
Prognostic Value of Metabolic Tumor Volume and Heterogeneity Index in Diffuse Large B-Cell Lymphoma

 , , , , , ,
, , , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. PET/CT Technique
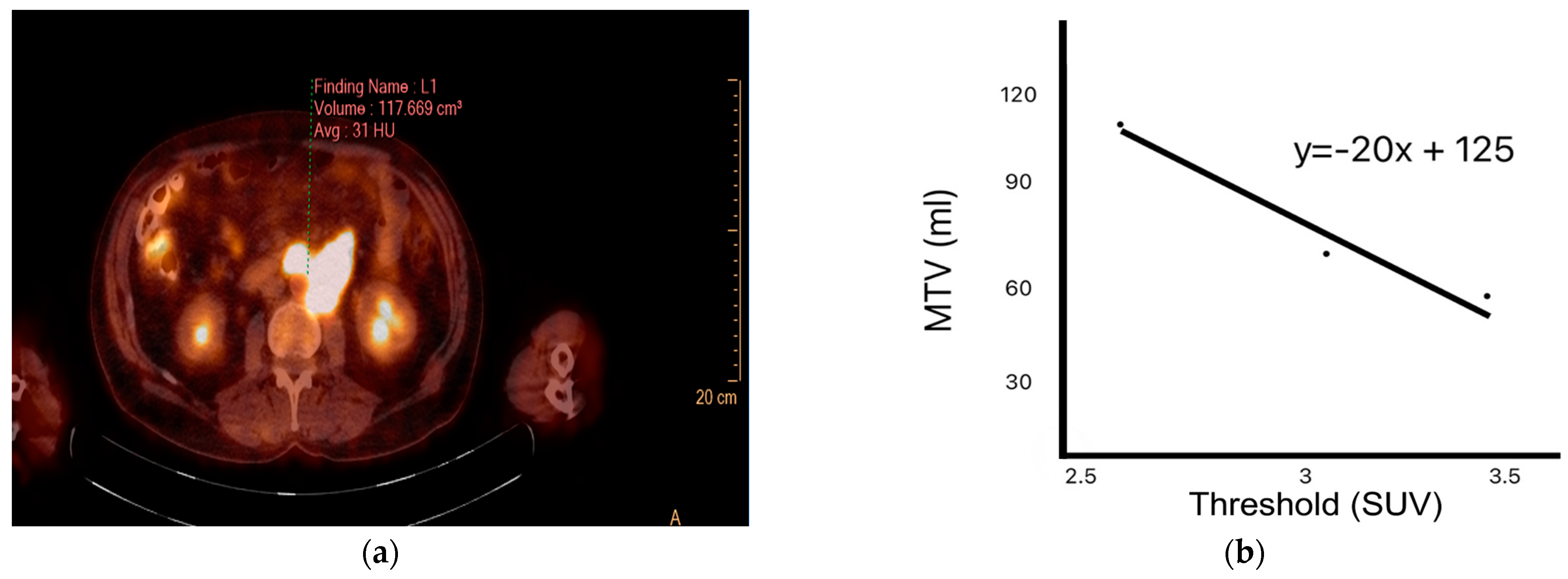
2.2. PET/CT Image Analysis
2.3. Statistical Analysis
3. Results
3.1. Baseline Patient Characteristics
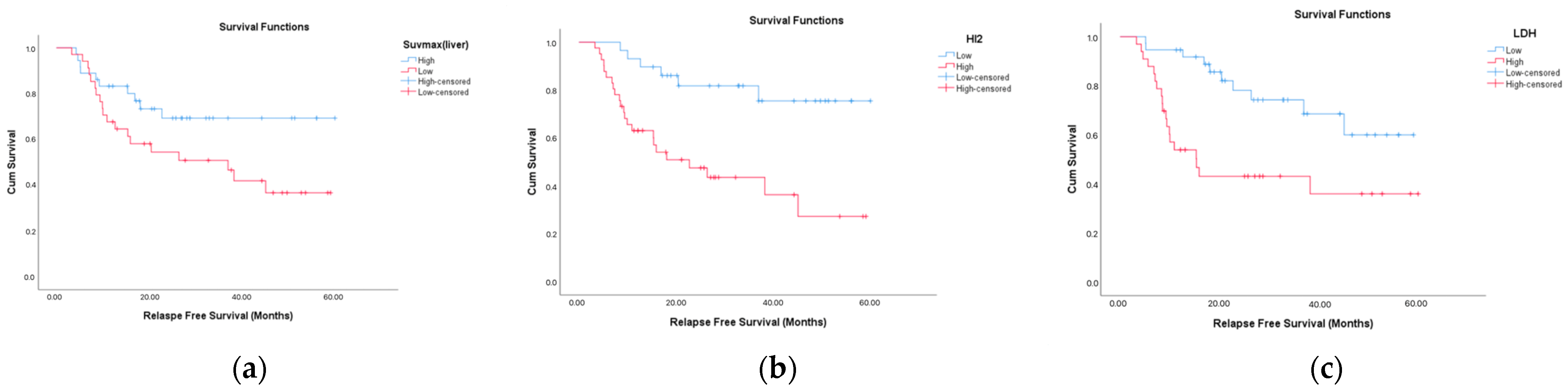
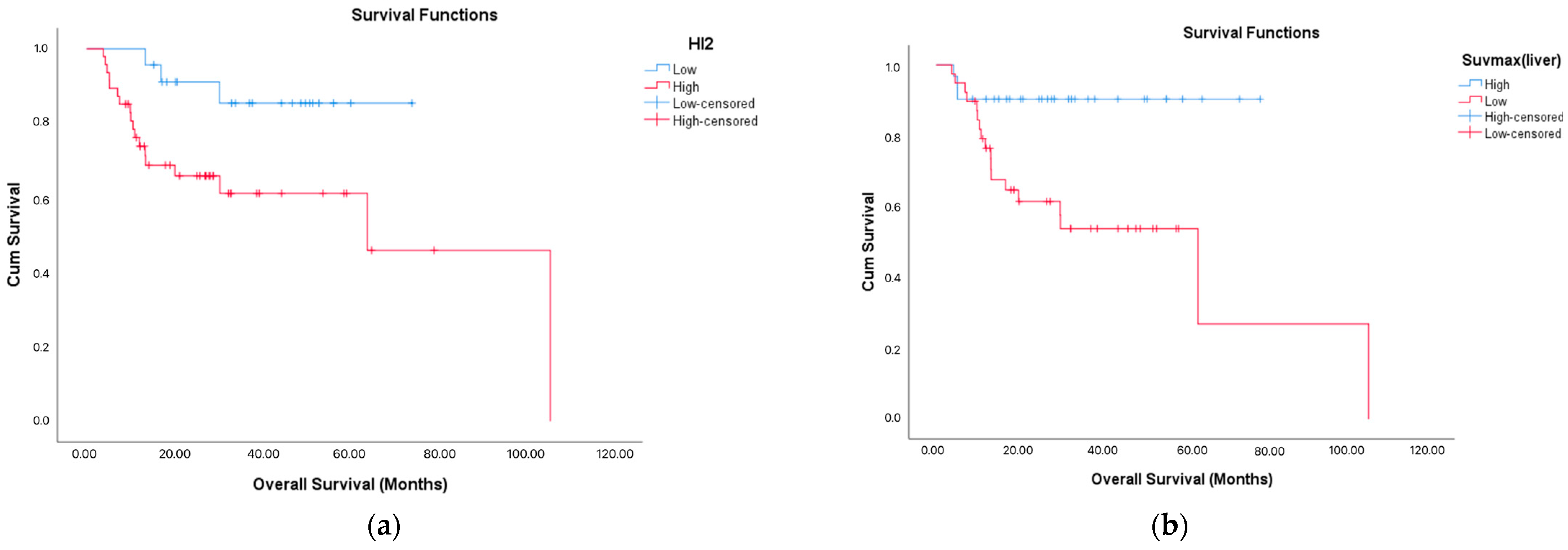
3.2. OS and RFS
3.3. Predictive Role of ROC-Based Biomarkers in Mortality
3.4. Associations with Treatment Response
3.5. Factors Associated with Relapse
3.6. Factors Associated with Mortality
3.7. Logistic Regression Analysis

{kind=link}
{kind=link}
{kind=link}
| Categorical Variables | |||
|---|---|---|---|
| Variable | Mortality (+) (n = 21) | Mortality (–) (n = 49) | p-Value |
| Age Group | |||
| >60 years | 13 (61.9%) | 25 (51.0%) | 0.402 |
| ≤60 years | 8 (38.1%) | 24 (49.0%) | |
| Gender | |||
| Male | 16 (76.2%) | 25 (51.0%) | 0.043 |
| Female | 5 (23.8%) | 24 (49.0%) | |
| Disease Stage | 0.971 | ||
| Stage 1 | 4 (19.0%) | 10 (20.4%) | |
| Stage 2 | 3 (14.3%) | 6 (12.2%) | |
| Stage 3 | 3 (14.3%) | 9 (18.4%) | |
| Stage 4 | 11 (52.4%) | 24 (49.0%) | |
| Stages 3–4 | 14 (66.7%) | 33 (67.3%) | 0.956 |
| ≥1 Comorbidity | 6 (28.6%) | 17 (34.7%) | 0.617 |
| Chemotherapy Regimen | 0.678 | ||
| R-EPOCH | 3 (14.3%) | 9 (18.4%) | |
| R-CHOP | 18 (85.7%) | 40 (81.6%) | |
| ECOG Performance Score (PS) | 0.842 | ||
| 1 | 9 (42.9%) | 24 (49.0%) | |
| 2 | 6 (28.6%) | 14 (28.6%) | |
| 3 | 6 (28.6%) | 11 (22.4%) | |
| ECOG ≥ 2 | 12 (57.1%) | 25 (51.0%) | 0.638 |
| Treatment Response | 19 (90.5%) | 49 (100.0%) | 0.028 |
| Complete/Near Complete Response | 10 (47.6%) | 24 (49.0%) | 0.917 |
| Relapse | 21 (100.0%) | 8 (16.3%) | <0.001 |
| Elevated LDH | 14 (66.7%) | 28 (57.1%) | 0.456 |
| IPI Score | 0.414 | ||
| Low–Low Intermediate | 15 (71.4%) | 30 (61.2%) | |
| High–High Intermediate | 6 (28.6%) | 19 (38.8%) | |
| Bone Marrow Involvement | 2 (11.8%) | 3 (8.6%) | 0.714 |
| Bulky Disease | 5 (23.8%) | 10 (20.4%) | 0.751 |
| Continuous Variables (Median [25th–75th Percentile]) | |||
| Variable | Mortality (+) | Mortality (–) | p-Value |
| Age (years) | 63 (58–67) | 60.5 (47–69) | 0.453 |
| LDH (U/L) | 372 (212–565) | 297 (206–432) | 0.112 |
| Albumin (g/dL) | 3.5 (3.2–3.8) | 3.7 (3.2–4.12) | 0.230 |
