1. Introduction
The Fédération Internationale de Football (FIFA) estimates that there are over 22 million youth soccer players globally [
1], and the frequency of injury in this population represents a significant public health burden. Estimated injury rates in youth soccer range from 3.4–5.6 injuries/1000 participation hours, or 22.0–30.0 injuries/100 participants/year [
2,
3,
4]. These are characterized by a high proportion of lower extremity injuries, with the majority being to the ankle and knee joints [
2,
3,
4,
5,
6,
7,
8,
9]. Aside from their immediate impact on individual health, there is evidence that joint injuries result in an increased risk of early osteoarthritis development [
10,
11,
12] and may have lasting impacts on physical activity participation and health-related quality of life [
12]. Implementing successful injury prevention strategies in this population is, therefore, critical in reducing health care costs and decreasing risks for disability and inactivity through adulthood.
Exercise-based prevention programs are efficacious at reducing sport injury risk [
13,
14,
15,
16]. Neuromuscular training programs, in particular, have demonstrated significant lower extremity injury reductions in youth sport (incidence rate ratio (IRR) = 0.6; 95% confidence interval (CI): 0.5, 0.8) [
15,
17]. The FIFA 11+ is a neuromuscular training program designed specifically to reduce lower extremity injuries in amateur soccer, and in randomized trials has produced significant risk reductions of 32.0%–56.0% [
18,
19,
20]. Previous studies, however, have reported only moderate adherence to the FIFA 11+ and, despite its efficacy, there has been limited uptake of the program in the soccer community [
21]. This reflects many degrees of influence for program implementation including the broader sport culture as well as institutional/organizational, team, and individual levels. Although the most effective driver for implementation may come from institutional change [
21], this process often takes significant time and resources and there remains the challenge of modifying individual behavior in the absence of enforced program use. Effecting change at this level relies on an understanding of the determinants of program uptake in the target population, including barriers and facilitators to its use in context.
A number of barriers to FIFA 11+ use have been identified amongst youth soccer players and their coaches, including low expectation that prevention strategies are effective and having insufficient time or resources to implement the program [
22]. Notably, promotion strategies for prevention programs often rely on communicating injury risk information to the target audience. In youth soccer, however, knowledge of injury rates and perceptions about whether injuries are preventable have demonstrated poor associations with program uptake [
23]. Furthermore, factors such as personal injury history, which should provide realistic risk perceptions, have not been supported as adherence predictors [
23]. Such counterintuitive findings may be related to the absence of an underlying behavioral theory in the majority of existing research. Cataloguing perceptions and potential barriers without establishing how they interact with cognitive processes to produce behavioral intentions and actions limits our understanding of program adoption in the soccer community.
Prevention program delivery must also be considered when evaluating adherence. In both research and practical settings, emphasis has been placed on providing injury prevention content to coaches who can then disseminate information to players. This has been moderately successful [
18,
19], but results of a recent study investigating different FIFA 11+ delivery strategies suggest that program adherence increases by 8.0%–12.0% when coaches are given comprehensive, workshop-style instruction instead of simply providing program resources [
20]. Understanding the underlying determinants of behavior change may help to explain this finding and better inform the content of coach workshops to promote greater program uptake and maintenance in the face of identified barriers to program use.
Behavior change theory has seen limited application in sport injury research [
24,
25]. In a systematic review, McGlashan and Finch report that only 11.0% of prevention studies included explicit application of a behavioral or social science theory, and only four of 11 total papers formally tested a theory-driven hypothesis [
24]. A number of common behavior change theories were notably absent from the literature. Given the limited success in promoting prevention program uptake in sport settings, there is considerable scope for additional work in this area to facilitate behavior change at individual and team levels [
24].
