Effect of Omega-3 Polyunsaturated Fatty Acids Treatment on Lipid Pattern of HIV Patients: A Meta-Analysis of Randomized Clinical Trials

 ,
, 
 and
and 
Abstract
1. Introduction
2. Results
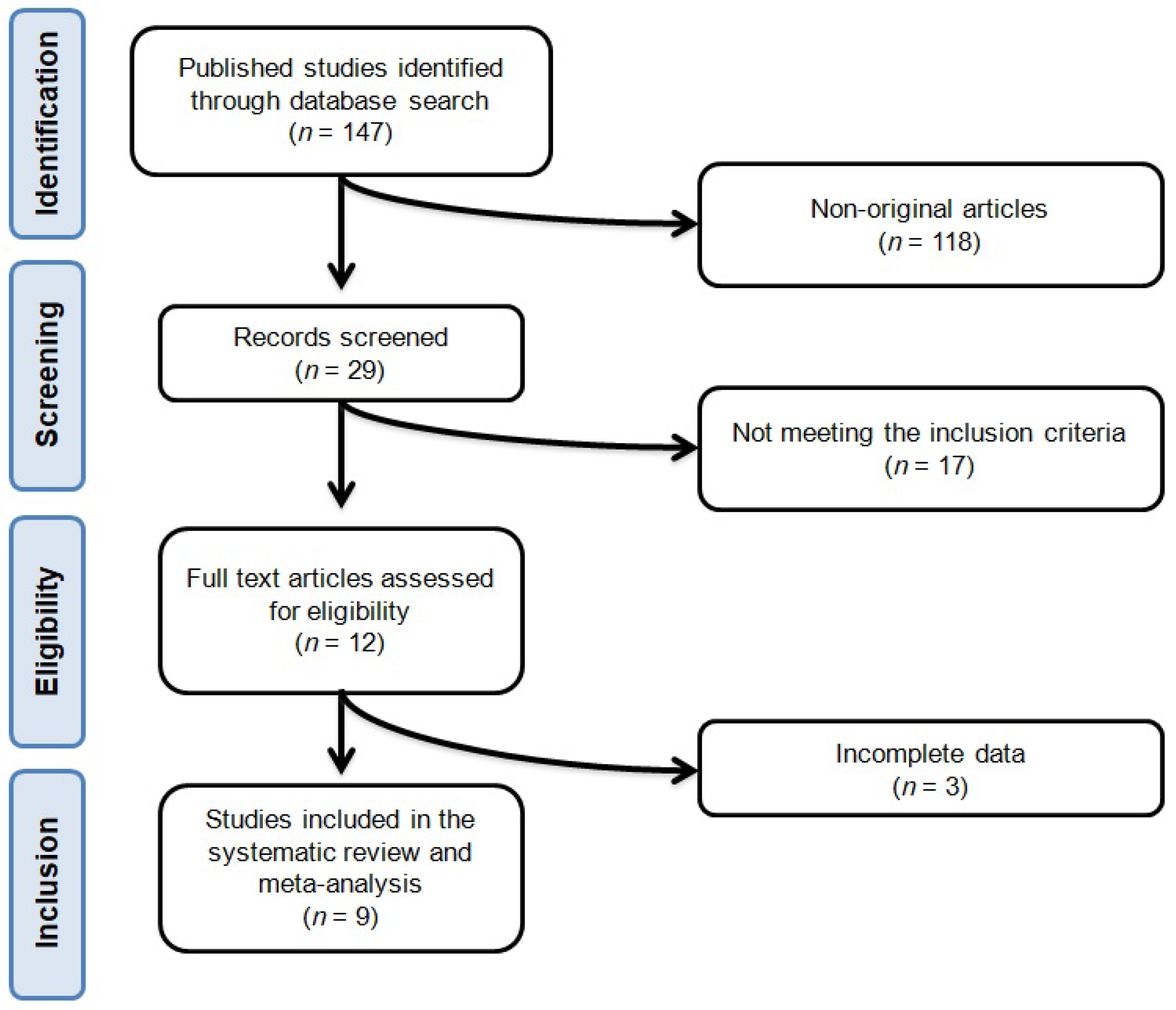
2.1. Flow and Characteristics of the Included Studies
2.2. Risk of Bias Assessment
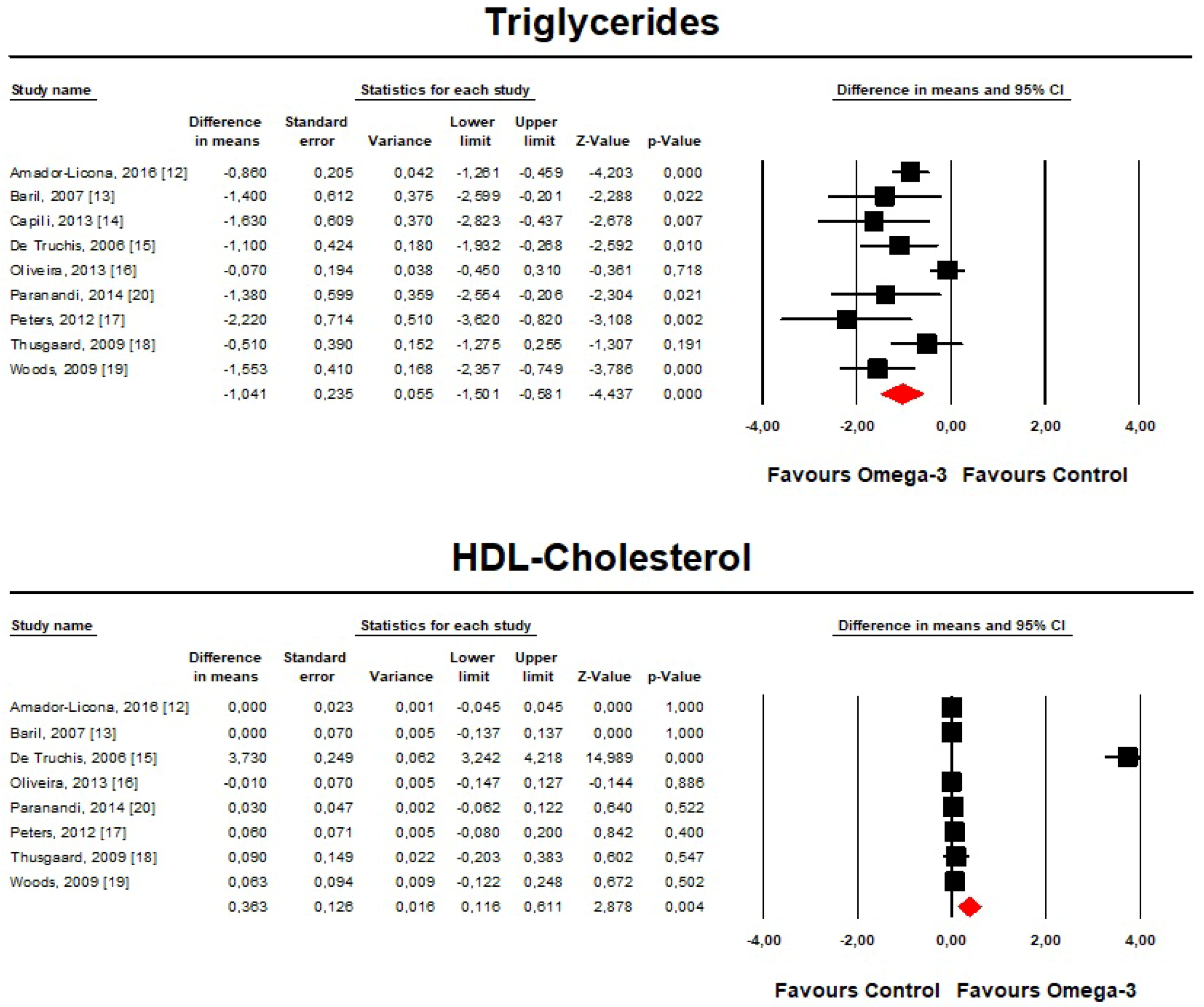
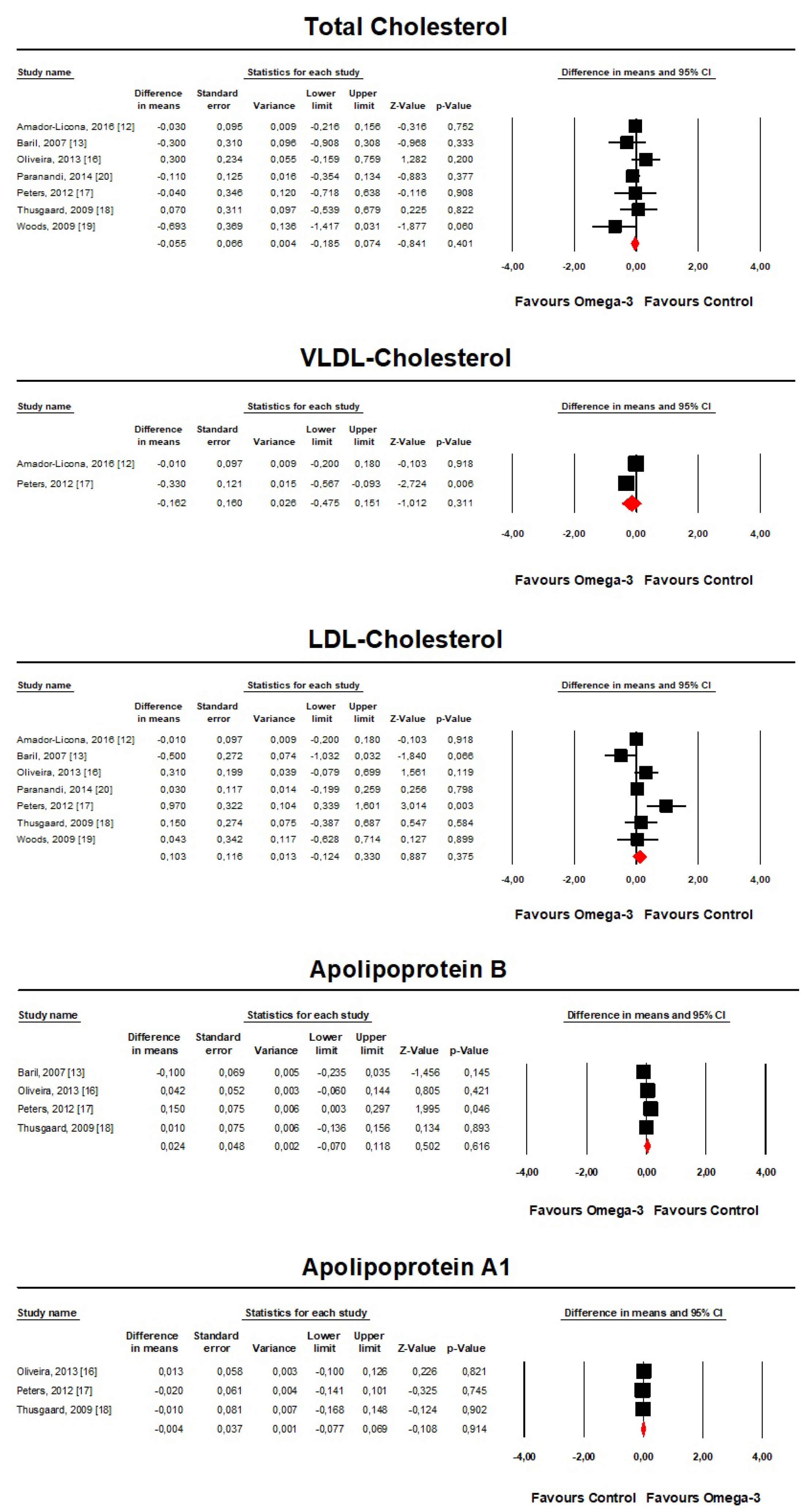
2.3. Lipid-Lowering Effect of Omega-3 Polyunsaturated Fatty Acids
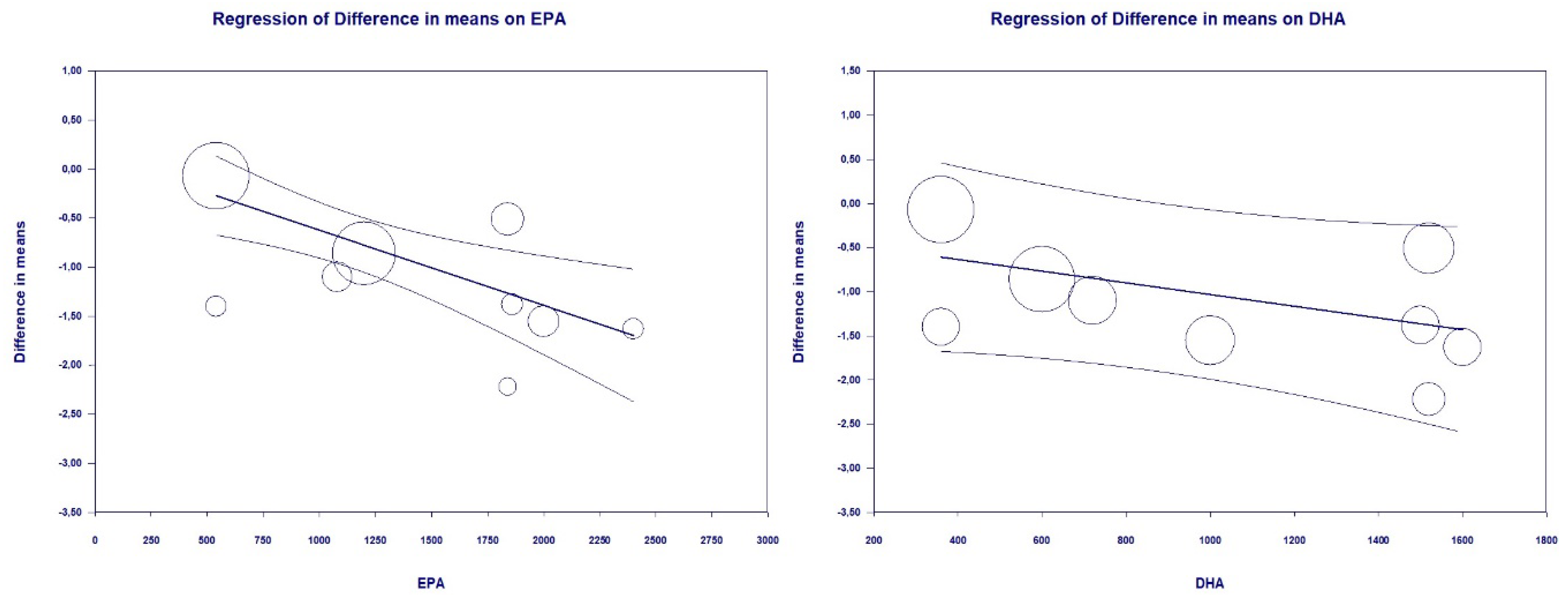
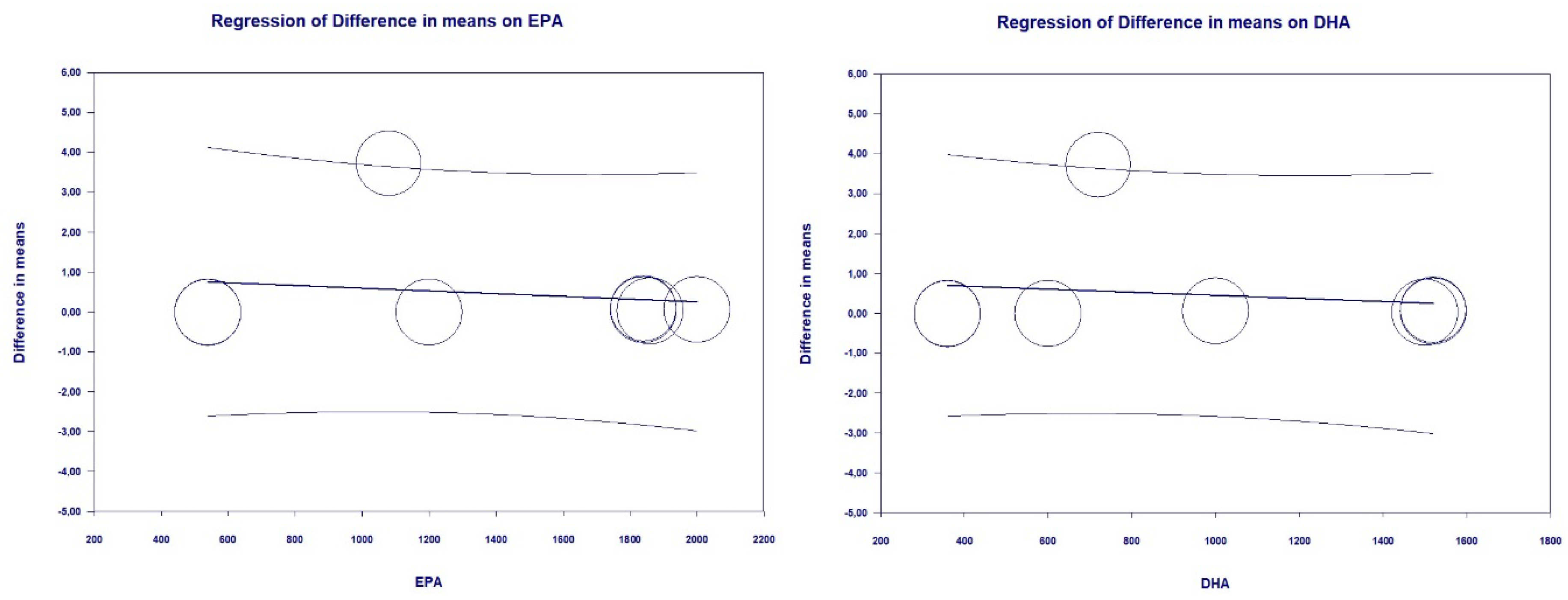
2.4. Differential Effectiveness of EPA and DHA on Lipids
2.5. Safety Analysis for Omega-3 Fatty Acids Administration
3. Discussion
4. Materials and Methods
4.1. Search Strategy
4.2. Study Selection Criteria
4.3. Data Extraction
4.4. Quality Assessment
4.5. Data Synthesis
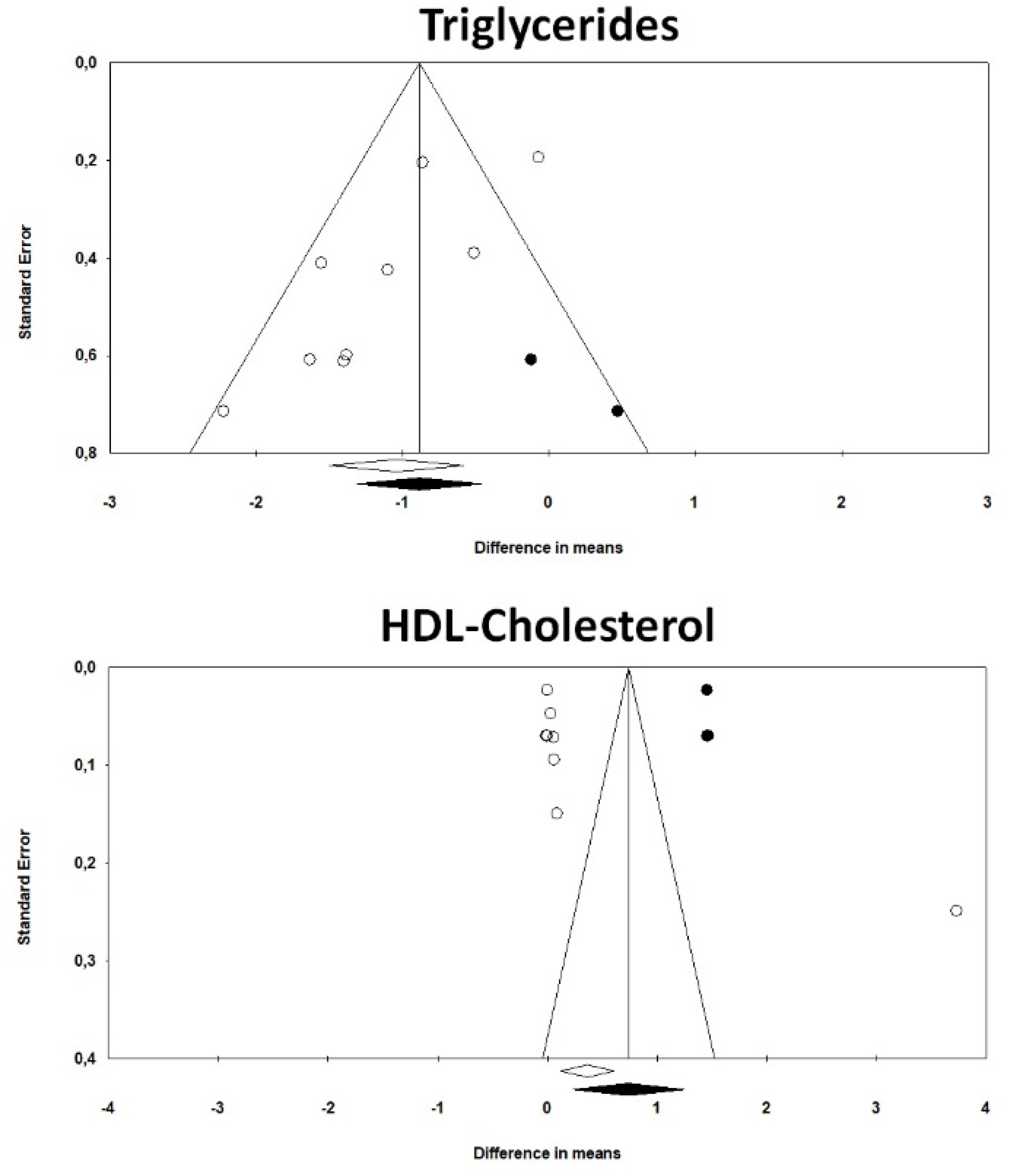
