
Risk of Osteonecrosis of the Jaw in Patients Treated with Zoledronic or Alendronic Acid: A Systematic Review

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Focus Question
2.3. Information Sources
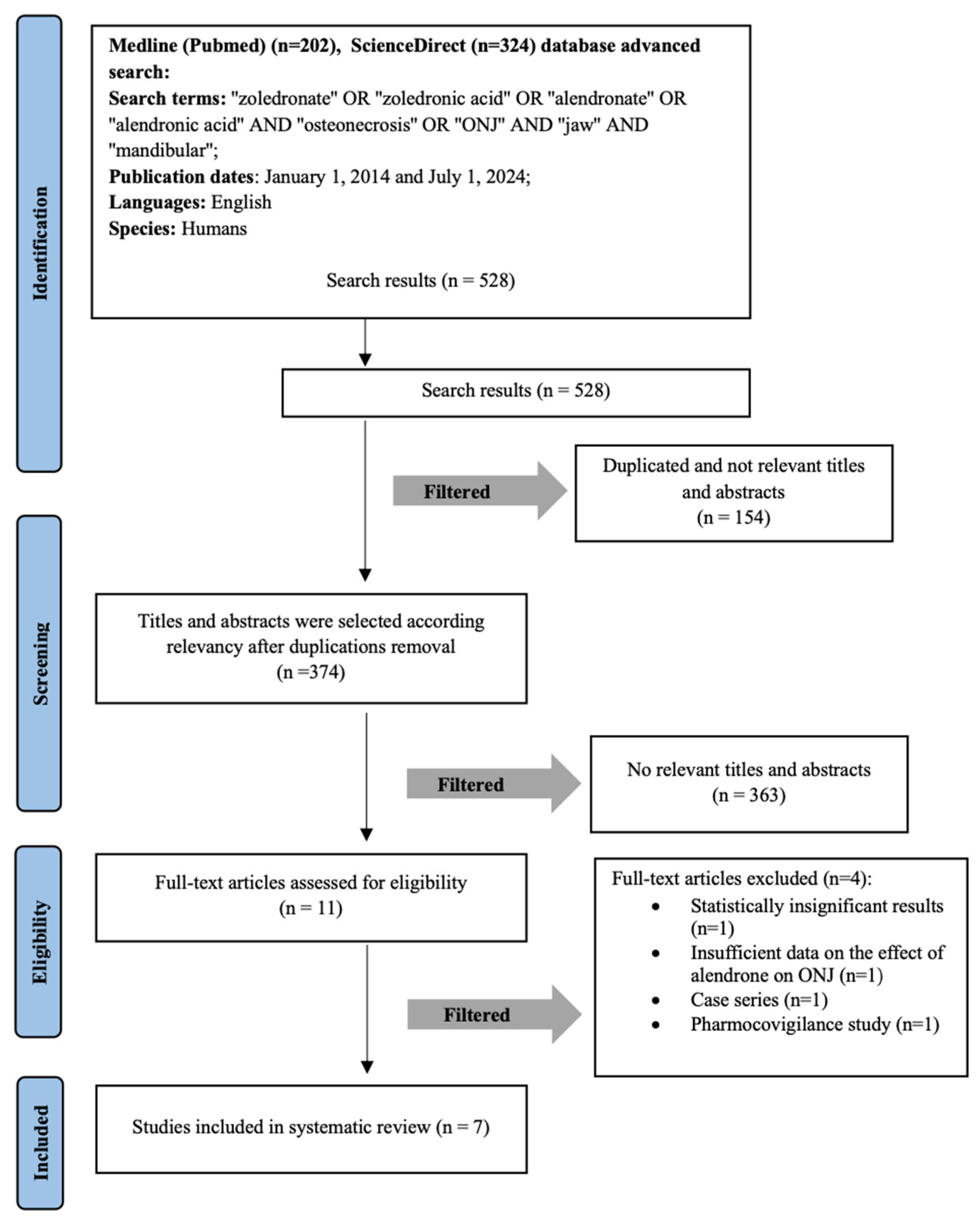
2.4. Search
2.5. Selection of Studies
2.6. Types of Publications
2.7. Inclusion and Exclusion Criteria
- Type of publication: retrospective cohort studies, prospective studies. and observational studies
- Studies examining the incidence, risk and the impact of treatment duration of ZA or AA on the development of ONJ.
