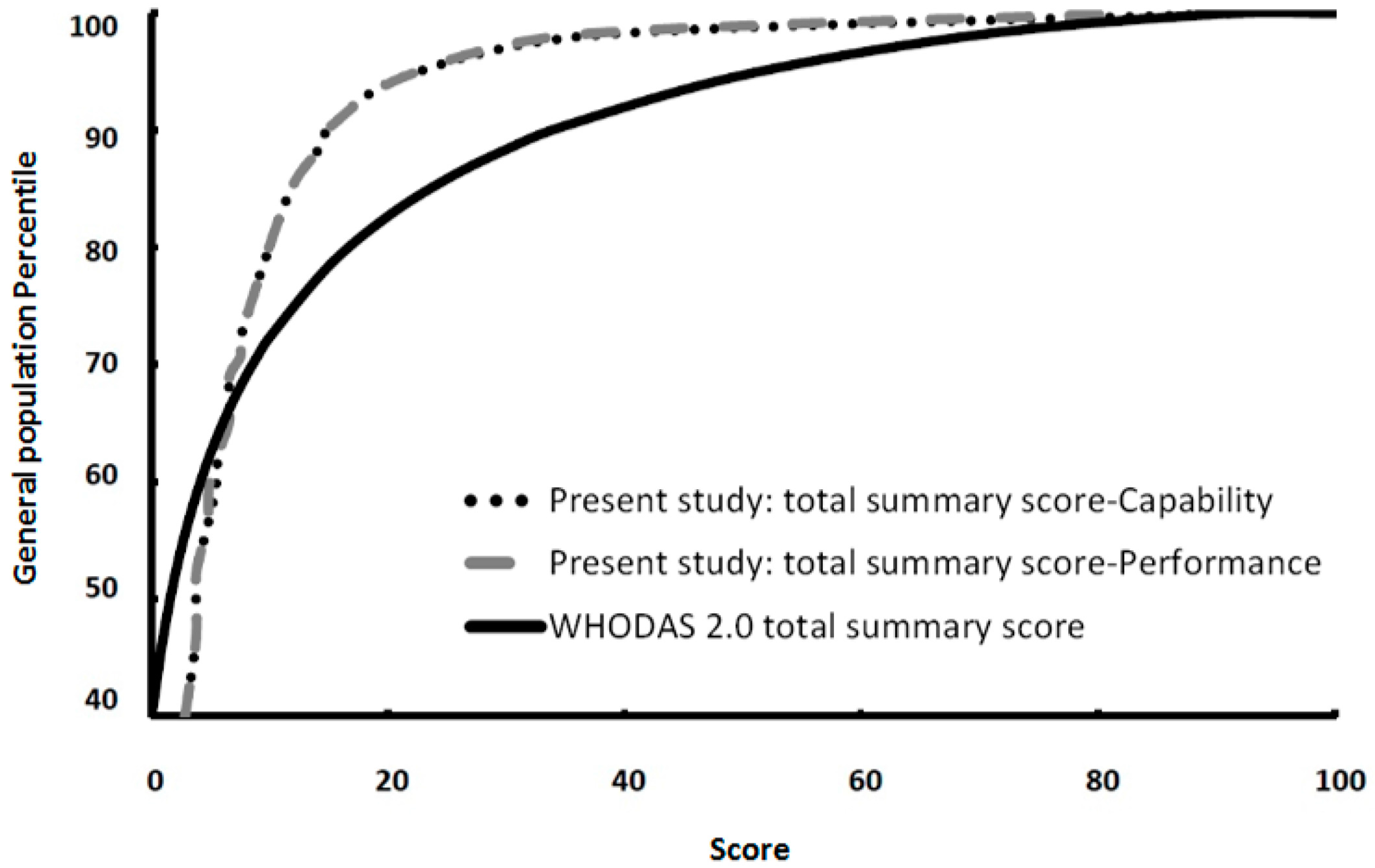
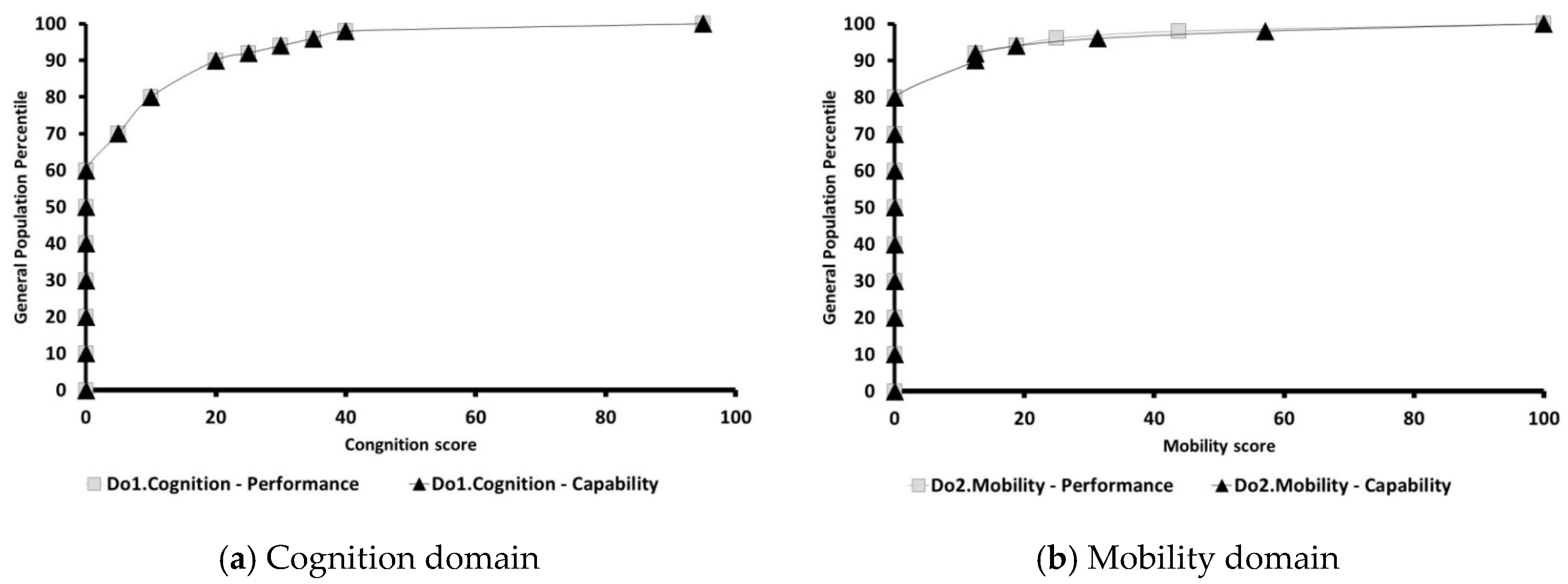
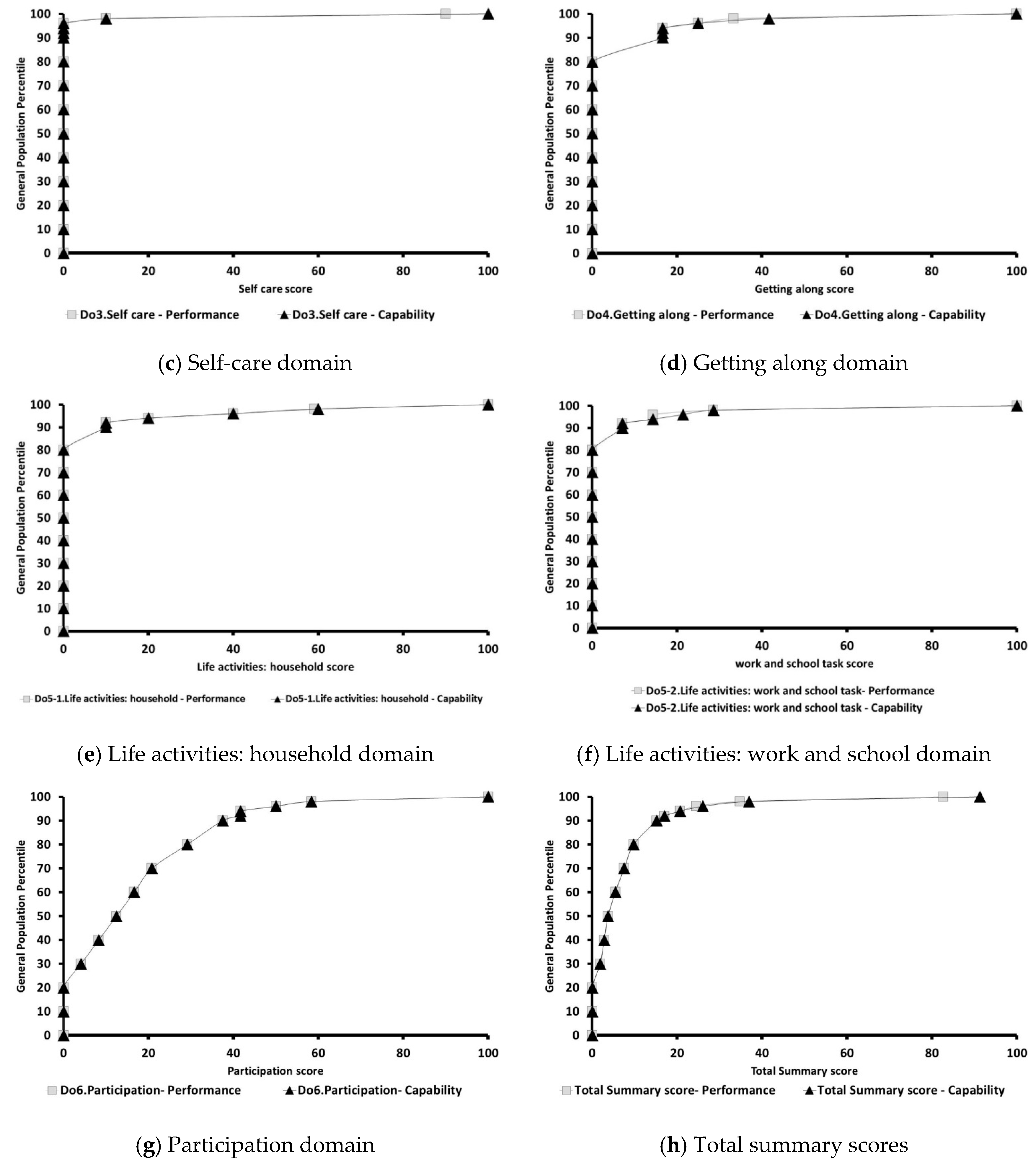
3.3. Activity and Participation Functioning Norms among the General Adult Population
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kessler, R.C.; Üstün, T.B. The WHO World Mental Health Surveys: Global Perspectives on the Epidemiology of Mental Disorders; Cambridge University Press: Cambridge, UK, 2008. [Google Scholar]
- Bickenbach, J.; Cieza, A.; Rauch, A.; Stucki, G. ICF Core Sets-Manual for Clinical Practice; Hogrefe: Göttingen, Germany, 2012. [Google Scholar]
- Lin, Y.-N.; Chang, K.-H.; Lin, C.-Y.; Hsu, M.-I.; Chen, H.-C.; Chen, H.-H.; Liou, T.-H. Developing comprehensive and Brief ICF core sets for morbid obesity for disability assessment in Taiwan: A preliminary study. Eur. J. Phys. Rehabil. Med. 2013, 49, 1–9. [Google Scholar]
- World Health Organization. International Classification of Functioning, Disability and Health (ICF); World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Fayed, N.; Camargo, O.K.D.; Elahi, I.; Dubey, A.; Fernandes, R.M.; Houtrow, A.; Cohen, E. Patient-important