

Associations Between Smoking, Stress, Quality of Life, and Oral Health Among Dental Students in Romania: A Cross-Sectional Study

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Study Group
2.2. Instruments
2.2.1. Lifestyle Questionnaire
2.2.2. DMFT Index
2.2.3. Student Stress Inventory (SSI) Indicator
- Subscale 1 (physical stress) addresses the impact of stress on the body from a physical perspective.
- Subscale 2 (stress in interpersonal relationships) describes how stress influences the ability to have healthy and effective interpersonal relationships.
- Subscale 3 (academic stress) focuses on the stress felt by students due to the desire to acquire advanced academic knowledge and skills in an often insufficient amount of time. This represents a key element of academic stress among students.
- Subscale 4 (environmental stress) examines how the physical and social environment affects an individual’s perceived stress, including their response to external stressors. Environmental stress highlights how the external environment influences the individual self, as well as how a person responds to stressful situations generated by external influences [40,41].
2.2.4. EQ-5D-5L Indicator
2.3. Statistical Analysis
3. Results
3.1. Socio-Demographics
3.2. Lifestyle and Smoking Behaviour
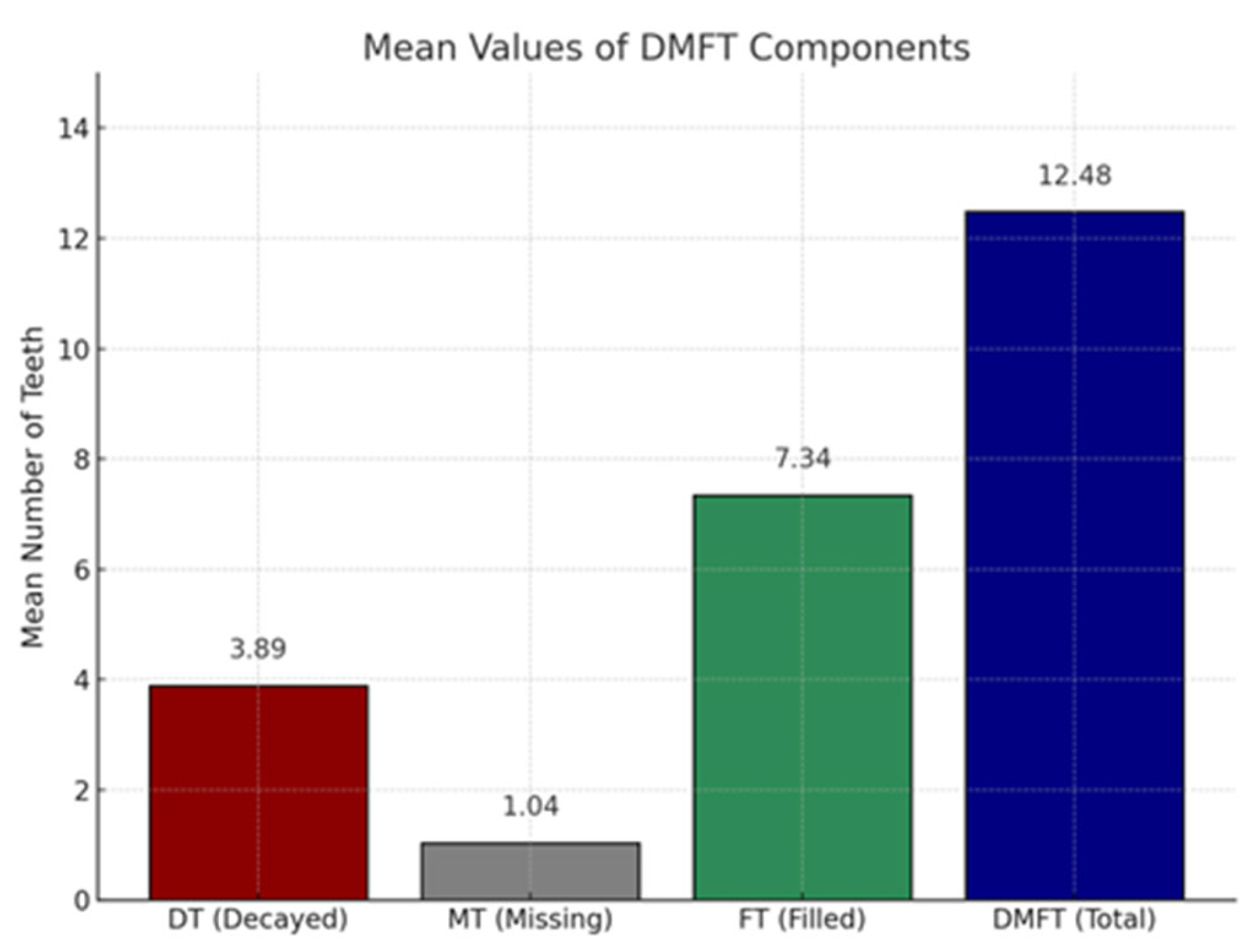
3.3. Oral Health (DMFT Index)
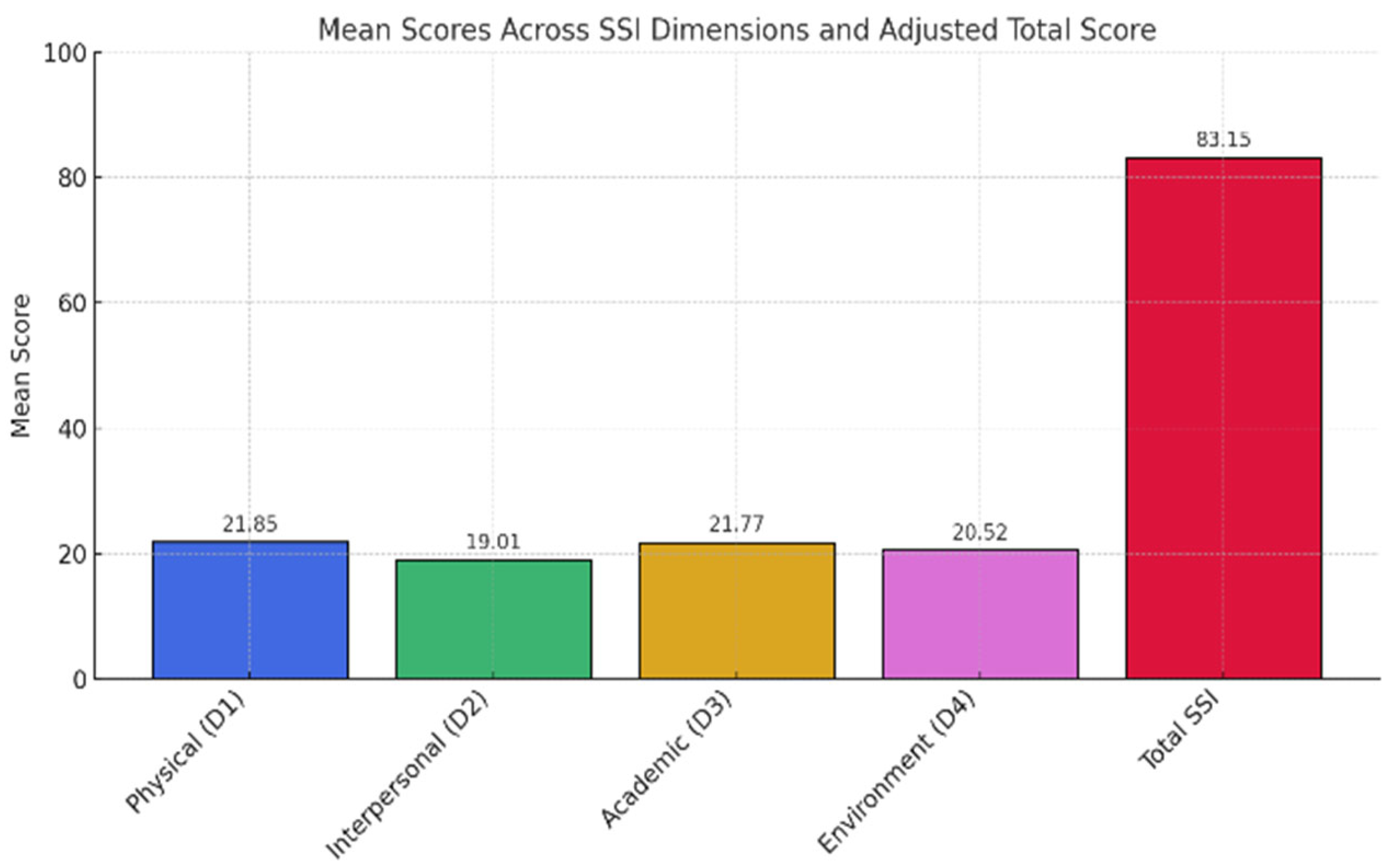
3.4. Perceived Stress (SSI)
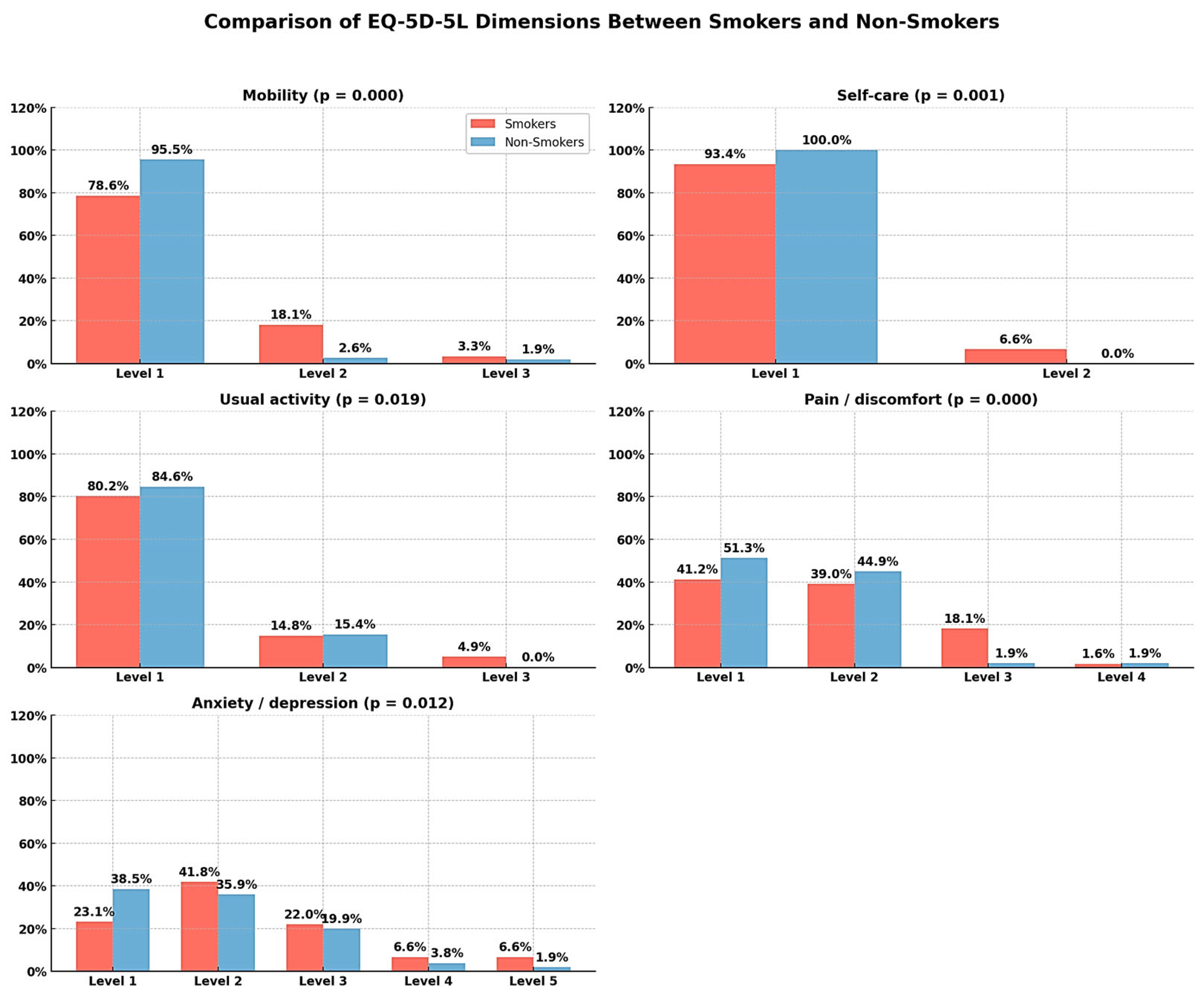
3.5. Quality of Life (EQ-5D-5L)
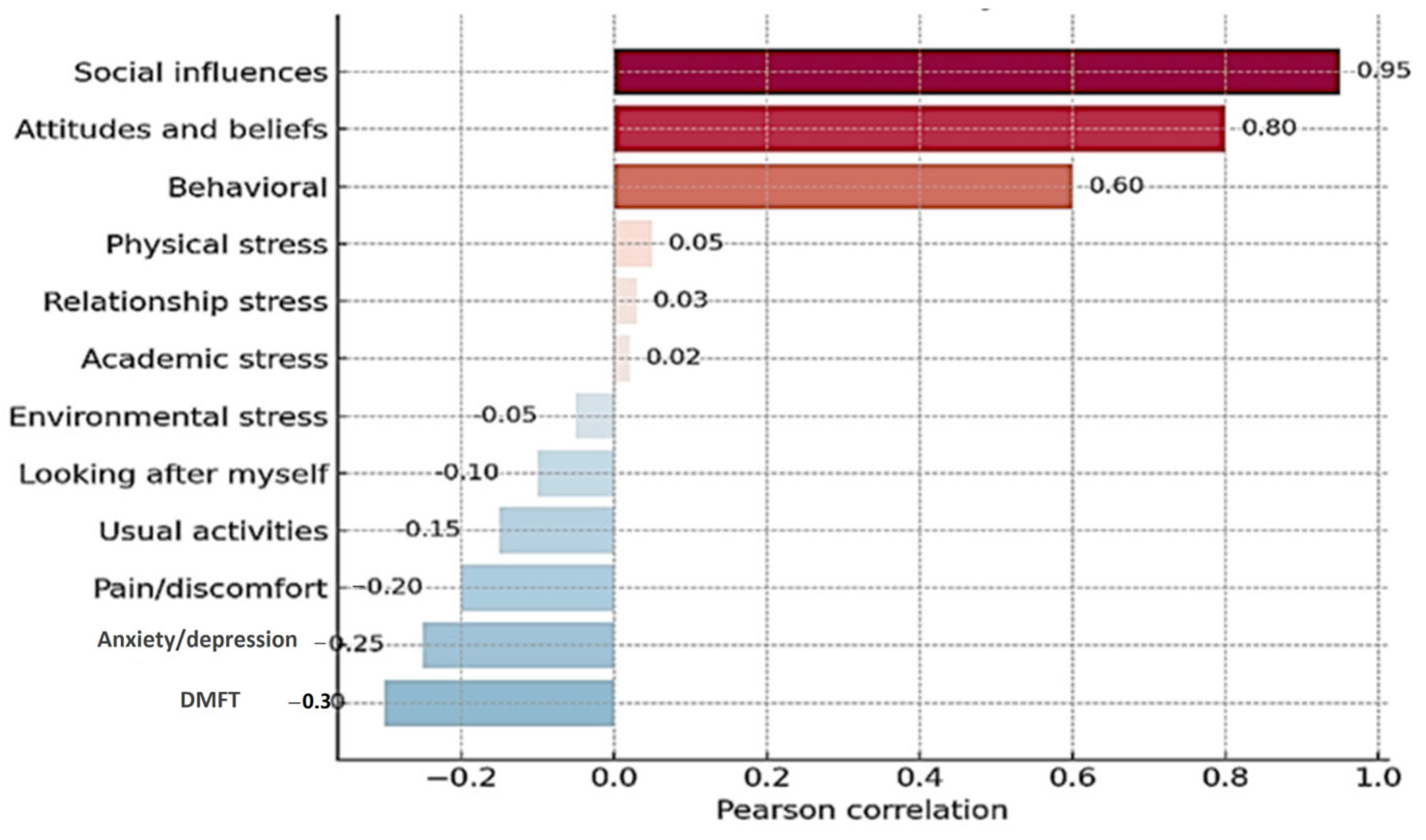
3.6. Correlation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gorter, R.; Freeman, R.; Hammen, S.; Murtomaa, H.; Blinkhorn, A.; Humphris, G. Psychological stress and health in undergraduate dental students: Fifth year outcomes compared with first year baseline results from five European dental schools. Eur. J. Dent. Educ. 2008, 12, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Alzahem, A.M.; van der Molen, H.T.; Alaujan, A.H.; Schmidt, H.G.; Zamakhshary, M.H. Stress amongst dental students: A systematic review. Eur. J. Dent. Educ. 2011, 15, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Al-Sowygh, Z.H. Academic distress, perceived stress and coping strategies among dental students in Saudi Arabia. Saudi Dent. J. 2013, 25, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Folkman, S.; Lazarus, R.S. An analysis of coping in a middle-aged community sample. J. Health Soc. Behav. 1980, 21, 219–239. [Google Scholar] [CrossRef] [PubMed]