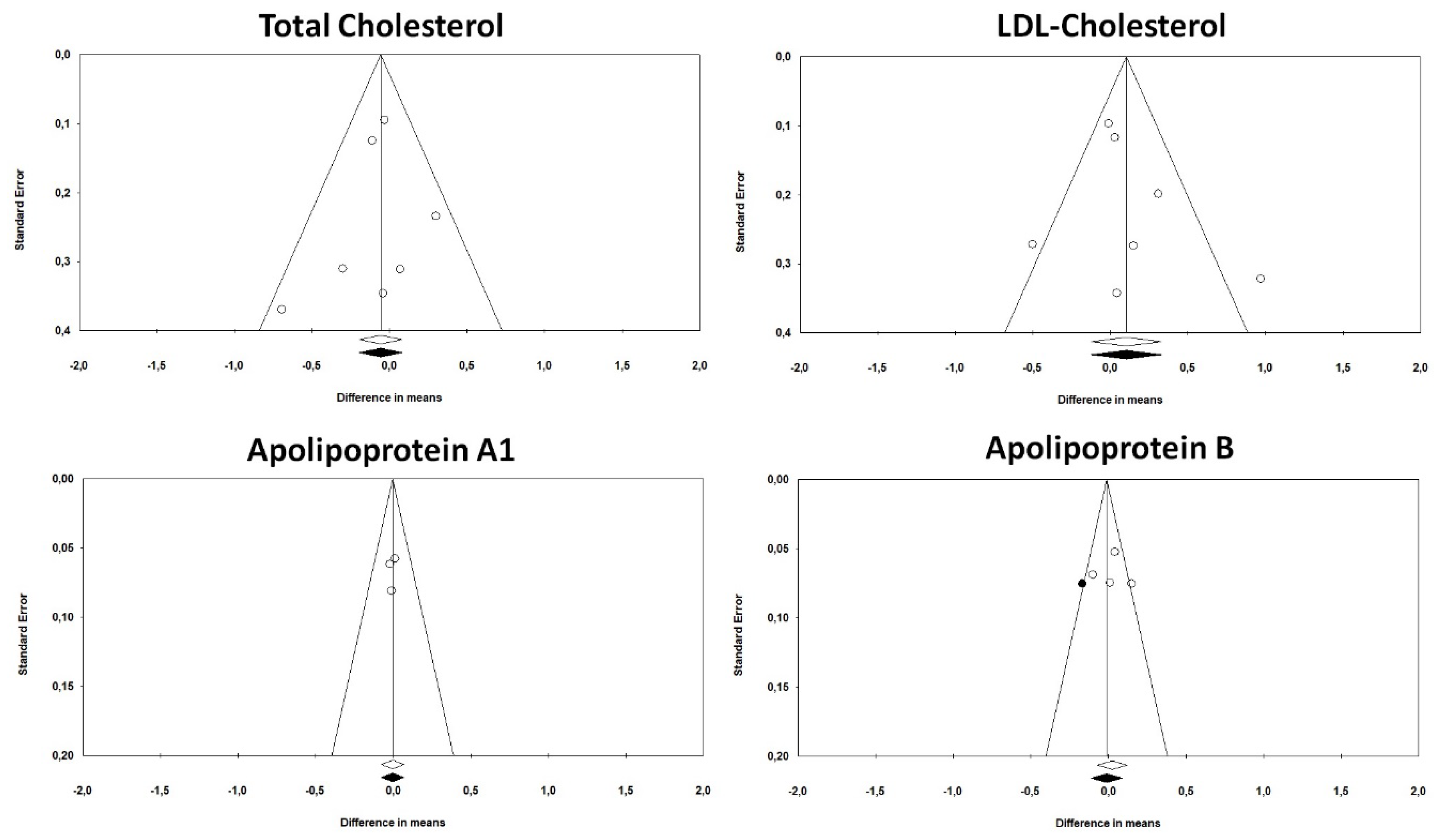
4.6. Publication Biases
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Grand, M.; Bia, D.; Diaz, A. Cardiovascular Risk Assessment in People Living With HIV: A Systematic Review and Meta-Analysis of Real-Life Data. Curr. HIV Res. 2020, 18, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Worm, S.W.; Kamara, D.A.; Reiss, P.; Kirk, O.; El-Sadr, W.; Fux, C.; Fontas, E.; Phillips, A.; D’Arminio Monforte, A.; De Wit, S.; et al. Elevated triglycerides and risk of myocardial infarction in HIV-positive persons. AIDS 2011, 25, 1497–1504. [Google Scholar] [CrossRef] [PubMed]
- Fontas, E.; van Leth, F.; Sabin, C.A.; Friis-Møller, N.; Rickenbach, M.; D’Arminio Monforte, A.; Kirk, O.; Dupon, M.; Morfeldt, L.; Mateu, S.; et al. Lipid profiles in HIV-infected patients receiving combination antiretroviral