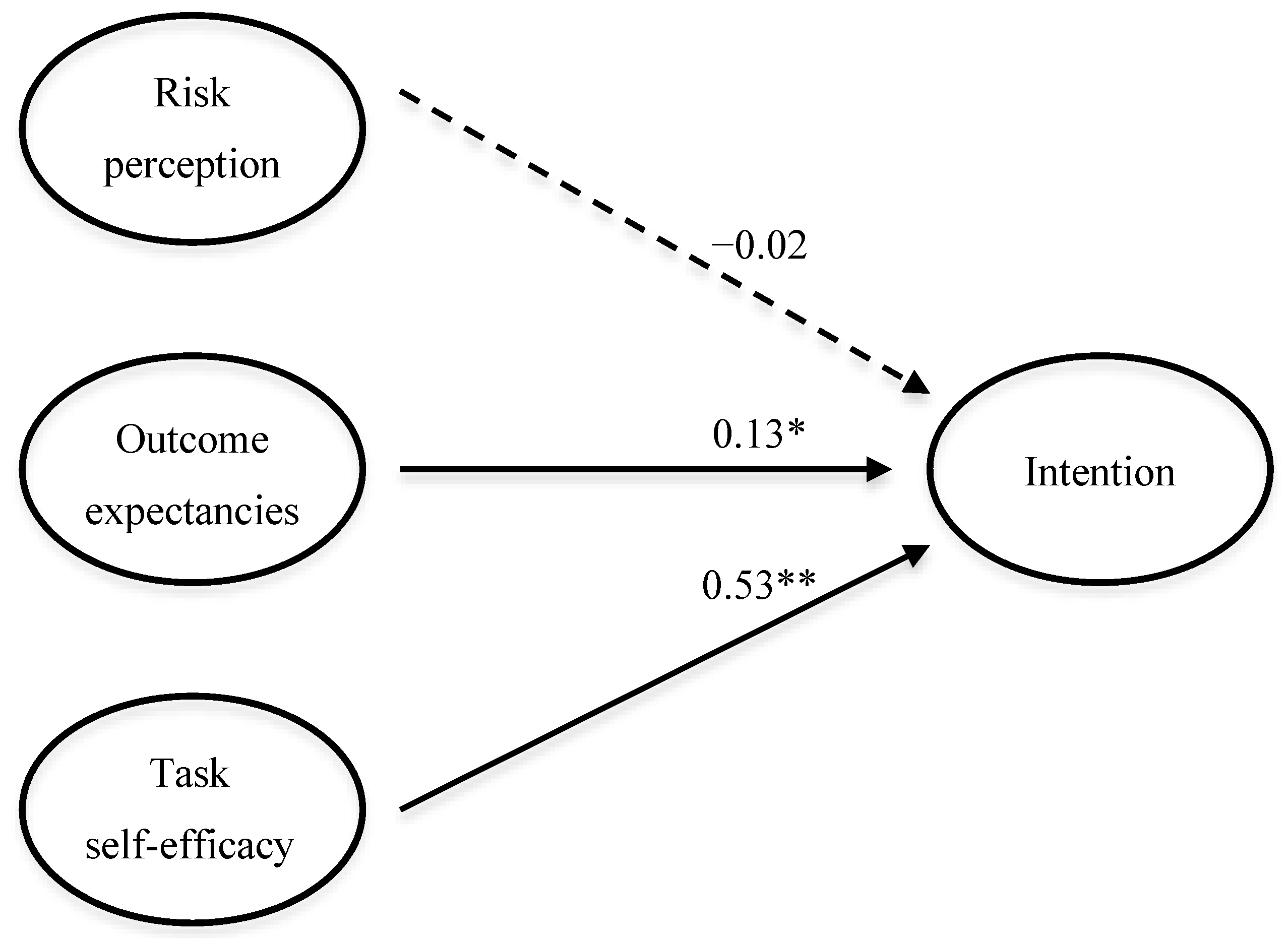
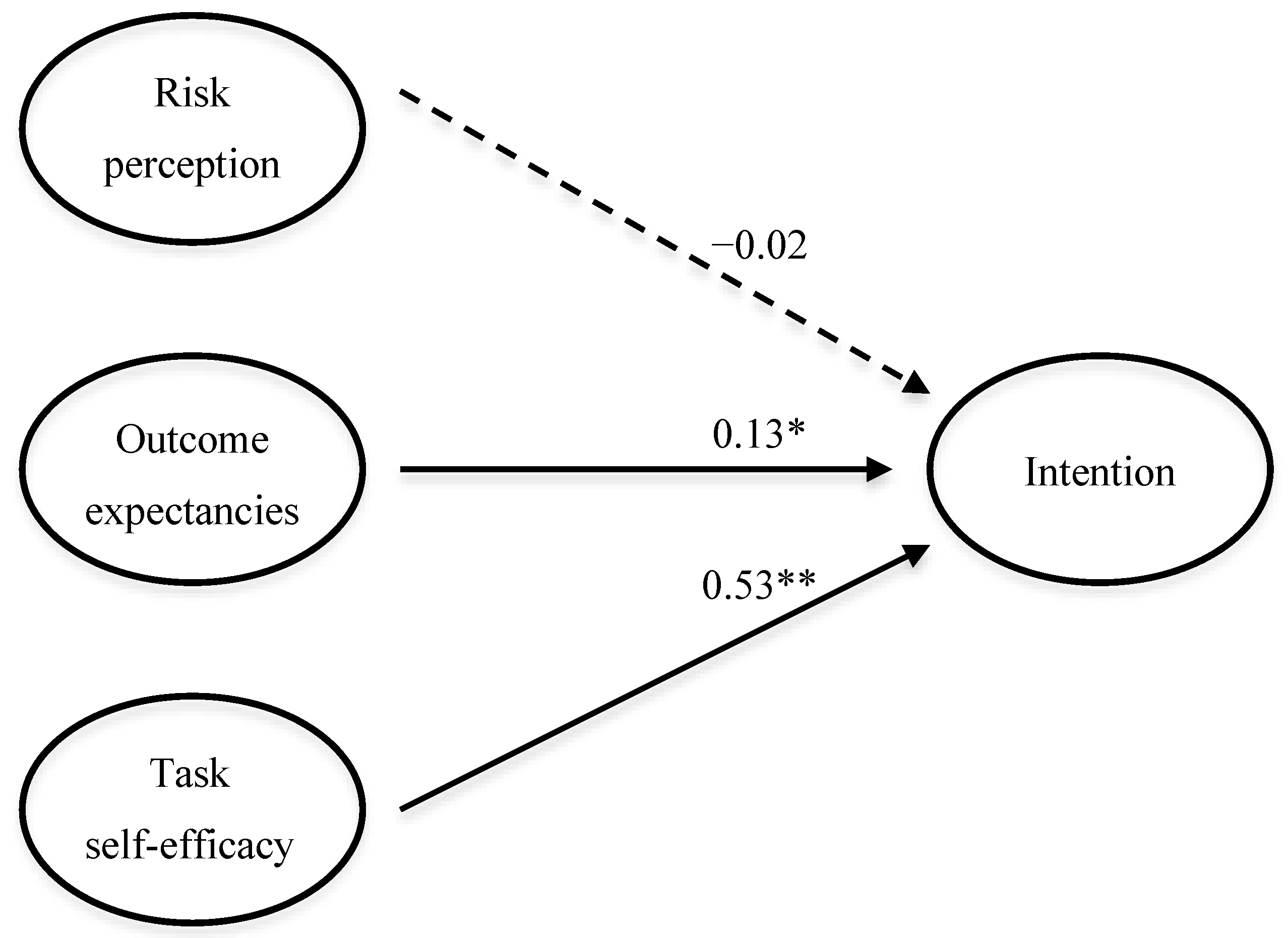
The Health Action Process Approach (HAPA) model is a theory of health behavior change that is particularly suited to describing the adoption of preventive behaviors [
26]. It comprises a motivation phase during which individuals form a behavioral intention, and a two-stage goal-pursuit (volitional) phase where intenders form plans to enact, and actors actually engage in, a target behavior. In the motivation phase, perceived task self-efficacy and outcome expectancies are posited as major predictors of intention, with risk perception exerting a minor direct influence [
26]. In the volitional phase, intention must be translated into action through a process of action and coping planning, influenced by perceived maintenance self-efficacy. Once the behavior has been initiated, perceived maintenance and recovery self-efficacy govern self-regulatory processes that can be influenced by environmental barriers and facilitators that can promote or inhibit continued action. The HAPA model has demonstrated utility in predicting and directing behavior in a number of health domains, including health screening, diet, and sunscreen use [
27,
28,
29], and has been advocated as a framework for designing health promotion interventions.
Although other theories of behavior change have been explored in injury prevention [
24,
25], many focus on social cognitive processes that originate well before the behavior in question (e.g., motivation) and are, therefore, unable to account for substantial amounts of variance when modeled in real world settings. The HAPA model, however, is centered on more proximal constructs that can be readily measured and may be amenable to change in a short period of time [
26]. Additionally, whereas other models (e.g., Theory of Planned Behavior) are oriented toward volitional processes for undertaking positively- framed behaviors, such as exercise for health benefit or enjoyment, injury prevention is inherently an avoidance-framed action and, therefore, suited to models that account for individual perceptions of risk and outcome expectancy. The HAPA model also satisfies this criterion. Moreover, the model describes the influence of factors that influence behavioral maintenance following initial uptake, which is appropriate considering the dose-response nature of the FIFA 11+ [
19]. This added predictive power represents an incremental step beyond previously explored models, and as such could provide additional insight into the implementation challenges faced in sport injury prevention contexts.