| WBC (/mm3) | 8800 (6700–9800) | 9500 (7775–12,350) | 0.290 |
| Neutrophils (/mm3) | 5800 (4300–7600) | 6650 (4775–8525) | 0.513 |
| Lymphocytes (/mm3) | 1300 (600–1700) | 1400 (975–2300) | 0.186 |
| Platelets (/mm3) | 276,000 (256 k–365 k) | 308,000 (259 k–415.75 k) | 0.465 |
| SUVmaxliver | 19 (13–22) | 24 (19–27.25) | 0.003 |
| SUVmax | 148 (21–256) | 132 (47.5–204) | 0.974 |
| SUVpeak | 138 (46–236) | 137.5 (70–235.25) | 0.853 |
| SUVmean | 9.6 (7.6–12.7) | 6.8 (5.07–10.4) | 0.088 |
| SUVmeanliver | 18 (15–19) | 21 (17–23.5) | 0.292 |
| MTV2.5 | 1089 (560–2028) | 1498.5 (413.75–4649.5) | 0.754 |
| MTV3 | 1378 (644–6633) | 1432.5 (242.25–4161.75) | 0.097 |
| MTV3.5 | 1194 (725–5358) | 636 (137.5–3628) | 0.121 |
| SUV SD | 3.4 (1.8–4.9) | 2.4 (1.5–4.0) | 0.407 |
| PNI | 4.8 (3.9–5.1) | 5.3 (4–6.43) | 0.144 |
| SII | 1319 (682–2650) | 1434.5 (566.25–2519.5) | 0.686 |
| NLR | 5.15 (2.63–8.63) | 4.38 (1.98–7.98) | 0.401 |
| HI1 | 0.3 (0.24–0.39) | 0.31 (0.25–0.38) | 0.744 |
| HI2 | 185.5 (27–476) | 93.5 (5–2044) | 0.016 |
| Ki-67 (%) | 75 (50–80) | 75 (65–80) | 0.475 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Odd Ratio | 95% CI | p | Odd Ratio | 95% CI | p | |
| SUVmaxliver (≤22) | ||||||
| Low | 8.000 | 2.080–30.763 | 0.002 ** | 7.116 | 1.750–28.932 | 0.006 ** |
| High | ||||||
| HI2 (≤62.3) | ||||||
| Low | 0.188 | 0.049–0.723 | 0.015 * | 0.225 | 0.053–0.955 | 0.043 * |
| High | ||||||
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Odd Ratio | 95% CI | p | Odd Ratio | 95% CI | p | |
| LDH (≤301) | ||||||
| Low | 0.273 | 0.100–0.743 | 0.001 ** | 0.462 | 0.145–1.467 | 0.190 |
| High | ||||||
| SUVmaxliver (≤21) | ||||||
| Low | 3.293 | 1.218–8.908 | 0.019 * | 2.577 | 0.841–7.899 | 0.098 |
| High | ||||||
| HI2 (≤87.9) | ||||||
| Low | 0.204 | 0.069–0.607 | 0.004 ** | 0.272 | 0.079–0.940 | 0.040 * |
| High | ||||||
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| TMV | Tumor Metabolic Volume |
| DLBCL | Diffuse Large B-Cell Lymphoma |
| SUV | Standardized Uptake Value |
| HI | Heterogenity Index |
| RFS | Relapse-Free Survival |
| OS | Overall Survival |
| IPI | International Prognostic Index |
| NLR | Neutrophil-to-Lymphocyte Ratio |
| ROI | Region of İnterest |
| ECOG | Eastern Cooperative Oncology Group |
| SPSS | Statistical Package for the Social Sciences |
| ROC | Receiver Operating Characteristic |