- Studies were required to confirm both OP diagnosis and ONJ occurrence, ensuring that the findings were relevant to the target patient population.
- Patients diagnosed with a rheumatologic condition or cancer who are prescribed ZA.
- Research conducted with human subjects.
- Studies published in English within the last 10 years.
- Access to the full text of the article.
- Type of publications: meta-analyses, systematic reviews, conference abstracts, case reports, or case series, as these do not provide original patient data.
- Research conducted on animals or in vitro/ex vivo models.
- Studies involving patients diagnosed with Paget’s disease or malignant neoplasm.
- Studies involving patients receiving denosumab or other bisphosphonates (except ZA or AA).
- Studies involving minors.
- Studies that lacked sufficient data or whose authors could not be contacted for clarification.
2.8. Sequential Search Strategy
2.9. Data Extraction and Items
- Author;
- Type of publication;
- Sample size;
- Type of BP;
- Number of subjects;
- Method of assessment;
- Results;
- Conclusions;
- Follow-up.
2.10. Risk of Bias Within Studies
2.11. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Quality Assessment of the Included Studies
3.3. Study Characteristics
3.4. Zoledronic Acid
3.4.1. The Incidence of ONJ Development
3.4.2. Risk and Impact of Treatment Duration on ONJ Development
3.5. Alendronic Acid
3.5.1. The Incidence of ONJ Development
3.5.2. Risk and Impact of Treatment Duration on ONJ Development
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| OP | Osteoporosis |
| ONJ | Osteonecrosis of the jaw |
| BP | Bisphosphonate |
| ZA | Zoledronic Acid |
| AA | Alendronic Acid |
| MRONJ | Medication-related osteonecrosis of the jaw |
| PRISMA | Preferred Reporting Item for Systematic Review and Meta-Analyses |
| JBI | The Joanna Briggs Institute |
| TTO | Median time to ONJ onset |
| TE | Tooth extraction |
References
- Sharma, N.; Reche, A. Unraveling the Relationship Between Osteoporosis, Treatment Modalities, and Oral Health: A Comprehensive Review. Cureus 2023, 15, e49399. [Google Scholar] [CrossRef] [PubMed]
- Sozen, T.; Ozisik, L.; Calik Basaran, N. An overview and management of osteoporosis. Eur. J. Rheumatol. 2017, 4, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Riggs, B.L.; Wahner, H.W.; Seeman, E.; Offord, K.P.; Dunn, W.L.; Mazess, R.B.; Johnson, K.A.; Melton, L.J. Changes in Bone Mineral Density of the Proximal Femur and Spine with Aging. J. Clin. Investig. 1982, 70, 716–723. [Google Scholar] [CrossRef]
- Siris, E.S.; Adler, R.; Bilezikian, J.; Bolognese, M.; Dawson-Hughes, B.; Favus, M.J.; Harris, S.T.; Jan de Beur, S.M.; Khosla, S.; Lane, N.E.; et al. The clinical diagnosis of osteoporosis: A position statement from the National Bone Health Alliance Working Group. Osteoporos. Int. 2014, 25, 1439–1443. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Wang, X.; He, Y.; Han, R.; Wang, T.; Guo, Y. Jaw osteoporosis: Challenges to oral health and emerging perspectives of treatment. Biomed. Pharmacother. 2024, 177, 116995. [Google Scholar] [CrossRef]
