
Alcoholic Beverage Consumption and Chronic Diseases



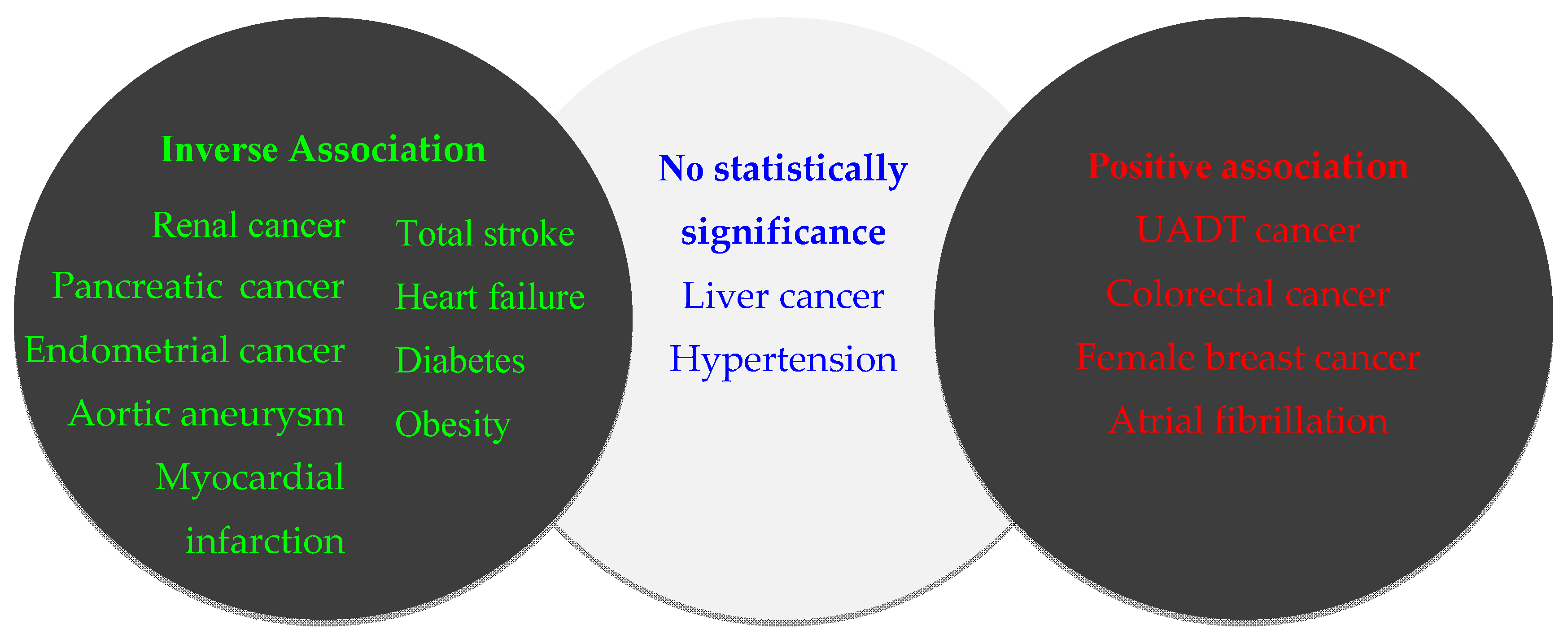
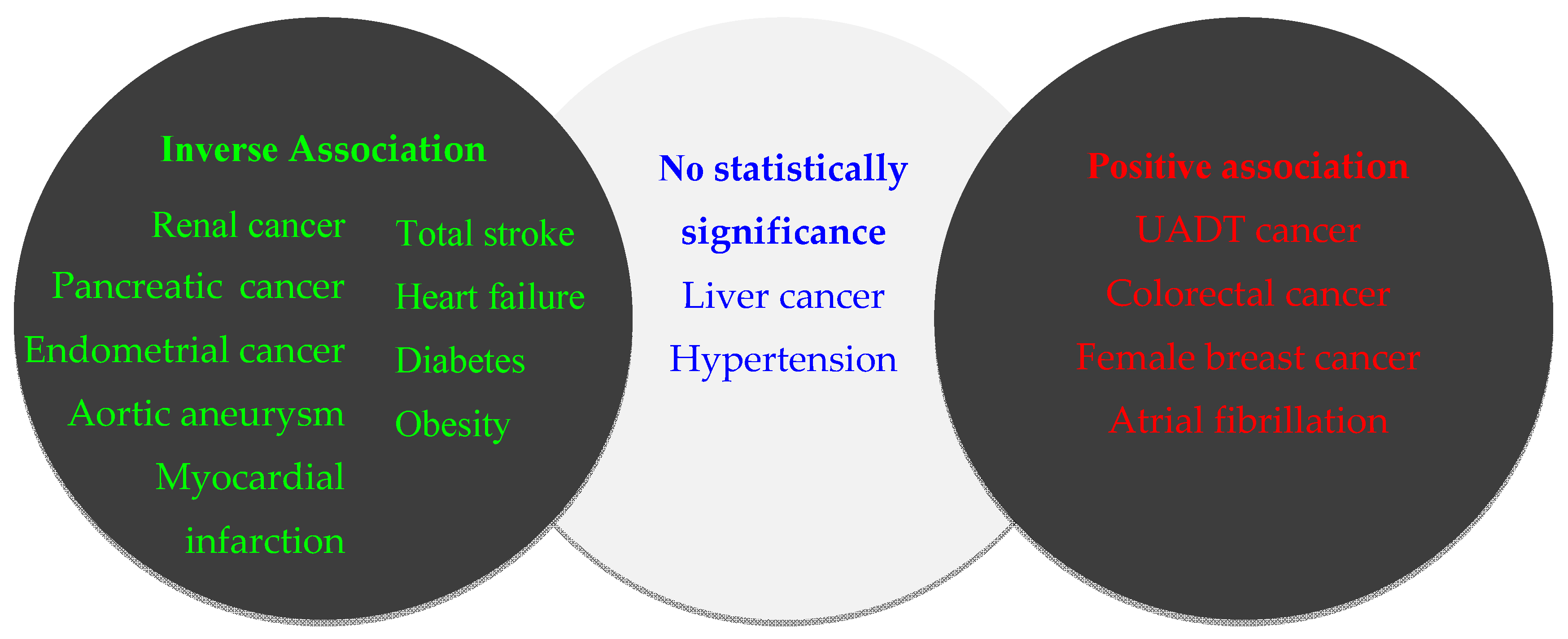
Abstract
:1. Introduction
2. Cancer
2.1. Drinking and UADT Cancers
2.2. Drinking and Liver Cancer
2.3. Drinking and Colorectal Cancer
2.4. Drinking and Breast Cancer
2.5. Drinking and Pancreatic Cancer
2.6. Drinking and Other Cancers
2.7. Potential Mechanisms for Protective Effects of Drinking in Cancer Development
2.8. Potential Mechanisms for Detrimental Effects of Drinking in Cancer Development
2.8.1. Modulating Sex Hormone Levels
2.8.2. Promoting Age-Related Biological Processes
2.8.3. Interfering with Folate Metabolism
2.8.4. Promoting Cancer Cell Invasion and Metastasis
2.8.5. Possible Carcinogenic Mechanisms of Acetaldehyde
3. Cardiovascular Diseases
3.1. Drinking and Coronary Artery Disease
3.2. Drinking and Stroke
3.3. Drinking and Atrial Fibrillation
3.4. Drinking and Hypertension
3.5. Drinking and Heart Failure
3.6. Potential Mechanisms
3.6.1. Potential Mechanisms for Protective Effects in the Development of Cardiovascular Disease
3.6.2. Potential Mechanisms for Detrimental Effects in the Development of Cardiovascular Disease
4. Diabetes Mellitus
4.1. Evidence from Epidemiological Studies
4.2. Potential Mechanisms
4.2.1. Potential Mechanisms for Protective Effects in the Development Diabetes Mellitus
4.2.2. Potential Mechanisms for the Detrimental Effects of Drinking in Diabetes Mellitus
5. Obesity
5.1. Evidences from Epidemiological Studies
5.2. Potential Mechanisms
5.2.1. Potential Mechanisms for Protective Effects in the Development of Obesity
5.2.2. Potential Mechanisms for Detrimental Effects in the Development of Obesity
6. Prospects
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- WHO. Global Status Report on Alcohol and Health 2014. Available online: http://www.who.int/substance_abuse/publications/global_alcohol_report/en/ (accessed on 29 March 2016).