| AUC | Area Under the Curve |
| HR | Hazard Ratio |
References
- Berhan, A.; Almaw, A.; Damtie, S.; Solomon, Y. Diffuse Large B Cell Lymphoma (DLBCL): Epidemiology, Pathophysiology, Risk Stratification, Advancement in Diagnostic Approaches and Prospects: Narrative Review. Discov. Oncol. 2025, 16, 184. [Google Scholar] [CrossRef]
- Wang, Y.; Shi, Q.; Shi, Z.Y.; Tian, S.; Zhang, M.C.; Shen, R.; Fu, D.; Dong, L.; Yi, H.M.; Ouyang, B.S.; et al. Biological Signatures of the International Prognostic Index in Diffuse Large B-Cell Lymphoma. Blood Adv. 2024, 8, 1587–1599. [Google Scholar] [CrossRef]
- Zanoni, L.; Bezzi, D.; Nanni, C.; Paccagnella, A.; Farina, A.; Broccoli, A.; Casadei, B.; Zinzani, P.L.; Fanti, S. PET/CT in Non-Hodgkin Lymphoma: An Update. Semin. Nucl. Med. 2023, 53, 320–351. [Google Scholar] [CrossRef]
- Zeman, M.N.; Akin, E.A.; Merryman, R.W.; Jacene, H.A. Interim FDG-PET/CT for Response Assessment of Lymphoma. Semin. Nucl. Med. 2023, 53, 371–388. [Google Scholar] [CrossRef]
- Gallamini, A.; Zwarthoed, C.; Borra, A. Positron Emission Tomography (PET) in Oncology. Cancers 2014, 6, 1821–1889. [Google Scholar] [CrossRef]
- Husby, J.A.; Reitan, B.C.; Biermann, M.; Trovik, J.; Bjørge, L.; Magnussen, I.J.; Salvesen, O.O.; Salvesen, H.B.; Haldorsen, I.S. Metabolic Tumor Volume on 18F-FDG PET/CT Improves Preoperative Identification of High-Risk Endometrial Carcinoma Patients. J. Nucl. Med. 2015, 56, 1191–1198. [Google Scholar] [CrossRef]
- Zhao, W.; Wu, X.; Huang, S.; Wang, H.; Fu, H. Evaluation of Therapeutic Effect and Prognostic Value of 18F-FDG PET/CT in Different Treatment Nodes of DLBCL Patients. EJNMMI Res. 2024, 14, 20. [Google Scholar] [CrossRef]
- Brose, A.; Miederer, I.; König, J.; Gkika, E.; Sahlmann, J.; Schimek-Jasch, T.; Schreckenberger, M.; Nestle, U.; Kappes, J.; Miederer, M. Prognostic Value of Metabolic Tumor Volume on [18F]FDG PET/CT in Addition to the TNM Classification System of Locally Advanced Non-Small Cell Lung Cancer. Cancer Imaging 2024, 24, 171. [Google Scholar] [CrossRef]
- Kim, Y.I.; Paeng, J.C.; Cheon, G.J.; Suh, K.S.; Lee, D.S.; Chung, J.K.; Kang, K.W. Prediction of Posttransplantation Recurrence of Hepatocellular Carcinoma Using Metabolic and Volumetric Indices of 18F-FDG PET/CT. J. Nucl. Med. 2016, 57, 1045–1051. [Google Scholar] [CrossRef]