activity and participation outcomes in clinical trials involving children with chronic conditions. Qual. Life Res. 2014, 23, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, B.; Eggermont, L.; Soundy, A.; Probst, M.; Vandenbulcke, M.; Vancampfort, D. What are the factors associated with physical activity (PA) participation in community dwelling adults with dementia? A systematic review of PA correlates. Arch. Gerontol. Geriatr. 2014, 59, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Brage, S.; Donceel, P.; Falez, F. Working Group of the European Union of Medicine in Assurance and Social Security. Development of ICF core set for disability evaluation in social security. Disabil. Rehabil. 2008, 30, 1392–1396. [Google Scholar] [CrossRef] [PubMed]
- Sanches-Ferreira, M.; Simeonsson, R.; Silveira-Maia, M.; Alves, S.; Tavares, A.; Pinheiro, S. Portugal’s special education law: Implementing the International Classification of Functioning, Disability and Health in policy and practice. Disabil. Rehabil. 2013, 35, 868–873. [Google Scholar] [CrossRef] [PubMed]
- Liao, H.-F.; Yen, C.-F.; Hwang, A.-W.; Liou, T.-H.; Chang, B.-S.; Wu, T.-F.; Lu, S.-C.; Chi, W.-C.; Chang, K.-H. Introduction to the application of the Functioning Scale of the Disability Evaluation System. Formos. J. Med. 2013, 17, 368–380. [Google Scholar]
- Chiu, W.-T.; Yen, C.-F.; Teng, S.-W.; Liao, H.-F.; Chang, K.-H.; Chi, W.-C.; Wang, Y.-H.; Liou, T.-H. Implementing disability evaluation and welfare services based on the framework of the International Classification of Functioning, Disability and Health: Experiences in Taiwan. BMC Health Serv. Res. 2013, 13, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Teng, S.-W.; Yen, C.-F.; Liao, H.-F.; Chang, K.-H.; Chi, W.-C.; Wang, Y.-H.; Liou, T.-H. Evolution of system for disability assessment based on the ICF: A Taiwanese study. J. Formos. Med. Assoc. 2013, 112, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Liao, H.-F.; Yen, C.-F.; Hwang, A.-W.; Liou, T.-H.; Chi, W.-C. The Development and Application of the Functioning Disability Evaluation Scale. Community Dev. J. 2015, 105, 77–79. [Google Scholar]