- Lesclous, P.; Cloitre, A.; Catros, S.; Devoize, L.; Louvet, B.; Châtel, C.; Foissac, F.; Roux, C. Alendronate or Zoledronic acid do not impair wound healing after tooth extraction in postmenopausal women with osteoporosis. Bone 2020, 137, 115412. [Google Scholar] [CrossRef]
- Russell, R.G.G. Bisphosphonates: The first 40 years. Bone 2011, 49, 2–19. [Google Scholar] [CrossRef]
- Sereikaite, G.; Guzeviciene, V.; Peceliunaite, G.; Daugela, P.; Juodzbalys, G. Assessment Results of Dental Students’ Knowledge about Bisphosphonates and Bisphosphonate-Related Osteonecrosis of the Jaw. J. Oral Maxillofac. Res. 2023, 14, e3. [Google Scholar] [CrossRef]
- Lockwood, M.; Banderudrappagari, R.; Suva, L.J.; Makhoul, I. Atypical femoral fractures from bisphosphonate in cancer patients—Review. J. Bone Oncol. 2019, 18, 100259. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Prisma-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Ma, L.-L.; Wang, Y.-Y.; Yang, Z.-H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Tian, Y.; Yang, J.; Huser, V.; Jin, P.; Lambert, C.G.; Park, H.; You, S.C.; Park, R.W.; Rijnbeek, P.R.; et al. Comparative safety and effectiveness of alendronate versus raloxifene in women with osteoporosis. Sci. Rep. 2020, 10, 11115. Available online: https://www.nature.com/articles/s41598-020-68037-8 (accessed on 29 November 2023). [CrossRef]
- Sammut, S.; Malden, N.; Lopes, V.; Ralston, S. Epidemiological study of alendronate-related osteonecrosis of the jaw in the southeast of Scotland. Br. J. Oral Maxillofac. Surg. 2016, 54, 501–505. Available online: https://pubmed.ncbi.nlm.nih.gov/26975575/ (accessed on 29 November 2023). [CrossRef]
- Martins, L.H.I.; Ferreira, D.C.; Silva, M.T.; Motta, R.H.L.; Franquez, R.T.; Bergamaschi, C.d.C. Frequency of osteonecrosis in bisphosphonate users submitted to dental procedures: A systematic review. Oral Dis. 2023, 29, 75–99. [Google Scholar] [CrossRef]
- Manzano-Moreno, F.J.; Ramos-Torrecillas, J.; de Luna-Bertos, E.; Illescas-Montes, R.; Arnett, T.R.; Ruiz, C.; García-Martínez, O. Influence of pH on osteoclasts treated with zoledronate and alendronate. Clin. Oral Investig. 2019, 23, 813–820. [Google Scholar] [CrossRef]
- Eiken, P.A.; Prieto-Alhambra, D.; Eastell, R.; Abrahamsen, B. Surgically treated osteonecrosis and osteomyelitis of the jaw and oral cavity in patients highly adherent to alendronate treatment: A nationwide user-only cohort study including over 60,000 alendronate users. Osteoporos. Int. 2017, 28, 2921–2928. [Google Scholar] [CrossRef]
- Chen, S.; Ren, H.; He, Y.; An, J.; Zhang, Y. Recurrence-Related Factors of Medication-Related Osteonecrosis of the Jaw: A Five-Year Experience. J. Oral Maxillofac. Surg. 2021, 79, 2472–2481. [Google Scholar] [CrossRef]
- Fung, P.P.L.; Bedogni, G.; Bedogni, A.; Petrie, A.; Porter, S.; Campisi, G.; Bagan, J.; Fusco, V.; Saia, G.; Acham, S.; et al. Time to onset of bisphosphonate-related osteonecrosis of the jaws: A multicentre retrospective cohort study. Oral Dis. 2017, 23, 477–483. [Google Scholar] [CrossRef]