- Folkman, S. Stress: Appraisal and Coping. In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 1913–1915. [Google Scholar]
- Alshamrani, A.S.; Alshalan, T.A. Stress among Dental Students: Brief Review and Messages to All Related. Oral Health Dent. Stud. 2021, 2, 5. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Report: Mortality Attributable to Tobacco; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Cardoso, T.C.A.; Rotondano Filho, A.F.; Dias, L.M.; Arruda, J.T. Aspectos associados ao tabagismo e os efeitos sobre a saúde. Res. Soc. Dev. 2021, 10, e11210312975. [Google Scholar] [CrossRef]
- World Health Organization. WHO Report on the Global Tobacco Epidemic, 2011: Warning About the Dangers of Tobacco; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Ben Hassan, S.A.; Kumar, L.; Verma, A.; Mittal, P.; Yadav, A.; Al Malwi, A.A.; Sindi, A.S.; Yassin, S.M.; Shafi, S.; Morsy, M.S.M.; et al. Evaluation of Perceived Stress and Its Association with Dental Caries in 290 Undergraduate Medical Students. Med. Sci. Monit. 2024, 30, e946528. [Google Scholar] [CrossRef]
- Deep, A.; Singh, M.; Sharma, R.; Singh, M.; Mattoo, K.A. Perceived oral health status and treatment needs of dental students. Nat. J. Maxillofac. Sur 2020, 11, 76–80. [Google Scholar] [CrossRef]
- Chan, S.F.; La Greca, A.M. Perceived stress scale (PSS). In Encyclopedia of Behavioral Medicine; Springer International Publishing: Cham, Switzerland, 2020; pp. 1646–1648. [Google Scholar]
- Chaudhary, F.A.; Shakoor, A.; Fareed, M.A.; Khattak, O.; Alqarni, M.S.; Issrani, R.; Alsharari, T. Association of sociodemographic and occupational stress factors with smoking behavior among healthcare professionals: The mediating role of physical exercise. Tob. Induc. Dis. 2025, 23, 66. [Google Scholar] [CrossRef]
- Pereira, E.D.B.; Freitas, E.P.P.; Moreira, B.A.; Paula, F.A.; Santos, R.D.P.; Matos, A.G.C. Impact of smoking on oral health of patients attending an outpatient medical clinic. Rev. Bras. Em Promoção De Saúde 2014, 27, 37–42. [Google Scholar] [CrossRef]
- Soares, A.C.; Taldo Picinini, N.B.; Sayed Picciani, B.L.; Silveira, F.M.; Gomes, C.C.; Videira Assaf, A.; Bastos Valente, M.I. Impact of Smoking on Oral Health-related Quality of Life. Res. Soc. Dev. 2022, 11, e497111436526. [Google Scholar] [CrossRef]