- Liang, Y.; Mente, A.; Yusuf, S.; Gao, P.; Sleight, P.; Zhu, J.; Fagard, R.; Lonn, E.; Teo, K.K. Alcohol consumption and the risk of incident atrial fibrillation among people with cardiovascular disease. CMAJ 2012, 184, E857–E866. [Google Scholar] [CrossRef] [PubMed]
- Jin, M.; Cai, S.; Guo, J.; Zhu, Y.; Li, M.; Yu, Y.; Zhang, S.; Chen, K. Alcohol drinking and all cancer mortality: A meta-analysis. Ann. Oncol. 2013, 24, 807–816. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Duan, H.; Yang, H.; Lin, J. A pooled analysis of alcohol intake and colorectal cancer. Int. J. Clin. Exp. Med. 2015, 8, 6878–6889. [Google Scholar] [PubMed]
- Blomster, J.I.; Zoungas, S.; Chalmers, J.; Li, Q.; Chow, C.K.; Woodward, M.; Mancia, G.; Poulter, N.; Williams, B.; Harrap, S.; et al. The relationship between alcohol consumption and vascular complications and mortality in individuals with type 2 diabetes. Diabetes Care 2014, 37, 1353–1359. [Google Scholar] [CrossRef] [PubMed]
- Leong, D.P.; Smyth, A.; Teo, K.K.; McKee, M.; Rangarajan, S.; Pais, P.; Liu, L.; Anand, S.S.; Yusuf, S. Patterns of alcohol consumption and myocardial infarction risk: Observations from 52 countries in the INTERHEART case-control study. Circulation 2014, 130, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Shield, K.D.; Parry, C.; Rehm, J. Chronic diseases and conditions related to alcohol use. Alcohol Res. 2013, 35, 155–173. [Google Scholar] [PubMed]
- Toth, A.; Sandor, B.; Papp, J.; Rabai, M.; Botor, D.; Horvath, Z.; Kenyeres, P.; Juricskay, I.; Toth, K.; Czopf, L. Moderate red wine consumption improves hemorheological parameters in healthy volunteers. Clin. Hemorheol. Microcirc. 2014, 56, 13–23. [Google Scholar] [PubMed]
- Bargallo, M.; Grau, A.; Fernandezlarrea, J.; Anguiano, G.; Segarra, M.; Rovira, M.; Ferre, L.; Olive, M. Moderate red-wine consumption partially prevents body weight gain in rats fed a hyperlipidic diet. J. Nutr. Biochem. 2006, 17, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Fang, N.; Chen, D.D.Y.; Donkor, K.K. Determination of potentially anti-carcinogenic flavonoids in wines by micellar electrokinetic chromatography. Food Chem. 2008, 106, 415–420. [Google Scholar] [CrossRef]
- Arranz, S.; Chiva-Blanch, G.; Valderas-Martínez, P.; Medina-Remón, A.; Lamuela-Raventós, R.M.; Estruch, R. Wine, beer, alcohol and polyphenols on cardiovascular disease and cancer. Nutrients 2012, 4, 759–781. [Google Scholar] [CrossRef] [PubMed]
- Lachenmeier, D.W.; Przybylski, M.C.; Rehm, J. Comparative risk assessment of carcinogens in alcoholic beverages using the margin of exposure approach. Int. J. Cancer 2012, 131, E995–E1003. [Google Scholar] [CrossRef] [PubMed]
- Bagnardi, V.; Rota, M.; Botteri, E.; Tramacere, I.; Islami, F.; Fedirko, V.; Scotti, L.; Jenab, M.; Turati, F.; Pasquali, E.; et al. Alcohol consumption and site-specific cancer risk: A comprehensive dose-response meta-analysis. Br. J. Cancer 2015, 112, 580–593. [Google Scholar] [CrossRef] [PubMed]
- Kontou, N.; Psaltopoulou, T.; Soupos, N.; Polychronopoulos, E.; Xinopoulos, D.; Linos, A.; Panagiotakos, D. Alcohol consumption and colorectal cancer in a Mediterranean population: A case-control study. Dis. Colon Rectum 2012, 55, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Angel-Morales, G.; Noratto, G.; Mertens-Talcott, S. Red wine polyphenolics reduce the expression of inflammation markers in human colon-derived CCD-18Co myofibroblast cells: Potential role of microRNA-126. Food Funct. 2012, 3, 745–752. [Google Scholar] [CrossRef] [PubMed]
- Barron, C.C.; Moore, J.; Tsakiridis, T.; Pickering, G.; Tsiani, E. Inhibition of human lung cancer cell proliferation and survival by wine. Cancer Cell Int. 2014, 14, 6. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.J.; Mao, Y.Y.; Zhang, Y.; Cai, S.F.; Chen, G.D.; Ding, Y.; Guo, J.; Chen, K.; Jin, M.J. Alcohol drinking and upper aerodigestive tract cancer mortality: A systematic review and meta-analysis. Oral Oncol. 2014, 50, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Turati, F.; Galeone, C.; Rota, M.; Pelucchi, C.; Negri, E.; Bagnardi, V.; Corrao, G.; Boffetta, P.; La Vecchia, C. Alcohol and liver cancer: A systematic review and meta-analysis of prospective studies. Ann. Oncol. 2014, 25, 1526–1535. [Google Scholar] [CrossRef] [PubMed]
- Romieu, I.; Scoccianti, C.; Chajes, V.; de Batlle, J.; Biessy, C.; Dossus, L.; Baglietto, L.; Clavel-Chapelon, F.; Overvad, K.; Olsen, A.; et al. Alcohol intake and breast cancer in the European prospective investigation into cancer and nutrition. Int. J. Cancer 2015, 137, 1921–1930. [Google Scholar] [CrossRef] [PubMed]
- Tramacere, I.; Scottie, L.; Jenab, M.; Bagnardi, V.; Bellocco, R.; Rota, M.; Corrao, G.; Bravi, F.; Boffetta, P.; La Vecchia, C. Alcohol drinking and pancreatic cancer risk: A meta-analysis of the dose-risk relation. Int. J. Cancer 2010, 126, 1474–1486. [Google Scholar] [CrossRef] [PubMed]
- Marron, M.; Boffetta, P.; Møller, H.; Ahrens, W.; Pohlabeln, H.; Benhamou, S.; Bouchardy, C.; Lagiou, P.; Lagiou, A.; Slámová, A.; et al. Risk of upper aerodigestive tract cancer and type of alcoholic beverage: A European multicenter case-control study. Eur. J. Epidemiol. 2012, 27, 499–517. [Google Scholar] [CrossRef] [PubMed]
- Petti, S.; Masood, M.; Scully, C. The magnitude of tobacco smoking-betel quid chewing-alcohol drinking interaction effect on oral cancer in South-East Asia. A meta-analysis of observational studies. PLoS ONE 2013, 8, e78999. [Google Scholar] [CrossRef] [PubMed]
- Radoi, L.; Paget-Bailly, S.; Cyr, D.; Papadopoulos, A.; Guida, F.; Schmaus, A.; Cenee, S.; Menvielle, G.; Carton, M.; Lapotre-Ledoux, B.; et al. Tobacco smoking, alcohol drinking and risk of oral cavity cancer by subsite: Results of a French population-based case-control study, the ICARE study. Eur. J. Cancer Prev. 2013, 22, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Jerjes, W.; Upile, T.; Radhi, H.; Petrie, A.; Abiola, J.; Adams, A.; Kafas, P.; Callear, J.; Carbiner, R.; Rajaram, K.; et al. The effect of tobacco and alcohol and their reduction/cessation on mortality in oral cancer patients: Short communication. Head Neck Oncol. 2012, 4, 6. [Google Scholar] [CrossRef] [PubMed]
- Wu, I.C.; Wu, C.C.; Lu, C.Y.; Hsu, W.H.; Wu, M.C.; Lee, J.Y.; Chou, S.H.; Lee, J.M.; Chou, Y.P.; Wu, D.C.; et al. Substance use (alcohol, areca nut and cigarette) is associated with poor prognosis of esophageal squamous cell carcinoma. PLoS ONE 2013, 8, e55834. [Google Scholar] [CrossRef] [PubMed]
- Lubin, J.H.; Cook, M.B.; Pandeya, N.; Vaughan, T.L.; Abnet, C.C.; Giffen, C.; Webb, P.M.; Murray, L.J.; Casson, A.G.; Risch, H.A.; et al. The importance of exposure rate on odds ratios by cigarette smoking and alcohol consumption for esophageal adenocarcinoma and squamous cell carcinoma in the Barrett’s esophagus and esophageal adenocarcinoma consortium. Cancer Epidemiol. 2012, 36, 306–316. [Google Scholar] [CrossRef] [PubMed]