- Chiu, T.-Y.; Yen, C.-F.; Chou, C.-H.; Lin, J.-D.; Hwang, A.-W.; Liao, H.-F.; Chi, W.-C. Development of traditional Chinese version of World Health Organization Disability Assessment Schedule 2.0 36-item (WHODAS 2.0) in Taiwan: Validity and reliability analyses. Res. Dev. Disabil. 2014, 35, 2812–2828. [Google Scholar] [CrossRef] [PubMed]
- Chi, W.-C.; Liou, T.-H.; Huang, W.W.-N.; Yen, C.-F.; Teng, S.-W.; Chang, I.-C. Developing a disability determination model using a decision support system in Taiwan: A pilot study. J. Formos. Med. Assoc. 2013, 112, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Directorate General of Budget, Accounting and Statistics (DGBAS). Available online: http://www.dgbas.gov.tw/public/data/dgbas04/bc6/census011(final).html (accessed on 12 June 2015).
- Dillman, D.A. Mail and Telephone Surveys: The Total Design Method; Wiley: New York, NY, USA, 1978. [Google Scholar]
- Üstün, T.B.; Chatterji, S.; Villanueva, M.; Bendib, L.; Çelik, C.; Sadana, R.; Salomon, J. WHO Multi-Country Survey Study on Health and Responsiveness 2001. Available online: http://www.who.int/healthinfo/survey/whspaper37.pdf (accessed on 4 November 2016).