- Ahsan, I.; Menon, I.; Gupta, R.; Sharma, A.; Das, D.; Ashraf, A. Comparison of oral health status among adult tobacco users and non-tobacco users of Ghaziabad District, Uttar Pradesh: A cross sectional study. J. Fam. Med. Prim. Care 2020, 9, 1143–1148. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.S.; Brito, L.N.S.; Monteiro, M.G.; de Farias, R.A.; Cabral, L.P.d.A.; Leite, R.B.; Soares, R.d.S.C.; Bernardino, Í.d.M.; dos Santos, B.R.M.; Gomes, R.C.B. Condição periodontal associada à prática de higiene bucal e ao hábito de fumar de pacientes do serviço de periodontia da Universidade Estadual da Paraíba. Res. Soc. Dev. 2022, 11, e307111032702. [Google Scholar] [CrossRef]
- Alves, A.M.; Correa, M.B.; da Silva, K.D.; de Araújo, L.M.A.; Vasconcelos, A.C.U.; Gomes, A.P.N.; Etges, A.; Chaves Tarquinio, S.B. Demographic and Clinical Profile of Oral Squamous Cell Carcinoma from a Service-Based Population. Braz. Dent. J. 2017, 28, 301–306. [Google Scholar] [CrossRef]
- Lopes, A.C.A.d.S.; Barbosa, K.C.d.O.; Barroso, M.L.F.; Soares, A.L.F.d.H. Brasil: Tabagismo e consumo de bebida alcoólica nos últimos dez anos (vigitel) e o papel do Cirurgião-Dentista na prevenção do câncer bucal. Res. Soc. Dev. 2021, 10, e39110817278. [Google Scholar] [CrossRef]
- Doty, R.L.; Chen, J.H.; Overend, J. Taste quality confusions: Influences of age, smoking, ptc taster status, and other subject characteristics. Perception 2017, 46, 257–267. [Google Scholar] [CrossRef]
- Habibagahi, R.; Navabi, N.; Alsadat Hashemipour, M.; Hashemzehi, A. Does Smoking Cessation Improve Oral Health-related Quality of Life? A Pilot Study. Addict. Health 2020, 12, 167–173. [Google Scholar] [PubMed]
- Asiri, A.; Nazir, M.A.; Alsharief, M.; Shahin, S.; Al-Ansari, A.; Al-Khalifa, K.S. Effect of psychological distress on oral health: A cross-sectional study. BMC Oral Health 2024, 24, 1508. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.; Jeong, W.; Jung, Y. Association Between Self-Perceived Oral Health, Stress, and Oral Symptoms in South Korean University Students: A Cross-Sectional Study. Healthcare 2025, 13, 984. [Google Scholar] [CrossRef]
- Brondani, B.; Silveira Sfreddo, C.; Klöckner Knorst, J.; Hêllwaht Ramadan, Y.; Ruffo Ortiz, F.; Ardenghi, T.M. Oral health-related quality of life as a predictor of alcohol and cigarette consumption in adolescents. Braz. Oral Res. 2022, 36, e025. [Google Scholar] [CrossRef]
