
Antioxidant Efficacy of a Spirulina Liquid Extract on Oxidative Stress Status and Metabolic Disturbances in Subjects with Metabolic Syndrome

 , , and
, , and
Abstract
:1. Introduction
2. Result
2.1. Demographics and Anthropometric Measurements of Patients with Metabolic Syndrome
2.2. Effects of Spirulysat® on Oxidative Stress
2.3. Effects of Spirulysat® on Lipid and Glucose Metabolism

{kind=link}
{kind=link}
| Measured Variables | V1 | V2 | V3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Placebo n = 20 | Spirulysat® n = 20 | p-Value | Placebo n = 20 | Spirulysat® n = 20 | p-Value | Placebo n = 20 | Spirulysat® n = 20 | p-Value | |
| oxLDL/LDL cholesterol ratio (U/g) | 67.44 ± 23.04 | 61.15 ± 20.53 | 0.58 | 72.22 ± 17.76 | 67.16 ±14.37 | 0.41 | 74.06 ± 16.08 | 69.08 ± 12.72 | 0.36 |
| Triglycerides (g/L) | 1.83 ± 0.82 | 1.35 ± 0.46 | 0.11 | 2.02 ± 0.89 | 1.58 ± 0.80 | 0.13 | 1.97 ± 0.80 | 1.23 ± 0.57 | 0.003 |
| LDL cholesterol (g/L) | 1.53 ± 0.36 | 1.52 ± 0.33 | 0.88 | 1.51 ±0.44 | 1.49 ± 0.32 | 0.96 | 1.43 ± 0.38 | 1.49 ± 0.33 | 0.22 |
| HDL cholesterol (g/L) | 0.47 ± 0.13 | 0.54 ± 0.09 | 0.004 | 0.47 ± 0.16 | 0.54 ± 0.11 | 0.012 | 0.48 ± 0.18 | 0.55 ± 0.14 | 0.031 |
| Total cholesterol (g/L) | 2.36 ± 0.46 | 2.33 ± 0.36 | 0.96 | 2.38 ± 0.50 | 2.34 ± 0.35 | 0.77 | 2.31 ± 0.43 | 2.30 ± 0.34 | 0.57 |
| Fatty Liver Index (FLI) | 72.95 ± 15.39 | 68.90 ± 19.89 | 0.71 | 74.25 ± 16.46 | 69.18 ± 20.36 | 0.48 | 75.32 ± 17.53 | 65.63 ± 22.16 | 0.19 |
| Glycemia (mmol/L) | 5.26 ± 0.64 | 5.56 ± 0.56 | 0.072 | 5.48 ± 0.76 | 5.55 ± 0.65 | 0.84 | 5.38 ± 0.76 | 5.90 ± 0.67 | 0.056 |
| Insulinemia (mU/L) | 10.06 ± 4.78 | 14.17 ± 8.11 | 0.044 | 11.39 ± 3.41 | 13.89 ± 6.60 | 0.33 | 11.95 ± 4.82 | 16.13 ± 10.88 | 0.28 |
| Urinary isoprostane (µg/24 h) | 2.86 ± 1.96 | 2.61 ±1.44 | 0.82 | 2.98 ± 1.56 | 2.20 ± 1.09 | 0.057 | 3.51 ± 2.11 | 2.31 ± 0.91 | 0.014 |
| ALAT (µkat/L) | 0.48 ± 0.31 | 0.59 ± 0.35 | 0.27 | 0.45 ± 0.23 | 0.57 ± 0.33 | 0.16 | 0.62 ± 0.58 | 0.57 ± 0.48 | 0.7 |
| ASAT (µkat/L) | 0.41 ± 0.14 | 0.43 ± 0.14 | 0.63 | 0.42 ± 0.13 | 0.42 ± 0.15 | 0.85 | 0.49 ± 0.30 | 0.43 ± 0.16 | 0.64 |
| GGT (U/L) | 50.22 ± 50.07 | 46.84 ± 34.97 | >0.99 | 45.67 ± 37.75 | 45.23 ± 28.84 | 0.69 | 54.64 ± 59.04 | 49.07 ± 36.69 | 0.54 |
3. Discussion
4. Materials and Methods
4.1. Preparation of Arthrospira Liquid Extract (Spirulysat®)
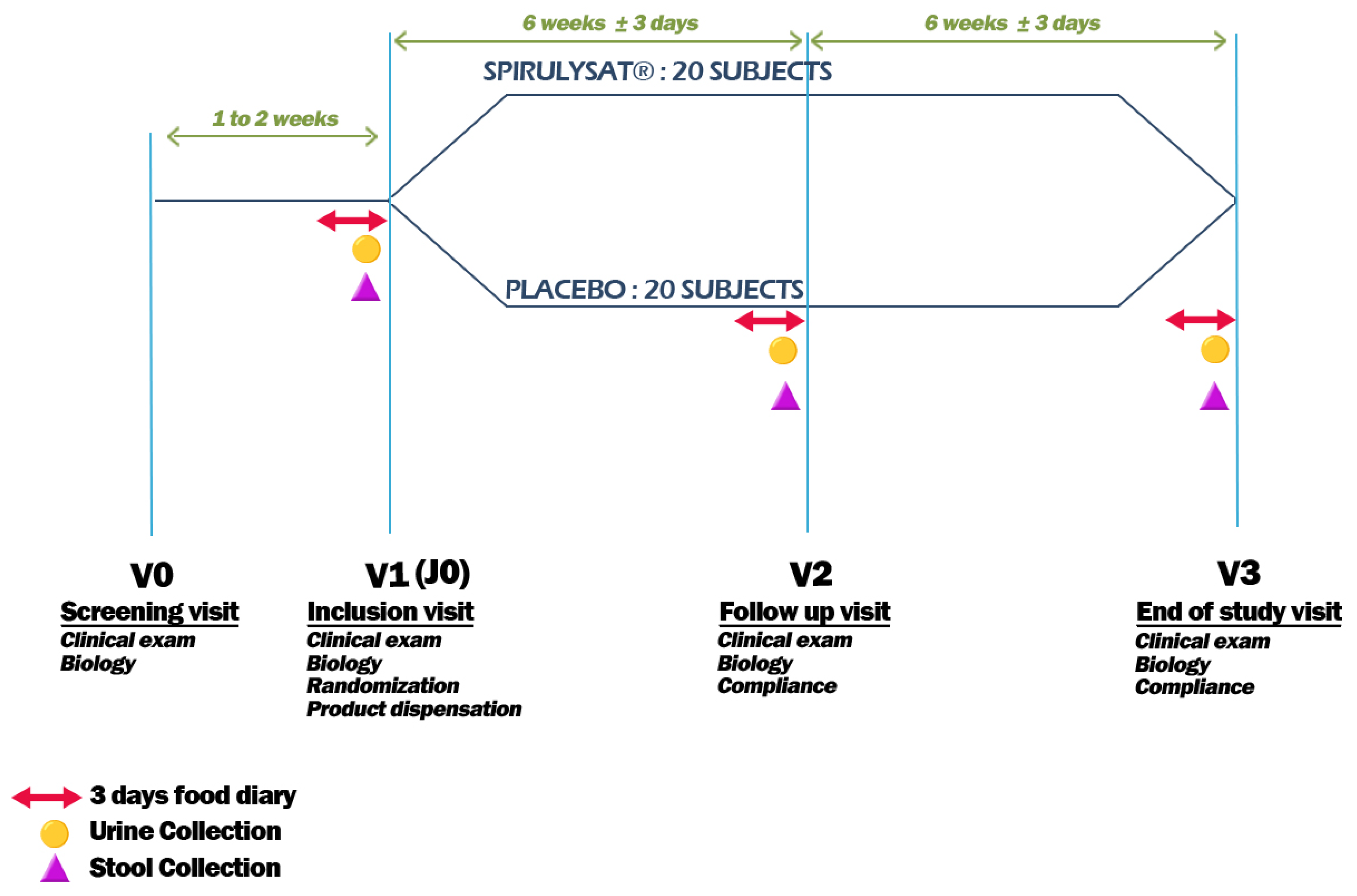
