Managing the Health Impacts of Drought in Brazil

Abstract
:
1. Drought, a Silent Public Health Disaster
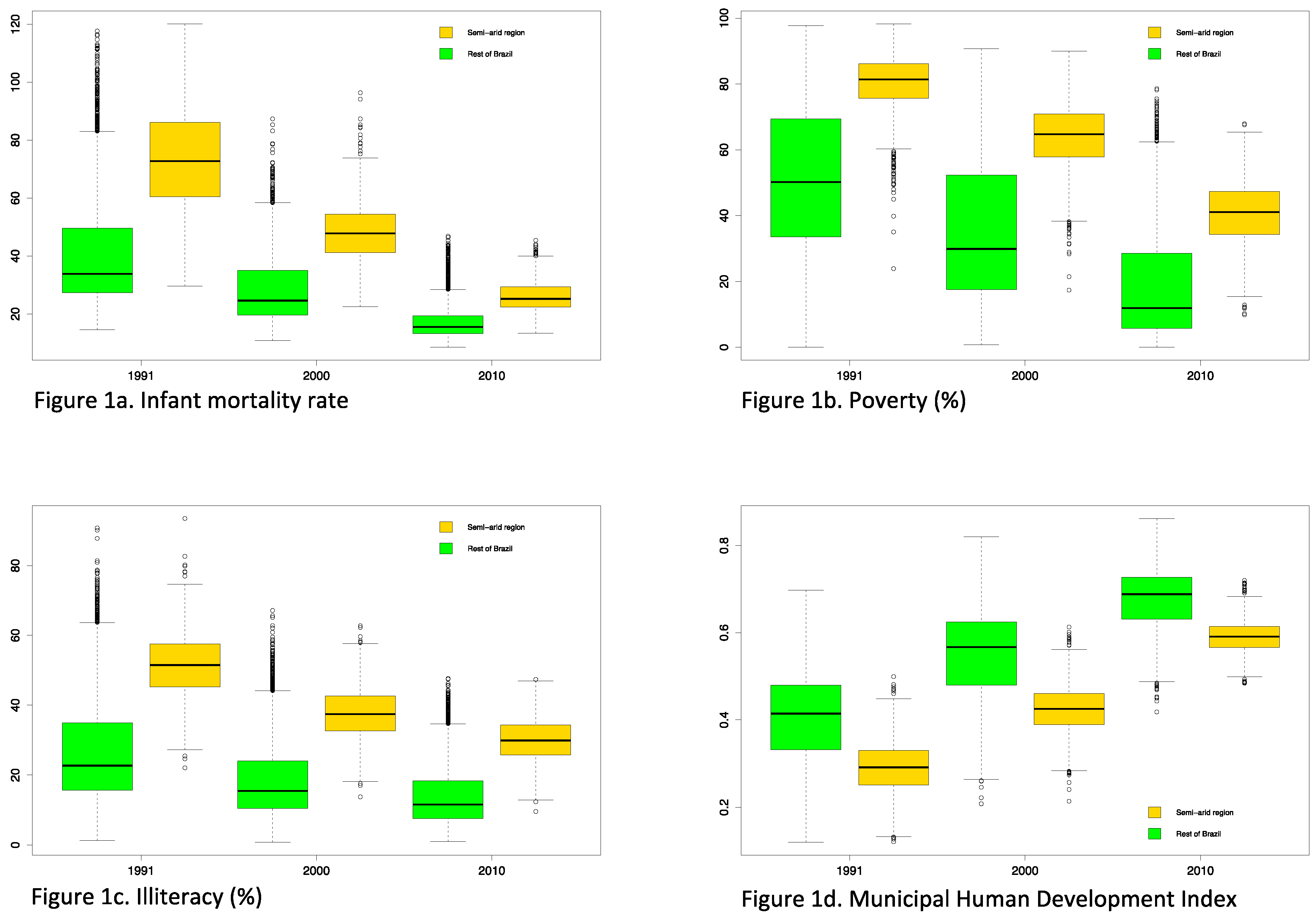
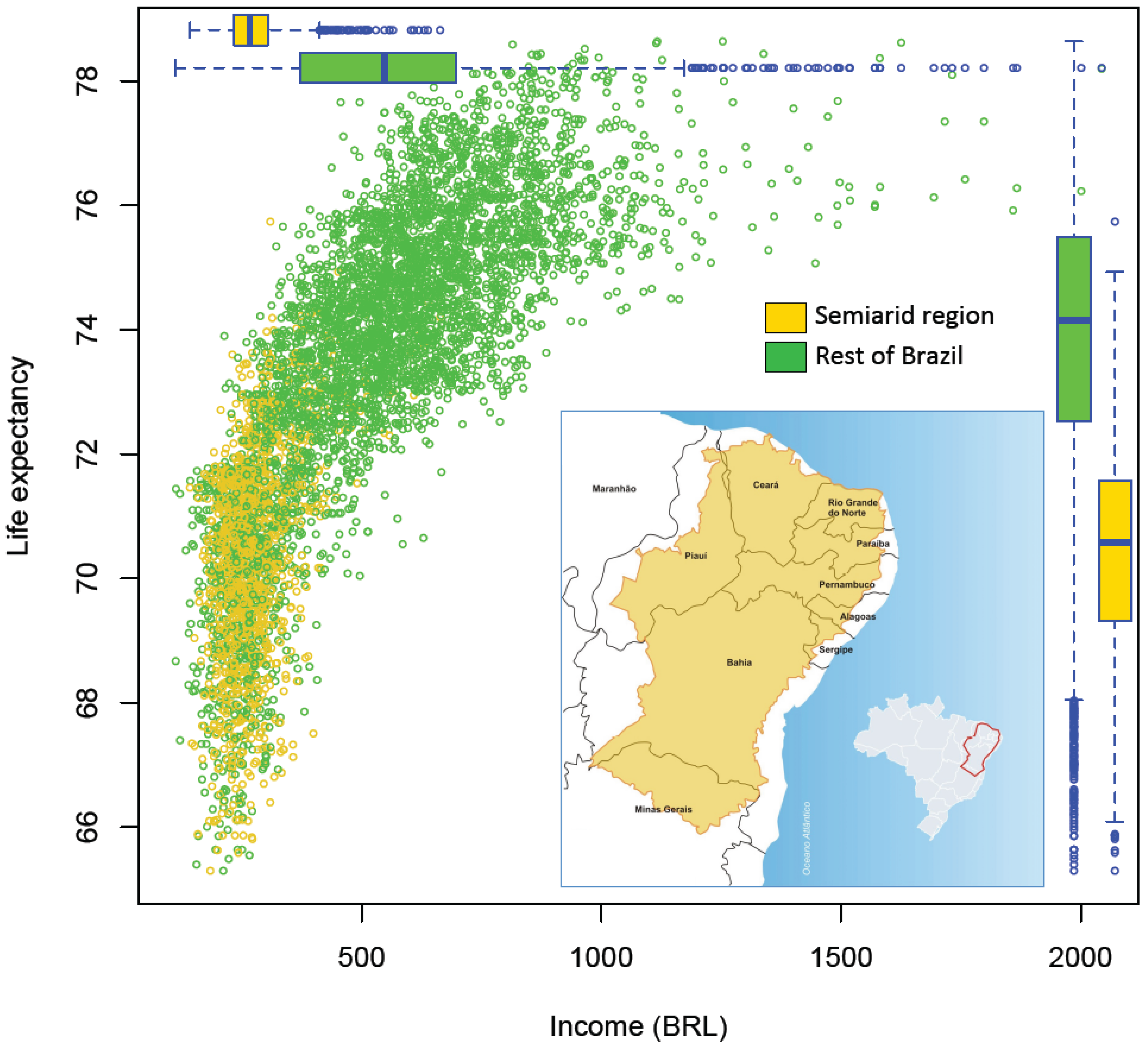
2. Drought Impacts, the Case of Brazil
3. Addressing the Health Impacts of Drought in Brazil

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Systems and services | Human health |
|---|---|
| Access to drinking water (quality and quantity, unsafe water storage, limited water for hygiene) |
|
| Food and nutrition (limited water for food hygiene, reduced or damaged crop yields, reduced health or death of animals and livestock) |
|
| Air quality (dust, drought related wild-fires) |
|
| Basic sanitation and hygiene (limited water for personal hygiene) |
|
| Mental health and behavior |
|
| Health services |
|
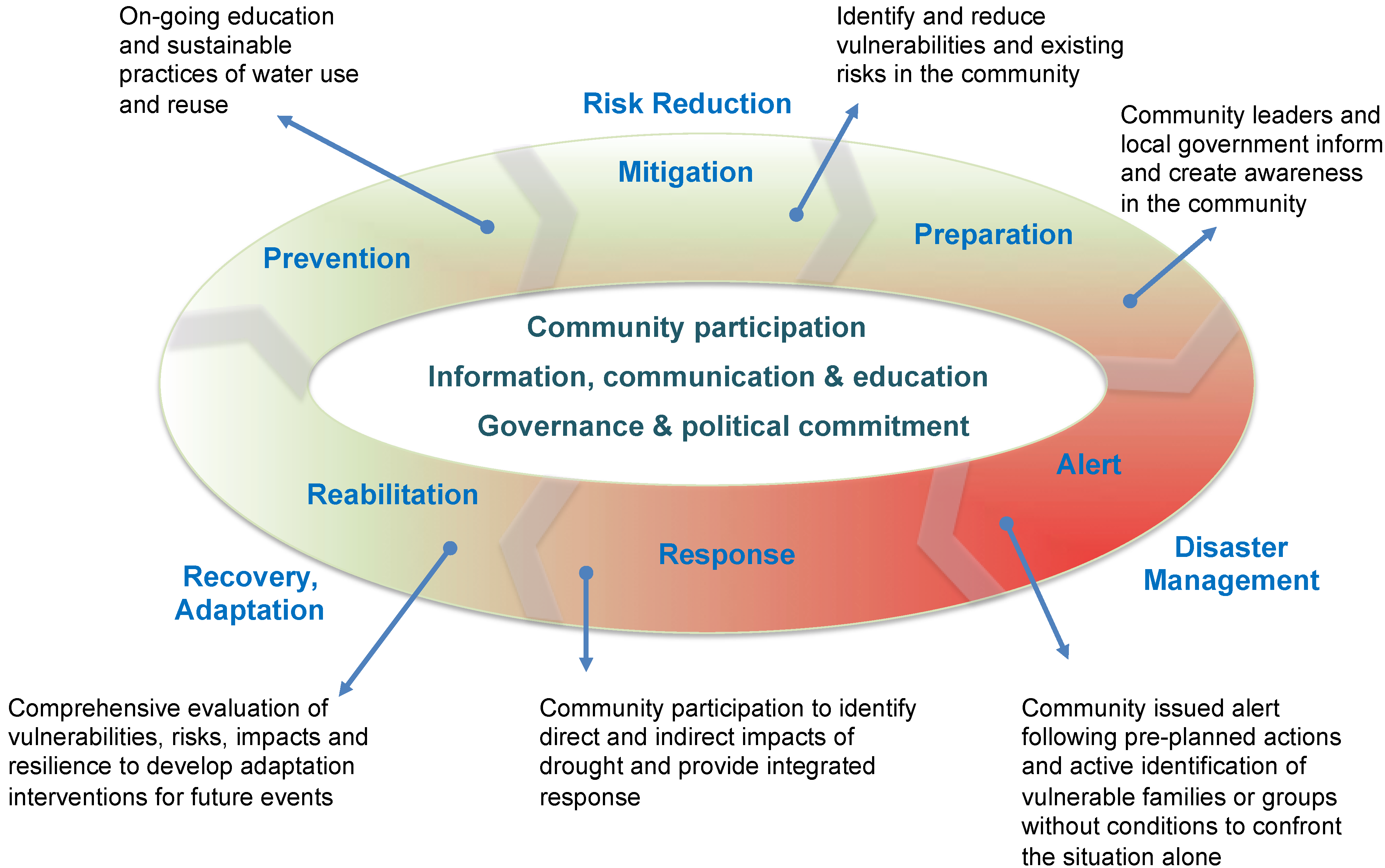
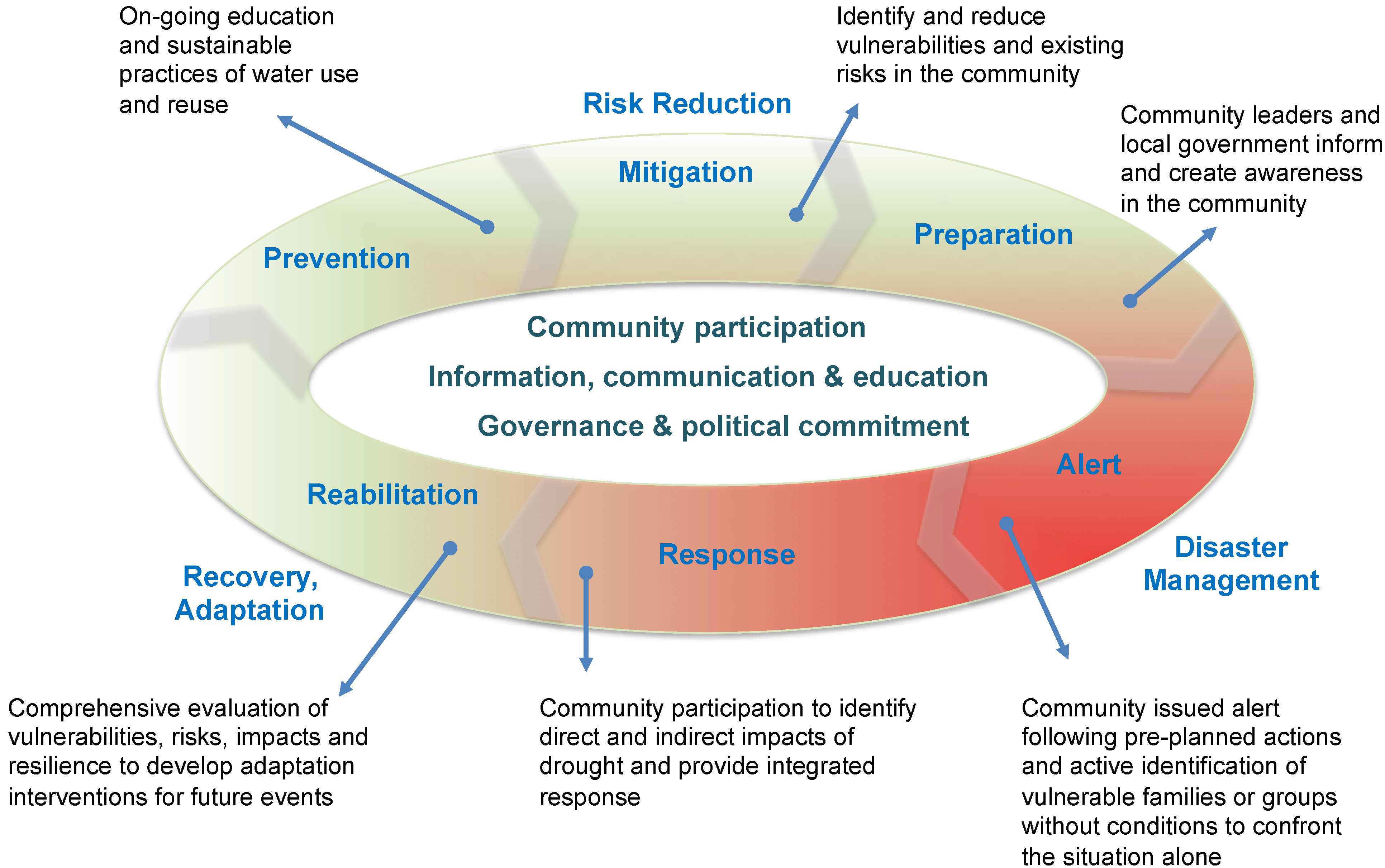
| Risk reduction stage | |
