
Assessing Community Readiness to Reduce Childhood Diarrheal Disease and Improve Food Security in Dioro, Mali



Abstract
:1. Introduction
2. Materials and Methods
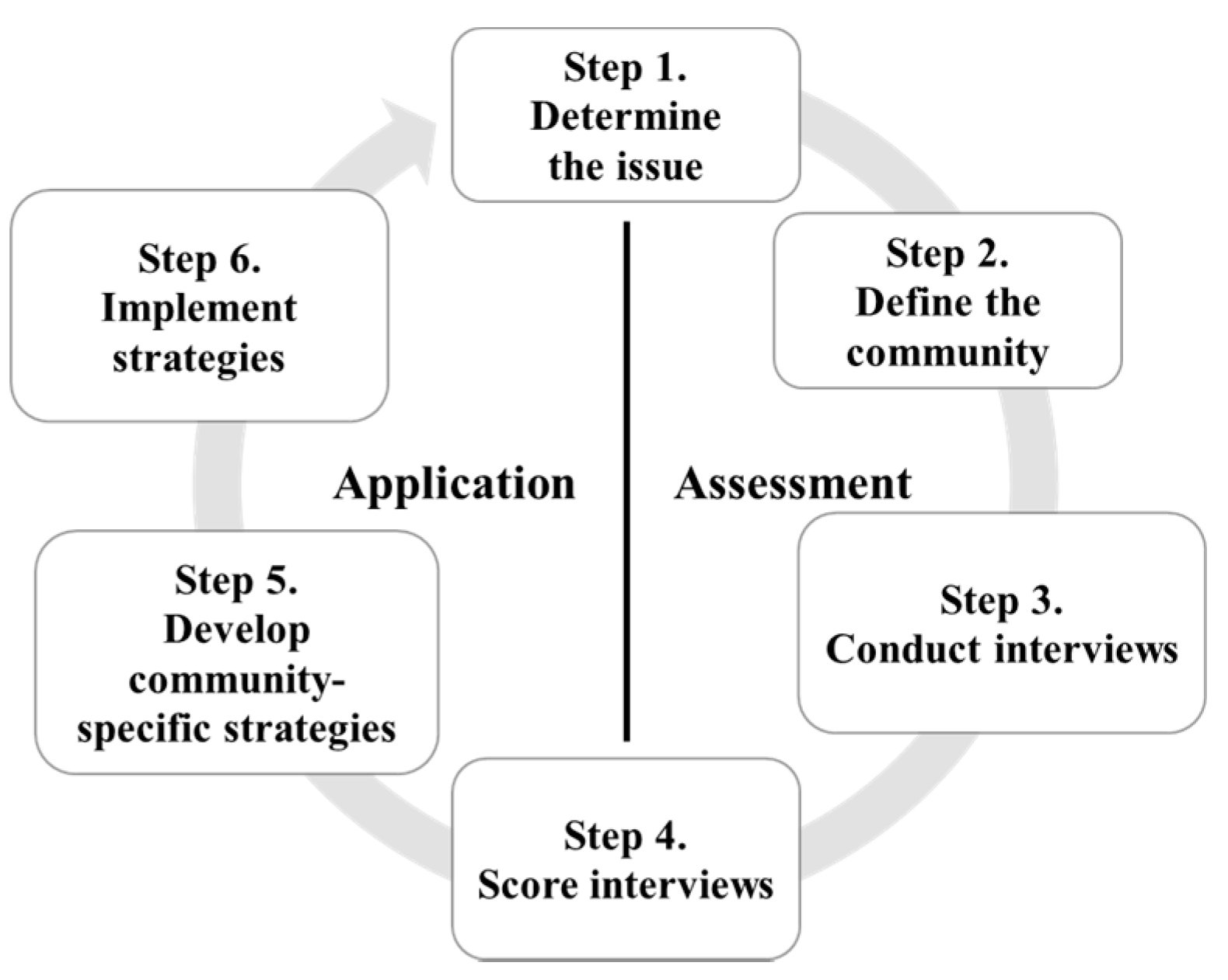
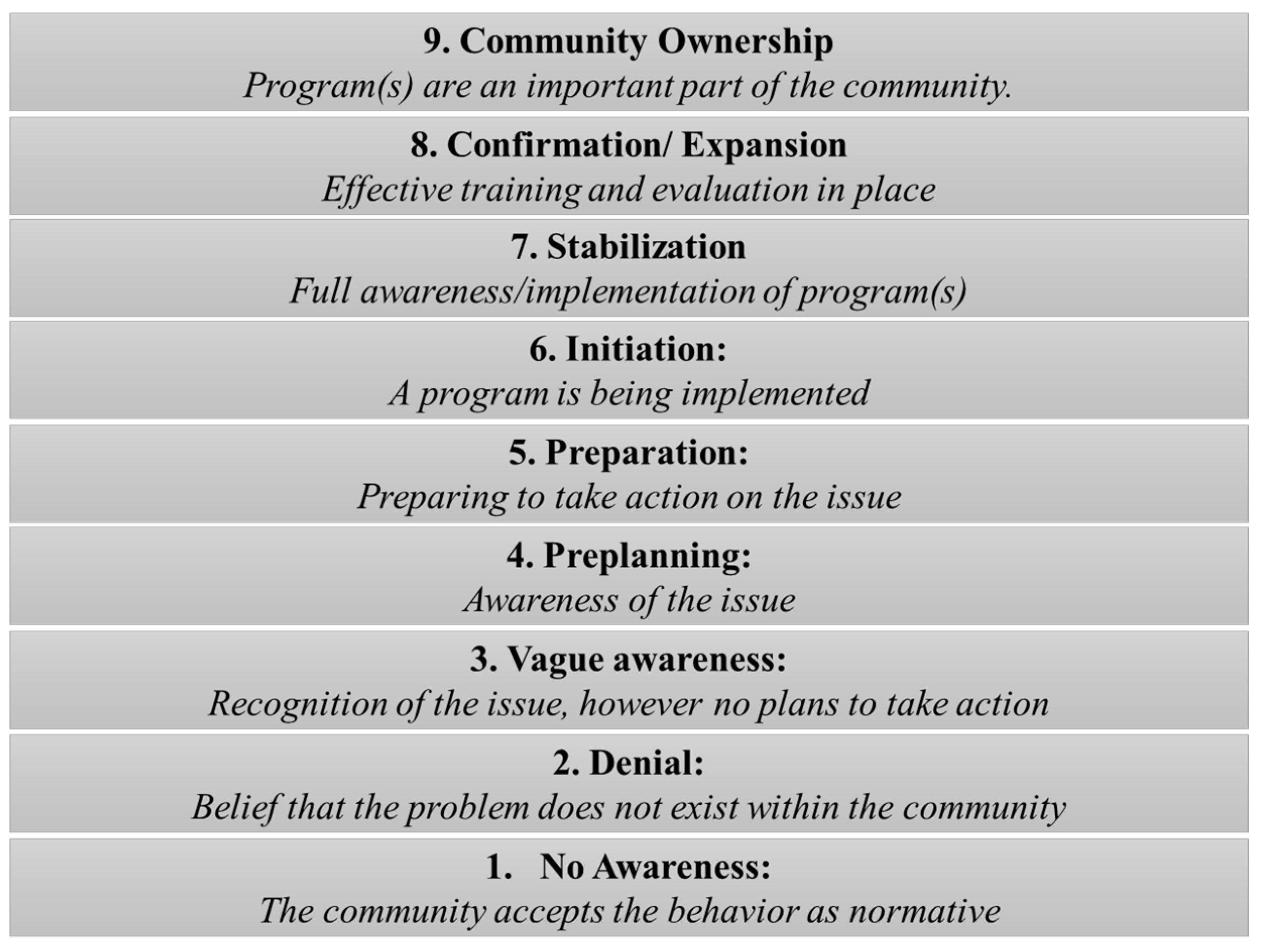
2.1. The Community Readiness Model (CRM)
2.2. Community, Study Population, and Interview Process
2.3. CRM Scores and Analysis
3. Results
3.1. Participant Characteristics
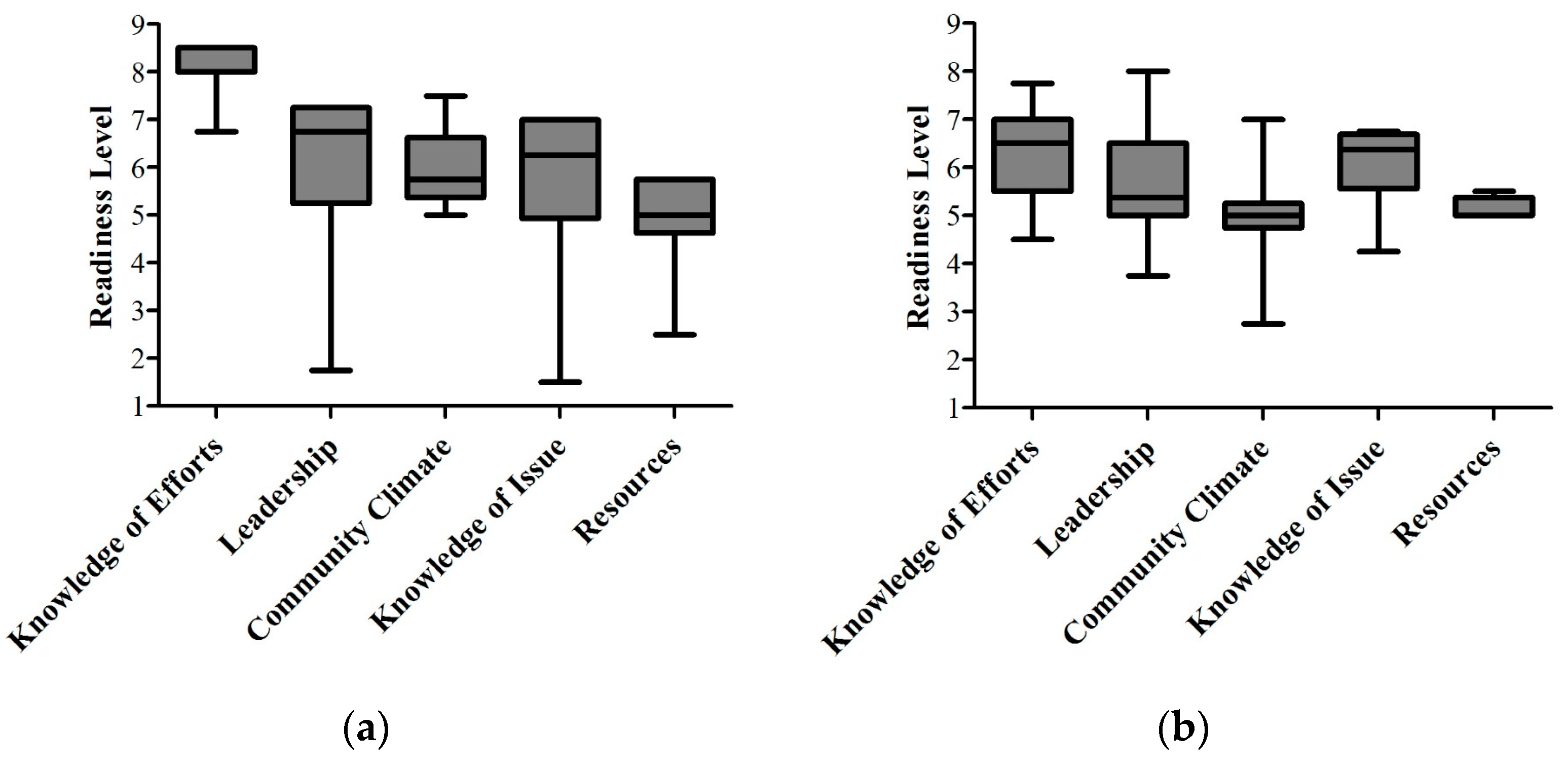
3.2. Community Readiness on Childhood Diarrheal Disease
3.3. Community Readiness on Food Security
3.4. Collection of Health and Food Behaviors within the Community