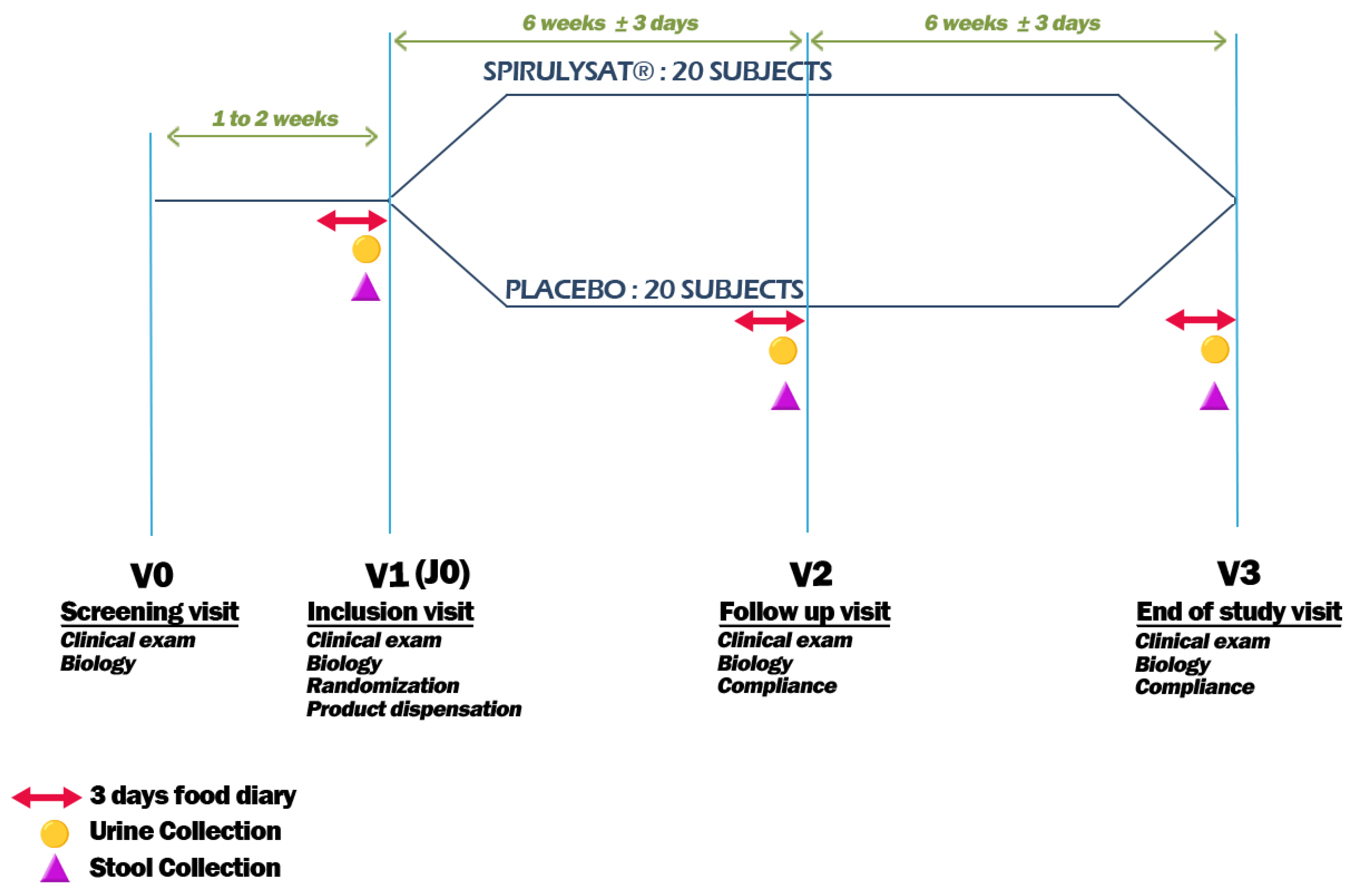
4.2. Study Design
4.2.1. Pre-study Recommendations
4.2.2. Study Design
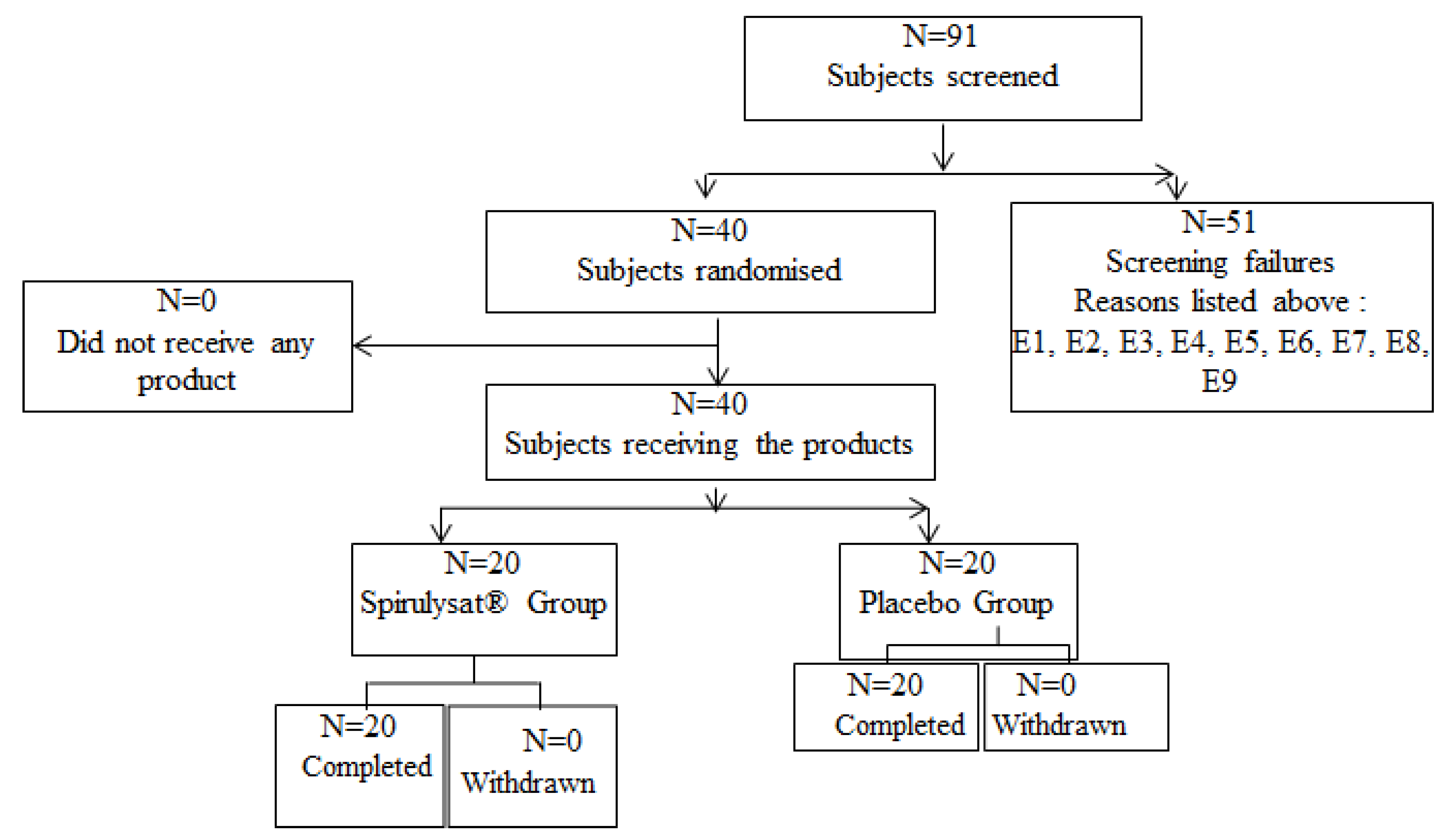
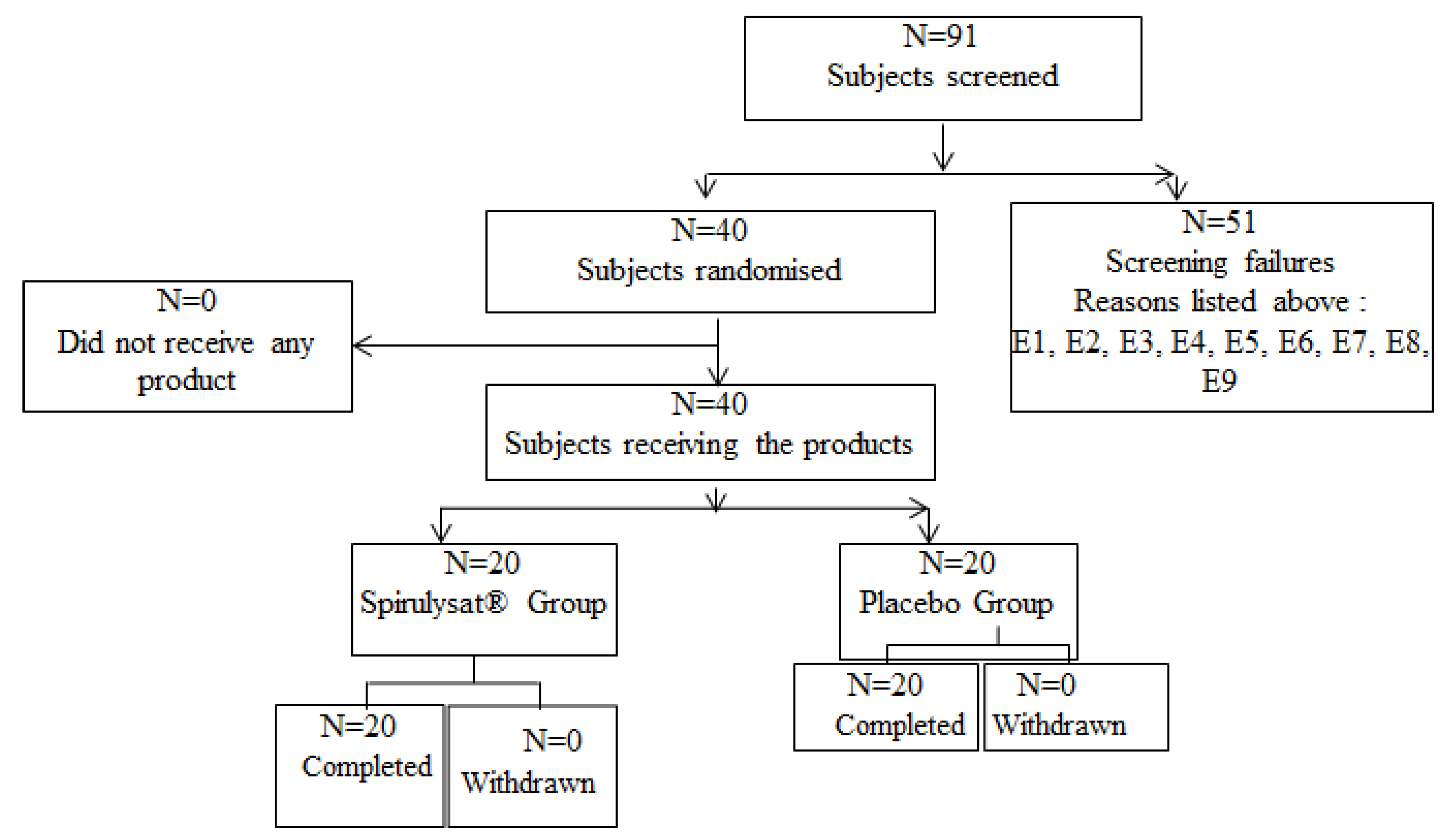
4.3. Study Participants
4.4. Anthropometric and Hemodynamic Measurements
4.5. Biological Parameters Measurements
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Farhangi, M.A.; Jahangiry, L. Dietary Diversity Score Is Associated with Cardiovascular Risk Factors and Serum Adiponectin Concentrations in Patients with Metabolic Syndrome. BMC Cardiovasc. Disord. 2018, 18, 68. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Status Report on Noncommunicable Diseases; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Vona, R.; Gambardella, L.; Cittadini, C.; Straface, E.; Pietraforte, D. Biomarkers of Oxidative Stress in Metabolic Syndrome and Associated Diseases. Oxid. Med. Cell. Longev. 2019, 2019, 8267234. [Google Scholar] [CrossRef] [Green Version]
- Le, N.-A. Postprandial Triglycerides, Oxidative Stress, and Inflammation; IntechOpen: London, UK, 2020; ISBN 978-1-83962-520-6. [Google Scholar]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C.; et al. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [Green Version]
- Milne, G.L.; Yin, H.; Morrow, J.D. Human Biochemistry of the Isoprostane Pathway. J. Biol. Chem. 2008, 283, 15533–15537. [Google Scholar] [CrossRef] [Green Version]
- Jürgens, G.; Hoff, H.F.; Chisolm, G.M.; Esterbauer, H. Modification of Human Serum Low Density Lipoprotein by Oxidation--Characterization and Pathophysiological Implications. Chem. Phys. Lipids 1987, 45, 315–336. [Google Scholar] [CrossRef]
- Bauer, J.; Ripperger, A.; Frantz, S.; Ergün, S.; Schwedhelm, E.; Benndorf, R.A. Pathophysiology of Isoprostanes in the Cardiovascular System: Implications of Isoprostane-Mediated Thromboxane A2 Receptor Activation. Br. J. Pharmacol. 2014, 171, 3115–3131. [Google Scholar] [CrossRef] [Green Version]
- Navab, M.; Ananthramaiah, G.M.; Reddy, S.T.; Van Lenten, B.J.; Ansell, B.J.; Fonarow, G.C.; Vahabzadeh, K.; Hama, S.; Hough, G.; Kamranpour, N.; et al. The Oxidation Hypothesis of Atherogenesis: The Role of Oxidized Phospholipids and HDL. J. Lipid Res. 2004, 45, 993–1007. [Google Scholar] [CrossRef] [Green Version]
- Mangge, H.; Becker, K.; Fuchs, D.; Gostner, J.M. Antioxidants, Inflammation and Cardiovascular Disease. World J. Cardiol. 2014, 6, 462–477. [Google Scholar] [CrossRef]