|---|---|
| PREVENTION | On-going community and local government involvement, information and communication |
| Promote educational measures and community actions for water conservation and measures to promote good nutrition | |
| Promote sustainable practices of water use and reuse | |
| On-going monitoring of water and food-borne diseases and selected non-communicable diseases in the communities at risk | |
| Follow-up the epidemiological profile of the community to identify adverse changes | |
| Promote capacity building of local health agents | |
| MITIGATION | Work with local stakeholders to identify and reduce vulnerabilities and existing risks in the community |
| Work with the local communities to develop measures aimed at minimizing risks and health impacts | |
| Promote health sector participation in public policy programs for water resource infrastructure | |
| Participate in inter-sectorial efforts to address drought impacts (e.g., with climate services to anticipate drought events) | |
| PREPARATION | Assess the internal response capacity; identify local resources; and establish intra and inter-sectorial partnerships for action |
| Participate in risk assessments, mapping, scenarios, to determine the severity of the problem from a health preparation perspective and to determine priority actions | |
| Implement the “Operative Committee of Health Emergencies*”, and establish the action plan. | |
| Work with community leaders and local government to inform and create awareness in the community | |
| Disaster management stage | |
| ALERT | Issue alert following pre-planned actions and monitor its implementation |
| Activate the “Operative Committee of Health Emergencies” and notify the event | |
| Actively identify families or groups without conditions to confront the situation alone | |