- Yates, M.; Cheong, E.; Luben, R.; Igali, L.; Fitzgerald, R.; Khaw, K.T.; Hart, A. Body mass index, smoking, and alcohol and risks of Barrett’s esophagus and esophageal adenocarcinoma: A UK prospective cohort study. Dig. Dis. Sci. 2014, 59, 1552–1559. [Google Scholar] [CrossRef] [PubMed]
- Dura, P.; Berkers, T.; van Veen, E.M.; Salomon, J.; Te Morsche, R.; Roelofs, H.; Kristinsson, J.O.; Wobbes, T.; Witteman, B.; Tan, A.; et al. Polymorphisms in alcohol-metabolizing enzymes and esophageal carcinoma susceptibility: A Dutch Caucasian case-control study. J. Hum. Genet. 2013, 58, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Persson, E.C.; Schwartz, L.M.; Park, Y.; Trabert, B.; Hollenbeck, A.R.; Graubard, B.I.; Freedman, N.D.; McGlynn, K.A. Alcohol consumption, folate intake, hepatocellular carcinoma, and liver disease mortality. Cancer Epidemiol. Biomark. 2013, 22, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.B.; Wang, H.B.; Pan, C.Q.; Shen, J.M.; Liang, Y. CYP2E1 PstI/RsaI polymorphism and interaction with alcohol consumption in hepatocellular carcinoma susceptibility: Evidence from 1661 cases and 2317 controls. Tumor Biol. 2012, 33, 979–984. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Yang, H.I.; Su, J.; Brenner, D.; Barrett-Connor, E.; Iloeje, U.; Chen, C.J. Synergism between obesity and alcohol in increasing the risk of hepatocellular carcinoma: A prospective cohort study. Am. J. Epidemiol. 2013, 177, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Cai, S.F.; Li, Y.J.; Ding, Y.; Chen, K.; Jin, M.J. Alcohol drinking and the risk of colorectal cancer death: A meta-analysis. Eur. J. Cancer Prev. 2014, 23, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Cho, E.; Lee, J.E.; Rimm, E.B.; Fuchs, C.S.; Giovannucci, E.L. Alcohol consumption and the risk of colon cancer by family history of colorectal cancer. Am. J. Clin. Nutr. 2012, 95, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Ding, J.; Li, S.; Liu, Y.; Cao, H.; Wu, J.; Tang, J.; Tajima, K. Polymorphisms in XRCC1 gene, alcohol drinking, and risk of colorectal cancer: A case-control study in Jiangsu province of China. Asian Pac. J. Cancer Prev. 2013, 14, 6613–6618. [Google Scholar] [CrossRef]
- Nan, H.M.; Lee, J.E.; Rimm, E.B.; Fuchs, C.S.; Giovannucci, E.L.; Cho, E. Prospective study of alcohol consumption and the risk of colorectal cancer before and after folic acid fortification in the United States. Ann. Epidemiol. 2013, 23, 558–563. [Google Scholar] [CrossRef] [PubMed]
- Fagherazzi, G.; Vilier, A.; Boutron-Ruault, M.C.; Mesrine, S.; Clavel-Chapelon, F. Alcohol consumption and breast cancer risk subtypes in the E3N-EPIC cohort. Eur. J. Cancer Prev. 2015, 24, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Kolonel, L.N.; Lim, U.; White, K.K.; Henderson, B.E.; Wilkens, L.R. Alcohol consumption and breast cancer risk among women from five ethnic groups with light to moderate intakes: The multiethnic cohort study. Int. J. Cancer 2014, 134, 1504–1510. [Google Scholar] [CrossRef] [PubMed]
- Hvidtfeldt, U.A.; Gunter, M.J.; Lange, T.; Chlebowski, R.T.; Lane, D.; Farhat, G.N.; Freiberg, M.S.; Keiding, N.; Lee, J.S.; Prentice, R.; et al. Quantifying mediating effects of endogenous estrogen and insulin in the relation between obesity, alcohol consumption, and breast cancer. Cancer Epidemiol. Biomark. 2012, 21, 1203–1212. [Google Scholar] [CrossRef] [PubMed]
- Chandran, U.; Zirpoli, G.; Ciupak, G.; McCann, S.E.; Gong, Z.; Pawlish, K.; Lin, Y.; Demissie, K.; Ambrosone, C.B.; Bandera, E.V. Does alcohol increase breast cancer risk in African-American women? Findings from a case-control study. Br. J. Cancer 2013, 109, 1945–1953. [Google Scholar] [CrossRef] [PubMed]
- Islam, T.; Ito, H.; Sueta, A.; Hosono, S.; Hirose, K.; Watanabe, M.; Iwata, H.; Tajima, K.; Tanaka, H.; Matsuo, K. Alcohol and dietary folate intake and the risk of breast cancer: A case-control study in Japan. Eur. J. Cancer Prev. 2013, 22, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Horn-Ross, P.L.; Canchola, A.J.; Bernstein, L.; Clarke, C.A.; Lacey, J.V.; Neuhausen, S.L.; Reynolds, P.; Ursin, G. Alcohol consumption and breast cancer risk among postmenopausal women following the cessation of hormone therapy use: The California teachers study. Cancer Epidemiol. Biomark. 2012, 21, 2006–2013. [Google Scholar] [CrossRef] [PubMed]
- Holm, M.; Olsen, A.; Christensen, J.; Kroman, N.T.; Bidstrup, P.E.; Johansen, C.; Overvad, K.; Tjonneland, A. Pre-diagnostic alcohol consumption and breast cancer recurrence and mortality: Results from a prospective cohort with a wide range of variation in alcohol intake. Int. J. Cancer 2013, 132, 686–694. [Google Scholar] [CrossRef] [PubMed]
- Newcomb, P.A.; Kampman, E.; Trentham-Dietz, A.; Egan, K.M.; Titus, L.J.; Baron, J.A.; Hampton, J.M.; Passarelli, M.N.; Willett, W.C. Alcohol consumption before and after breast cancer diagnosis: Associations with survival from breast cancer, cardiovascular disease, and other causes. J. Clin. Oncol. 2013, 31, 1939. [Google Scholar] [CrossRef] [PubMed]
- Lucenteforte, E.; La Vecchia, C.; Silverman, D.; Petersen, G.M.; Bracci, P.M.; Ji, B.T.; Bosetti, C.; Li, D.; Gallinger, S.; Miller, A.B.; et al. Alcohol consumption and pancreatic cancer: A pooled analysis in the International Pancreatic Cancer Case-Control Consortium (PanC4). Ann. Oncol. 2012, 23, 353–374. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.A.; Zolotarevsky, E.; Cooper, K.L.; Sherman, S.; Shats, O.; Whitcomb, D.C.; Lynch, H.T.; Ghiorzo, P.; Rubinstein, W.S.; Vogel, K.J.; et al. Alcohol and tobacco lower the age of presentation in sporadic pancreatic cancer in a dose-dependent manner: A multicenter study. Am. J. Gastroenterol. 2012, 107, 1730–1739. [Google Scholar] [CrossRef] [PubMed]
- Murugan, S.; Zhang, C.Q.; Mojtahedzadeh, S.; Sarkar, D.K. Alcohol exposure in utero increases susceptibility to prostate tumorigenesis in rat offspring. Alcohol. Clin. Exp. Res. 2013, 37, 1901–1909. [Google Scholar] [CrossRef] [PubMed]
- McGregor, S.E.; Courneya, K.S.; Kopciuk, K.A.; Tosevski, C.; Friedenreich, C.M. Case-control study of lifetime alcohol intake and prostate cancer risk. Cancer Cause Control 2013, 24, 451–461. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.Y.; Kim, M.K.; Seo, S.; Lee, D.O.; Chung, Y.K.; Lim, M.C.; Kim, J.; Lee, C.W.; Park, S. Alcohol consumption and persistent infection of high-risk human papillomavirus. Epidemiol. Infect. 2015, 143, 1442–1450. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.Y.; Seo, S.S.; Kim, M.K.; Lee, D.O.; Chung, Y.K.; Lim, M.C.; Kim, J.Y.; Lee, C.W.; Park, S.Y. Synergistic effect of viral load and alcohol consumption on the risk of persistent high-risk human papillomavirus infection. PLoS ONE 2014, 9, e104374. [Google Scholar] [CrossRef] [PubMed]
- Min, K.J.; Lee, J.K.; Lee, S.; Kim, M.K. Alcohol consumption and viral load are synergistically associated with CIN1. PLoS ONE 2013, 8, e72142. [Google Scholar] [CrossRef] [PubMed]