- Klotz, A.L.; Tauber, B.; Schubert, A.L.; Hassel, A.J.; Schröder, J.; Wahl, H.W.; Rammelsberg, P.; Zenthöfer, A. Oral health-related quality of life as a predictor of subjective well-being among older adults-A decade-long longitudinal cohort study. Community Dent. Oral Epidemiol. 2018, 46, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Ribeiron, I.J.S.; Pereira, R.; Freire, I.V.; de Oliveira, B.G.; Casotti, C.A.; Boery, E.N. Stress and Quality of Life Among University Students: A Systematic Literature Review. Health Prof. Educ. 2018, 4, 70–77. [Google Scholar]
- Feldens, C.A.; Ardenghi, T.M.; Dos Santos, D.A.I.; Vargas-Ferreira, F.; Hernandez, P.A.; Kramer, P.F. Clarifying the Impact of Untreated and Treated Dental Caries on Oral Health-Related Quality of Life among Adolescents. Caries Res. 2016, 50, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Kear, M.E. Psychosocial determinants of cigarette smoking among college students. J. Community Health Nurs. 2002, 19, 245–257. [Google Scholar] [CrossRef]
- Bakri, N.N.; Tsakos, G.; Masood, M. Smoking Status and Oral Health-related Quality of Life Among Adults in the United Kingdom. Br. Dent. J. 2018, 225, 153–158. [Google Scholar] [CrossRef]
- Sagtani, R.A.; Thapa, S.; Sagtani, A. Smoking, general and oral health related quality of life—A comparative study from Nepal. Health Qual. Life Outcomes 2020, 18, 257. [Google Scholar] [CrossRef]
- De Looze, M.E.; Raaijmakers, Q.A.W.; ter Bogt, T.F.M.; Bendtsen, P.; Farhat, T.; Ferreira, M.; Godeau, E.; Kuntsche, E.; Molcho, M.; Pförtner, T.; et al. Decreases in adolescent weekly alcohol use in Europe and North America: Evidence from 28 countries from 2002 to 2010. Eur. J. Public Health 2015, 25 (Suppl. S2), 69–72. [Google Scholar] [CrossRef]
- White, V.; Williams, T. Australian Secondary School Students’ Use of Tobacco, Alcohol, and Over-the-Counter and Illicit Substances in 2014; Cancer Council Victoria: Melbourne, VIC, Australia, 2014. [Google Scholar]