therapy: Are different antiretroviral drugs associated with different lipid profiles? J. Infect. Dis. 2004, 189, 1056–1074. [Google Scholar] [CrossRef] [PubMed]
- Dubé, M.P.; Stein, J.H.; Aberg, J.A.; Fichtenbaum, C.J.; Gerber, J.G.; Tashima, K.T.; Henry, W.K.; Currier, J.S.; Sprecher, D.; Glesby, M.J. Guidelines for the evaluation and management of dyslipidemia in human immunodeficiency virus (HIV)-infected adults receiving antiretroviral therapy: Recommendations of the HIV Medical Association of the Infectious Disease Society of America and the Adult AIDS Clinical Trials Group. Clin. Infect. Dis. 2003, 37, 613–627. [Google Scholar]
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Domingo, P.; Gallego-Escuredo, J.M.; Fernández, I.; Villarroya, J.; Torres, F.; Del Mar Gutierrez, M.; Mateo, M.G.; Villarroya, F.; Vidal, F.; Giralt, M.; et al. Effects of docosahexanoic acid supplementation on inflammatory and subcutaneous adipose tissue gene expression in HIV-infected patients on combination antiretroviral therapy (cART). A sub-study of a randomized, double-blind, placebo-controlled study. Cytokine 2018, 105, 73–79. [Google Scholar] [CrossRef]
- Gebhardt, A.; Fichtenbaum, C.J. Current pharmacotherapy for the treatment of dyslipidemia associated with HIV infection. Expert Opin. Pharmacother. 2019, 20, 1719–1729. [Google Scholar] [CrossRef]
- Muñoz, M.A.; Liu, W.; Delaney, J.A.; Brown, E.; Mugavero, M.J.; Mathews, W.C.; Napravnik, S.; Willig, J.H.; Eron, J.J.; Hunt, P.W.; et al. Comparative effectiveness of fish oil versus fenofibrate, gemfibrozil, and atorvastatin on lowering triglyceride levels among HIV-infected patients in routine clinical care. J. Acquir. Immune Defic. Syndr. 2013, 64, 254–260. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products NaAN. Scientific Opinion on the substantiation of health claims related to EPA, DHA, DPA and maintenance of normal blood pressure (ID 502), maintenance of normal HDL-cholesterol concentrations (ID 515), maintenance of normal (fasting) blood concentrations of triglycerides (ID 517), maintenance of normal LDL-cholesterol concentrations (ID 528, 698) and maintenance of joints (ID 503, 505, 507, 511, 518, 524, 526, 535, 537) pursuant to Article 13(1) of Regulation (EC) No 1924/2006. EFSA J. 2009, 7, 1263–1289. [Google Scholar]
- Howe, P.; Mori, T.; Buckley, J. Long Chain Omega-3 Fatty Acids and Cardiovascular Disease-FSANZ Consideration of a Commissioned Review. FSANZ 2013; 1–8. Available online:http://www.foodstandards.gov.au (accessed on 25 May 2020).