- Yen, C.-F.; Hwang, A.-W.; Liou, T.-H.; Chiu, T.-Y.; Hsu, H.-Y.; Chi, W.-C.; Wu, T.-F.; Chang, B.-S.; Lu, S.-J.; Liao, H.-F.; et al. Validity and reliability of the Functioning Disability Evaluation Scale-Adult Version based on the WHODAS 2.0—36 items. J. Formos. Med. Assoc. 2014, 113, 839–849. [Google Scholar] [CrossRef] [PubMed]
- Üstün, T.B.; Kostanjsek, N.; Chatterji, S.; Rehm, J. Measuring Health and Disability: Manual for WHO Disability Assessment Schedule. WHODAS 2.0; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Liou, T.-H.; Wong, M.-K.; Chiou, H.-Y.; Chen, S.-C.; Liang, C.-C.; Wei, T.-S.; Huang, M.-H.; Yen, C.-F. The Plan of New Disability Evaluation System; Ministry of Health and Welfare: Taipei, Taiwan, 2014.
- Baumann, C.; Erpelding, M.-L.; Perret-Guillaume, C.; Gautier, A.; Régat, S.; Collin, J.-F.; Guillemin, F.; Brianço, S. Health-related quality of life in French adolescents and adults: Norms for the DUKE Health Profile. BMC Public Health 2011, 11, 401. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, L.N.; Ferreira, P.L.; Pereira, L.N.; Oppe, M. EQ-5D Portuguese population norms. Qual. Life Res. 2014, 23, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.; Hopman, W.; Sweet, J.; VanTil, L.; MacLean, M.B.; VanDenKerkhof, E.; Sudom, K.; Poirier, A.; Pedlar, D. Health-related quality of life of Canadian Forces veterans after transition to civilian life. Can. J. Public Health 2013, 104, 15–21. [Google Scholar]
- Maglinte, G.A.; Hays, R.D.; Kaplan, R.M. US general population norms for telephone administration of the SF-36v2. J. Clin. Epidemiol. 2012, 65, 497–502. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variable | Sample n = 1505 | Weighted Sample n = 1507 | Taiwan Adult Population n = 19,092,745 | Chi-Square Value (p-Value) | ||
|---|---|---|---|---|---|---|
| Gender | n | % | n | % | % | 0.014 (0.91) |
| Male | 583 | 38.7 | 748 | 49.7 | 49.5 | |
| Female | 922 | 61.3 | 758 | 50.3 | 50.5 | |
| Age (years) | 0.623 (1.00) | |||||
| 18–19 | 25 | 1.7 | 48 | 3.2 | 3.4 | |
| 20–29 | 150 | 10.1 | 258 | 17.3 | 17.2 | |
| 30–39 | 244 | 16.4 | 310 | 20.8 | 20.6 | |
| 40–49 | 297 | 20.0 | 288 | 19.4 | 19.3 | |
| 50–59 | 385 | 25.9 | 275 | 18.5 | 18.5 | |
| 60–64 | 166 | 11.2 | 106 | 7.1 | 7.1 | |
| 65–69 | 96 | 6.5 | 60 | 4.1 | 4.1 | |
| 70–74 | 67 | 4.5 | 54 | 3.6 | 3.6 | |
| 75–79 | 35 | 2.4 | 38 | 2.6 | 2.7 | |
| 80–84 | 15 | 1.0 | 27 | 1.8 | 2.0 | |
| ≥85 | 4 | 0.3 | 24 | 1.6 | 1.5 | |
| Area | 0.1 (1.00) | |||||
| Northern | 633 | 42.2 | 665 | 44.3 | 44.7 | |