- Li, S.; Tan, H.-Y.; Wang, N.; Zhang, Z.-J.; Lao, L.; Wong, C.-W.; Feng, Y. The Role of Oxidative Stress and Antioxidants in Liver Diseases. Int. J. Mol. Sci. 2015, 16, 26087–26124. [Google Scholar] [CrossRef] [Green Version]
- Kay, R.A. Microalgae as Food and Supplement. Crit. Rev. Food Sci. Nutr. 1991, 30, 555–573. [Google Scholar] [CrossRef]
- Liu, Q.; Huang, Y.; Zhang, R.; Cai, T.; Cai, Y. Medical Application of Spirulina Platensis Derived C-Phycocyanin. Evid.-Based Complement Altern. Med. ECAM 2016, 2016, 7803846. [Google Scholar] [CrossRef] [Green Version]
- Venkataraman, L.V. Spirulina Platensis (Arthrospira): Physiology, Cell Biology and Biotechnologym, Edited by Avigad Vonshak. J. Appl. Phycol. 1997, 9, 295–296. [Google Scholar] [CrossRef]
- Humm, H.J.; Wicks, S.B. Introduction and Guide to the Marine Bluegreen Algae. Very Good Hardcover. Smith Family Bookstore. 1980. Available online: https://www.abebooks.com/9780471052173/Introduction-Guide-Marine-Bluegreen-Algae-0471052175/plp (accessed on 21 May 2022).
- Ciferri, O. Spirulina, the Edible Microorganism. Microbiol. Rev. 1983, 47, 551–578. [Google Scholar] [CrossRef]
- Sandgruber, F.; Gielsdorf, A.; Baur, A.C.; Schenz, B.; Müller, S.M.; Schwerdtle, T.; Stangl, G.I.; Griehl, C.; Lorkowski, S.; Dawczynski, C. Variability in Macro- and Micronutrients of 15 Commercially Available Microalgae Powders. Mar. Drugs 2021, 19, 310. [Google Scholar] [CrossRef]
- Finamore, A.; Palmery, M.; Bensehaila, S.; Peluso, I. Antioxidant, Immunomodulating, and Microbial-Modulating Activities of the Sustainable and Ecofriendly Spirulina. Oxid. Med. Cell. Longev. 2017, 2017, 3247528. [Google Scholar] [CrossRef] [Green Version]
- Zeinalian, R.; Farhangi, M.A.; Shariat, A.; Saghafi-Asl, M. The Effects of Spirulina Platensis on Anthropometric Indices, Appetite, Lipid Profile and Serum Vascular Endothelial Growth Factor (VEGF) in Obese Individuals: A Randomized Double Blinded Placebo Controlled Trial. BMC Complement Altern. Med. 2017, 17, 225. [Google Scholar] [CrossRef]
- Bobescu, E.; Bălan, A.; Moga, M.A.; Teodorescu, A.; Mitrică, M.; Dima, L. Are There Any Beneficial Effects of Spirulina Supplementation for Metabolic Syndrome Components in Postmenopausal Women? Mar. Drugs 2020, 18, 651. [Google Scholar] [CrossRef]