- Nakaya, A.; Fujita, S.; Satake, A.; Nakanishi, T.; Azuma, Y.; Tsubokura, Y.; Hotta, M.; Yoshimura, H.; Ishii, K.; Ito, T.; et al. Enhanced International Prognostic Index in Japanese Patients with Diffuse Large B-Cell Lymphoma. Leuk. Res. Rep. 2016, 6, 24–26. [Google Scholar] [CrossRef]
- Kim, T.H.; Yoon, J.K.; Kang, D.K.; Lee, S.J.; Jung, Y.S.; Yim, H.; An, Y.S. Correlation Between F-18 Fluorodeoxyglucose Positron Emission Tomography Metabolic Parameters and Dynamic Contrast-Enhanced MRI-Derived Perfusion Data in Patients with Invasive Ductal Breast Carcinoma. Ann. Surg. Oncol. 2015, 22, 3866–3872. [Google Scholar] [CrossRef]
- Hughes, N.M.; Mou, T.; O’Regan, K.N.; Murphy, P.; O’Sullivan, J.N.; Wolsztynski, E.; Huang, J.; Kennedy, M.P.; Eary, J.F.; O’Sullivan, F. Tumor Heterogeneity Measurement Using [18F] FDG PET/CT Shows Prognostic Value in Patients with Non-Small Cell Lung Cancer. Eur. J. Hybrid Imaging 2018, 2, 25. [Google Scholar] [CrossRef]
- Liu, G.; Yin, H.; Cheng, X.; Wang, Y.; Hu, Y.; Liu, T.; Shi, H. Intra-Tumor Metabolic Heterogeneity of Gastric Cancer on 18F-FDG PETCT Indicates Patient Survival Outcomes. Clin. Exp. Med. 2021, 21, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.H.; Yoon, J.K.; An, Y.S.; Shin, Y.S.; Kim, C.H.; Lee, D.H.; Jo, K.S.; Lee, S.J. Prognostic Significance of the Intratumoral Heterogeneity of 18F-FDG Uptake in Oral Cavity Cancer. J. Surg. Oncol. 2014, 110, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Kimura, M.; Kato, I.; Ishibashi, K.; Shibata, A.; Nishiwaki, S.; Fukumura, M.; Sone, Y.; Nagao, T.; Umemura, M. The Prognostic Significance of Intratumoral Heterogeneity of 18F-FDG Uptake in Patients with Oral Cavity Squamous Cell Carcinoma. Eur. J. Radiol. 2019, 114, 99–104. [Google Scholar] [CrossRef]
- Zwezerijnen, G.J.C.; Eertink, J.J.; Ferrández, M.C.; Wiegers, S.E.; Burggraaff, C.N.; Lugtenburg, P.J.; Heymans, M.W.; de Vet, H.C.W.; Zijlstra, J.M.; Boellaard, R. Reproducibility of [18F]FDG PET/CT Liver SUV as Reference or Normalisation Factor. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 486–493. [Google Scholar] [CrossRef]
- Kido, H.; Kato, S.; Funahashi, K.; Shibuya, K.; Sasaki, Y.; Urita, Y.; Hori, M.; Mizumura, S. The Metabolic Parameters Based on Volume in PET/CT Are Associated with Clinicopathological N Stage of Colorectal Cancer and Can Predict Prognosis. EJNMMI Res. 2021, 11, 87. [Google Scholar] [CrossRef]