3.5. Initial Proposed Activities to Improve Readiness
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- INFO-STAT. Enquête Démographique et de Santé du Mali (EDSM-V) 2012–2013 Rapport Préliminaire; Cellule de Planification et de Statistiques (CPS) & Institut National de la Statistique (INSTAT): Bamako, Mali; ICF International: Calverton, MD, USA, 2013. [Google Scholar]
- FAO; IFAD; WFP. Meeting the 2015 international hunger targets: Taking stock of uneven progress. In The State of Food Insecurity in the World 2015; FAO: Rome, Italy, 2015. [Google Scholar]
- Keusch, G.T.; Denno, D.M.; Black, R.E.; Duggan, C.; Guerrant, R.L.; Lavery, J.V.; Nataro, J.P.; Rosenberg, I.H.; Ryan, E.T.; Tarr, P.I.; et al. Environmental enteric dysfunction: Pathogenesis, diagnosis, and clinical consequences. Clin. Res. Infect. Dis. 2014, 59, S207–S212. [Google Scholar] [CrossRef] [PubMed]
- USAID; SPRING; GAIN. Designing the Future of Nutrition Social and Behavior Change Communication: How to Achieve Impact at Scale; USAID: Washington, DC, USA, 2014. [Google Scholar]
- World Bank. World Development Indicators. 2015. Available online: http://data.worldbank.org/data-catalog/world-development-indicators (accessed on 2 March 2016).