- Wolkers, H.; Barbosa, M.J.; Kleinegris, D.M.M.; Bosma, R.; Wijffels, R.H.; Harmsen, P.F.H. Microalgae: The Green Gold of the Future?: Large-Scale Sustainable Cultivation of Microalgae for the Production of Bulk Commodities; Wageningen UR—Food & Biobased Research: Wageningen, The Netherlands, 2011. [Google Scholar]
- Coué, M.; Tesse, A.; Falewée, J.; Aguesse, A.; Croyal, M.; Fizanne, L.; Chaigneau, J.; Boursier, J.; Ouguerram, K. Spirulina Liquid Extract Protects against Fibrosis Related to Non-Alcoholic Steatohepatitis and Increases Ursodeoxycholic Acid. Nutrients 2019, 11, 194. [Google Scholar] [CrossRef] [Green Version]
- Kasbi-Chadli, F.; Coué, M.; Aguesse, A.; Grit, I.; Souque, T.; Ferchaud-Roucher, V.; Ouguerram, K. Spirulina Liquid Extract Prevents Metabolic Disturbances and Improves Liver Sphingolipids Profile in Hamster Fed a High-Fat Diet. Eur. J. Nutr. 2021, 60, 4483–4494. [Google Scholar] [CrossRef]
- Coué, M.; Croyal, M.; Habib, M.; Castellano, B.; Aguesse, A.; Grit, I.; Gourdel, M.; Billard, H.; Lépine, O.; Michel, C.; et al. Perinatal Administration of C-Phycocyanin Protects Against Atherosclerosis in ApoE-Deficient Mice by Modulating Cholesterol and Trimethylamine-N-Oxide Metabolisms. Arterioscler. Thromb. Vasc. Biol. 2021, 41, e512–e523. [Google Scholar] [CrossRef]
- Benedetti, S.; Rinalducci, S.; Benvenuti, F.; Francogli, S.; Pagliarani, S.; Giorgi, L.; Micheloni, M.; D’Amici, G.M.; Zolla, L.; Canestrari, F. Purification and Characterization of Phycocyanin from the Blue-Green Alga Aphanizomenon Flos-Aquae. J. Chromatogr. B Analyt. Technol. Biomed. Life. Sci. 2006, 833, 12–18. [Google Scholar] [CrossRef]
- Wang, L.; Qu, Y.; Fu, X.; Zhao, M.; Wang, S.; Sun, L. Isolation, Purification and Properties of an R-Phycocyanin from the Phycobilisomes of a Marine Red Macroalga Polysiphonia Urceolata. PLoS ONE 2014, 9, e87833. [Google Scholar] [CrossRef] [Green Version]
- Minic, S.L.; Stanic-Vucinic, D.; Mihailovic, J.; Krstic, M.; Nikolic, M.R.; Cirkovic Velickovic, T. Digestion by Pepsin Releases Biologically Active Chromopeptides from C-Phycocyanin, a Blue-Colored Biliprotein of Microalga Spirulina. J. Proteomics 2016, 147, 132–139. [Google Scholar] [CrossRef] [Green Version]