- Miller, M.; Stone, N.J.; Ballantyne, C.; Bittner, V.; Criqui, M.H.; Ginsberg, H.N.; Goldberg, A.C.; Howard, W.J.; Jacobson, M.S.; Kris-Etherton, P.M.; et al. American Heart Association Clinical Lipidology, Thrombosis, and Prevention Committee of the Council on Nutrition, Physical Activity, and Metabolism; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Nursing; Council on the Kidney in Cardiovascular Disease. Triglycerides and cardiovascular disease: A scientific statement from the American Heart Association. Circulation 2011, 123, 2292–2333. [Google Scholar]
- Amador-Licona, N.; Díaz-Murillo, T.A.; Gabriel-Ortiz, G.; Pacheco-Moises, F.P.; Pereyra-Nobara, T.A.; Guízar-Mendoza, J.M.; Barbosa-Sabanero, G.; Orozco-Aviña, G.; Moreno-Martínez, S.C.; Luna-Montalbán, R.; et al. Omega 3 Fatty Acids Supplementation and Oxidative Stress in HIV-Seropositive Patients. A Clinical Trial. PLoS ONE 2016, 11, e0151637. [Google Scholar] [CrossRef]
- Baril, J.G.; Kovacs, C.M.; Trottier, S.; Roederer, G.; Martel, A.Y.; Ackad, N.; Koulis, T.; Sampalis, J.S. Effectiveness and tolerability of oral administration of low-dose salmon oil to HIV patients with HAART-associated dyslipidemia. HIV Clin. Trials 2007, 8, 400–411. [Google Scholar] [CrossRef]
- Capili, B.; Anastasi, J.K. Exploratory study: Evaluating the effects of fishoil and controlled diet reduce triglyceride levels in HIV. J. Assoc. Nurses AIDS Care 2013, 24, 276–282. [Google Scholar] [CrossRef]
- De Truchis, P.; Kirstetter, M.; Perier, A.; Meunier, C.; Zucman, D.; Force, G.; Doll, J.; Katlama, C.; Rozenbaum, W.; Masson, H.; et al. Reduction in triglyceride level with N-3 polyunsaturated fatty acids in HIV-infected patients taking potent antiretroviral therapy: A randomized prospective study. J. Acquir. Immune Defic. Syndr. 2007, 44, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, J.M.; Rondó, P.H.; Yudkin, J.S.; Souza, J.M.; Pereira, T.N.; Catalani, A.W.; Picone, C.M.; Segurado, A.A. Effects of fish oil on lipid profile and other metabolic outcomes in HIV-infected patients on antiretroviral therapy: A randomized placebo-controlled trial. Int. J. STD AIDS 2014, 25, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Peters, B.S.; Wierzbicki, A.S.; Moyle, G.; Nair, D.; Brockmeyer, N. The effect of a 12-week course of omega-3 polyunsaturated fatty acids on lipid parameters in hypertriglyceridemic adult HIV-infected patients undergoing HAART: A randomized, placebo-controlled pilot trial. Clin. Ther. 2012, 34, 67–76. [Google Scholar] [CrossRef]
- Thusgaard, M.; Christensen, J.H.; Mørn, B.; Andersen, T.S.; Vige, R.; Arildsen, H.; Schmidt, E.B.; Nielsen, H. Effect of fish oil (n-3 polyunsaturated fatty acids) on plasma lipids, lipoproteins and inflammatory markers in HIV-infected patients treated with antiretroviral therapy: A randomized, double-blind, placebo-controlled study. Scand. J. Infect. Dis. 2009, 41, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Woods, M.N.; Wanke, C.A.; Ling, P.R.; Hendricks, K.M.; Tang, A.M.; Knox, T.A.; Andersson, C.E.; Dong, K.R.; Skinner, S.C.; Bistrian, B.R. Effect of a dietary intervention and n-3 fatty acid supplementation on measures of serum lipid and insulin sensitivity in persons with HIV. Am. J. Clin. Nutr. 2009, 90, 1566–1578. [Google Scholar] [CrossRef]
- Paranandi, A.; Asztalos, B.F.; Mangili, A.; Kuvin, J.; Gerrior, J.; Sheehan, H.; Skinner, S.C.; Tang, A.M.; Wanke, C.A. Short communication: Effects of omega-3 fatty acids on triglycerides and high-density lipoprotein subprofiles in HIV-infected persons with hypertriglyceridemia. AIDS Res. Hum. Retrovir. 2014, 30, 800–805. [Google Scholar] [CrossRef]
- Oliveira, J.M.; Rondó, P.H. Omega-3 fatty acids and hypertriglyceridemia in HIV-infected subjects on antiretroviral therapy: Systematic review and meta-analysis. HIV Clin. Trials 2011, 12, 268–274. [Google Scholar] [CrossRef]
- Gutierrez, M.D.M.; Mateo, M.G.; Corbacho, N.; Vidal, F.; Domingo, P. Drug-drug interactions when treating HIV-related metabolic disorders. Expert Opin. Drug Metab. Toxicol. 2019, 15, 787–802. [Google Scholar] [CrossRef]
- Fitch, K.V. Contemporary Lifestyle Modification Interventions to Improve Metabolic Comorbidities in HIV. Curr. HIV/AIDS Rep. 2019, 16, 482–491. [Google Scholar] [CrossRef]
- Sun, H.Y.; Chang, S.Y.; Sheng, W.H.; Chen, M.Y.; Hsieh, S.M.; Tseng, Y.T.; Lu, C.L.; Yang, C.J.; Wu, H.; Liu, W.C.; et al. Incidence of acute pancreatitis in human immunodeficiency virus-positive patients with hypertriglyceridemia: Is it really high? Pancreas 2012, 41, 283–289. [Google Scholar] [CrossRef]