Therefore, the purpose of this study was to explore the utility of the HAPA model in predicting intention to adopt the FIFA 11+ amongst youth soccer coaches and players, as an initial proof of concept to inform the design of larger prospective studies. The primary objective was to describe perceived task self-efficacy, outcome expectancies, and risk perceptions in this setting. The secondary objectives were to determine whether these factors predicted intention to use the FIFA 11+ at the start of the soccer season and to assess the fit of the HAPA model as an appropriate behavior change theory to apply in this context.
2. Materials and Methods
2.1. Study Design
This was a cross-sectional study conducted at the start of the 2013 outdoor soccer season (May–August) in Calgary, Canada. This study was approved by the Conjoint Health Research Ethics Board at the University of Calgary (No. 24985).
2.2. Participants
The study population consisted of coaches and youth female soccer players (aged 12–16 years) competing in the Calgary Minor Soccer Association. Due to the exploratory nature of the study, no formal a priori sample size was calculated. Coaches were eligible to participate if they were the head or assistant coach of a female soccer team competing in Tier 1 or 2 of the U14 or U16 age group at the start of the season, and were excluded if they had any previous experience using the FIFA 11+. Players were eligible if they belonged to a female soccer team competing in the U14 or U16 age group at the start of the season and their team coach was participating in the study (as coach permission was required to approach players for recruitment). Exclusion criteria for players included a recent (within six weeks) history of injury requiring medical attention or the inability to participate in soccer for at least one day and preventing full participation at the start of the 2013 season, or a history of systemic disease or neurological disorder preventing full participation at the start of the 2013 season. Teams were randomly approached for recruitment by club once teams were formed prior to the start of the season. All coaches provided written informed consent, and players provided written informed parental consent and personal assent to take part in the study.
2.3. The FIFA 11+ Program
The FIFA 11+ program is a 20-min warm-up that consists of running exercises, dynamic stretching, plyometrics, and agility, strengthening, and balance exercises [
30]. It was developed specifically to reduce the risk of lower limb injury amongst recreational soccer players, and as such, the focus of the program is on cutting, jumping, and landing technique. The program is freely available online and is supported by a suite of resources, including a coaching manual, videos, posters, and flashcards [
30].
2.4. Procedure
Prior to the start of the season, coaches attended a two-hour FIFA 11+ instructional workshop, delivered by the lead author (who has experience playing and coaching soccer at the level targeted in this study). Each exercise in the program was demonstrated, with clear directions on identifying correct and incorrect technique, and coaches were given copies of the program resources. The emphasis of the workshop was on the program content, with only a brief rationale for its use (e.g., a why the program was developed and a short summary of evidence for its efficacy) presented for context. Coaches were clearly told that choosing to use the FIFA 11+ in the following season would be entirely voluntary, and the purpose of the study was to better understand why teams might or might not decide to use the program.
After this familiarization, coaches completed a questionnaire to assess demographic characteristics, perceptions about soccer injury, and the HAPA constructs.
Player questionnaires were administered by study personnel in a supervised team setting at a training session prior to the start of the season. Coaches explained the FIFA 11+ to the players, and the questionnaires were answered based on the players’ understanding of the program at that time.
2.5. Outcome Measures
A bespoke questionnaire was developed for this study, with separate versions for coaches and players (see
supplementary online content). Section A of the questionnaire captured demographic, soccer coaching/playing experience, and injury history information. Section B focused on the HAPA constructs, with questions assessing self-efficacy, outcome expectancies, risk perceptions, behavioral intentions, and barriers and facilitators to FIFA 11+ implementation.