- Gopal, A.; Xi, Y.; Subramaniam, R.M.; Pinho, D.F. Intratumoral Metabolic Heterogeneity and Other Quantitative 18F-FDG PET/CT Parameters for Prognosis Prediction in Esophageal Cancer. Radiol. Imaging Cancer 2021, 3, e200022. [Google Scholar] [CrossRef] [PubMed]
- Gu, F.; Wu, Q. Quantitation of Dynamic Total-Body PET Imaging: Recent Developments and Future Perspectives. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 3538–3557. [Google Scholar] [CrossRef]
- Demicco, M.; Liu, X.Z.; Leithner, K.; Fendt, S.M. Metabolic Heterogeneity in Cancer. Nat. Metab. 2024, 6, 18–38. [Google Scholar] [CrossRef]
- Sehn, L.H.; Berry, B.; Chhanabhai, M.; Fitzgerald, C.; Gill, K.; Hoskins, P.; Klasa, R.; Savage, K.J.; Shenkier, T.; Sutherland, J.; et al. The Revised International Prognostic Index (R-IPI) Is a Better Predictor of Outcome than the Standard IPI for Patients with Diffuse Large B-Cell Lymphoma Treated with R-CHOP. Blood 2007, 109, 1857–1861. [Google Scholar] [CrossRef] [PubMed]
- International Non-Hodgkin’s Lymphoma Prognostic Factors Project. A Predictive Model for Aggressive Non-Hodgkin’s Lymphoma. N. Engl. J. Med. 1993, 329, 987–994. [Google Scholar] [CrossRef]
- Zhou, Z.; Sehn, L.H.; Rademaker, A.W.; Gordon, L.I.; LaCasce, A.S.; Crosby-Thompson, A.; Vanderplas, A.; Zelenetz, A.D.; Abel, G.A.; Rodriguez, M.A.; et al. An Enhanced International Prognostic Index (NCCN-IPI) for Patients with Diffuse Large B-Cell Lymphoma Treated in the Rituximab Era. Blood 2014, 123, 837–842. [Google Scholar] [CrossRef]
- Adams, H.J.A.; Kwee, T.C. Prognostic Value of Interim FDG-PET in R-CHOP-Treated Diffuse Large B-Cell Lymphoma: Systematic Review and Meta-Analysis. Crit. Rev. Oncol. Hematol. 2016, 106, 55–63. [Google Scholar] [CrossRef]
- Zhou, M.; Chen, Y.; Huang, H.; Zhou, X.; Liu, J.; Huang, G. Prognostic Value of Total Lesion Glycolysis of Baseline 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography in Diffuse Large B-Cell Lymphoma. Oncotarget 2016, 7, 83544. [Google Scholar] [CrossRef]
- Esfahani, S.A.; Heidari, P.; Halpern, E.F.; Hochberg, E.P.; Palmer, E.L.; Mahmood, U. Baseline Total Lesion Glycolysis Measured with 18F-FDG PET/CT as a Predictor of Progression-Free Survival in Diffuse Large B-Cell Lymphoma: A Pilot Study. Am. J. Nucl. Med. Mol. Imaging 2013, 3, 272. [Google Scholar] [PubMed]