- Friedenreich, C.M.; Speidel, T.P.; Neilson, H.K.; Langley, A.R.; Courneya, K.S.; Magliocco, A.M.; Cook, L.S. Case-control study of lifetime alcohol consumption and endometrial cancer risk. Cancer Cause Control 2013, 24, 1995–2003. [Google Scholar] [CrossRef] [PubMed]
- Everatt, R.; Tamosiunas, A.; Kuzmickiene, I.; Virviciute, D.; Radisauskas, R.; Reklaitiene, R.; Milinaviciene, E. Alcohol consumption and risk of gastric cancer: A cohort study of men in Kaunas, Lithuania, with up to 30 years follow-up. BMC Cancer 2012, 12, 475. [Google Scholar] [CrossRef] [PubMed]
- Kubo, J.T.; Henderson, M.T.; Desai, M.; Wactawski-Wende, J.; Stefanick, M.L.; Tang, J.Y. Alcohol consumption and risk of melanoma and non-melanoma skin cancer in the Women’s Health Initiative. Cancer Cause Control 2014, 25, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.; Birch-Johansen, F.; Olesen, A.B.; Christensen, J.; Tjonneland, A.; Kjaer, S.K. Intake of alcohol may modify the risk for non-melanoma skin cancer: Results of a large danish prospective cohort study. J. Investig. Dermatol. 2012, 132, 2718–2726. [Google Scholar] [CrossRef] [PubMed]
- Song, D.Y.; Song, S.; Song, Y.; Lee, J.E. Alcohol intake and renal cell cancer risk: A meta-analysis. Br. J. Cancer 2012, 106, 1881–1890. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Alonso, S.; Collins, V.J.; Vauzour, D.; Rodríguez-Mateos, A.; Corona, G.; Spencer, J.P.E. Inhibition of colon adenocarcinoma cell proliferation by flavonols is linked to a G2/M cell cycle block and reduction in cyclin D1 expression. Food Chem. 2012, 130, 493–500. [Google Scholar] [CrossRef]
- Wallenborg, K.; Vlachos, P.; Eriksson, S.; Huijbregts, L.; Arnér, E.S.J.; Joseph, B.; Hermanson, O. Red wine triggers cell death and thioredoxin reductase inhibition: Effects beyond resveratrol and SIRT1. Exp. Cell Res. 2009, 315, 1360–1371. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Kim, Y.J.; Park, H.J.; Chung, J.H.; Leem, K.H.; Kim, H.K. Apoptotic effect of red wine polyphenols on human colon cancer SNU-C4 cells. Food Chem. Toxicol. 2006, 44, 898–902. [Google Scholar] [CrossRef] [PubMed]
- Sharif, T.; Auger, C.; Alhosin, M.; Ebel, C.; Achour, M.; Étienne-Selloum, N.; Fuhrmann, G.; Bronner, C.; Schini-Kerth, V.B. Red wine polyphenols cause growth inhibition and apoptosis in acute lymphoblastic leukaemia cells by inducing a redox-sensitive up-regulation of p73 and down-regulation of UHRF1. Eur. J. Cancer 2010, 46, 983–994. [Google Scholar] [CrossRef] [PubMed]
- Mertens-Talcott, S.U.; Percival, S.S.; Talcott, S.T. Extracts from red muscadine and cabernet sauvignon wines induce cell death in MOLT-4 human leukemia cells. Food Chem. 2008, 108, 824–832. [Google Scholar] [CrossRef] [PubMed]
- Sharif, T.; Auger, C.; Bronner, C.; Alhosin, M.; Klein, T.; Etienne-Selloum, N.; Schini-Kerth, V.B.; Fuhrmann, G. Selective proapoptotic activity of polyphenols from red wine on teratocarcinoma cell, a model of cancer stem-like cell. Investig. New Drug 2011, 29, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, R.; Azevedo, I.; Calhau, C. Modulation of aromatase activity by diet polyphenolic compounds. J. Agric. Food Chem. 2006, 54, 3535–3540. [Google Scholar] [CrossRef] [PubMed]
- Mazué, F.; Delmas, D.; Murillo, G.; Saleiro, D.; Limagne, E.; Latruffe, N. Differential protective effects of red wine polyphenol extracts (RWEs) on colon carcinogenesis. Food Funct. 2014, 5, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Hakimuddin, F.; Tiwari, K.; Paliyath, G.; Meckling, K. Grape and wine polyphenols down-regulate the expression of signal transduction genes and inhibit the growth of estrogen receptor–negative MDA-MB231 tumors in nu/nu mouse xenografts. Nutr. Res. 2008, 28, 702–713. [Google Scholar] [CrossRef] [PubMed]
- Vo, N.T.P.; Madlener, S.; Bago-Horvath, Z.; Herbacek, I.; Stark, N.; Gridling, M.; Probst, P.; Giessrigl, B.; Bauer, S.; Vonach, C.; et al. Pro- and anticarcinogenic mechanisms of piceatannol are activated dose dependently in MCF-7 breast cancer cells. Carcinogenesis 2010, 31, 2074–2081. [Google Scholar] [CrossRef] [PubMed]
- Touvier, M.; Druesne-Pecollo, N.; Kesse-Guyot, E.; Andreeva, V.A.; Fezeu, L.; Galan, P.; Hercberg, S.; Latino-Martel, P. Dual association between polyphenol intake and breast cancer risk according to alcohol consumption level: A prospective cohort study. Breast Cancer Res. Treat. 2013, 137, 225–236. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.K.; Larsen, S.B.; Jensen, D.M.; Christensen, J.; Olsen, A.; Loft, S.; Nellemann, C.; Overvad, K.; Kristiansen, K.; Tjonneland, A.; et al. PPARgamma-PGC-1alpha activity is determinant of alcohol related breast cancer. Cancer Lett. 2012, 315, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, S.; Peeters, P.H.M.; Bezemer, I.D.; Dossus, L.; Biessy, C.; Sacerdote, C.; Berrino, F.; Panico, S.; Palli, D.; Tumino, R.; et al. Relationship of alcohol intake and sex steroid concentrations in blood in pre- and post-menopausal women: The European Prospective Investigation into Cancer and Nutrition. Cancer Cause Control 2006, 17, 1033–1043. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.W.; Dunlap, S.M.; Holcomb, V.B.; Nunez, N.P. Alcohol promotes mammary tumor development via the estrogen pathway in estrogen receptor alpha-negative HER2/neu mice. Alcohol. Clin. Exp. Res. 2012, 36, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Chan, I.S.; Guy, C.D.; Machado, M.V.; Wank, A.; Kadiyala, V.; Michelotti, G.; Choi, S.; Swiderska-Syn, M.; Karaca, G.; Pereira, T.A.; et al. Alcohol activates the Hedgehog pathway and induces related procarcinogenic processes in the alcohol-preferring rat model of hepatocarcinogenesis. Alcohol. Clin. Exp. Res. 2014, 38, 787–800. [Google Scholar] [CrossRef] [PubMed]
- Pavanello, S.; Hoxha, M.; Dioni, L.; Bertazzi, P.A.; Snenghi, R.; Nalesso, A.; Ferrara, S.D.; Montisci, M.; Baccarelli, A. Shortened telomeres in individuals with abuse in alcohol consumption. Int. J. Cancer 2011, 129, 983–992. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.W.; Mason, J.B. Folate and carcinogenesis: An integrated scheme. J. Nutr. 2000, 130, 129–132. [Google Scholar] [PubMed]
- Lemos, C.; Peters, G.J.; Jansen, G.; Martel, F.; Calhau, C. Modulation of folate uptake in cultured human colon adenocarcinoma Caco-2 cells by dietary compounds. Eur. J. Nutr. 2007, 46, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Forsyth, C.B.; Tang, Y.; Shaikh, M.; Zhang, L.; Keshavarzian, A. Alcohol stimulates activation of Snail, epidermal growth factor receptor signaling, and biomarkers of epithelial-mesenchymal transition in colon and breast cancer cells. Alcohol. Clin. Exp. Res. 2010, 34, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.W.; Paulson, Q.X.; Hong, J.; Stubbins, R.E.; Poh, K.; Schrader, E.; Nunez, N.P. Alcohol promotes breast cancer cell invasion by regulating the Nm23-ITGA5 pathway. J. Exp. Clin. Cancer Res. 2011, 30, 75. [Google Scholar] [CrossRef] [PubMed]