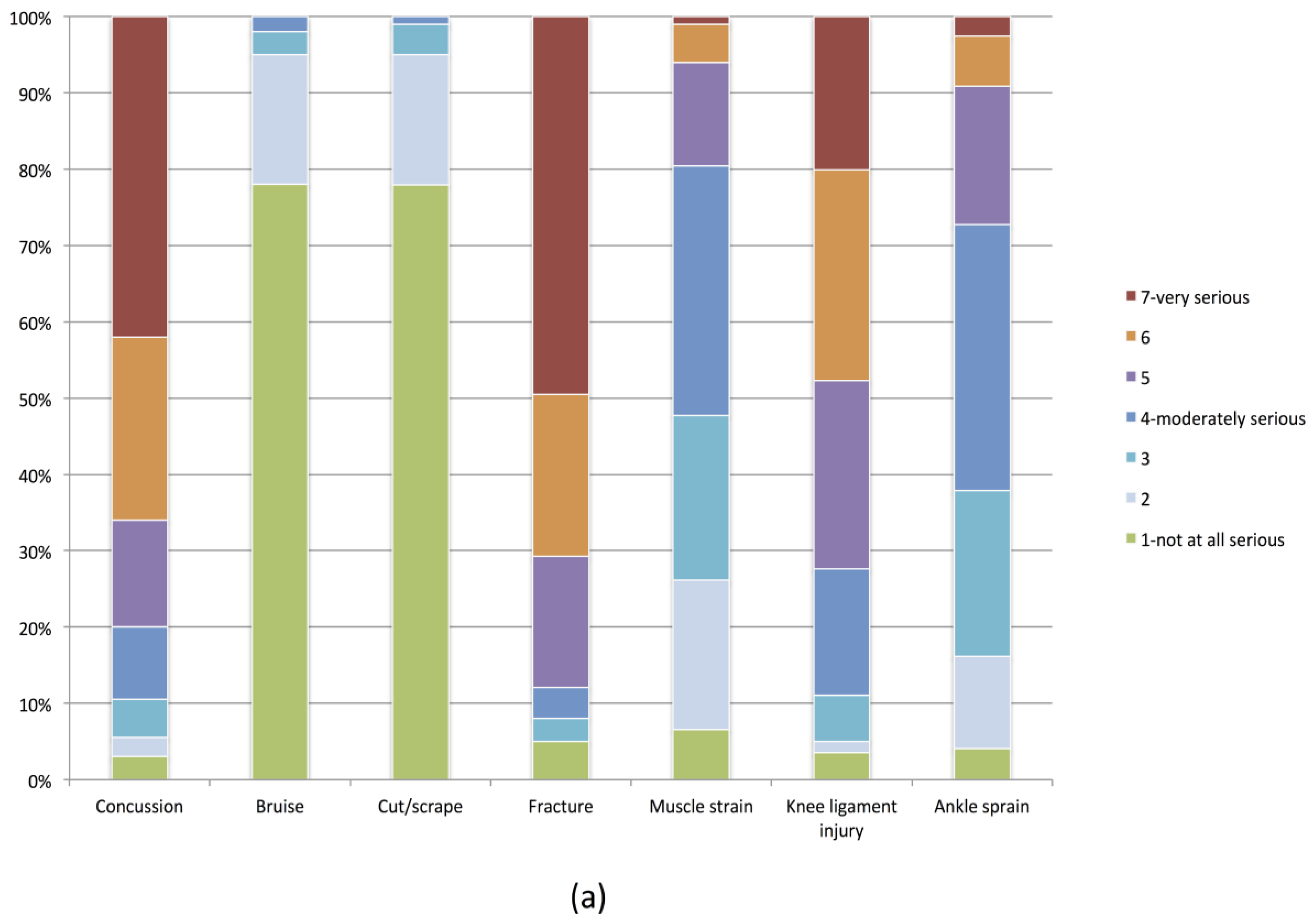
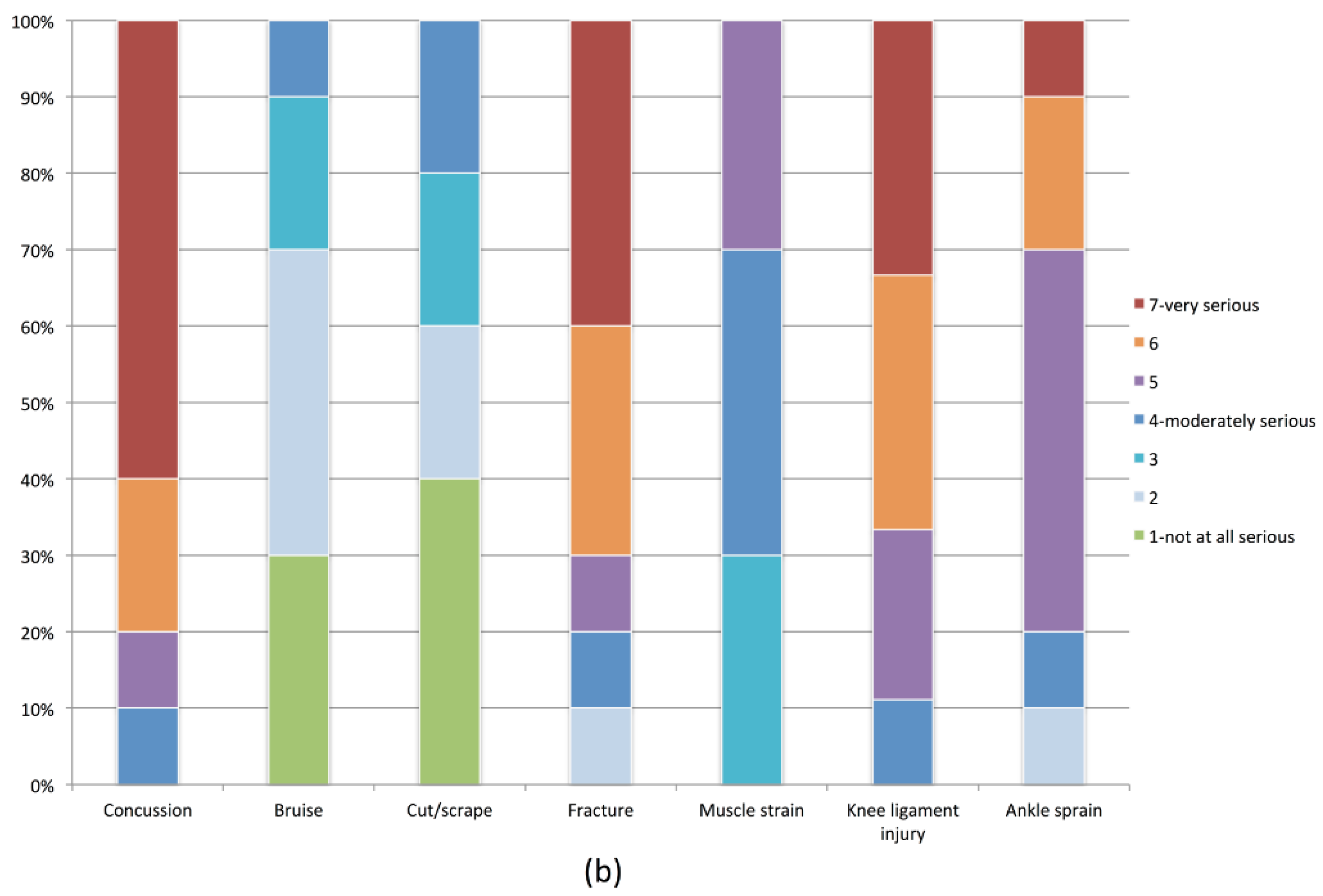
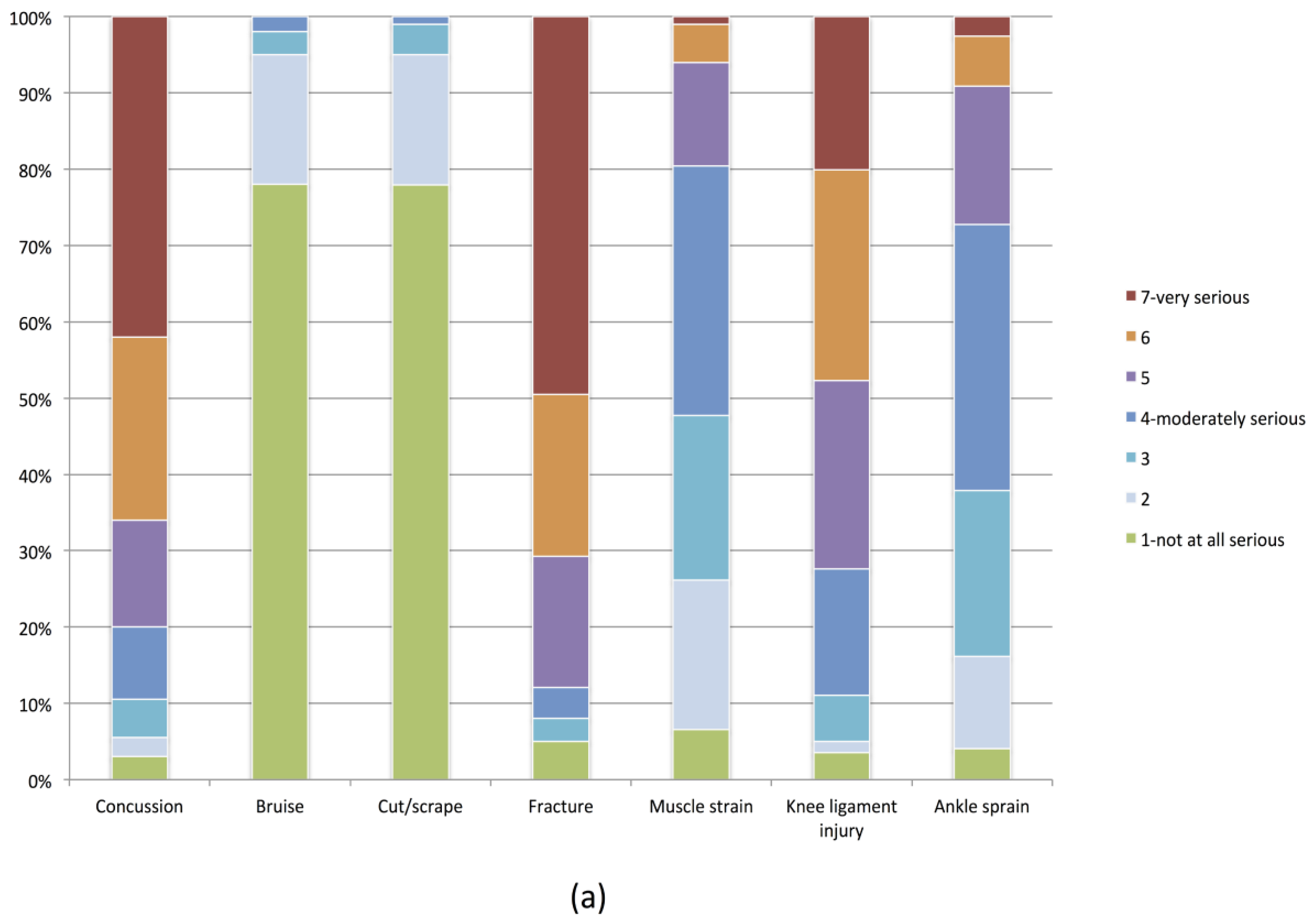
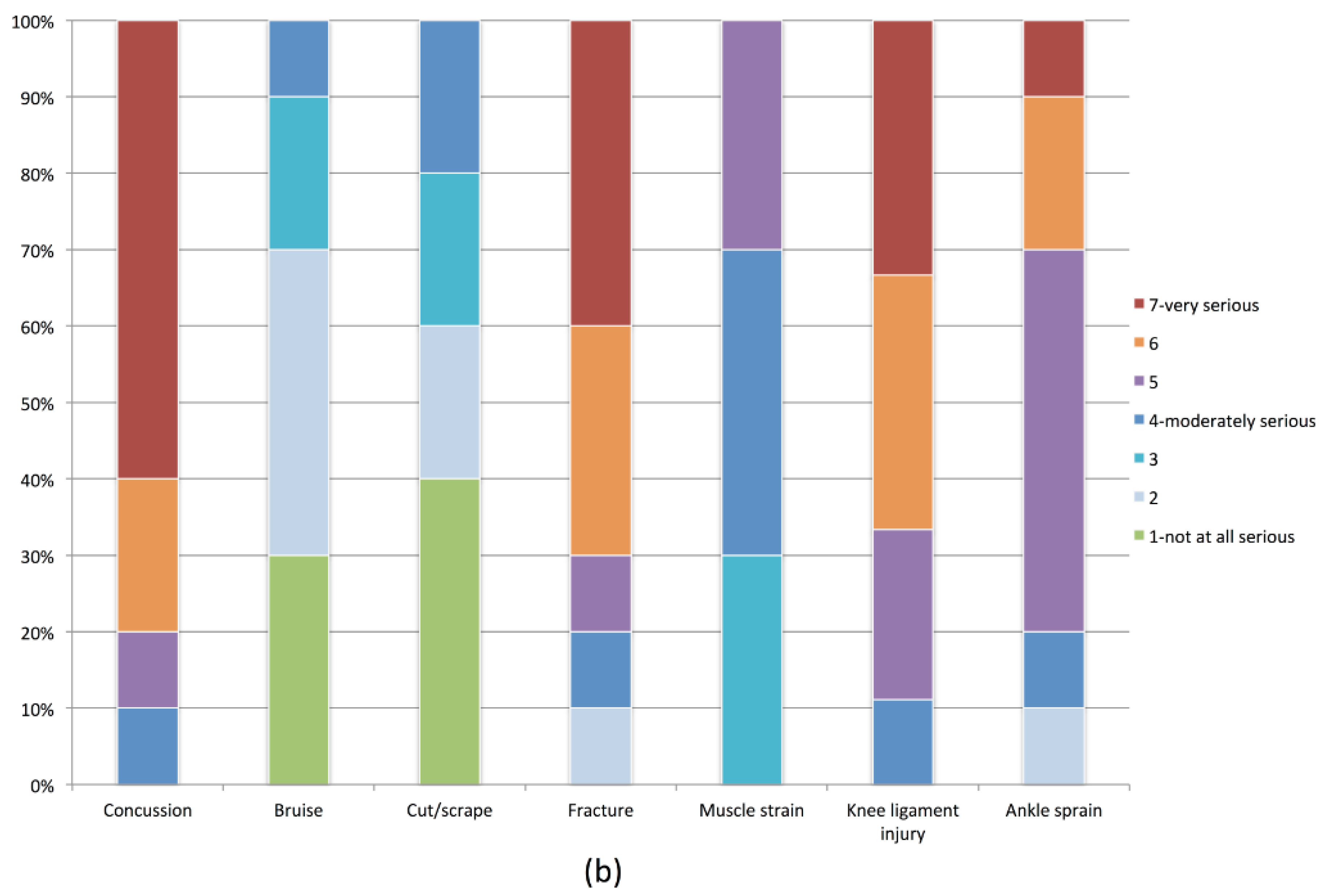
Questions were developed by adapting previously validated HAPA questionnaire item stems [
31] to reflect the youth soccer context. For example, the stem “How serious are the following health-related problems?” with a response list including heart attack, stroke, and high blood pressure [
31] was adapted to “How serious are the following types of soccer injury?” with a response list including ankle sprain, knee ligament injury, and broken bone (with both questions scored on a seven-point Likert scale ranging from