- Chiu, W.-Y.; Yang, W.-S.; Chien, J.-Y.; Lee, J.-J.; Tsai, K.-S. The influence of alendronate and tooth extraction on the incidence of osteonecrosis of the jaw among osteoporotic subjects. PLoS ONE 2018, 13, e0196419. [Google Scholar] [CrossRef]
- Chiu, W.-Y.; Chien, J.-Y.; Yang, W.-S.; Juang, J.-M.J.; Lee, J.-J.; Tsai, K.-S. The Risk of Osteonecrosis of the Jaws in Taiwanese Osteoporotic Patients Treated With Oral Alendronate or Raloxifene. J. Clin. Endocrinol. Metab. 2014, 99, 2729–2735. [Google Scholar] [CrossRef]
- Amigues, C.; Fresse, A.; Roux, C.H.; Gauthier, S.; Vieillard, M.H.; Drici, M.D.; Breuil, V. Zoledronate and osteonecrosis of the jaw in osteoporosis: Incidence and risk factors. Analysis of the French Pharmacovigilance Database. Jt. Bone Spine 2023, 90, 105599. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.-C.; Yang, C.-Y.; Kao Yang, Y.-H.; Lin, S.-J. Incidence and risk of osteonecrosis of the jaw among the Taiwan osteoporosis population. Osteoporos. Int. 2014, 25, 1503–1511. [Google Scholar] [CrossRef] [PubMed]
- Saag, K.G.; Petersen, J.; Brandi, M.L.; Karaplis, A.C.; Lorentzon, M.; Thomas, T.; Maddox, J.; Fan, M.; Meisner, P.D.; Grauer, A. Romosozumab or Alendronate for Fracture Prevention in Women with Osteoporosis. N. Engl. J. Med. 2017, 377, 1417–1427. [Google Scholar] [CrossRef] [PubMed]
- Pelaz, A.; Junquera, L.; Gallego, L.; García-Consuegra, L.; García-Martínez, L.; Cutilli, T.; Olay, S. Epidemiología, farmacología y caracterización clínica de la osteonecrosis de los maxilares. Un estudio retrospectivo de 70 casos. Acta Otorrinolaringol. Española 2015, 66, 139–147. [Google Scholar] [CrossRef]

{kind=link}
| Component | Description |
|---|---|
| Population (P) | Patients with OP taking BPs medications such as ZA or AA. |
| Intervention/ Exposure to a risk factor (I) | The effect of ZA or AA on the occurrence of ONJ. |
| Control (C) | Patients without OP and patients who do not use BPs. |
| Outcome (O) | The occurrence of ONJ in patients receiving BP therapy. |
| Question Number | Defined Question |
|---|---|
| Q1 | Were the two groups similar and recruited from the same population? |
| Q2 | Were the exposures measured similarly to assign people to both exposed and unexposed groups? |
| Q3 | Was the exposure measured in a valid and reliable way? |
| Q4 | Were confounding factors stated? |
| Q5 | Were strategies to deal with confounding factors stated? |
| Q6 | Were the groups/participants free of the outcome at the start of the study (or at the moment of exposure)? |
| Q7 | Were the outcomes measured in a valid and reliable way? |
| Q8 | Was the follow-up time reported and sufficient to be long enough for outcomes to occur? |
| Q9 | Was follow-up complete, and if not, were the reasons to lose to follow-up described and explored? |
| Q10 | Were strategies to address incomplete follow-up utilized? |
| Q11 | Was appropriate statistical analysis used? |
| Study | Study Design | Checklist | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | ||
| Eiken et al., 2017 [16] | Cohort study | + | + | + | + | + | + | + | + | ? | ? | + |