- Shekar, M.; Mattern, M.; Eozenou, P.; Eberwein, J.; Akoku, J.; Di Gropello, E.; Karamba, W. Scaling Up Nutrition for A More Resilient Mali: Nutrition Diagnostics and Costed Plan for Scaling Up; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2015. [Google Scholar]
- Edwards, R.W.; Jumper-Thurman, P.; Plested, B.A.; Oetting, E.R.; Swanson, L. Community readiness: Research to practice. J. Community Psychol. 2000, 28, 291–307. [Google Scholar] [CrossRef]
- Kostadinov, I.; Daniel, M.; Stanley, L.; Gancia, A.; Cargo, M. A systematic review of community readiness tool applications: Implications for reporting. Int. J. Environ. Res. Public Health 2015, 12, 3453–3468. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.D.; Ngure, F.M.; Pelto, G.; Young, S.L. What are we assessing when we measure food security? A compendium and review of current metrics. Int. J. Environ. Res. Public Health 2013, 4, 481–505. [Google Scholar] [CrossRef] [PubMed]
- Oetting, E.R.; Plested, B.A.; Edwards, R.W.; Thurman, K.; Kelly, J.; Beauvais, F.; Stanley, L. Community Readiness for Community Change: Tri-Ethnic Center Community Readiness Handbook; Tri-Ethnic Center for Prevention Research: Fort Collins, CO, USA, 2014. [Google Scholar]
- Millennium Villages. Available online: http://millenniumvillages.org/ (accessed on 23 March 2016).

{kind=link}
{kind=link}
{kind=link}
| Characteristic | Number of Key Respondents (%) |
|---|---|
| Sex | |
| Male | 9 (69%) |
| Female | 4 (31%) |
| Age range | |
| 25–34 y | 2 (15%) |
| 35–44 y | 2 (15%) |
| 45–54 y | 1 (10%) |
| 55–64 y | 4 (30%) |
| 65+ y | 4 (30%) |
| Dioro neighborhood | |
| Bozola | 3 (23%) |
| Darsalam | 2 (15%) |
| Djeda | 1 (8%) |
| Hamdalaye | 2 (15%) |
| Mairie | 2 (15%) |
| Médine | 1 (8%) |
| Missira | 1 (8%) |
| Tinti | 1 (8%) |
| Social roles/Professions | |
| CAFO 1 | 2 (15%) |
| Community Health Worker | 1 (8%) |
| Fisherman | 1 (8%) |
| Merchant | 2 (15%) |
| Neighborhood chief | 2 (15%) |
| Radio director | 1 (8%) |
| Rice farmer | 2 (15%) |
| Teacher | 2 (15%) |
| Community Issue | Knowledge of Efforts | Leadership | Community Climate | Knowledge of Issue | Resources | Overall Readiness |
|---|---|---|---|---|---|---|
| Childhood diarrheal disease | 8.0 ± 0.5 (Confirmation) | 5.75 ± 1.75 (Preparation) | 5.75 ± 0.75 (Preparation) | 5.5 ± 1.75 (Preparation) | 4.75 ± 1.0 (Preplanning) | 5.75 ± 1.0 (Preparation) |
| Food security | 6.25 ± 1.0 (Initiation) | 5.5 ± 1.0 (Preparation) | 5.0 ± 1.25 (Preparation) | 5.75 ± 1.0 (Preparation) | 5.0 ± 0.5 (Preparation) | 5.5 ± 0.5 (Preparation) |
| Dimension | Score/Stage | Stage Definition | Goal to Maintain/Improve Stage | Activities to Increase Stage |
|---|---|---|---|---|
| Knowledge of Efforts | 8.0/Confirmation | Most community members know a great deal about local efforts. | Conduct training and meetings to review progress and modify programs | Develop formal network Prepare community specific risk profile |
| Leadership | 5.75/Preparation | Leadership is participating in developing and improving efforts. Some leaders are playing a key role. | Gather existing information to help plan strategies | Utilize community leaders to speak to groups and participate in local radio talk shows |
| Community Climate | 5.75/Preparation | The community’s attitude is concerned about this issue and wants to do something about it. | Gather existing information to help plan strategies | Conduct community surveys and public forums to develop strategies Sponsor a community event to initiate the effort |