- Ceriani, L.; Martelli, M.; Zinzani, P.L.; Ferreri, A.J.M.; Botto, B.; Stelitano, C.; Gotti, M.; Cabras, M.G.; Rigacci, L.; Gargantini, L.; et al. Utility of Baseline 18FDG-PET/CT Functional Parameters in Defining Prognosis of Primary Mediastinal (Thymic) Large B-Cell Lymphoma. Blood 2015, 126, 950–956. [Google Scholar] [CrossRef] [PubMed]
- Mikhaeel, N.G.; Smith, D.; Dunn, J.T.; Phillips, M.; Møller, H.; Fields, P.A.; Wrench, D.; Barrington, S.F. Combination of Baseline Metabolic Tumour Volume and Early Response on PET/CT Improves Progression-Free Survival Prediction in DLBCL. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1209–1219. [Google Scholar] [CrossRef]
- Sasanelli, M.; Meignan, M.; Haioun, C.; Berriolo-Riedinger, A.; Casasnovas, R.O.; Biggi, A.; Gallamini, A.; Siegel, B.A.; Cashen, A.F.; Véra, P.; et al. Pretherapy Metabolic Tumour Volume Is an Independent Predictor of Outcome in Patients with Diffuse Large B-Cell Lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 2017–2022. [Google Scholar] [CrossRef]
- Casasnovas, R.-O.; Sasanelli, M.; Berriolo-Riedinger, A.; Morschhauser, F.; Itti, E.; Huglo, D.; Versari, A.; Coiffier, B.; Meignan, M. Baseline Metabolic Tumor Volume Is Predictive of Patient Outcome in Diffuse Large B Cell Lymphoma. Blood 2012, 120, 1598. [Google Scholar] [CrossRef]
- Xie, M.; Zhai, W.; Cheng, S.; Zhang, H.; Xie, Y.; He, W. Predictive Value of F-18 FDG PET/CT Quantization Parameters for Progression-Free Survival in Patients with Diffuse Large B-Cell Lymphoma. Hematology 2016, 21, 99–105. [Google Scholar] [CrossRef]
- Chihara, D.; Oki, Y.; Onoda, H.; Taji, H.; Yamamoto, K.; Tamaki, T.; Morishima, Y. High Maximum Standard Uptake Value (SUVmax) on PET Scan Is Associated with Shorter Survival in Patients with Diffuse Large B Cell Lymphoma. Int. J. Hematol. 2011, 93, 502–508. [Google Scholar] [CrossRef]
- Liu, X.; Xiang, K.; Geng, G.Y.; Wang, S.C.; Ni, M.; Zhang, Y.F.; Pan, H.F.; Lv, W.F. Prognostic Value of Intratumor Metabolic Heterogeneity Parameters on 18F-FDG PET/CT for Patients with Colorectal Cancer. Contrast Media Mol. Imaging 2022, 2022, 2586245. [Google Scholar] [CrossRef]
- Chung, H.H.; Kang, S.Y.; Ha, S.; Kim, J.W.; Park, N.H.; Song, Y.S.; Cheon, G.J. Prognostic Value of Preoperative Intratumoral FDG Uptake Heterogeneity in Early Stage Uterine Cervical Cancer. J. Gynecol. Oncol. 2016, 27, e15. [Google Scholar] [CrossRef]