- WHO. The World Health Organization Quality of Life Assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Miotto, M.H.M.B.; Barcellos, L.A.; Velten, D.B. Evaluation of the impact on quality of life caused by oral health problems in adults and the elderly in a southeastern Brazilian city. Ciência Saúde Coletiva 2012, 17, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Alvarenga, F.A.S.; Henriques, C.; Takatsui, F.; Montandon, A.A.B.; Telarolli, R., Jr.; Monteiro, A.L.C.C.; Pinelli, C.; Loffredo, L.C.M. Oral health impact profile in the quality of life of patients over 50 years old of two public institutions of Araraquara city, SP, Brazil. Rev. Odontol. UNESP 2011, 40, 118–124. [Google Scholar]
- Xia, F.; Hughes, J.P.; Voldal, E.C.; Heagerty, P.J. Power and sample size calculation for stepped-wedge designs with discrete outcomes. Trials 2021, 22, 598. [Google Scholar] [CrossRef] [PubMed]
- Armencia, A.O.; Bamboi, I.; Toader, B.; Rapis, A.; Balcos, C.; Hanganu, C.S.; Nicolau, A. Evaluation of smoking attitudes among young adults: Validation of a smoking behavior measurement questionnaire. Rom. J. Med. Dent. Educ. 2025, 14, 18–25. [Google Scholar]
- WHO. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Minja, I.K. Dental Health Epidemiology; Elsevier Inc.: Amsterdam, The Netherlands, 2025. [Google Scholar]
- Arip, M.A.S.M.; Kamaruzaman, D.N.; Roslan, A.; Ahmad, A. Development, Validity and Reliability of Student Stress Inventory (SSI). Soc. Sci. 2015, 10, 1631–1638. [Google Scholar]
- Monserrat-Hernández, M.; Checa-Olmos, J.C.; Arjona-Garrido, Á.; López-Liria, R.; Rocamora-Pérez, P. Academic Stress in University Students: The Role of Physical Exercise and Nutrition. Healthcare 2023, 11, 2401. [Google Scholar] [CrossRef]
- Simonelli-Muñoza, A.J.; Balanzaa, S.; Rivera-Caravacab, H.M.; Vera-Catalána, T.; Lorentea, A.M.; Gallego-Gómez, J.I. Reliability and validity of the student stress inventory-stress manifestations questionnaire and its association with personal and academic factors in university students. Nurse Educ. Today 2018, 64, 156–160. [Google Scholar] [CrossRef]
- Armencia, A.O.; Bamboi, I.; Toader, B.; Nicolau, A.; Rapis, A.; Balcos, C. Validation of the romanian version of the Student Stress Inventory (SSI). Rom. J. Med. Dent. Educ. 2025, 14, 6–12. [Google Scholar]
- Secnik Boye, K.; Herdman, M.; Ludwig, K.; Kennedy-Martin, M.; Slaap, B.; Verstraete, J. EQ-5D-Y-5L User Guide: How to Apply and Score, and Present Results from the EQ-5D-Y-5L; EuroQol Research Foundation: Rotterdam, The Netherlands, 2024. [Google Scholar]
- Olariu, E.; Mohammed, W.; Oluboyede, Y.; Caplescu, R.; Niculescu-Aron, I.G.; Paveliu, M.S.; Vale, L. EQ-5D-5L: A value set for Romania. Eur. J. Health Econ. 2023, 24, 399–412. [Google Scholar] [CrossRef]