- Zheng, J.; Inoguchi, T.; Sasaki, S.; Maeda, Y.; McCarty, M.F.; Fujii, M.; Ikeda, N.; Kobayashi, K.; Sonoda, N.; Takayanagi, R. Phycocyanin and Phycocyanobilin from Spirulina Platensis Protect against Diabetic Nephropathy by Inhibiting Oxidative Stress. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2013, 304, R110–R120. [Google Scholar] [CrossRef] [Green Version]
- Libby, P. Inflammation in Atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2045–2051. [Google Scholar] [CrossRef] [Green Version]
- Romay, C.; Ledón, N.; González, R. Further Studies on Anti-Inflammatory Activity of Phycocyanin in Some Animal Models of Inflammation. Inflamm. Res. Off. J. Eur. Histamine Res. Soc. Al 1998, 47, 334–338. [Google Scholar] [CrossRef]
- Thangam, R.; Suresh, V.; Asenath Princy, W.; Rajkumar, M.; Senthilkumar, N.; Gunasekaran, P.; Rengasamy, R.; Anbazhagan, C.; Kaveri, K.; Kannan, S. C-Phycocyanin from Oscillatoria Tenuis Exhibited an Antioxidant and in Vitro Antiproliferative Activity through Induction of Apoptosis and G0/G1 Cell Cycle Arrest. Food Chem. 2013, 140, 262–272. [Google Scholar] [CrossRef]
- Romay, C.; Armesto, J.; Remirez, D.; González, R.; Ledon, N.; García, I. Antioxidant and Anti-Inflammatory Properties of C-Phycocyanin from Blue-Green Algae. Inflamm. Res. 1998, 47, 36–41. [Google Scholar] [CrossRef]
- Romay, C.; González, R.; Ledón, N.; Remirez, D.; Rimbau, V. C-Phycocyanin: A Biliprotein with Antioxidant, Anti-Inflammatory and Neuroprotective Effects. Curr. Protein Pept. Sci. 2003, 4, 207–216. [Google Scholar] [CrossRef]
- Ku, C.S.; Yang, Y.; Park, Y.; Lee, J. Health Benefits of Blue-Green Algae: Prevention of Cardiovascular Disease and Nonalcoholic Fatty Liver Disease. J. Med. Food 2013, 16, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Sámano, J.; Torres-Montes de Oca, A.; Luqueño-Bocardo, O.I.; Torres-Durán, P.V.; Juárez-Oropeza, M.A. Spirulina Maxima Decreases Endothelial Damage and Oxidative Stress Indicators in Patients with Systemic Arterial Hypertension: Results from Exploratory Controlled Clinical Trial. Mar. Drugs 2018, 16, 496. [Google Scholar] [CrossRef] [Green Version]
- Romay, C.; Delgado, R.; Remirez, D.; González, R.; Rojas, A. Effects of Phycocyanin Extract on Tumor Necrosis Factor-Alpha and Nitrite Levels in Serum of Mice Treated with Endotoxin. Arzneimittelforschung 2001, 51, 733–736. [Google Scholar] [CrossRef]