| Central | 460 | 30.7 | 369 | 24.6 | 24.5 | |
| Southern | 363 | 24.2 | 414 | 27.6 | 27.4 | |
| Eastern | 35 | 2.4 | 37 | 2.4 | 2.4 | |
| Islands | 8 | 0.5 | 16 | 1.1 | 1 | |
| With Disability | 8.134 (0.004) | |||||
| Yes | 49 | 3.3 | 50 | 3.3 | 4.81 ψ | |
| No | 1456 | 96.7 | 1457 | 96.7 | 95.19 | |
| Variable | n | % |
|---|---|---|
| Marriage (n = 1506) | ||
| Married | 1024 | 68.0 |
| Single | 430 | 28.5 |
| Divorced | 15 | 1.0 |
| Separated | 18 | 1.2 |
| Widowed | 19 | 1.3 |
| Education (n = 1501) | ||
| Illiterate | 32 | 2.1 |
| Elementary | 138 | 9.2 |
| Junior high | 148 | 9.9 |
| Senior high | 408 | 27.2 |
| Junior college | 203 | 13.5 |
| University | 460 | 30.7 |
| Graduate school | 112 | 7.4 |
| Disability Type (n = 41) | ||
| Intellectual | 2 | 4.9 |
| Chronic psychosis | 10 | 24.4 |
| Epilepsy | 1 | 2.4 |
| Vision | 1 | 2.4 |
| Hearing | 2 | 4.9 |
| Balance | 2 | 4.9 |
| Loss of functions of primary organs | 4 | 9.8 |
| Physical | 19 | 46.3 |
| Severity of Disability (n = 46) | ||
| Mild | 16 | 33.6 |
| Moderate | 24 | 52.1 |
| Severe | 5 | 11.2 |
| Profound | 1 | 3.1 |
| Qualified by New Disability Eligibility System (n = 1507) | ||
| No | 1480 | 98.2 |
| Yes | 27 | 1.8 |
| Catastrophic Illness Card (n = 1505) | ||
| No | 1454 | 96.6 |
| Yes | 51 | 3.4 |
| Dimension and Domain | Domain Score Mean ± SD | Median | Range | Missing (%) |
|---|---|---|---|---|
| Performance Dimension (n = 1507) | ||||
| Do1. Cognition | 5.9 ± 11.6 | 0.0 | 0.0~95.0 | 0 |
| Do2. Mobility | 3.4 ± 10.7 | 0.0 | 0.0~100.0 | 0 |
| Do3. Self-care | 0.6 ± 4.7 | 0.0 | 0.0~90.0 | 0 |
| Do4. Getting along | 3.5 ± 9.8 | 0.0 | 0.0~100.0 | 0 |
| Do5-1. Household | 3.6 ± 13.4 | 0.0 | 0.0~100.0 | 0 |
| Do5-2. Work/ school task (n = 1017) | 1.9 ± 7.7 | 0.0 | 0.0~100.0 | 490 (32.5) |
| Do6. Participation | 15.2 ± 16.0 | 12.5 | 0.0~100.0 | 0 |
| Total Summary Score | 6.4 ± 8.6 | 3.8 | 0.0~82.6 | 490 (32.5) |
| Capability Dimension (n = 1507) | ||||
| Do1. Cognition | 5.9 ± 11.7 | 0.0 | 0.0~95.0 | 0 |
| Do2. Mobility | 4.0 ± 13.6 | 0.0 | 0.0~100.0 | 0 |
| Do3. Self-care | 0.9 ± 6.7 | 0.0 | 0.0~100.0 | 0 |
| Do4. Getting along | 3.8 ± 10.7 | 0.0 | 0.0~100.0 | 0 |
| Do5-1. Household | 4.1 ± 14.9 | 0.0 | 0.0~100.0 | 0 |
| Do5-2. Work/school task (n = 1017) | 2.1 ± 8.6 | 0.0 | 0.0~100.0 | 490 (32.5) |
| Do6. Participation | 15.5 ± 16.8 | 12.5 | 0.0~100.0 | 0 |
| Total Summary Score | 6.7 ± 10.0 | 3.8 | 0.0~91.3 | 490 (32.5) |
| Percentile | Present Study | People with Disabilities [20] | ||