| Activate human and financial resources | |
| RESPONSE | Provide for the health needs to the affected persons |
| Intensify epidemiological, environmental and sanitary surveillance | |
| Monitor morbidity and mortality of direct and indirect impacts of drought | |
| Ongoing assessment of the response to determine future action | |
| Recovery and adaptation stage | |
| REHABILITATION | Activate mechanisms to ensure the continuation of basic services, essential to the functioning of health facilities (e.g., water, energy) |
| Activate specialized health care (e.g., for early identification and management of outbreaks) | |
| Activate psychosocial health care for the community and workers involved in the process | |
| Implement a comprehensive evaluation of vulnerabilities, risks, impacts and resilience to develop adaptation options for future events | |
| * Operative Committee of Health Emergencies: A team formed by local stakeholders to organize and conduct risk management actions. | |
4. Conclusions
Author Contributions
Conflicts of Interest
References
- EM-DAT. The OFDA/CRED International Disaster Database. Université Catholique de Louvain, Brussels, Belgium. Available online: www.emdat.be (accessed on 3 August 2014).
- Mazyck, P.R. Drought and health. Am. J. Public Health Nations Health 1931, 21, 1198–1202. [Google Scholar] [CrossRef] [PubMed]
- Stanke, C.; Kerac, M.; Prudhomme, C.; Medlock, J.; Murray, V. Health effects of drought: A systematic review of the evidence. PLoS Curr. Disasters 2013. [Google Scholar] [CrossRef]
- WMO. Atlas of Mortality and Economic Losses from Weather, Climate and Water Extremes; World Meteorological Organization: Geneva, Switzerland, 2014; pp. 1970–2012. Available online: http://www.wmo.int/pages/prog/drr/transfer/2014.06.12-WMO1123_Atlas_120614.pdf (accessed on 27 July 2014).