- Rajasekar, P.; Palanisamy, S.; Anjali, R.; Vinosha, M.; Elakkiya, M.; Marudhupandi, T.; Tabarsa, M.; You, S.; Prabhu, N.M. Isolation and Structural Characterization of Sulfated Polysaccharide from Spirulina Platensis and Its Bioactive Potential: In Vitro Antioxidant, Antibacterial Activity and Zebrafish Growth and Reproductive Performance. Int. J. Biol. Macromol. 2019, 141, 809–821. [Google Scholar] [CrossRef]
- Ngo, D.-H.; Kim, S.-K. Sulfated Polysaccharides as Bioactive Agents from Marine Algae. Int. J. Biol. Macromol. 2013, 62, 70–75. [Google Scholar] [CrossRef]
- Pak, W.; Takayama, F.; Mine, M.; Nakamoto, K.; Kodo, Y.; Mankura, M.; Egashira, T.; Kawasaki, H.; Mori, A. Anti-Oxidative and Anti-Inflammatory Effects of Spirulina on Rat Model of Non-Alcoholic Steatohepatitis. J. Clin. Biochem. Nutr. 2012, 51, 227–234. [Google Scholar] [CrossRef] [Green Version]
- Spahis, S.; Borys, J.-M.; Levy, E. Metabolic Syndrome as a Multifaceted Risk Factor for Oxidative Stress. Antioxid. Redox Signal. 2017, 26, 445–461. [Google Scholar] [CrossRef]
- Medina-Vera, I.; Gómez-de-Regil, L.; Gutiérrez-Solis, A.L.; Lugo, R.; Guevara-Cruz, M.; Pedraza-Chaverri, J.; Avila-Nava, A. Dietary Strategies by Foods with Antioxidant Effect on Nutritional Management of Dyslipidemias: A Systematic Review. Antioxidants 2021, 10, 225. [Google Scholar] [CrossRef]
- Wu, Q.; Liu, L.; Miron, A.; Klímová, B.; Wan, D.; Kuča, K. The Antioxidant, Immunomodulatory, and Anti-Inflammatory Activities of Spirulina: An Overview. Arch. Toxicol. 2016, 90, 1817–1840. [Google Scholar] [CrossRef]
- Serban, M.-C.; Sahebkar, A.; Dragan, S.; Stoichescu-Hogea, G.; Ursoniu, S.; Andrica, F.; Banach, M. A Systematic Review and Meta-Analysis of the Impact of Spirulina Supplementation on Plasma Lipid Concentrations. Clin. Nutr. 2016, 35, 842–851. [Google Scholar] [CrossRef]
- Bohórquez-Medina, S.L.; Bohórquez-Medina, A.L.; Benites Zapata, V.A.; Ignacio-Cconchoy, F.L.; Toro-Huamanchumo, C.J.; Bendezu-Quispe, G.; Pacheco-Mendoza, J.; Hernandez, A.V. Impact of Spirulina Supplementation on Obesity-Related Metabolic Disorders: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. NFS J. 2021, 25, 21–30. [Google Scholar] [CrossRef]
- Hatami, E.; Ghalishourani, S.-S.; Najafgholizadeh, A.; Pourmasoumi, M.; Hadi, A.; Clark, C.C.T.; Assaroudi, M.; Salehi-sahlabadi, A.; Joukar, F.; Mansour-Ghanaei, F. The Effect of Spirulina on Type 2 Diabetes: A Systematic Review and Meta-Analysis. J. Diabetes Metab. Disord. 2021, 20, 883–892. [Google Scholar] [CrossRef]
