
Effect of High-Flow Nasal Cannula vs. Facemask on Arterial Oxygenation During Liver Radiofrequency Ablation: Randomized Controlled Trial


Abstract
1. Introduction
2. Materials and Methods
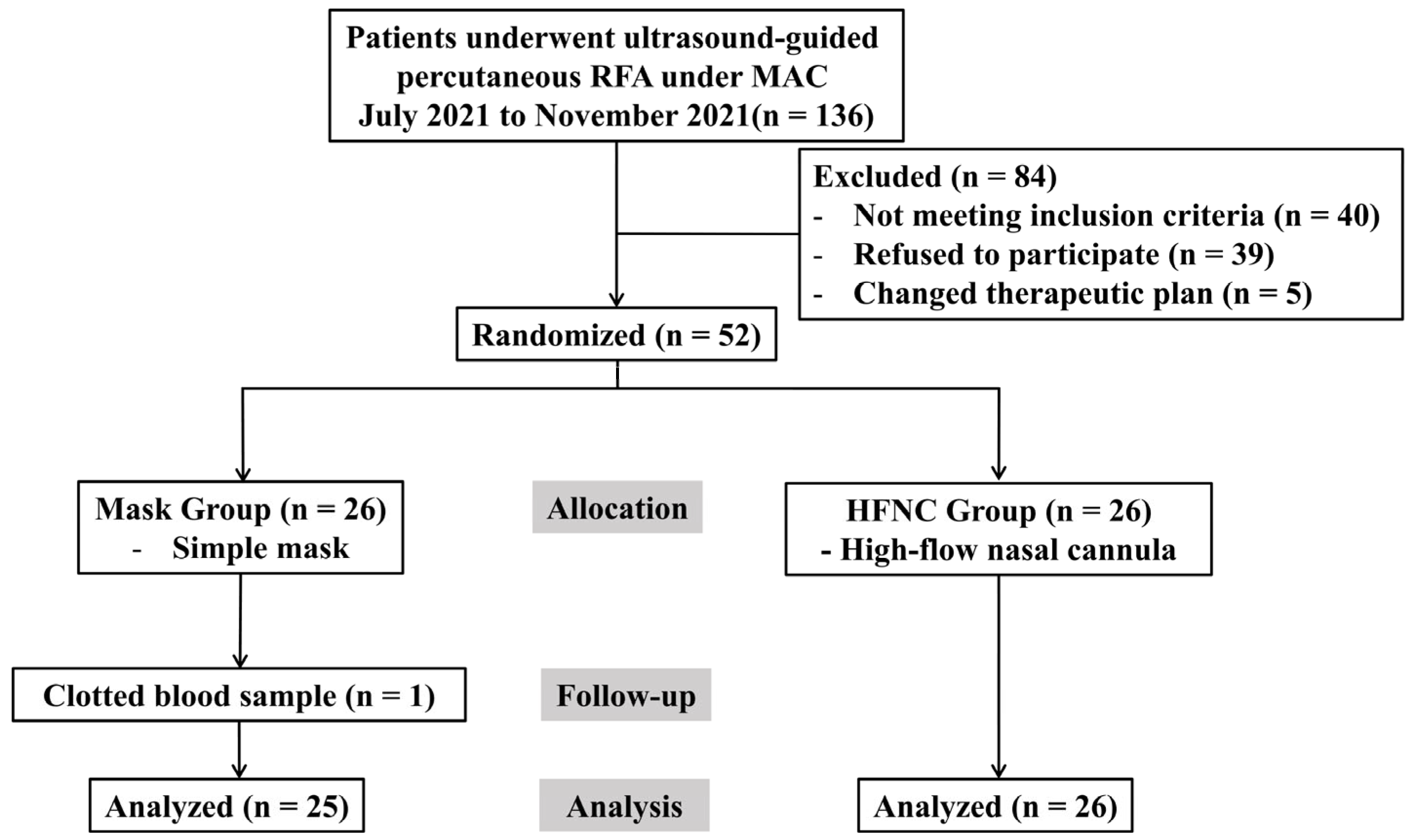
2.1. Participants
2.2. Anesthetic Management
2.3. Ablation Procedure
2.4. Outcome Measurements
2.5. Sample Size Calculation
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| RFA | Radiofrequency ablation |
| MAC | Monitored anesthesia care |
| HFNC | High-flow nasal cannula |
| FiO2 | Fraction of inspired oxygen |
| PEEP | Positive end-expiratory pressure |
| SpO2 | Peripheral oxygen saturation |
| PaO2 | Arterial oxygen partial pressure |
| PaCO2 | Arterial partial pressure of carbon dioxide |
| RR | Respiratory rate |
| BIS | Bispectral index |
| ABGA | Arterial blood gas analysis |
| P/F | Ratio of arterial partial pressure of oxygen to fraction of inspired oxygen |
| ISAS | Iowa Satisfaction with Anesthesia Scale |
| ANCOVA | Analysis of covariance |
| COPD | Chronic obstructive pulmonary disease |
| CI | Confidence interval |
References
- Tatli, S.; Tapan, U.; Morrison, P.R.; Silverman, S.G. Radiofrequency ablation: Technique and clinical applications. Diagn. Interv. Radiol. 2012, 18, 508–516. [Google Scholar] [CrossRef] [PubMed]
- McGhana, J.P.; Dodd, G.D., 3rd. Radiofrequency ablation of the liver: Current status. Am. J. Roentgenol. 2001, 176, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Jeong, H.; Kim, D.; Kim, D.K.; Chung, I.S.; Bang, Y.J.; Kim, K.; Kim, M.; Choi, J.W. Comparison of respiratory effects between dexmedetomidine and propofol sedation for ultrasound-guided radiofrequency ablation of hepatic neoplasm: A randomized controlled trial. J. Clin. Med. 2021, 10, 3040. [Google Scholar] [CrossRef]
- Sato, K.; Taniki, N.; Kanazawa, R.; Shimizu, M.; Ishii, S.; Ohama, H.; Takawa, M.; Nagamatsu, H.; Imai, Y.; Shiina, S. Efficacy and safety of deep sedation in percutaneous radiofrequency ablation for hepatocellular carcinoma. Adv. Ther. 2019, 36, 344–354. [Google Scholar] [CrossRef]
- Ghisi, D.; Fanelli, A.; Tosi, M.; Nuzzi, M.; Fanelli, G. Monitored anesthesia care. Minerva Anestesiol. 2005, 71, 533–538. [Google Scholar]
- Kimura, S.; Sone, M.; Sugawara, S.; Itou, C.; Ozawa, M.; Sato, T.; Matsui, Y.; Arai, Y.; Kusumoto, M. Safety of propofol sedation administered by interventional radiologists for radiofrequency ablation in patients with hepatocellular carcinoma. Jpn. J. Radiol. 2024, 42, 1290–1297. [Google Scholar] [CrossRef]
- Bhananker, S.M.; Posner, K.L.; Cheney, F.W.; Caplan, R.A.; Lee, L.A.; Domino, K.B. Injury and liability associated with monitored anesthesia care: A closed claims analysis. Anesthesiology 2006, 104, 228–234. [Google Scholar] [CrossRef]