- McMichael, A.J. Drought, drying and mental health: Lessons from recent experiences for future risk-lessening policies. Aust. J. Rural Health 2011, 19, 227–228. [Google Scholar] [CrossRef] [PubMed]
- Obrien, L.V.; Berry, H.L.; Coleman, C.; Hanigan, I.C. Drought as a mental health exposure. Environ.Res. 2014, 131, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.; Aragao, L.; Sabel, C.; Nakaya, T. Drought impacts on children’s respiratory health in the Brazilian Amazon. Sci. Rep. 2014. [Google Scholar] [CrossRef]
- UN/ISDR. Global Assessment Report on Disaster Risk Reduction: Revealing Risk, Redefining Development. International Strategy for Disaster Risk Reduction; Information Press: Oxford, UK, 2011; pp. 54–69. Available online: www.preventionweb.net/english/hyogo/gar/2011/en/bgdocs/GAR-2011/GAR2011_Report_Chapter3.pdf (accessed on 27 July 2014).
- Guha-Sapir, D.; Vos, F.; Below, R.; Ponserre, S. Annual Disaster Statistical Review 2011: The Numbers and Trends; CRED: Brussels, Belgium, 2012. Available online: www.cred.be/sites/default/files/ADSR_2011.pdf (accessed on 28 July 2014).
- Wilhite, D.A.; Sivakumar, M.V.K.; Pulwarty, R. Managing drought risk in a changing climate: The role of national drought policy. Weather Clim. Extrem. 2014, 3, 4–13. [Google Scholar] [CrossRef]
- Atlas of Health and Climate; World Health Organization and World Meteorological Organization: Geneva, Switzerland, 2012.
- Corvalan, C.; Hales, S.; McMichael, A. Ecosystems and Human Well-Being: Health Synthesis. Millennium Ecosystem Assessment; World Health Organization: Geneva, Switzerland, 2005. Available online: www.millenniumassessment.org/documents/document.357.aspx.pdf (accessed on 28 July 2014).
- UN/ISDR. Drought Risk Reduction Framework and Practices: Contributing to the Implementation of the Hyogo Framework for Action; United Nations secretariat of the International Strategy for Disaster Reduction: Geneva, Switzerland, 2009. Available online: www.unisdr.org/files/11541_DroughtRiskReduction2009library.pdf (accessed on 2 August 2014).
- Berry, H.; Bowen, K.; Kjellstrom, T. Climate change and mental health: A causal pathways framework. Int. J. Public Health 2010, 55, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Coêlho, A.; Adair, J.; Mocellin, J. Psychological responses to drought in northeastern Brazil. Interamerican J. Psychol. 2004, 38, 95–103. [Google Scholar]
- United Nations Convention to Combat Desertification. Available online: www.unccd.int/en/about-the-convention/Pages/Text-Part-I.aspx (accessed on 30 July 2014).
- Patz, J.; Corvalan, C.; Hortwitz, P.; Campbell-Lendrum, D. Our Planet, Our Health, Our Future. Human Health and the Rio Conventions: Biological Diversity, Climate Change and Desertification; World Health Organization: Geneva, Switzerland, 2012. Available online: www.who.int/globalchange/publications/reports/health_rioconventions.pdf (accessed on 29 July 2014).
- Protecting Health from Climate Change—Vulnerability and Adaptation Assessment; World Health Organization: Geneva, Switzerland, 2012.
- CEPED-UFSC. Atlas Brasileiro de Desastres Naturais 1991 a 2010: Volume Brasil; Centro Universitário de Estudos e Pesquisas sobre Desastres. Universidade Federal de Santa Catarina: Florianópolis/SC, Brasil, 2012. Available online: http://150.162.127.14:8080/atlas/Brasil%20Rev.pdf (accessed on 25 July 2014).
- Nova Delimitação do Semiárido; Ministério da Integração Nacional. Secretaria de Políticas de Desenvolvimento Regional: Brasília/DF, Brasil, 2005. Available online: www.integracao.gov.br/c/document_library/get_file?uuid=0aa2b9b5-aa4d-4b55-a6e1-82faf0762763&groupId=24915 (accessed on 30 July 2014).