- Olariu, E.; Caplescu, R.; Vale, L.; Niculescu-Aron, I.G.; Oluboyede, Y.; Paveliu, M.S. Population norms for the EQ-5D-3L and EQ-5D-5L in Romania. Health Qual. Life Outcomes 2023, 21, 80. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Report on Trends in Prevalence of Tobacco Use 2000–2025, 3rd ed.; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Milic, M.; Gazibara, T.; Pekmezovic, T.; Kisic Tepavcevic, D.; Maric, G.; Popovic, A.; Stevanovic, J.; Patil, K.H.; Levine, H. Tobacco smoking and health-related quality of life among university students: Mediating effect of depression. PLoS ONE 2020, 15, e0227042. [Google Scholar] [CrossRef] [PubMed]
- Batra, M.; Shah, A.F.; Dany, S.S.; Rajput, P. Determinants related to oral health-related quality of life among subjects attending a dental institute in Morabad city—A cross-sectional study. J. Indian Assoc. Public Health Dent. 2017, 15, 23–26. [Google Scholar]
- Yiengprugsawan, V.; Somkotra, T.; Seubsman, S.; Sleigh, A.C. Oral health-related quality of life among a large national cohort of 87,134 Thai adults. Health Qual. Life Outcomes 2011, 9, 42. [Google Scholar] [CrossRef]
- Caglayan, F.; Altun, O.; Miloglu, O.; Kaya, M.D.; Yilmaz, A.B. Correlation between oral health-related quality of life (OHQOL) and oral disorders in a Turkish patient population. Med. Oral Patol. Oral Cir. Bucal 2009, 14, e573–e578. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Li, M.; Huang, R. The effect of smoking on caries-related microorganisms. Tob. Induc. Dis. 2019, 17, 32. [Google Scholar] [CrossRef] [PubMed]
- Gajendra, S.; McIntosh, S.; Ghosh, S. Effects of tobacco product use on oral health and the role of oral healthcare providers in cessation: A narrative review. Tob. Induc. Dis. 2023, 21, 12. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.; Li, M.; Gregory, R.L. Nicotine promotes Streptococcus mutans extracellular polysaccharide synthesis, cell aggregation and overall lactate dehydrogenase activity. Arch. Oral Biol. 2015, 60, 1083–1090. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Oral Health Surveillance Report: Trends in Dental Caries and Sealants, Tooth Retention, and Edentulism, United States, 1999–2004 to 2011–2016; Centers for Disease Control and Prevention, US Department of Health and Human Services: Atlanta, GA, USA, 2019.