- Lee, M.; Lee, H.; Cheon, G.J.; Kim, H.S.; Chung, H.H.; Kim, J.W.; Park, N.H.; Song, Y.S. Prognostic Value of Preoperative Intratumoral FDG Uptake Heterogeneity in Patients with Epithelial Ovarian Cancer. Eur. Radiol. 2017, 27, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Geng, H.; Lian, K.; Zhang, W. Prognostic Value of 18F-FDG PET/CT Tumor Metabolic Parameters and Ki-67 in Pre-Treatment Diffuse Large B-Cell Lymphoma. Quant. Imaging Med. Surg. 2024, 14, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Xie, P.; Li, M.; Zhao, H.; Sun, X.; Fu, Z.; Yu, J. 18F-FDG PET or PET-CT to Evaluate Prognosis for Head and Neck Cancer: A Meta-Analysis. J. Cancer Res. Clin. Oncol. 2011, 137, 1085–1093. [Google Scholar] [CrossRef]
- Liu, J.; Ren, Q.; Xiao, H.; Li, S.; Zheng, L.; Yang, X.; Feng, L.; Zhou, Z.; Wang, H.; Yang, J.; et al. Whole-Tumoral Metabolic Heterogeneity in 18F-FDG PET/CT Is a Novel Prognostic Marker for Neuroblastoma. Cancer Imaging 2024, 24, 72. [Google Scholar] [CrossRef]
- Park, S.; Moon, S.H.; Park, L.C.; Hwang, D.W.; Ji, J.H.; Maeng, C.H.; Cho, S.H.; Ahn, H.K.; Lee, J.Y.; Kim, S.J.; et al. The Impact of Baseline and Interim PET/CT Parameters on Clinical Outcome in Patients with Diffuse Large B Cell Lymphoma. Am. J. Hematol. 2012, 87, 937–940. [Google Scholar] [CrossRef] [PubMed]
- Gallicchio, R.; Mansueto, G.; Simeon, V.; Nardelli, A.; Guariglia, R.; Capacchione, D.; Soscia, E.; Pedicini, P.; Gattozzi, D.; Musto, P.; et al. F-18 FDG PET/CT Quantization Parameters as Predictors of Outcome in Patients with Diffuse Large B-Cell Lymphoma. Eur. J. Haematol. 2014, 92, 382–389. [Google Scholar] [CrossRef]
- Adams, H.J.A.; de Klerk, J.M.H.; Fijnheer, R.; Heggelman, B.G.F.; Dubois, S.V.; Nievelstein, R.A.J.; Kwee, T.C. Prognostic Superiority of the National Comprehensive Cancer Network International Prognostic Index over Pretreatment Whole-Body Volumetric-Metabolic FDG-PET/CT Metrics in Diffuse Large B-Cell Lymphoma. Eur. J. Haematol. 2015, 94, 532–539. [Google Scholar] [CrossRef] [PubMed]
| Characteristic | N | % |
|---|---|---|
| Age > 60 | 38 | 54.3 |
| Age ≤ 60 | 32 | 45.7 |
| Male | 41 | 58.6 |
| Female | 29 | 41.4 |
| Stage | N | % |
| Stage 1 | 14 | 20.0 |
| Stage 2 | 9 | 12.9 |
| Stage 3 | 12 | 17.1 |
| Stage 4 | 35 | 50.0 |