- Huang, H.; Liao, D.; Pu, R.; Cui, Y. Quantifying the Effects of Spirulina Supplementation on Plasma Lipid and Glucose Concentrations, Body Weight, and Blood Pressure. Diabetes Metab. Syndr. Obes. Targets Ther. 2018, 11, 729–742. [Google Scholar] [CrossRef] [Green Version]
- Mazloomi, S.M.; Samadi, M.; Davarpanah, H.; Babajafari, S.; Clark, C.C.T.; Ghaemfar, Z.; Rezaiyan, M.; Mosallanezhad, A.; Shafiee, M.; Rostami, H. The Effect of Spirulina Sauce, as a Functional Food, on Cardiometabolic Risk Factors, Oxidative Stress Biomarkers, Glycemic Profile, and Liver Enzymes in Nonalcoholic Fatty Liver Disease Patients: A Randomized Double-blinded Clinical Trial. Food Sci. Nutr. 2021, 10, 317–328. [Google Scholar] [CrossRef]
- Mazokopakis, E.E.; Papadomanolaki, M.G.; Fousteris, A.A.; Kotsiris, D.A.; Lampadakis, I.M.; Ganotakis, E.S. The Hepatoprotective and Hypolipidemic Effects of Spirulina (Arthrospira Platensis) Supplementation in a Cretan Population with Non-Alcoholic Fatty Liver Disease: A Prospective Pilot Study. Ann. Gastroenterol. Q. Publ. Hell. Soc. Gastroenterol. 2014, 27, 387–394. [Google Scholar]
- Ou, Y.; Lin, L.; Pan, Q.; Yang, X.; Cheng, X. Preventive Effect of Phycocyanin from Spirulina Platensis on Alloxan-Injured Mice. Environ. Toxicol. Pharmacol. 2012, 34, 721–726. [Google Scholar] [CrossRef]
- Gupta, M.; Dwivedi, U.N.; Khandelwal, S. C-Phycocyanin: An Effective Protective Agent against Thymic Atrophy by Tributyltin. Toxicol. Lett. 2011, 204, 2–11. [Google Scholar] [CrossRef]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A Simple and Accurate Predictor of Hepatic Steatosis in the General Population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef] [Green Version]
- Birkett, M.A.; Day, S.J. Internal Pilot Studies for Estimating Sample Size. Stat. Med. 1994, 13, 2455–2463. [Google Scholar] [CrossRef]
- Browne, R.H. On the Use of a Pilot Sample for Sample Size Determination. Stat. Med. 1995, 14, 1933–1940. [Google Scholar] [CrossRef]
- Julious, S.A. Sample Size of 12 per Group Rule of Thumb for a Pilot Study. Pharm. Stat. 2005, 4, 287–291. [Google Scholar] [CrossRef]
- Hertzog, M.A. Considerations in Determining Sample Size for Pilot Studies. Res. Nurs. Health 2008, 31, 180–191. [Google Scholar] [CrossRef]
- Sim, J.; Lewis, M. The Size of a Pilot Study for a Clinical Trial Should Be Calculated in Relation to Considerations of Precision and Efficiency. J. Clin. Epidemiol. 2012, 65, 301–308. [Google Scholar] [CrossRef]