- Campus, G.; Cagetti, M.G.; Senna, A.; Blasi, G.; Mascolo, A.; Demarchi, P.; Strohmenger, L. Does smoking increase risk for caries? A cross-sectional study in an Italian military academy. Caries Res. 2011, 45, 40–46. [Google Scholar] [CrossRef]
- Bernabé, E.; Delgado-Angulo, E.K.; Vehkalahti, M.M.; Aromaa, A.; Suominen, A.L. Daily smoking and 4-year caries increment in Finnish adults. Community Dent. Oral Epidemiol. 2014, 42, 428–434. [Google Scholar] [CrossRef]
- Restrepo, J.E.; Sánchez, O.; Vallejo, G.; Quirama, T.C.; Sánchez, Y.; Cardona, P. Depresión y su relación con el consumo de sustancias psicoactivas, el estrés académico y la ideación suicida en estudiantes universitarios colombianos. Health Addict. 2018, 18, 227–239. [Google Scholar] [CrossRef]
- Vallejo, M.; Valle, J.; Angulo, J. Estrés percibido en estudiantes universitarios: Influencia del burnout y del engagement académico. IJERI 2018, 9, 220–236. [Google Scholar]
- McSharry, P.; Timmins, F. Promoting healthy lifestyle behaviours and well-being among nursing students. Nurs. Stand. 2017, 31, 51–63. [Google Scholar] [CrossRef]
- Cavallo, P.; Carpinelli, L.; Savarese, G. Perceived stress and bruxism in university students. BMC Res. Notes 2016, 9, 514. [Google Scholar] [CrossRef] [PubMed]
- Saleh, D.; Camart, N.; Romo, L. Predictors of stress in college students. Front. Psychol. 2017, 8, 19. [Google Scholar] [CrossRef]
- Heinen, I.; Bullinger, M.; Kocalevent, R.D. Perceived stress in first year medical students—Associations with personal resources and emotional distress. BMC Med. Educ. 2017, 17, 4. [Google Scholar] [CrossRef] [PubMed]
- Jamali, A.; Tofangchiha, S.; Jamali, R.; Nedjat, S.; Delnavaz, J.; Narimani, A.; Montazeri, A. Medical students’ health-related quality of life: Role of social and behavioral factors. Med. Educ. 2013, 47, 1001–1012. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Variable | Frequency | Percentage (%) |
|---|---|---|---|
| Gender | Man | 86 | 25.4 |
| Woman | 252 | 74.6 | |
| Age | 18–20 years old | 7 | 2.1 |
| 21–24 years old | 199 | 58.9 | |
| Over 25 years old | 132 | 39.1 | |
| Year of study | Year III | 69 | 20.4 |
| Year V | 269 | 79.6 | |
| Residence environment | Urban | 207 | 61.2 |
| Rural | 131 | 38.8 | |
| Smoker | Yes | 182 | 53.8 |
| No | 156 | 46.2 |
| Field | Representative Question | Smoker | F | p | |
|---|---|---|---|---|---|
| Yes (Mean Value + DS) | No (Mean Value + DS) | ||||
| Social (Social influences, social pressure, social integration) | “To what extent do you think smoking behaviours are influenced by social factors, such as the perceptions of others, integration into a group, social pressure, and norms associated with smoking?” | 3.09 ± 1.65 | 3.26 ± 1.76 | 4.40 | 0.29 |
| Atittudes (Perceptions about smoking, beliefs, self-efficacy) | “To what extent do you think your personal perceptions about smoking, beliefs about this behaviour, and confidence in your ability to quit smoking influence your smoking decisions?” | 2.96 ± 2.64 | 2.74 ± 1.01 | 5.75 | 0.51 |
| Behavioural (Actual behaviour, behavioural intentions, lifestyle) | “To what extent are your smoking-related behaviours, such as smoking frequency, intentions to quit, and associated habits, influenced by your lifestyle and the social context in which you find yourself?” | 3.49 ± 6.16 | 3.82 ± 8.84 | 3.44 | 0.25 |
| Field | Smoker | F | p | |
|---|---|---|---|---|
| Yes (Mean Value + DS) | No (Mean Value + DS) | |||