not at all serious to
very serious) (see
supplementary content). The questionnaires underwent face validation by a group of experts (a soccer coach, a youth soccer player, a sport psychology researcher, and a physiotherapist) who were all familiar with the FIFA 11+ program. Questions were answered on a seven-point Likert scales that included reverse-coded items to ensure accurate completion. For analysis purposes, items were scored on a scale of 1 = ‘extremely negative’ to 7 = ‘extremely positive’.
2.6. Analysis
Descriptive analyses (frequencies, means, standard deviations (SD)) were used to assess demographic characteristics and questionnaire responses. Due to the low number of coaches in the sample, data were checked for normal distribution and Pearson correlations were subsequently used to assess the association between HAPA variables and intent to use the FIFA 11+. The threshold for statistical significance was set at p = 0.05 and, due to the exploratory nature of the study, no corrections were made for multiple comparisons. These analyses were conducted using STATA v.13 (StataCorp; College Station, TX, USA).
To assess the fit of the HAPA model for predicting player intention, structural equation modeling was employed [
32] and a two-step approach was applied [
33]. The standardized root mean square residual (SRMR) and the root mean square of error of approximation (RMSEA) were chosen as indicators of absolute fit [
34]. SRMR and RMSEA values ≤0.08 and ≤0.06, respectively, have been deemed to indicate a model with good fit to the data [
34]. The incremental fit indices were represented by the comparative fit index (CFI) and the Tucker Lewis index (TLI). Values >0.90 indicate adequate model fit, and values >0.95 are considered to indicate excellent fit [
34]. Modeling was conducted in AMOS v.22 (SPSS; Chicago, IL, USA).



{kind=link}
{kind=link}
{kind=link}