| Chen et al., 2021 [17] | Cohort study | ? | + | + | + | + | + | + | + | + | - | + |
| Fung et al., 2016 [18] | Cohort study | + | + | ? | NA | + | + | + | ? | + | + | + |
| Chiu et al., 2014 [20] | Cohort study | + | + | ? | + | + | + | ? | + | + | + | + |
| Chiu et al., 2018 [19] | Cohort study | + | + | ? | + | + | + | + | + | + | ? | + |
| Lin et al., 2014 [22] | Cohort study | + | + | ? | + | - | + | ? | + | + | + | + |
| Amigues et al., 2023 [21] | Cohort study | + | + | + | + | + | + | + | + | ? | + | + |
| Type of BP | Author (Year) | Follow-Up (Years) | Number of Patients | Number of Females | Mean Age | Number of ONJ Cases | Females with ONJ |
|---|---|---|---|---|---|---|---|
| AA | Eiken et al., 2017 [16] | 6.8 | 61.990 | 51.558 | 74.9 | 107 | 85 |
| Fung et al., 2016 [18] | 8 | 349 | 247 | ≥60 | 88 | - | |
| Chiu et al., 2014 [20] | 12 | 7.332 | 6.485 | 74.9 | 40 | 39 | |
| Chiu et al., 2018 [19] | 12 | 7.625 | 6.356 | 73.7 | 26 | - | |
| Lin et al., 2014 [22] | 6 | 18.030 | 14.213 | 78.1 | 25 | - | |
| Amigues et al., 2023 [21] | 10 | 1.039 | - | 70 | 188 | - | |
| ZA | Chen et al., 2021 [17] | 5 | 58 | 39 | 63.2 | 58 | - |
| Fung et al., 2016 [18] | 8 | 349 | 247 | ≥60 | 218 | - | |
| ZA1 | Amigues et al., 2023 [21] | 10 | 2.294 | - | 68 | 70 | - |
| ZA2 | Amigues et al., 2023 [21] | 10 | 1.103 | - | 66 | 568 | - |
| Type of BP | Author (Year) | Risk Increase with BP Duration | ONJ Dependence on BP Timing |
|---|---|---|---|
| AA | Eiken et al. [16] | >5 years | Positive |
| Fung et al. [18] | 6 years | Positive | |
| Chiu et al. [20] | >3 years | Positive | |
| Chiu et al. [19] | >1 year | Positive | |
| Lin et al. [22] | - | Negative | |
| Amigues et al. [21] | 69 ± 54 months | - | |
| ZA | Chen et al. [17] | >18 months | Positive |
| Fung et al. [18] | 2.2 years | Positive | |
| ZA1 | Amigues et al. [21] | 49 ± 22 months | Positive |
| ZA2 | Amigues et al. [21] | 27 ± 22 months | Positive |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jakonyte, A.; Gustainyte, E.; Petronis, Z.; Hafizov, A.; Janovskiene, A.; Razukevicius, D. Risk of Osteonecrosis of the Jaw in Patients Treated with Zoledronic or Alendronic Acid: A Systematic Review. Medicina 2025, 61, 1159. https://doi.org/10.3390/medicina61071159
Jakonyte A, Gustainyte E, Petronis Z, Hafizov A, Janovskiene A, Razukevicius D. Risk of Osteonecrosis of the Jaw in Patients Treated with Zoledronic or Alendronic Acid: A Systematic Review. Medicina. 2025; 61(7):1159. https://doi.org/10.3390/medicina61071159
Chicago/Turabian StyleJakonyte, Aine, Egle Gustainyte, Zygimantas Petronis, Aviad Hafizov, Audra Janovskiene, and Dainius Razukevicius. 2025. "Risk of Osteonecrosis of the Jaw in Patients Treated with Zoledronic or Alendronic Acid: A Systematic Review" Medicina 61, no. 7: 1159. https://doi.org/10.3390/medicina61071159
APA StyleJakonyte, A., Gustainyte, E., Petronis, Z., Hafizov, A., Janovskiene, A., & Razukevicius, D. (2025). Risk of Osteonecrosis of the Jaw in Patients Treated with Zoledronic or Alendronic Acid: A Systematic Review. Medicina, 61(7), 1159. https://doi.org/10.3390/medicina61071159