- Ambrizzi, T.; Araújo, M.; Silva Dias, P.L.; Wainer, I.; Artaxo, P.; Marengo, J.A. Base Científica das Mudanças Climáticas: Contribuição do Grupo de Trabalho 1 para o Primeiro Relatório de Avaliação Nacional do Painel Brasileiro de Mudanças Climáticas—Sumário Executivo; Ministério da Ciência e Tecnologia, Painel Brasileiro de Mudança Climática: Rio de Janeiro/RJ, Brasil, 2013; Volume 1. Available online: www.pbmc.coppe.ufrj.br/documentos/MCTI_PBMC_Sumario%20Executivo%204_Finalizado.pdf (accessed on 23 July 2014).
- Bouzid, M.; Hooper, L.; Hunter, P.R. The Effectiveness of public health interventions to reduce the health impact of climate change: A systematic review of systematic reviews. PLoS One 2013, 8, e62041. [Google Scholar] [CrossRef]
- CEDEPLAR-UFMG & FIOCRUZ. Mudanças Climáticas, Migrações e saúde: Cenários para o Nordeste Brasileiro 2000–2050; Centro de Desenvolvimento e Planejamento Regional da Universidade Federal de Minas Gerais & Fundação Oswaldo Cruz: Belo Horizonte/MG, Brasil, 2008. Available online: www.antaq.gov.br/portal/Pdf/MeioAmbiente/MIGRACAOESAUDENORDESTE.pdf (accessed on 25 July 2014).
- Confalonieri, U. Mudança climática global e saúde humana no Brasil. In Parcerias Estratégicas. Mudança do clima no Brasil: Vulnerabilidade, impactos e adaptação; Ministério da Ciência e Tecnologia. Centro de Gestão e Estudos Estratégicos (CGEE): Brasília/DF, Brasil, 2008; Number 27; pp. 323–349. [Google Scholar]
- Finan, T.J.; Nelson, D.R. Making rain, making roads, making do: public and private adaptations to drought in Ceará, Northeast Brazil. Clim. Res. 2001, 19, 97–108. [Google Scholar] [CrossRef]
- UNDP. Atlas de Desenvolvimento Humano do Brasil, 2013. Programa das Nações Unidas para o Desenvolvimento, Instituto de Pesquisa Econômica Aplicada e Fundação João Pinheiro, 2013. Available online: www.atlasbrasil.org.br/2013/ (accessed on 25 July 2014).
- Shiferaw, B.; Tesfaye, K.; Kassie, M.; Abate, T.; Prasanna, B.M.; Menkir, A. Managing vulnerability to drought and enhancing livelihood resilience in sub-Saharan Africa: Technological, institutional and policy options. Weather Clim. Extrem. 2014, 3, 67–79. [Google Scholar] [CrossRef]
- Marengo, J.A. Vulnerabilidade, impactos e adaptação à mudança do clima no semi-árido do Brasil. In Parcerias Estratégicas. Mudança do clima no Brasil: Vulnerabilidade, impactos e adaptação. Ministério da Ciência e Tecnologia; Centro de Gestão e Estudos Estratégicos (CGEE): Brasília/DF, Brazil, 2008; Number 27; pp. 149–176. [Google Scholar]
- Anyamba, A.; Small, J.L.; Britch, S.C.; Tucker, C.J.; Pak, E.W.; Reynolds1, C.A.; Crutchfield, J.; Linthicum, K.J. Recent weather extremes and impacts on agricultural production and vector-borne disease outbreak patterns. PLoS One 2014, 9, e92538. [Google Scholar] [CrossRef]
- Jancloes, M.; Thomson, M.; Máñez Costa, M.; Hewitt, C.; Corvalan, C.; Dinku, T.; Lowe, R.; Hayden, M. Climate services to improve public health. Int. J. Environ. Res. Public Health 2014, 11, 4555–4559. [Google Scholar] [CrossRef]
- Lemos, M.C.; Finan, T.J.; Fox, R.W.; Nelson, D.R.; Tucker, J. The use of seasonal climate forecasting in policymaking: Lessons from northeast Brazil climatic change. Clim. Chang. 2002, 55, 479–507. [Google Scholar] [CrossRef]
- IPCC. Summary for Policymakers. In Managing the Risks of Extremes Events and disasters to Advance Climate Change Adaptation. A special Report of Working Groups I and II of the Intergovernmental Panel on Climate Change; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2012; pp. 1–19. [Google Scholar]
- Narváez, L.; Lavell, A.; Ortega, G.P. La Gestión del Riesgo de Desastres: Un Enfoque Basado en Procesos; Secretaria General de la Comunidad Andina: Lima, Perú, 2009, 1st ed. Available online: www.comunidadandina.org/predecan/doc/libros/PROCESOS_ok.pdf (accessed on 29 July 2014).