- Teare, M.D.; Dimairo, M.; Shephard, N.; Hayman, A.; Whitehead, A.; Walters, S.J. Sample Size Requirements to Estimate Key Design Parameters from External Pilot Randomised Controlled Trials: A Simulation Study. Trials 2014, 15, 264. [Google Scholar] [CrossRef]
| Variables | Placebo (n = 20) | Spirulysat® (n = 20) |
|---|---|---|
| Age (years) | 48.1 ± 11.01 | 51.8 ± 8.52 |
| Gender: | ||
| Male (n, %) | 11 (55.0) | 11 (55.0) |
| Female (n, %) | 9 (45.0) | 9 (45.0) |
| BMI (kg/m2) | 29.73 ± 2.74 | 29.65 ± 2.72 |
| Waist circumference (cm) | 100 ± 7 | 100 ± 6 |
| Triglycerides (g/L) | 1.83 ± 0.82 | 1.35 ± 0.46 |
| Total cholesterol (g/L) | 2.36 ± 0.46 | 2.33 ± 0.36 |
| LDL cholesterol (g/L) | 1.53 ± 0.36 | 1.52 ± 0.33 |
| HDL cholesterol (g/L) | 0.47 ± 0.13 | 0.54 ± 0.09 |
| Amount in 100 mL | |
|---|---|
| Proteins | ˃0.2 g |
| Carbohydrate | 0.05 g |
| Lipids | Traces |
| Vitamin B12 | 0.3 µg |
| Iron | 0.2 mg |
| Magnesium | 30 mg |
| Calcium | 40 mg |
| Potassium | 8 mg |
| Sodium | 20 mg |
| Copper | 30 µg |
| Zinc | 20 µg |
| Phycocyanine | 110 mg |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koite, N.L.N.; Sanogo, N.I.; Lépine, O.; Bard, J.-M.; Ouguerram, K. Antioxidant Efficacy of a Spirulina Liquid Extract on Oxidative Stress Status and Metabolic Disturbances in Subjects with Metabolic Syndrome. Mar. Drugs 2022, 20, 441. https://doi.org/10.3390/md20070441
Koite NLN, Sanogo NI, Lépine O, Bard J-M, Ouguerram K. Antioxidant Efficacy of a Spirulina Liquid Extract on Oxidative Stress Status and Metabolic Disturbances in Subjects with Metabolic Syndrome. Marine Drugs. 2022; 20(7):441. https://doi.org/10.3390/md20070441
Chicago/Turabian StyleKoite, N’Deye Lallah Nina, N’gouro Issa Sanogo, Olivier Lépine, Jean-Marie Bard, and Khadija Ouguerram. 2022. "Antioxidant Efficacy of a Spirulina Liquid Extract on Oxidative Stress Status and Metabolic Disturbances in Subjects with Metabolic Syndrome" Marine Drugs 20, no. 7: 441. https://doi.org/10.3390/md20070441
APA StyleKoite, N. L. N., Sanogo, N. I., Lépine, O., Bard, J.-M., & Ouguerram, K. (2022). Antioxidant Efficacy of a Spirulina Liquid Extract on Oxidative Stress Status and Metabolic Disturbances in Subjects with Metabolic Syndrome. Marine Drugs, 20(7), 441. https://doi.org/10.3390/md20070441