- Wimberly, A.L.; Forsyth, C.B.; Khan, M.W.; Pemberton, A.; Khazaie, K.; Keshavarzian, A. Ethanol-induced mast cell-mediated inflammation leads to increased susceptibility of intestinal tumorigenesis in the APC (Delta 468) min mouse model of colon cancer. Alcohol. Clin. Exp. Res. 2013, 371, E199–E208. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Xu, M.; Li, F.; Wang, X.; Bower, K.A.; Frank, J.A.; Lu, Y.; Chen, G.; Zhang, Z.; Ke, Z.; et al. Ethanol promotes mammary tumor growth and angiogenesis: The involvement of chemoattractant factor MCP-1. Breast Cancer Res. Treat. 2012, 133, 1037–1048. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Yang, J.; Yu, K.; Xu, M.; Xu, Y.; Chen, L.; Lu, Y.; Fang, H.; Wang, X.; Hu, Z.; et al. Activation of the NF-κB pathway as a mechanism of alcohol enhanced progression and metastasis of human hepatocellular carcinoma. Mol. Cancer 2015, 14, 10. [Google Scholar] [CrossRef] [PubMed]
- Darvin, M.E.; Sterry, W.; Lademann, J.; Patzelt, A. Alcohol consumption decreases the protection efficiency of the antioxidant network and increases the risk of sunburn in human skin. Skin Pharmacol. Phys. 2013, 26, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Lachenmeier, D.W.; Sohnius, E. The role of acetaldehyde outside ethanol metabolism in the carcinogenicity of alcoholic beverages: Evidence from a large chemical survey. Food Chem. Toxicol. 2008, 46, 2903–2911. [Google Scholar] [CrossRef] [PubMed]
- Lachenmeier, D.W.; Monakhova, Y.B. Short-term salivary acetaldehyde increase due to direct exposure to alcoholic beverages as an additional cancer risk factor beyond ethanol metabolism. J. Exp. Clin. Cancer Res. 2011, 30, 3. [Google Scholar] [CrossRef] [PubMed]
- Fanelli, S.L.; Maciel, M.E.; Diaz Gomez, M.I.; Delgado De Layno, A.M.A.; Bietto, F.M.; Castro, J.A.; Castro, G.D. Further studies on the potential contribution of acetaldehyde accumulation and oxidative stress in rat mammary tissue in the alcohol drinking promotion of breast cancer. J. Appl. Toxicol. 2011, 31, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.J.; Wang, F.; Zhou, Y.; Li, Y.; Zhou, T.; Zheng, J.; Zhang, J.J.; Li, S.; Xu, D.P.; Li, H.B. Effects of 20 selected fruits on ethanol metabolism: Potential health benefits and harmful impacts. Int. J. Environ. Res. Public Health 2016, 13, 399. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Gan, L.Q.; Li, S.K.; Zheng, J.C.; Xu, D.P.; Li, H.B. Effects of herbal infusions, tea and carbonated beverages on alcohol dehydrogenase and aldehyde dehydrogenase activity. Food Funct. 2014, 5, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Li, Y.; Zhang, Y.J.; Zhou, Y.; Li, S.; Li, H.B. Natural products for the prevention and treatment of hangover and alcohol use disorder. Molecules 2016, 21, 64. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Zhang, Y.J.; Zhou, Y.; Li, Y.; Zhou, T.; Zheng, J.; Zhang, J.J.; Li, S.; Xu, D.P.; Li, H.B. Effects of beverages on alcohol metabolism: Potential health benefits and harmful impacts. Int. J. Mol. Sci. 2016, 17, 354. [Google Scholar] [CrossRef] [PubMed]
- Nurmi, K.; Virkanen, J.; Rajamaki, K.; Niemi, K.; Kovanen, P.T.; Eklund, K.K. Ethanol inhibits activation of NLRP3 and AIM2 inflammasomes in human macrophages-a novel anti-inflammatory action of alcohol. PLoS ONE 2013, 8, e78537. [Google Scholar] [CrossRef] [PubMed]
- Rantakomi, S.H.; Laukkanen, J.A.; Sivenius, J.; Kauhanen, J.; Kurl, S. Hangover and the risk of stroke in middle-aged men. Acta Neurol. Scand. 2013, 127, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Roerecke, M.; Rehm, J. Alcohol consumption, drinking patterns, and ischemic heart disease: A narrative review of meta-analyses and a systematic review and meta-analysis of the impact of heavy drinking occasions on risk for moderate drinkers. BMC Med. 2014, 12, 182. [Google Scholar] [CrossRef] [PubMed]
- Dai, J.; Mukamal, K.J.; Krasnow, R.E.; Swan, G.E.; Reed, T. Higher usual alcohol consumption was associated with a lower 41-y mortality risk from coronary artery disease in men independent of genetic and common environmental factors: The prospective NHLBI Twin Study. Am. J. Clin. Nutr. 2015, 102, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Pai, J.K.; Mukamal, K.J.; Rimm, E.B. Long-term alcohol consumption in relation to all-cause and cardiovascular mortality among survivors of myocardial infarction: The Health Professionals Follow-up Study. Eur. Heart J. 2012, 33, 1598–1605. [Google Scholar] [CrossRef] [PubMed]
- Rosenbloom, J.I.; Mukamal, K.J.; Frost, L.E.; Mittleman, M.A. Alcohol consumption patterns, beverage type, and long-term mortality among women survivors of acute myocardial infarction. Am. J. Cardiol. 2012, 109, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Qin, Y.Y.; Chen, Q.; Jiang, H.; Chen, X.Z.; Xu, C.L.; Mao, P.J.; He, J.; Zhou, Y.H. Alcohol intake and risk of stroke: A dose-response meta-analysis of prospective studies. Int. J. Cardiol. 2014, 174, 669–677. [Google Scholar] [CrossRef] [PubMed]
- Rantakomi, S.H.; Kurl, S.; Sivenius, J.; Kauhanen, J.; Laukkanen, J.A. The frequency of alcohol consumption is associated with the stroke mortality. Acta Neurol. Scand. 2014, 130, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Fekete, K.; Szatmari, S.; Szocs, I.; Szekeres, C.; Szasz, J.; Mihalka, L.; Smolanka, V.; Kardos, L.; Csiba, L.; Bereczki, D. Prestroke alcohol consumption and smoking are not associated with stroke severity, disability at discharge, and case fatality. J. Stroke Cerebrovasc. Dis. 2014, 23, e31–e37. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Drca, N.; Wolk, A. Alcohol consumption and risk of atrial fibrillation: A prospective study and dose-response meta-analysis. J. Am. Coll. Cardiol. 2014, 64, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Overvad, T.F.; Rasmussen, L.H.; Skjoth, F.; Overvad, K.; Albertsen, I.E.; Lane, D.A.; Lip, G.Y.; Larsen, T.B. Alcohol intake and prognosis of atrial fibrillation. Heart 2013, 99, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Briasoulis, A.; Agarwal, V.; Messerli, F.H. Alcohol consumption and the risk of hypertension in men and women: A systematic review and meta-analysis. J. Clin. Hypertens. 2012, 14, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Zhan, J.; Liu, Y.J.; Li, D.J.; Wang, S.Q.; He, Q.Q. Association between alcohol consumption and risk of cardiovascular disease and all-cause mortality in patients with hypertension: A meta-analysis of prospective cohort studies. Mayo Clin. Proc. 2014, 89, 1201–1210. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, A.; Claggett, B.; Jhund, P.S.; Rosamond, W.; Deswal, A.; Aguilar, D.; Shah, A.M.; Cheng, S.; Solomon, S.D. Alcohol consumption and risk of heart failure: The Atherosclerosis Risk in Communities Study. Eur. Heart J. 2015, 36, 939–945. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Orsini, N.; Wolk, A. Alcohol consumption and risk of heart failure: A dose-response meta-analysis of prospective studies. Eur. J. Heart Fail. 2015, 17, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Dorans, K.S.; Mostofsky, E.; Levitan, E.B.; Hakansson, N.; Wolk, A.; Mittleman, M.A. Alcohol and incident heart failure among middle-aged and elderly men: Cohort of Swedish men. Circ. Heart Fail. 2015, 8, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Gargiulo, G.; Testa, G.; Cacciatore, F.; Mazzella, F.; Galizia, G.; Della-Morte, D.; Langellotto, A.; Pirozzi, G.; Ferro, G.; Ferrara, N.; et al. Moderate alcohol consumption predicts long-term mortality in elderly subjects with chronic heart failure. J. Nutr. Health Aging 2013, 17, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Toda, N.; Ayajiki, K. Vascular actions of nitric oxide as affected by exposure to alcohol. Alcohol Alcohol. 2010, 45, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Emel’Yanov, M.O.; Korystova, A.F.; Kublik, L.N.; Levitman, M.; Shaposhnikova, V.V.; Korystov, Y.N. Low doses of ethanol decrease the activity of the angiotensin-converting enzyme in the aorta of aging rats and rats treated with a nitric oxide synthase inhibitor and dexamethasone. Clin. Sci. 2012, 122, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Elmadhun, N.Y.; Sabe, A.A.; Lassaletta, A.D.; Sellke, F.W. Ethanol promotes new vessel growth in remote nonischemic myocardium. J. Surg. Res. 2015, 193, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Elmadhun, N.Y.; Sabe, A.A.; Lassaletta, A.D.; Sellke, F.W. Alcohol consumption mitigates apoptosis and mammalian target of rapamycin signaling in myocardium. J. Am. Coll. Surg. 2014, 218, 1175–1181. [Google Scholar] [CrossRef] [PubMed]
- Roerecke, M.; Rehm, J. The cardioprotective association of average alcohol consumption and ischaemic heart disease: A systematic review and meta-analysis. Addiction 2012, 107, 1246–1260. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.; McMillan, M.R.; Jones, R.W.; Kowalik, G.T.; Steeden, J.A.; Pruessner, J.C.; Taylor, A.M.; Deanfield, J.E.; Muthurangu, V. Habitual alcohol consumption is associated with lower cardiovascular stress responses—A novel explanation for the known cardiovascular benefits of alcohol? Stress 2013, 16, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Xiong, W.; Arrick, D.M.; Mayhan, W.G. Low-dose alcohol consumption protects against transient focal cerebral ischemia in mice: Possible role of PPARgamma. PLoS ONE 2012, 7, e41716. [Google Scholar] [CrossRef] [PubMed]
- Tsang, C.; Higgins, S.; Duthie, G.G.; Duthie, S.J.; Howie, M.; Mullen, W.; Lean, M.E.J.; Crozier, A. The influence of moderate red wine consumption on antioxidant status and indices of oxidative stress associated with CHD in healthy volunteers. Br. J. Nutr. 2005, 93, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Sacanella, E.; Mota, F.; Chiva-Blanch, G.; Antunez, E.; Casals, E.; Deulofeu, R.; Rotilio, D.; Andres-Lacueva, C.; Lamuela-Raventos, R.M.; et al. Moderate consumption of red wine, but not gin, decreases erythrocyte superoxide dismutase activity: A randomised cross-over trial. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.H.; Tsai, H.Y.; Wang, C.H.; Chen, Y.H.; Chen, J.S.; Lin, F.Y.; Lin, C.P.; Wu, T.C.; Sata, M.; Chen, J.W.; et al. Moderate intake of red wine improves ischemia-induced neovascularization in diabetic mice—Roles of endothelial progenitor cells and nitric oxide. Atherosclerosis 2010, 212, 426–435. [Google Scholar] [CrossRef] [PubMed]
- Kurin, E.; Atanasov, A.G.; Donath, O.; Heiss, E.H.; Dirsch, V.M.; Nagy, M. Synergy study of the inhibitory potential of red wine polyphenols on vascular smooth muscle cell proliferation. Planta Med. 2012, 78, 772–778. [Google Scholar] [CrossRef] [PubMed]
- Chiva-Blanch, G.; Urpi-Sarda, M.; Ros, E.; Arranz, S.; Valderas-Martinez, P.; Casas, R.; Sacanella, E.; Llorach, R.; Lamuela-Raventos, R.M.; Andres-Lacueva, C.; et al. Dealcoholized red wine decreases systolic and diastolic blood pressure and increases plasma nitric oxide: Short communication. Circ. Res. 2012, 111, 1065–1068. [Google Scholar] [CrossRef] [PubMed]
- Luciano, M.N.; Ribeiro, T.P.; Franca-Silva, M.S.; Do, N.R.; de Jesus, O.E.; Franca, K.C.; Antunes, A.A.; Nakao, L.S.; Aita, C.A.; Braga, V.A.; et al. Uncovering the vasorelaxant effect induced by Vale do Sao Francisco red wine: A role for nitric oxide. J. Cardiovasc. Pharmacol. 2011, 57, 696–701. [Google Scholar] [CrossRef] [PubMed]
- Auger, C.; Chaabi, M.; Anselm, E.; Lobstein, A.; Schini-Kerth, V.B. The red wine extract-induced activation of endothelial nitric oxide synthase is mediated by a great variety of polyphenolic compounds. Mol. Nutr. Food Res. 2010, 54 (Suppl. 2), S171–S183. [Google Scholar] [CrossRef] [PubMed]
- Gresele, P.; Pignatelli, P.; Guglielmini, G.; Carnevale, R.; Mezzasoma, A.M.; Ghiselli, A.; Momi, S.; Violi, F. Resveratrol, at concentrations attainable with moderate wine consumption, stimulates human platelet nitric oxide production. J. Nutr. 2008, 138, 1602–1608. [Google Scholar] [PubMed]
- Vilahur, G.; Casani, L.; Mendieta, G.; Lamuela-Raventos, R.M.; Estruch, R.; Badimon, L. Beer elicits vasculoprotective effects through Akt/eNOS activation. Eur. J. Clin. Investig. 2014, 44, 1177–1188. [Google Scholar] [CrossRef] [PubMed]
- Chiva-Blanch, G.; Magraner, E.; Condines, X.; Valderas-Martinez, P.; Roth, I.; Arranz, S.; Casas, R.; Navarro, M.; Hervas, A.; Siso, A.; et al. Effects of alcohol and polyphenols from beer on atherosclerotic biomarkers in high cardiovascular risk men: A randomized feeding trial. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Martinez, A.J.; Belles, V.V.; Lopez-Jaen, A.B.; Marin, A.V.; Codoner-Franch, P. Effects of alcohol-free beer on lipid profile and parameters of oxidative stress and inflammation in elderly women. Nutrition 2009, 25, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Crestani, C.C.; Lopes, D.S.A.; Scopinho, A.A.; Ruginsk, S.G.; Uchoa, E.T.; Correa, F.M.; Elias, L.L.; Antunes-Rodrigues, J.; Resstel, L.B. Cardiovascular alterations at different stages of hypertension development during ethanol consumption: Time-course of vascular and autonomic changes. Toxicol. Appl. Pharmacol. 2014, 280, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Da, S.A.; Ruginsk, S.G.; Uchoa, E.T.; Crestani, C.C.; Scopinho, A.A.; Correa, F.M.; De Martinis, B.S.; Elias, L.L.; Resstel, L.B.; Antunes-Rodrigues, J. Time-course of neuroendocrine changes and its correlation with hypertension induced by ethanol consumption. Alcohol Alcohol. 2013, 48, 495–504. [Google Scholar]
- Shirpoor, A.; Salami, S.; Khadem-Ansari, M.H.; Heshmatian, B.; Ilkhanizadeh, B. Long-term ethanol consumption initiates atherosclerosis in rat aorta through inflammatory stress and endothelial dysfunction. Vascul. Pharmacol. 2012, 57, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Shirpoor, A.; Salami, S.; Khadem, A.M.; Ilkhanizadeh, B.; Abdollahzadeh, N. Ethanol promotes rat aortic vascular smooth muscle cell proliferation via increase of homocysteine and oxidized-low-density lipoprotein. J. Cardiol. 2013, 62, 374–378. [Google Scholar] [CrossRef] [PubMed]
