
Clinical Prediction of Suicide and Undetermined Death: A Pseudo-Prospective Clinical and Medico-Legal Study of Substance Abusers

Abstract
:1. Introduction
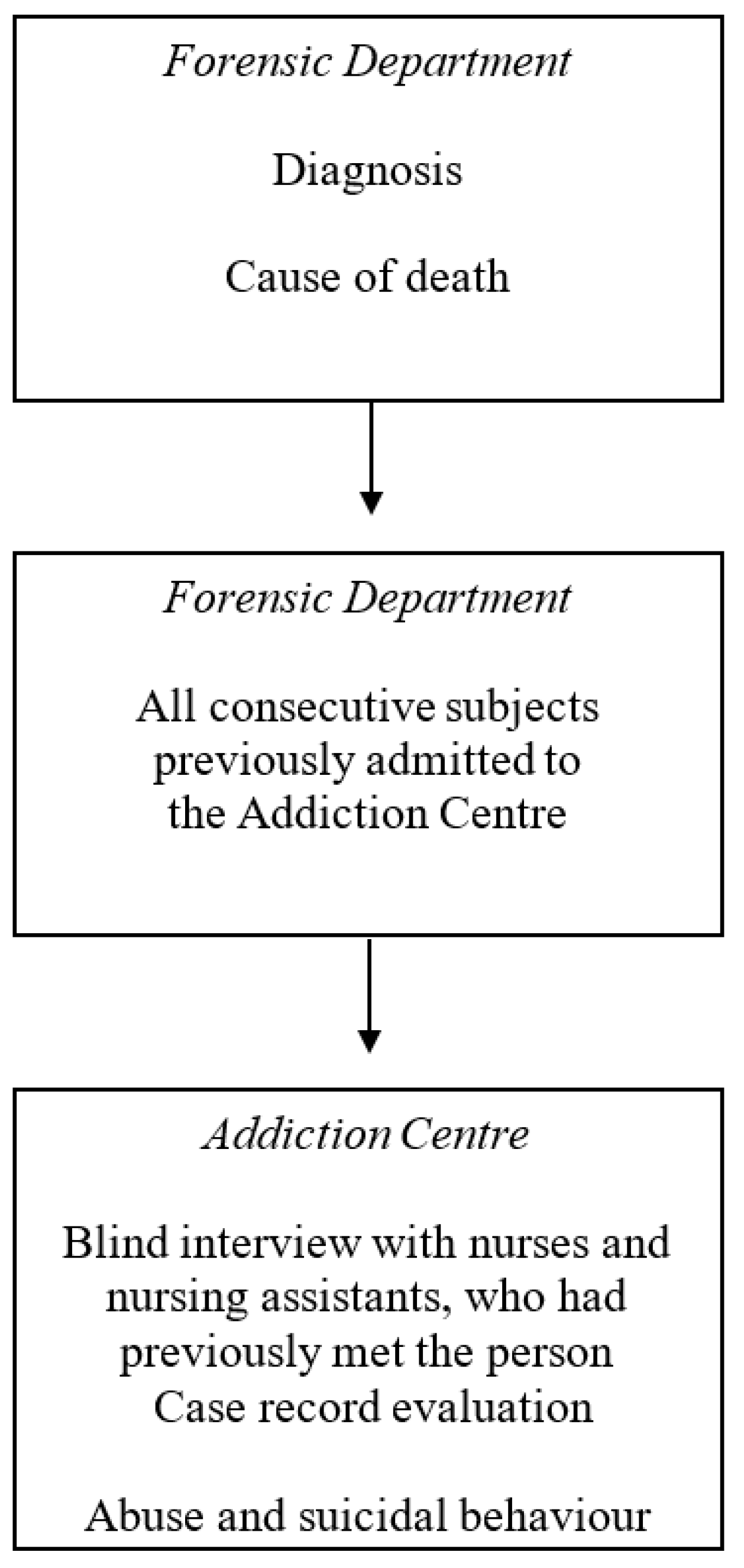
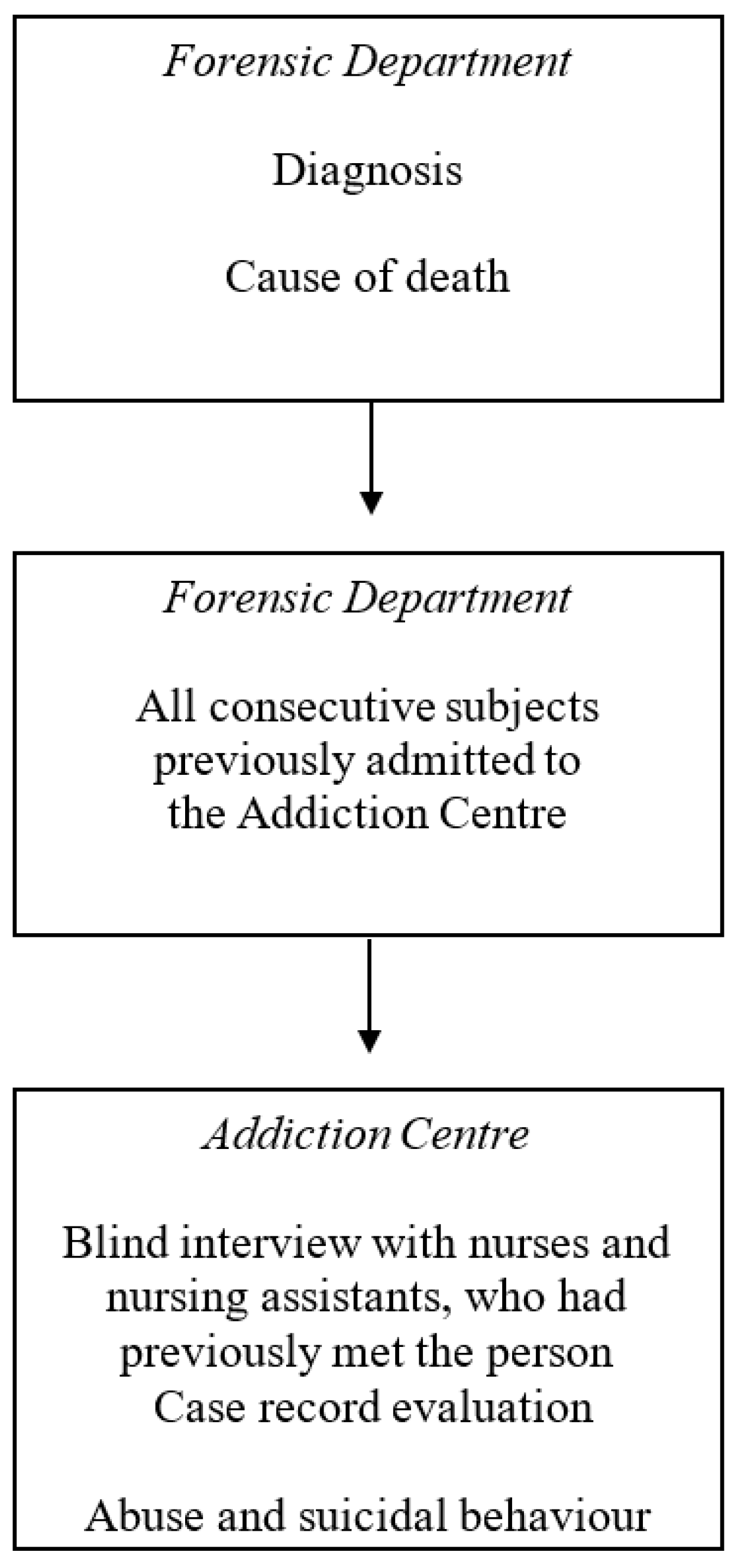
2. Material and Methods
2.1. Statistics
2.2. Ethical Considerations
3. Results
3.1. Staff Judgement
3.1.1. Suicide versus Non-Suicide
3.1.2. Suicide and Undetermined Intent versus Other Manners of Death
3.2. Suicidal Behaviour Reported in the Case Records Related to Suicide and Undetermined Death
3.3. Toxicological Autopsy Findings
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization 2016. Available online: http://www.who.int/mental_health/prevention/suicide/suicideprevent/en/ (accessed on 30 January 2017).