| Knowledge of Issue | 5.5/Preparation | The community members have basic knowledge about causes, consequences, signs and symptoms of childhood diarrheal diseases. | Gather existing information to help plan strategies | Conduct community surveys Present in-depth local information |
| Resources | 4.75/Preplanning | There are limited resources currently available to address the issue. | Raise awareness with concrete ideas | Review existing efforts in community to determine who benefits and what the degree of success has been |
| Dimension | Score/Stage | Stage Definition | Goal to Maintain/Improve Stage | Activities to Increase Stage |
|---|---|---|---|---|
| Knowledge of Efforts | 6.25/Initiation | Most community members have at least basic knowledge of local efforts. | Provide community specific information | Plan publicity efforts associated with start-up of program/activity |
| Leadership | 5.50/Preparation | Leadership is participating in developing and improving efforts. Some leaders are playing a key role. | Gather existing information to help plan strategies | Utilize key leaders and influential people to speak to groups and to participate in local radio shows |
| Community Climate | 5.0/Preparation | The community’s attitude is concerned about this issue and wants to do something about it. | Gather existing information to help plan strategies | Conduct community surveys and public forums to develop strategies Sponsor a community event to initiate the effort |
| Knowledge of Issue | 5.75/Preparation | The community members have basic knowledge about causes and consequences regarding lack of food security. | Gather existing information to help plan strategies | Conduct community surveys Present in-depth local information. |
| Resources | 5.0/Preparation | There are some resources identified that could be used to address the issue. | Gather existing information to help plan strategies | Conduct formal surveys with stakeholders to determine long-term plan of resources (both monetary and non-monetary) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Borresen, E.C.; Stone, C.; Boré, A.; Cissoko, A.; Maiga, A.; Koita, O.A.; Ryan, E.P. Assessing Community Readiness to Reduce Childhood Diarrheal Disease and Improve Food Security in Dioro, Mali. Int. J. Environ. Res. Public Health 2016, 13, 571. https://doi.org/10.3390/ijerph13060571
Borresen EC, Stone C, Boré A, Cissoko A, Maiga A, Koita OA, Ryan EP. Assessing Community Readiness to Reduce Childhood Diarrheal Disease and Improve Food Security in Dioro, Mali. International Journal of Environmental Research and Public Health. 2016; 13(6):571. https://doi.org/10.3390/ijerph13060571
Chicago/Turabian StyleBorresen, Erica C., Cordelia Stone, Abdoulaye Boré, Alima Cissoko, Ababacar Maiga, Ousmane A. Koita, and Elizabeth P. Ryan. 2016. "Assessing Community Readiness to Reduce Childhood Diarrheal Disease and Improve Food Security in Dioro, Mali" International Journal of Environmental Research and Public Health 13, no. 6: 571. https://doi.org/10.3390/ijerph13060571
APA StyleBorresen, E. C., Stone, C., Boré, A., Cissoko, A., Maiga, A., Koita, O. A., & Ryan, E. P. (2016). Assessing Community Readiness to Reduce Childhood Diarrheal Disease and Improve Food Security in Dioro, Mali. International Journal of Environmental Research and Public Health, 13(6), 571. https://doi.org/10.3390/ijerph13060571