| Physical stress | 21.91 ± 4.72 | 21.77 ± 4.49 | 0.073 | 0.787 |
| Interpersonal Relationship Stress | 18.73 ± 4.89 | 19.33 ± 4.66 | 1.357 | 0.245 |
| Academic Stress | 22.00 ± 4.51 | 21.48 ± 5.18 | 0.964 | 0.327 |
| Environmental Stress | 20.78 ± 5.78 | 20.20 ± 5.50 | 0.885 | 0.348 |
| Field | Level (1–5) | Smoker | χ2 | |
|---|---|---|---|---|
| Yes (%) | No (%) | |||
| Mobility | Level 1 | 78.6 | 95.5 | 0.000 |
| Level 2 | 18.1 | 2.6 | ||
| Level 3 | 3.3 | 1.9 | ||
| Self-care | Level 1 | 93.4 | 100 | 0.001 |
| Level 2 | 6.6 | |||
| Usual activity | Level 1 | 80.2 | 84.6 15.4 | 0.019 |
| Level 2 | 14.8 | |||
| Level 3 | 4.9 | |||
| Pain/discomfort | Level 1 | 41.2 | 51.3 | 0.000 |
| Level 2 | 39.0 | 44.9 | ||
| Level 3 | 18.1 | 1.9 | ||
| Level 4 | 1.6 | 1.9 | ||
| Anxiety/depression | Level 1 | 23.1 | 38.5 | 0.012 |
| Level 2 | 41.8 | 35.9 | ||
| Level 3 | 22.0 | 19.9 | ||
| Level 4 | 6.6 | 3.8 | ||
| Level 5 | 6.6 | 1.9 | ||
| Do You Smoke? | n | Mean of DMFT | Std. Deviation | F | Sig. |
|---|---|---|---|---|---|
| Yes | 182 | 24.3901 | 11.74388 | 0.351 | 0.554 |
| No | 156 | 25.1731 | 12.51794 | ||
| Total | 338 | 24.7515 | 12.09546 |
| DMFT a | B | Std. Error | Wald | df | Sig. | Exp(B) | 95% Confidence Interval for Exp(B) | ||
|---|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||||
| DMFT ≤ 10”—sănătate orală relativ bună | Intercept | −1.717 | 0.300 | 32.850 | 1 | 0.000 | |||
| Gender | 0.378 | 0.363 | 1.089 | 1 | 0.297 | 1.460 | 0.717 | 2.971 | |
| Age | 0.415 | 0.310 | 1.788 | 1 | 0.181 | 1.514 | 0.824 | 2.780 | |
| Study year | 1.484 | 0.621 | 5.709 | 1 | 0.017 | 4.409 | 1.306 | 14.890 | |
| Place of residence | −0.123 | 0.338 | 0.132 | 1 | 0.717 | 0.885 | 0.456 | 1.717 | |
| [High stress level] | −0.909 | 0.775 | 1.376 | 1 | 0.241 | 0.403 | 0.088 | 1.841 | |
| [Moderate stress level] | −1.353 | 0.370 | 13.379 | 1 | 0.000 | 0.258 | 0.125 | 0.534 | |
| [Non-Smoker] | 0.660 | 0.332 | 3.960 | 1 | 0.047 | 1.935 | 1.010 | 3.706 | |
| Independent Variable | OR (95% CI) | p-Value |
|---|---|---|
| Smoking (smoker vs. non-smoker) | 1.935 (95% CI: 1.01–3.71) | 0.047 |
| Moderate stress (vs. low stress) | 0.258 (CI not specified) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Armencia, A.O.; Nicolau, A.; Bamboi, I.; Toader, B.; Rapis, A.; Panaite, T.; Argatu, D.; Balcos, C. Associations Between Smoking, Stress, Quality of Life, and Oral Health Among Dental Students in Romania: A Cross-Sectional Study. Medicina 2025, 61, 1394. https://doi.org/10.3390/medicina61081394
Armencia AO, Nicolau A, Bamboi I, Toader B, Rapis A, Panaite T, Argatu D, Balcos C. Associations Between Smoking, Stress, Quality of Life, and Oral Health Among Dental Students in Romania: A Cross-Sectional Study. Medicina. 2025; 61(8):1394. https://doi.org/10.3390/medicina61081394
Chicago/Turabian StyleArmencia, Adina Oana, Andrei Nicolau, Irina Bamboi, Bianca Toader, Anca Rapis, Tinela Panaite, Daniela Argatu, and Carina Balcos. 2025. "Associations Between Smoking, Stress, Quality of Life, and Oral Health Among Dental Students in Romania: A Cross-Sectional Study" Medicina 61, no. 8: 1394. https://doi.org/10.3390/medicina61081394
APA StyleArmencia, A. O., Nicolau, A., Bamboi, I., Toader, B., Rapis, A., Panaite, T., Argatu, D., & Balcos, C. (2025). Associations Between Smoking, Stress, Quality of Life, and Oral Health Among Dental Students in Romania: A Cross-Sectional Study. Medicina, 61(8), 1394. https://doi.org/10.3390/medicina61081394