- Beck, AT.; Kovacs, M.; Weissman, A. Assessment of suicidal intention: The Scale for Suicide Ideation. J. Consult. Clin. Psychol. 1979, 47, 343–352. [Google Scholar] [CrossRef] [PubMed]
- Beck, R.W.; Morris, J.B.; Beck, A.T. Cross-validation of the Suicidal Intent Scale. Psychol. Rep. 1974, 34, 445–446. [Google Scholar] [CrossRef] [PubMed]
- Patterson, W.M.; Dohn, H.H.; Bird, J.; Patterson, G.A. Evaluation of suicidal patients: The SAD PERSONS scale. Psychosomatics 1983, 24, 343–349. [Google Scholar] [CrossRef]
- Swedish Council on Health Technology Assessment (SBU). Instrument för Bedömning av Suicidrisk. En Systematisk Litteraturöversikt; SBU-Rapport Nr 242; Statens Beredning för Medicinsk Och Social Utvärdering: Stockholm, Sweden, 2015. (In Swedish) [Google Scholar]
- Arsenault-Lapierre, G.; Kim, C.; Turecki, G. Psychiatric diagnoses in 3275 suicides: A meta-analysis. BMC Psychiatry 2004, 4, 37. [Google Scholar] [CrossRef] [PubMed]
- Bertolote, J.M.; Fleischmann, A.; De Leo, D.; Wasserman, D. Psychiatric diagnoses and suicide: Revisiting the evidence. Crisis 2004, 25, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Brådvik, L.; Mattisson, C.; Bogren, M.; Nettelbladt, P. Mental disorders in suicide and undetermined death in the Lundby study. The contribution of severe depression and alcohol dependence. Arch. Suicide Res. 2010, 14, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, A.E.; Larsen, G.Y.; Fullerton-Gleason, L.; Olsson, L.M. Classifying undetermined poisoning deaths. Inj. Prev. 2006, 12, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Björkenstam, C.; Johansson, L.-A.; Nordström, P.; Thiblin, I.; Fugelstad, A.; Hallqvist, J.; Ljung, R. Suicide or undetermined intent? A register-based study of signs of misclassification. Popul. Health Metr. 2014, 12, 11. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; Bergen, H.; Simkin, S.; Dodd, S.; Pocock, P.; Bernal, W.; Gunnell, D.; Kapur, N. Long term effect of reduced pack sizes of paracetamol in poisoning deaths and liver transplant activity in England and Wales: Interrupted time series analyses. BMJ 2013, 346, f403. [Google Scholar] [CrossRef] [PubMed]
- Runeson, B.; Tidemalm, D.; Dahlin, M.; Lichtenstein, P.; Långström, N. Method of attempted suicide as predictor of subsequent successful suicide: National long term cohort study. BMJ 2010, 340, c3222. [Google Scholar] [CrossRef] [PubMed]
- Evenson, R.C.; Cho, D.W.; Holland, R. Identifying psychiatric suicides for research purposes. J. Clin. Psychol. 1988, 44, 1029–1032. [Google Scholar] [CrossRef]
- Gray, D.; Coon, H.; McGlade, E.; Callor, W.B.; Byrd, J.; Viskochil, J.; Bakian, A.; Yurgelun-Todd, D.; Grey, T.; McMahon, W.M. Comparative analysis of suicide, accidental, and undetermined cause of death classification. Suicide Life-Threat. Behav. 2014, 44, 304–316. [Google Scholar] [CrossRef] [PubMed]
- Linsley, K.R.; Schapira, K.; Kelly, T.P. Open verdict v. suicide—Importance to research. Br. J. Psychiatry 2001, 178, 465–468. [Google Scholar] [CrossRef] [PubMed]
- Olsson, M.O.; Brådvik, L.; Öjehagen, A.; Håkansson, A. Risk factors for unnatural death; Fatal accidental intoxication, undetermined intent and suicide: Register follow-up in a criminal justice population with substance use problems. Drug Alcohol Depend. 2016, 162, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Inskip, H.M.; Harris, E.C.; Barraclough, B. Lifetime risk of suicide for affective disorder, alcoholism, and schizophrenia. Br. J. Psychiatry 1998, 172, 35–37. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, H.C.; Conner, K.R.; Caine, E.D. Association of alcohol and drug use disorders and completed suicide: An empirical review of cohort studies. Drug Alcohol Depend. 2004, 76, S11–S19. [Google Scholar] [CrossRef] [PubMed]