- Madruga, J.R.; Cassetti, I.; Suleiman, J.M.; Etzel, A.; Zhong, L.; Holmes, C.B.; Cheng, A.K.; Enejosa, J.; Study 903E Team. The safety and efficacy of switching stavudine to tenofovir df in combination with lamivudine and efavirenz in hiv-1-infected patients: Three-year follow-up after switching therapy. HIV Clin. Trials 2007, 8, 381–390. [Google Scholar] [CrossRef]
- Laufs, U.; Parhofer, K.G.; Ginsberg, H.N.; Hegele, R.A. Clinical review on triglycerides. Eur. Heart J. 2020, 41, 99–109c. [Google Scholar] [CrossRef]
- Harris, W.S.; Bulchandani, D. Why do omega-3 fatty acids lower serum triglycerides? Curr. Opin. Lipidol. 2006, 17, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Abdelhamid, A.S.; Brown, T.J.; Brainard, J.S.; Biswas, P.; Thorpe, G.C.; Moore, H.J.; Deane, K.H.; Summerbell, C.D.; Worthington, H.V.; Song, F.; et al. Omega-3 fatty acids for the primary and secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2020, 3, CD003177. [Google Scholar] [CrossRef] [PubMed]
- Eyawo, O.; Brockman, G.; Goldsmith, C.H.; Hull, M.W.; Lear, S.A.; Bennett, M.; Guillemi, S.; Franco-Villalobos, C.; Adam, A.; Mills, E.J.; et al. Risk of myocardial infarction among people living with HIV: An updated systematic review and meta-analysis. BMJ Open 2019, 9, e025874. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.; Reggi, A.; Parini, A.; Borghi, C. Application of polyunsaturated fatty acids in internal medicine: Beyond the established cardiovascular effects. Arch. Med. Sci. 2012, 8, 784–793. [Google Scholar] [CrossRef] [PubMed]
- Cicero, A.F.; Morbini, M.; Borghi, C. Do we need ‘new’ omega-3 polyunsaturated fatty acids formulations? Expert Opin. Pharmacother. 2015, 16, 285–288. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.0. 2. 2009; Ref Type: Report; John Wiley and Sons Ltd.: Chichester, UK, 2010. [Google Scholar]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Comprehensive Meta-Analysis Version 3; Biostatistics: Englewood, NJ, USA, 2005; Volume 104. [Google Scholar]
- Follmann, D.; Elliott, P.; Suh, I.; Cutler, J. Variance imputation for overviews of clinical trials with continuous response. J. Clin. Epidemiol. 1992, 45, 769–773. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef]
- Melsen, W.G.; Bootsma, M.C.; Rovers, M.M.; Bonten, M.J. The effects of clinical and statistical heterogeneity on the predictive values of results from meta-analyses. Clin. Microbiol. Infect. 2014, 20, 123–129. [Google Scholar] [CrossRef]
- Haenszel, W.; Hon, N.B. Statistical approaches to the study of cancer with particular reference to case registers. J. Clin. Epidemiol. 1956, 4, 589–599. [Google Scholar] [CrossRef]
- Bown, M.J.; Sutton, A.J. Quality control in systematic reviews and meta-analyses. Eur. J. Vasc. Endovasc. Surg. 2010, 40, 669–677. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Sterne, J.A.; Gavaghan, D.; Egger, M. Publication and related bias in meta-analysis: Power of statistical tests and prevalence in the literature. J. Clin. Epidemiol. 2000, 53, 1119–1129. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Study Design | Follow-Up | Main Inclusion Criteria | Study Group | Patients (n) | Male (n (%)) | Age (Years; Mean ± SD) | Years Since HIV Diagnosis (Mean ± SD) | Years Since ART Therapy Started (Mean ± SD) | CD4+ T Cell Count (cell/mL) |
|---|---|---|---|---|---|---|---|---|---|---|
| Amador-Licona, 2016 [12] | Randomized, double-blind, placebo-controlled, parallel-group, clinical study | 6 months | HIV infection treated with stable HAART regimen for ≥ 3 months; TG ≥ 2.26 mmol/L and ≤ 5.65 mmol/L; LDL-C ≥ 3.36 mmol/L and ≤ 4.13 mmol/L; CD4+ T cell count> 200 cell/mL | 2.4 g/day omega-3 PUFA (EPA/DHA 1200/600 mg/day) | 35 | 28 (80) | 39.9 ± 9.5 | 5.6 ± 2 | 4.5 ± 1.7 | 525.7 ± 129.6 |
| Placebo | 30 | 23 (65.7) | 39.9 ± 8 | 6.8 ± 2.2 | 5.4 ± 2 | 663.7 ± 180 | ||||
| Baril, 2007 [13] | Multicenter, randomized, open-label, placebo-controlled, parallel-group, clinical study | 12 weeks | HIV infection treated with stable ARV regimen for ≥6 months; TG ≥ 6 mmol/L and ≤ 6 mmol/L | 3 g/day salmon oil omega-3 PUFA (EPA/DHA 540/360 mg/day) | 26 | 26 (100) | 50.9 ± 8.4 | 9.9 ± 5.2 | NA | 736 ± 456 |
| Placebo | 32 | 31 (96.9) | 47.8 ± 5.5 | 11.8 ± 5.2 | NA | 540 ± 307 | ||||
| Capili, 2013 [14] | Randomized, double-blind, placebo-controlled, parallel-group, clinical study | 8 weeks | HIV infection treated with stable PI-ART regimen for ≥ 6 months; TG ≥ 1.69 mmol/L and ≤ 5.65 mmol/L; LDL-C < 3.36 mmol/L; CD4+ T cell count ≥ 300 cells/mL | 4 g/day omega-3 PUFA (EPA/DHA 2400/1600 mg/day) | 8 | 6 (75) | 46.9 ± 11.5 | 9.5 ± 6.1 | NA | 573 ± 284 |
| Placebo | 10 | 6 (60) | 45.6 ± 6.5 | 12.6 ± 4.9 | NA | 525 ± 182 | ||||
| De Truchis, 2006 [15] | Multicenter, randomized, double-blind, placebo-controlled, parallel-group, clinical study | 8 weeks | HIV infection treated with stable HAART regimen for ≥ 2 months; TG ≥ 3.43 mmol/L | 6 g/day omega-3 PUFA (EPA/DHA 1080/720 mg/day) | 58 | 52 (89.7) | 45.6 ± 8.6 | 11 ± 4.5 | 7.1 ± 2.8 | NA |