- Oros, M.; Zavaczki, E.; Vadasz, C.; Jeney, V.; Tosaki, A.; Lekli, I.; Balla, G.; Nagy, L.; Balla, J. Ethanol increases phosphate-mediated mineralization and osteoblastic transformation of vascular smooth muscle cells. J. Cell. Mol. Med. 2012, 16, 2219–2226. [Google Scholar] [CrossRef] [PubMed]
- Jing, L.; Jin, C.M.; Li, S.S.; Zhang, F.M.; Yuan, L.; Li, W.M.; Sang, Y.; Li, S.; Zhou, L.J. Chronic alcohol intake-induced oxidative stress and apoptosis: Role of CYP2E1 and calpain-1 in alcoholic cardiomyopathy. Mol. Cell. Biochem. 2012, 359, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Qi, Q.; Liu, X.; Zhang, G.; He, W.; Ma, R.; Cong, B.; Li, Y. Morphological changes of cerebral vessels and expression patterns of MMP-2 and MMP-9 on cerebrovascular wall of alcoholic rats. Int. J. Clin. Exp. Pathol. 2014, 7, 1880–1888. [Google Scholar] [PubMed]
- Zoechling, A.; Liebner, F.; Jungbauer, A. Red wine: A source of potent ligands for peroxisome proliferator-activated receptor gamma. Food Funct. 2011, 2, 28–38. [Google Scholar] [CrossRef] [PubMed]
- Pazzini, C.E.; Colpo, A.C.; Poetini, M.R.; Pires, C.F.; de Camargo, V.B.; Mendez, A.S.; Azevedo, M.L.; Soares, J.C.; Folmer, V. Effects of Red Wine Tannat on Oxidative Stress Induced by Glucose and Fructose in Erythrocytes in Vitro. Int. J. Med. Sci. 2015, 12, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Knott, C.; Bell, S.; Britton, A. Alcohol consumption and the risk of Type 2 diabetes: A systematic review and dose-response meta-analysis of more than 1.9 million individuals from 38 observational studies. Diabetes Care 2015, 38, 1804–1812. [Google Scholar] [CrossRef] [PubMed]
- Koloverou, E.; Panagiotakos, D.B.; Pitsavos, C.; Chrysohoou, C.; Georgousopoulou, E.N.; Metaxa, V.; Stefanadis, C. Effects of alcohol consumption and the metabolic syndrome on 10-year incidence of diabetes: The ATTICA study. Diabetes Metab. 2015, 41, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Gepner, Y.; Golan, R.; Harman-Boehm, I.; Henkin, Y.; Schwarzfuchs, D.; Shelef, I.; Durst, R.; Kovsan, J.; Bolotin, A.; Leitersdorf, E.; et al. Effects of initiating moderate alcohol intake on cardiometabolic risk in adults with Type 2 diabetes: A 2-year randomized, controlled trial. Ann. Intern. Med. 2015, 163, 569–579. [Google Scholar] [CrossRef] [PubMed]
- Schrieks, I.C.; Heil, A.L.; Hendriks, H.F.; Mukamal, K.J.; Beulens, J.W. The effect of alcohol consumption on insulin sensitivity and glycemic status: A systematic review and meta-analysis of intervention studies. Diabetes Care 2015, 38, 723–732. [Google Scholar] [PubMed]
- Seshasai, S.R.; Kaptoge, S.; Thompson, A.; Di Angelantonio, E.; Gao, P.; Sarwar, N.; Whincup, P.H.; Mukamal, K.J.; Gillum, R.F.; Holme, I.; et al. Diabetes mellitus, fasting glucose, and risk of cause-specific death. N. Engl. J. Med. 2011, 364, 829–841. [Google Scholar] [PubMed]
- Liu, M.; Yin, H.; Liu, G.; Dong, J.; Qian, Z.; Miao, J. Xanthohumol, a prenylated chalcone from beer hops, acts as an alpha-glucosidase inhibitor in vitro. J. Agric. Food Chem. 2014, 62, 5548–5554. [Google Scholar] [CrossRef] [PubMed]
- Costa, R.; Negrao, R.; Valente, I.; Castela, A.; Duarte, D.; Guardao, L.; Magalhaes, P.J.; Rodrigues, J.A.; Guimaraes, J.T.; Gomes, P.; et al. Xanthohumol modulates inflammation, oxidative stress, and angiogenesis in type 1 diabetic rat skin wound healing. J. Nat. Prod. 2013, 76, 2047–2053. [Google Scholar] [CrossRef] [PubMed]
- Buschard, K.; Hansen, A.K.; Jensen, K.; Lindenbergh-Kortleve, D.J.; de Ruiter, L.F.; Krohn, T.C.; Hufeldt, M.R.; Vogensen, F.K.; Aasted, B.; Osterbye, T.; et al. Alcohol facilitates CD1d loading, subsequent activation of NKT cells, and reduces the incidence of diabetes in NOD mice. PLoS ONE 2011, 6, e17931. [Google Scholar] [CrossRef] [PubMed]
- Schaller, G.; Kretschmer, S.; Gouya, G.; Haider, D.G.; Mittermayer, F.; Riedl, M.; Wagner, O.; Pacini, G.; Wolzt, M.; Ludvik, B. Alcohol acutely increases vascular reactivity together with insulin sensitivity in type 2 diabetic men. Exp. Clin. Endocrinol. Diabetes 2010, 118, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Paulson, Q.X.; Hong, J.; Holcomb, V.B.; Nunez, N.P. Effects of body weight and alcohol consumption on insulin sensitivity. Nutr. J. 2010, 9, 14. [Google Scholar] [CrossRef] [PubMed]
- Fromenty, B.; Vadrot, N.; Massart, J.; Turlin, B.; Barri-Ova, N.; Letteron, P.; Fautrel, A.; Robin, M.A. Chronic ethanol consumption lessens the gain of body weight, liver triglycerides, and diabetes in obese ob/ob mice. J. Pharmacol. Exp. Ther. 2009, 331, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Imhof, A.; Plamper, I.; Maier, S.; Trischler, G.; Koenig, W. Effect of drinking on adiponectin in healthy men and women: A randomized intervention study of water, ethanol, red wine, and beer with or without alcohol. Diabetes Care 2009, 32, 1101–1103. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.F.; Zhang, G.J.; Wang, L.; Kang, P.F.; Li, J.; Wang, H.J.; Gao, Q.; Chen, Y.Q. Ethanol at low concentration attenuates diabetes induced lung injury in rats model. J. Diabetes Res. 2014, 2014, 107152. [Google Scholar] [CrossRef] [PubMed]
- Drel, V.R.; Sybirna, N. Protective effects of polyphenolics in red wine on diabetes associated oxidative/nitrative stress in streptozotocin-diabetic rats. Cell Biol. Int. 2010, 34, 1147–1153. [Google Scholar] [CrossRef] [PubMed]
- Chiva-Blanch, G.; Urpi-Sarda, M.; Ros, E.; Valderas-Martinez, P.; Casas, R.; Arranz, S.; Guillen, M.; Lamuela-Raventos, R.M.; Llorach, R.; Andres-Lacueva, C.; et al. Effects of red wine polyphenols and alcohol on glucose metabolism and the lipid profile: A randomized clinical trial. Clin. Nutr. 2013, 32, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Obara, K.; Mizutani, M.; Hitomi, Y.; Yajima, H.; Kondo, K. Isohumulones, the bitter component of beer, improve hyperglycemia and decrease body fat in Japanese subjects with prediabetes. Clin. Nutr. 2009, 28, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Shimomura, T.; Wakabayashi, I. Inverse associations between light-to-moderate alcohol intake and lipid-related indices in patients with diabetes. Cardiovasc. Diabetol. 2013, 12, 104. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, F.; Disse, E.; Laville, M.; Mari, A.; Hojlund, K.; Anderwald, C.H.; Piatti, P.; Balkau, B. Moderate alcohol consumption is associated with improved insulin sensitivity, reduced basal insulin secretion rate and lower fasting glucagon concentration in healthy women. Diabetologia 2012, 55, 3228–3237. [Google Scholar] [CrossRef] [PubMed]
- He, Z.; Li, M.; Zheng, D.; Chen, Q.; Liu, W.; Feng, L. Adipose tissue hypoxia and low-grade inflammation: A possible mechanism for ethanol-related glucose intolerance? Br. J. Nutr. 2015, 113, 1355–1364. [Google Scholar] [CrossRef] [PubMed]