- Darvishi, N.; Farhadi, M.; Haghtalab, T.; Poorolajal, J. Alcohol-related risk of suicidal ideation, suicide attempt, and completed suicide: A meta-analysis. PLoS ONE 2015, 20, e0126870. [Google Scholar] [CrossRef] [PubMed]
- Rossow, I.; Romelsjö, A.; Leifman, H. Alcohol abuse and suicidal behaviour in young and middle aged men: Differentiating between attempted and completed suicide. Addiction 1999, 94, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Suokas, J.; Lönnqvist, J. Suicide attempts in which alcohol is involved: A special group in general hospital emergency rooms. Acta Psychiatr. Scand. 1995, 91, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, A.S.; Stenager, E.; Brahe, U.B. Attempted suicide, suicidal intent, and alcohol. Crisis 1993, 14, 32–38. [Google Scholar] [PubMed]
- Haw, C.; Casey, D.; Holmes, J.; Hawton, K. Suicidal Intent and Method of Self-Harm: A Large-scale Study of Self-Harm Patients Presenting to a General Hospital. Suicide Life-Threat. Behav. 2015, 45, 732–746. [Google Scholar] [CrossRef] [PubMed]
- Ghanbari, B.; Malakouti, S.K.; Nojomi, M.; De Leo, D.; Saeed, K. Alcohol Abuse and Suicide Attempt in Iran: A Case-Crossover Study. Glob. J. Health Sci. 2015, 3, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, D.B.; Terra, M.G.; Soccol, K.L.; Schneider, J.F.; Camillo, L.A.; Plein, F.A. Reasons for attempting suicide among men who use alcohol and other drugs. Rev. Gauch. Enferm. 2016, 37, e54896. [Google Scholar]
- Bryan, C.J.; Garland, E.L.; Rudd, M.D. From impulse to action among military personnel hospitalized for suicide risk: Alcohol consumption and the reported transition from suicidal thought to behavior. Gen. Hosp. Psychiatry 2016, 41, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Berglund, M.; Krantz, P.; Lundqvist, G. Suicide in alcoholism: A prospective study of 55 cases with autopsy findings. Acta Psychiatr. Scand. 1987, 76, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Borges, G.; Cherpitel, C.J.; Orozco, R.; Ye, Y.; Monteiro, M.; Hao, W.; Benegal, V. A dose-response estimate for acute alcohol use and risk of suicide attempt. Addict. Biol. 2016, 10. [Google Scholar] [CrossRef] [PubMed]
- Brådvik, L.; Berglund, M.; Frank, A.; Lindgren, A.; Löwenhielm, P. Number of addictive substances used related to increased risk for unnatural death: A combined medico-legal and case-record study. BMC Psychiatry 2009, 9, 48. [Google Scholar] [CrossRef] [PubMed]
- International Stastistical Classification of Disease ICD 9; Center for Disease Control and Prevention, National Center for Health Statistics: Hyattsville, MD, USA, 1977. (In Swedish)
- International Stastistical Classification of Disease ICD 10; Center for Disease Control and Prevention, National Center for Health Statistics: Hyattsville, MD, USA, 1997. (In Swedish)
- Large, M.; Smith, G.; Sharma, S.; Nielssen, O.; Singh, S.P. Systematic review and meta-analysis of the clinical factors associated with the suicide of psychiatric in-patients. Acta Psychiatr. Scand. 2011, 124, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Goldston, D.B.; Reboussin, B.A.; Daniel, S.S. Predictors of suicide attempts: State and trait components. J. Abnorm. Psychol. 2006, 115, 842–849. [Google Scholar] [CrossRef] [PubMed]