- CDC. When Every Drop Counts: Protecting Public Health during Drought Conditions—A Guide for Public Health Professionals; Department of Health and Human Services: Atlanta, GA, USA, 2010. Available online: www.cdc.gov/nceh/ehs/docs/when_every_drop_counts.pdf (accessed on 25 July 2014).
- Adeel, Z.; Safriel, U.; Niemeijer, D.; White, R. Ecosystems and Human Well-Being: Desertification Synthesis. Millennium Ecosystem Assessment; World Resources Institute: Washington, DC, USA, 2005. Available online: www.millenniumassessment.org/documents/document.355.aspx.pdf (accessed on 28 July 2014).
- Keim, M.E. Building human resilience. The role of public health preparedness and response as an adaptation to climate change. Am. J. Prev. Med. 2008, 35, 508–516. [Google Scholar] [CrossRef]
- Guia de preparação e resposta aos desastres associados às inundações para a gestão municipal do sistema único de saúde; Ministry of Health: Brasilia, Brazil, 2011. Available online: www.cve.saude.sp.gov.br/htm/zoo/pdf/lepto11_guia_sms_desastres.pdf (accessed on 28 July 2014).
- Bowen, K.J.; Friel, S.; Ebi, K.; Butler, C.D.; Fiona Miller, F.; McMichael, A.J. Governing for a healthy population: Towards an understanding of how decision-making will determine our global health in a changing climate. Int. J. Environ. Res. Public Health 2012, 9, 55–72. [Google Scholar] [CrossRef] [PubMed]
- Ebi, K.L. Resilience to the health risks of extreme weather events in a changing climate in the United States. Int. J. Environ. Res. Public Health 2011, 8, 4582–4595. [Google Scholar] [CrossRef]
- Rasella, D.; Aquino, R.; Santos, C.A.; Paes-Sousa, R.; Barreto, M.L. Effect of a conditional cash transfer programme on childhood mortality: A nationwide analysis of Brazilian municipalities. Lancet 2013, 382, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Villa, M.A. Vida e morte no sertão: História das secas no Nordeste nos séculos XIX e XX; Ática: São Paulo, Brasil, 2000; p. 269. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sena, A.; Barcellos, C.; Freitas, C.; Corvalan, C. Managing the Health Impacts of Drought in Brazil. Int. J. Environ. Res. Public Health 2014, 11, 10737-10751. https://doi.org/10.3390/ijerph111010737
Sena A, Barcellos C, Freitas C, Corvalan C. Managing the Health Impacts of Drought in Brazil. International Journal of Environmental Research and Public Health. 2014; 11(10):10737-10751. https://doi.org/10.3390/ijerph111010737
Chicago/Turabian StyleSena, Aderita, Christovam Barcellos, Carlos Freitas, and Carlos Corvalan. 2014. "Managing the Health Impacts of Drought in Brazil" International Journal of Environmental Research and Public Health 11, no. 10: 10737-10751. https://doi.org/10.3390/ijerph111010737
APA StyleSena, A., Barcellos, C., Freitas, C., & Corvalan, C. (2014). Managing the Health Impacts of Drought in Brazil. International Journal of Environmental Research and Public Health, 11(10), 10737-10751. https://doi.org/10.3390/ijerph111010737