| Placebo | 62 | 55 (88.7) | 47.1 ± 8.4 | 11.6 ± 4.2 | 7.7 ± 3.1 | NA | ||||
| Oliveira, 2013 [16] | Randomized, double-blind, placebo-controlled, parallel-group, clinical study | 24 weeks | HIV infection treated with stable ART regimen for ≥ 3 months; TG > 1.3 mmol/L; LDL-C < 4.14 mmol/L; FPG < 7 mmol/L | 3 g/day omega-3 PUFA (EPA/DHA 540/360 mg/day) | 63 | 33 (76.7) | 43.1 ± 7.4 | 10.3 ± 5.7 | 8.3 ± 4.1 | 591.8 ± 259.6 |
| Placebo | 40 | 31 (77.5) | 42.8 ± 6.3 | 10.9 ± 5 | 9.2 ± 3.5 | 616.2 ± 366.9 | ||||
| Paranandi, 2014 [20] | Randomized, double-blind, placebo controlled, crossover, clinical study | 12 weeks | HIV infection treated with stable HAART regimen for ≥ 3 months; TG ≥ 1.69 mmol/L | 4 g/day omega-3 PUFA (EPA/DHA 1860/1500 mg/day) | 41 | 35 (85) | 51.7 ± 9.6 | 16.7 ± 5.2 | NA | 621.3 ± 277 |
| Placebo | 20 | |||||||||
| Peters, 2012 [17] | Multicenter, randomized, double-blind, placebo-controlled, parallel-group, pilot clinical study | 12 weeks | HIV infection treated with stable HAART regimen for ≥ 3 months; TG ≥ 3.39 mmol/L and ≤ 11.3 mmol/L; lipid-lowering treatment with fibrate or niacin | 4 g/day omega-3 PUFA (EPA/DHA 1840/1520 mg/day) | 23 | 23 (100) | 46.1 ± 2.9 | NA | NA | 633 ± 217 |
| Placebo | 25 | 24 (96) | 43.6 ± 8.9 | NA | NA | 546 ± 257 | ||||
| Thusgaard, 2009 [18] | Randomized, double-blind, placebo-controlled, parallel-group, clinical study | 12 weeks | HIV infection treated with stable ART regimen for ≥ 3 months | 3.6 g/day omega-3 PUFA (EPA/DHA 1840/1520 mg/day) | 26 | 19 (73) | 43 ± 10 | NA | 8.1 | 503 ± 306 |
| Placebo | 25 | 21 (84) | 47 ± 11 | NA | 8 | 483 ± 267 | ||||
| Woods, 2009 [19] | Randomized, open label, diet-controlled, parallel-group, clinical study | 10 weeks | HIV infection; TG > 1.69 mmol/L and/or QUICKI score < 0.35 or > 0.30 | 3 g/day omega-3 PUFA (EPA/DHA 2000/1000 mg/day) | 28 | 24 (86) | 46.2 ± 8.2 | NA | NA | 527.3 ± 225.2 |
| Control diet | 26 | 19 (73) | 46.3 ± 5 | NA | NA | 489.7 ± 228.1 |
| Author, Year | Sequence Generation | Allocation Concealment | Blinding of Participants, Personnel and Outcome Assessment | Incomplete Outcome Data | Selective Outcome Reporting | Other Potential Threats to Validity |
|---|---|---|---|---|---|---|
| Amador-Licona, 2016 [12] | L | L | L | L | L | L |
| Baril, 2007 [13] | L | L | L | H | L | H |
| Capili, 2013 [14] | L | L | L | H | H | U |
| De Truchis, 2006 [15] | L | L | L | H | H | U |
| Oliveira, 2013 [16] | L | L | U | L | L | L |
| Paranandi, 2014 [20] | U | U | L | L | L | L |
| Peters, 2012 [17] | L | L | L | L | L | H |
| Thusgaard, 2009 [18] | L | L | L | L | L | L |
| Woods, 2009 [19] | U | U | H | L | U | U |
| Adverse Event | Number of Studies | Odd Ratio | 95% Confidence Interval | Z-Value | p-Value | I2 | |
|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | ||||||
| Renal colic and urinary stones | 2 | 5.34 | 0.61 | 46.59 | 1.517 | 0.129 | 0% |
| Nausea | 2 | 4.33 | 0.47 | 40.4 | 1.287 | 0.198 | 0% |
| Flatulence | 4 | 3.47 | 0.88 | 13.63 | 1.781 | 0.075 | 0% |
| Diarrhea | 5 | 2.3 | 0.79 | 6.72 | 1.528 | 0.127 | 0% |
| Generic gastrointestinal disorders | 3 | 1.25 | 0.55 | 2.82 | 0.534 | 0.593 | 0% |
| Cholelithiasis | 2 | 1.04 | 0.11 | 10.33 | 0.036 | 0.971 | 1% |
| Skin rash | 2 | 1.02 | 0.1 | 10.2 | 0.015 | 0.988 | 0% |
| Heartburn | 2 | 1 | 0.14 | 7.02 | 0.001 | 0.999 | 0% |
| Generic infections | 2 | 0.67 | 0.3 | 1.48 | −0.989 | 0.322 | 0% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fogacci, F.; Strocchi, E.; Veronesi, M.; Borghi, C.; Cicero, A.F.G. Effect of Omega-3 Polyunsaturated Fatty Acids Treatment on Lipid Pattern of HIV Patients: A Meta-Analysis of Randomized Clinical Trials. Mar. Drugs 2020, 18, 292. https://doi.org/10.3390/md18060292
Fogacci F, Strocchi E, Veronesi M, Borghi C, Cicero AFG. Effect of Omega-3 Polyunsaturated Fatty Acids Treatment on Lipid Pattern of HIV Patients: A Meta-Analysis of Randomized Clinical Trials. Marine Drugs. 2020; 18(6):292. https://doi.org/10.3390/md18060292
Chicago/Turabian StyleFogacci, Federica, Enrico Strocchi, Maddalena Veronesi, Claudio Borghi, and Arrigo F. G. Cicero. 2020. "Effect of Omega-3 Polyunsaturated Fatty Acids Treatment on Lipid Pattern of HIV Patients: A Meta-Analysis of Randomized Clinical Trials" Marine Drugs 18, no. 6: 292. https://doi.org/10.3390/md18060292
APA StyleFogacci, F., Strocchi, E., Veronesi, M., Borghi, C., & Cicero, A. F. G. (2020). Effect of Omega-3 Polyunsaturated Fatty Acids Treatment on Lipid Pattern of HIV Patients: A Meta-Analysis of Randomized Clinical Trials. Marine Drugs, 18(6), 292. https://doi.org/10.3390/md18060292