- Ringel, E. Selbstmordverhütung; Verlag Hans Huber: Bern, Switzerland; Stuttgart, Germany; Vienna, Austria, 1969. (In German) [Google Scholar]
- Crona, L.; Stenmarker, M.; Öjehagen, A.; Asklund, U.; Brådvik, L. Taking care of oneself by regaining control—A key to staying alive four to five decades after a suicide attempt in severe depression. BMC Psychiatry 2017, 17, 69. [Google Scholar] [CrossRef] [PubMed]
- Sjögren, H.; Eriksson, A.; Ahlm, K. Role of alcohol in unnatural deaths: A study of all deaths in Sweden. Alcohol.: Clin. Exp. Res. 2000, 24, 1050–1056. [Google Scholar] [CrossRef]
- Ohberg, A.; Lonnqvist, J. Suicides hidden among undetermined deaths. Acta Psychiatr. Scand. 1998, 98, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Bergen, H.; Hawton, K.; Kapur, N.; Cooper, J.; Steeg, S.; Ness, J.; Waters, K. Shared characteristics of suicides and other unnatural deaths following non-fatal self-harm? A multicentre study of risk factors. Psychol. Med. 2012, 42, 727–741. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Time | All Patients | Patients Remembered |
|---|---|---|
| <3 months | 98 | 64 (65) |
| <1 year | 86 | 43 (50) |
| <5 years | 106 | 37 (35) |
| <10 years | 44 | 11 (25) |
| >10 years | 51 | 2 (4) |
| Total | 385 | 157 (41) |
| Manner of Death | <3 Months | 1 Year | 5 Years | 5–10 Years | >10 Years |
|---|---|---|---|---|---|
| Suicide | 12 (27) | 13 (29) | 5 (11) | 8 (18) | 6 (13) |
| Undetermined | 27 (30) | 20 (22) | 21 (23) | 16 (18) | 7 (8) |
| Other | 59 (23) | 53 (21) | 80 (32) | 20 (8) | 42 (17) |
| Total | 98 (25) | 86 (22) | 106 (28) | 44 (11) | 51 (13) |
| Manner of Death | No | Intent Not Considered Serious | Yes | Total |
|---|---|---|---|---|
| Suicide | 11 | 0 | 9 | 20 |
| Undetermined death | 30 | 8 * | 9 | 47 |
| Other | 84 | 4 | 2 | 90 |
| Total | 125 | 12 | 20 | 157 |
| Manner of Death | Suicidal Ideation | Suicide Attempt | Total |
|---|---|---|---|
| Suicide | 16 (36%) | 15 (33%) | 45 |
| Undetermined death | 24 (26%) | 17 (18%) | 91 |
| Other manners of death | 30 (12%) | 42 (17%) | 252 |
| Total | 70 (18%) | 74 (19%) | 388 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brådvik, L.; Berglund, M.; Frank, A.; Löwenhielm, P. Clinical Prediction of Suicide and Undetermined Death: A Pseudo-Prospective Clinical and Medico-Legal Study of Substance Abusers. Int. J. Environ. Res. Public Health 2017, 14, 310. https://doi.org/10.3390/ijerph14030310
Brådvik L, Berglund M, Frank A, Löwenhielm P. Clinical Prediction of Suicide and Undetermined Death: A Pseudo-Prospective Clinical and Medico-Legal Study of Substance Abusers. International Journal of Environmental Research and Public Health. 2017; 14(3):310. https://doi.org/10.3390/ijerph14030310
Chicago/Turabian StyleBrådvik, Louise, Mats Berglund, Arne Frank, and Peter Löwenhielm. 2017. "Clinical Prediction of Suicide and Undetermined Death: A Pseudo-Prospective Clinical and Medico-Legal Study of Substance Abusers" International Journal of Environmental Research and Public Health 14, no. 3: 310. https://doi.org/10.3390/ijerph14030310
APA StyleBrådvik, L., Berglund, M., Frank, A., & Löwenhielm, P. (2017). Clinical Prediction of Suicide and Undetermined Death: A Pseudo-Prospective Clinical and Medico-Legal Study of Substance Abusers. International Journal of Environmental Research and Public Health, 14(3), 310. https://doi.org/10.3390/ijerph14030310