- Meng, Z.; Bao, X.; Zhang, M.; Wei, S.; Chang, W.; Li, J.; Chen, L.; Nyomba, B.L. Alteration of 11beta-hydroxysteroid dehydrogenase type 1 and glucocorticoid receptor by ethanol in rat liver and mouse hepatoma cells. J. Diabetes Res. 2013, 2013, 218102. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Ju, A.; Lim, S.G.; Kim, D.J. Chronic alcohol consumption, type 2 diabetes mellitus, insulin-like growth factor-I (IGF-I), and growth hormone (GH) in ethanol-treated diabetic rats. Life Sci. 2013, 93, 778–782. [Google Scholar] [CrossRef] [PubMed]
- Gardebjer, E.M.; Anderson, S.T.; Pantaleon, M.; Wlodek, M.E.; Moritz, K.M. Maternal alcohol intake around the time of conception causes glucose intolerance and insulin insensitivity in rat offspring, which is exacerbated by a postnatal high-fat diet. FASEB J. 2015, 29, 2690–2701. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Hwang, J.Y.; Lee, D.Y.; Song, E.H.; Park, K.J.; Kim, G.H.; Jeong, E.A.; Lee, Y.J.; Go, M.J.; Kim, D.J.; et al. Chronic ethanol consumption inhibits glucokinase transcriptional activity by Atf3 and triggers metabolic syndrome in vivo. J. Biol. Chem. 2014, 289, 27065–27079. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S.; Hong, O.K.; Ju, A.; Kim, M.J.; Kim, B.J.; Kim, S.R.; Kim, W.H.; Cho, N.H.; Kang, M.I.; Kang, S.K.; et al. Chronic alcohol consumption results in greater damage to the pancreas than to the liver in the rats. Korean J. Physiol. Pharmacol. 2015, 19, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Dobson, C.C.; Mongillo, D.L.; Brien, D.C.; Stepita, R.; Poklewska-Koziell, M.; Winterborn, A.; Holloway, A.C.; Brien, J.F.; Reynolds, J.N. Chronic prenatal ethanol exposure increases adiposity and disrupts pancreatic morphology in adult guinea pig offspring. Nutr. Diabetes 2012, 2, e57. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.H.; Lee, J.H.; Nyomba, B.L. Ethanol causes endoplasmic reticulum stress and impairment of insulin secretion in pancreatic beta-cells. Alcohol 2012, 46, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Luo, Y.; Feng, A.; Li, T.; Yang, X.; Nofech-Mozes, R.; Yu, M.; Wang, C.; Li, Z.; Yi, F.; et al. Ethanol induced impairment of glucose metabolism involves alterations of GABAergic signaling in pancreatic beta-cells. Toxicology 2014, 326, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Shanmugam, K.R.; Mallikarjuna, K.; Reddy, K.S. Effect of alcohol on blood glucose and antioxidant enzymes in the liver and kidney of diabetic rats. Indian J. Pharmacol. 2011, 43, 330–335. [Google Scholar] [PubMed]
- Wang, K.; Song, H.; Jin, M.; Xiao, H.; Zhao, G.; Zou, H.; Yu, L. Chronic alcohol consumption from adolescence to adulthood in mice-hypothalamic gene expression changes in insulin-signaling pathway. Alcohol 2014, 48, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Shelton, N.J.; Knott, C.S. Association between alcohol calorie intake and overweight and obesity in English adults. Am. J. Public Health 2014, 104, 629–631. [Google Scholar] [CrossRef] [PubMed]
- Bergmann, M.M.; Schutze, M.; Steffen, A.; Boeing, H.; Halkjaer, J.; Tjonneland, A.; Travier, N.; Agudo, A.; Slimani, N.; Rinaldi, S.; et al. The association of lifetime alcohol use with measures of abdominal and general adiposity in a large-scale European cohort. Eur. J. Clin. Nutr. 2011, 65, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Bendsen, N.T.; Christensen, R.; Bartels, E.M.; Kok, F.J.; Sierksma, A.; Raben, A.; Astrup, A. Is beer consumption related to measures of abdominal and general obesity? A systematic review and meta-analysis. Nutr. Rev. 2013, 71, 67–87. [Google Scholar] [CrossRef] [PubMed]
- Brandhagen, M.; Forslund, H.B.; Lissner, L.; Winkvist, A.; Lindroos, A.K.; Carlsson, L.M.; Sjostrom, L.; Larsson, I. Alcohol and macronutrient intake patterns are related to general and central adiposity. Eur. J. Clin. Nutr. 2012, 66, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, I. Age-dependent inverse association between alcohol consumption and obesity in Japanese men. Obesity (Silver Spring) 2011, 19, 1881–1886. [Google Scholar] [CrossRef] [PubMed]
- Thomson, C.A.; Wertheim, B.C.; Hingle, M.; Wang, L.; Neuhouser, M.L.; Gong, Z.; Garcia, L.; Stefanick, M.L.; Manson, J.E. Alcohol consumption and body weight change in postmenopausal women: Results from the Women’s Health Initiative. Int. J. Obes. 2012, 36, 1158–1164. [Google Scholar] [CrossRef] [PubMed]
- Dumesnil, C.; Dauchet, L.; Ruidavets, J.B.; Bingham, A.; Arveiler, D.; Ferrieres, J.; Ducimetiere, P.; Haas, B.; Bongard, V.; Wagner, A.; et al. Alcohol consumption patterns and body weight. Ann. Nutr. Metab. 2013, 62, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, R.; Soares, R.; Guerreiro, S.; Pestana, D.; Calhau, C.; Azevedo, I. Red wine increases adipose tissue aromatase expression and regulates body weight and adipocyte size. Nutrition 2009, 25, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Miranda, C.L.; Elias, V.D.; Hay, J.J.; Choi, J.; Reed, R.L.; Stevens, J.F. Xanthohumol improves dysfunctional glucose and lipid metabolism in diet-induced obese C57BL/6J mice. Arch. Biochem. Biophys. 2016. [Google Scholar] [CrossRef] [PubMed]
- Traversy, G.; Chaput, J.P. Alcohol consumption and obesity: An update. Curr. Obes. Rep. 2015, 4, 122–130. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Cancer Sites | Relative Risks or Odds Ratio for Drinkers | Reference |
|---|---|---|
| Upper aero-digestive tract | less than 12.5 g/day: 1.26 (95% CI, 0.94–1.67); | [17] |
| 12.6 to 49.9 g/day: 1.79 (95% CI, 1.26–2.53); | ||
| more than 50 g/day: 3.63 (95% CI, 2.63–5.00) | ||
| Colorectum | less than 12.5 g/day: 1.07 (95% CI, 1.02–1.13); | [4] |
| 12.6 to 49.9 g/day: 1.23 (95% CI, 1.15–1.32); | ||
| more than 50 g/day: 1.37 (95% CI, 1.26–1.49) | ||
| Liver | less than 37.5 g/day: 0.91 (95% CI, 0.81–1.02); | [18] |
| 37.5 g/day or more: 1.16 (95% CI, 1.01–1.34) | ||
| Breast | 5 to 15 g/day: 1.06 (95% CI, 1.01–1.11); | [19] |
| 15 to 30 g/day: 1.12 (95% CI, 1.06–1.19); | ||
| more than 30 g/day: 1.25 (95% CI, 1.17–1.35) | ||
| Pancreas | less than 37.5 g/day: 0.92 (95% CI, 0.86–0.97); | [20] |
| 37.5 g/day or more: 1.22 (95% CI, 1.12–1.34) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, Y.; Zheng, J.; Li, S.; Zhou, T.; Zhang, P.; Li, H.-B. Alcoholic Beverage Consumption and Chronic Diseases. Int. J. Environ. Res. Public Health 2016, 13, 522. https://doi.org/10.3390/ijerph13060522
Zhou Y, Zheng J, Li S, Zhou T, Zhang P, Li H-B. Alcoholic Beverage Consumption and Chronic Diseases. International Journal of Environmental Research and Public Health. 2016; 13(6):522. https://doi.org/10.3390/ijerph13060522
Chicago/Turabian StyleZhou, Yue, Jie Zheng, Sha Li, Tong Zhou, Pei Zhang, and Hua-Bin Li. 2016. "Alcoholic Beverage Consumption and Chronic Diseases" International Journal of Environmental Research and Public Health 13, no. 6: 522. https://doi.org/10.3390/ijerph13060522
APA StyleZhou, Y., Zheng, J., Li, S., Zhou, T., Zhang, P., & Li, H.-B. (2016). Alcoholic Beverage Consumption and Chronic Diseases. International Journal of Environmental Research and Public Health, 13(6), 522. https://doi.org/10.3390/ijerph13060522