|---|---|---|---|---|
| Performance | Capability | Performance | Capability | |
| 25 | 0.94 | 0.94 | 23.58 | 26.42 |
| 50 | 3.77 | 3.77 | 40.57 | 45.28 |
| 75 | 8.49 | 8.49 | 61.32 | 69.81 |
| Percentile | WHODAS 2.0 World Norm | Taiwan General Population | People with Disabilities in Taiwan [20] | ||
|---|---|---|---|---|---|
| Performance | Performance | Capability | Performance | Capability | |
| 40 | 0 | 2.8 | 2.8 | 33.7 | 37.7 |
| 46.83 | 1 | 3.8 | 3.8 | 38.0 | 42.5 |
| 52.08 | 2 | 3.8 | 3.8 | 41.5 | 47.2 |
| 56.2 | 3 | 4.7 | 4.7 | 44.6 | 50.9 |
| 59.58 | 4 | 4.9 | 5.4 | 47.2 | 53.8 |
| 62.46 | 5 | 5.7 | 5.7 | 50.0 | 56.6 |
| 64.94 | 6 | 6.5 | 6.5 | 51.9 | 59.4 |
| 67.12 | 7 | 6.6 | 6.6 | 53.8 | 61.3 |
| 69.05 | 8 | 6.6 | 6.6 | 55.7 | 63.2 |
| 70.78 | 9 | 7.5 | 7.5 | 57.5 | 65.2 |
| 72.35 | 10 | 7.5 | 7.5 | 58.7 | 67.4 |
| 78.42 | 15 | 9.4 | 9.4 | 65.2 | 74.5 |
| 82.66 | 20 | 10.9 | 10.9 | 70.8 | 80.2 |
| 85.85 | 25 | 12.3 | 12.3 | 75.5 | 84.8 |
| 88.35 | 30 | 14.1 | 14.1 | 79.2 | 87.7 |
| 90.38 | 35 | 15.2 | 15.2 | 83.0 | 90.6 |
| 94.69 | 50 | 21.7 | 21.7 | 91.3 | 96.2 |
| 98.14 | 70 | 35.9 | 38 | 99.1 | 100.0 |
| 99.9 | 90 | 81 | 90.8 | 100.0 | 100.0 |
| 100 | 100 | 82.6 | 91.3 | 100.0 | 100.0 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yen, C.-F.; Chiu, T.-Y.; Liou, T.-H.; Chi, W.-C.; Liao, H.-F.; Liang, C.-C.; Escorpizo, R. Development of Activity and Participation Norms among General Adult Populations in Taiwan. Int. J. Environ. Res. Public Health 2017, 14, 603. https://doi.org/10.3390/ijerph14060603
Yen C-F, Chiu T-Y, Liou T-H, Chi W-C, Liao H-F, Liang C-C, Escorpizo R. Development of Activity and Participation Norms among General Adult Populations in Taiwan. International Journal of Environmental Research and Public Health. 2017; 14(6):603. https://doi.org/10.3390/ijerph14060603
Chicago/Turabian StyleYen, Chia-Feng, Tzu-Ying Chiu, Tsan-Hon Liou, Wen-Chou Chi, Hua-Fang Liao, Chung-Chao Liang, and Reuben Escorpizo. 2017. "Development of Activity and Participation Norms among General Adult Populations in Taiwan" International Journal of Environmental Research and Public Health 14, no. 6: 603. https://doi.org/10.3390/ijerph14060603
APA StyleYen, C.-F., Chiu, T.-Y., Liou, T.-H., Chi, W.-C., Liao, H.-F., Liang, C.-C., & Escorpizo, R. (2017). Development of Activity and Participation Norms among General Adult Populations in Taiwan. International Journal of Environmental Research and Public Health, 14(6), 603. https://doi.org/10.3390/ijerph14060603