| Advanced Stage (3 and 4) | N | % |
| Yes | 47 | 67.1 |
| No | 23 | 32.9 |
| >1 Extranodal Site | N | % |
| Yes | 23 | 32.9 |
| No | 47 | 67.1 |
| Regimen | N | % |
| R-EPOCH | 12 | 17.1 |
| R-CHOP | 58 | 82.9 |
| ECOG PS | N | % |
| Score 1 | 33 | 47.1 |
| Score 2 | 20 | 28.6 |
| Score 3 | 17 | 24.3 |
| ECOG ≥2 | N | % |
| Yes | 37 | 52.9 |
| No | 33 | 47.1 |
| Treatment Response | N | % |
| Response Present | 68 | 97.1 |
| No Response | 2 | 2.9 |
| Response Type | N | % |
| Complete or Near Complete | 34 | 48.6 |
| Others | 36 | 51.4 |
| Mortality | N | % |
| Yes | 21 | 30.0 |
| No | 49 | 70.0 |
| Relapse | N | % |
| Yes | 29 | 41.4 |
| No | 41 | 58.6 |
| Elevated LDH | N | % |
| Yes | 42 | 60.0 |
| No | 28 | 40.0 |
| IPI Group | N | % |
| Low/Low-Intermediate | 45 | 64.3 |
| High-Intermediate/High | 25 | 35.7 |
| Bone Marrow Infiltration | N | % |
| Yes | 5 | 7.1 |
| No | 65 | 92.9 |
| Ki67 | N | % |
| ≥70% | 37 | 63.8 |
| <70% | 21 | 36.2 |
| Bulky Disease | N | % |
| Yes | 15 | 21.4 |
| No | 55 | 78.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solmaz, A.A.; Birsenogul, I.; Kelle, A.P.; Peker, P.; Arslan Benli, B.; Ata, S.; Koyuncu, M.B.; Gurbuz, M.; Ogul, A.; Duman, B.B.; et al. Prognostic Value of Metabolic Tumor Volume and Heterogeneity Index in Diffuse Large B-Cell Lymphoma. Medicina 2025, 61, 1370. https://doi.org/10.3390/medicina61081370
Solmaz AA, Birsenogul I, Kelle AP, Peker P, Arslan Benli B, Ata S, Koyuncu MB, Gurbuz M, Ogul A, Duman BB, et al. Prognostic Value of Metabolic Tumor Volume and Heterogeneity Index in Diffuse Large B-Cell Lymphoma. Medicina. 2025; 61(8):1370. https://doi.org/10.3390/medicina61081370
Chicago/Turabian StyleSolmaz, Ali Alper, Ilhan Birsenogul, Aygul Polat Kelle, Pinar Peker, Burcu Arslan Benli, Serdar Ata, Mahmut Bakir Koyuncu, Mustafa Gurbuz, Ali Ogul, Berna Bozkurt Duman, and et al. 2025. "Prognostic Value of Metabolic Tumor Volume and Heterogeneity Index in Diffuse Large B-Cell Lymphoma" Medicina 61, no. 8: 1370. https://doi.org/10.3390/medicina61081370
APA StyleSolmaz, A. A., Birsenogul, I., Kelle, A. P., Peker, P., Arslan Benli, B., Ata, S., Koyuncu, M. B., Gurbuz, M., Ogul, A., Duman, B. B., & Cil, T. (2025). Prognostic Value of Metabolic Tumor Volume and Heterogeneity Index in Diffuse Large B-Cell Lymphoma. Medicina, 61(8), 1370. https://doi.org/10.3390/medicina61081370