- Sharma, V.K.; Nguyen, C.C.; Crowell, M.D.; Lieberman, D.A.; de Garmo, P.; Fleischer, D.E. A national study of cardiopulmonary unplanned events after GI endoscopy. Gastrointest. Endosc. 2007, 66, 27–34. [Google Scholar] [CrossRef]
- Arrowsmith, J.B.; Gerstman, B.B.; Fleischer, D.E.; Benjamin, S.B. Results from the American Society for Gastrointestinal Endoscopy/U.S. Food and Drug Administration collaborative study on complication rates and drug use during gastrointestinal endoscopy. Gastrointest. Endosc. 1991, 37, 421–427. [Google Scholar] [CrossRef]
- Spoletini, G.; Alotaibi, M.; Blasi, F.; Hill, N.S. Heated humidified high-flow nasal oxygen in adults: Mechanisms of action and clinical implications. Chest 2015, 148, 253–261. [Google Scholar] [CrossRef]
- Ghoshal, A.G. Hypoxemia and oxygen therapy. J. Assoc. Chest Physicians 2020, 8, 42–47. [Google Scholar] [CrossRef]
- Lin, Y.; Zhang, X.; Li, L.; Wei, M.; Zhao, B.; Wang, X.; Pan, Z.; Tian, J.; Yu, W.; Su, D. High-flow nasal cannula oxygen therapy and hypoxia during gastroscopy with propofol sedation: A randomized multicenter clinical trial. Gastrointest. Endosc. 2019, 90, 591–601. [Google Scholar] [CrossRef] [PubMed]
- Renda, T.; Corrado, A.; Iskandar, G.; Pelaia, G.; Abdalla, K.; Navalesi, P. High-flow nasal oxygen therapy in intensive care and anaesthesia. Br. J. Anaesth. 2018, 120, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Douglas, N.; Ng, I.; Nazeem, F.; Lee, K.; Mezzavia, P.; Krieser, R.; Steinfort, D.; Irving, L.; Segal, R. A randomised controlled trial comparing high-flow nasal oxygen with standard management for conscious sedation during bronchoscopy. Anaesthesia 2018, 73, 169–176. [Google Scholar] [CrossRef]
- Sheahan, C.G.; Mathews, D.M. Monitoring and delivery of sedation. Br. J. Anaesth. 2014, 113 (Suppl. S2), ii37–ii47. [Google Scholar] [CrossRef]
- Kim, H.J.; Lee, C.Y.; Lee, K.; Kim, N.; Lee, S.; Oh, Y.J. Comparison of high-flow nasal oxygenation and standard low-flow nasal oxygenation during rigid bronchoscopy: A randomized controlled trial. Korean J. Anesthesiol. 2025, 78, 39–47. [Google Scholar] [CrossRef]
- Dexter, F. Iowa Satisfaction with Anesthesia Scale. Korean J. Anesthesiol. 2012, 62, 297. [Google Scholar] [CrossRef]
- Sohn, H.M.; Ryu, J.H. Monitored anesthesia care in and outside the operating room. Korean J. Anesthesiol. 2016, 69, 319–326. [Google Scholar] [CrossRef]
- Heinrich, S.; Horbach, T.; Stubner, B.; Prottengeier, J.; Irouschek, A.; Schmidt, J. Benefits of heated and humidified high flow nasal oxygen for preoxygenation in morbidly obese patients undergoing bariatric surgery: A randomized controlled study. J. Obes. Bariatrics 2014, 1, 7. [Google Scholar]
- Hillman, D.R.; Platt, P.R.; Eastwood, P.R. The upper airway during anaesthesia. Br. J. Anaesth. 2003, 91, 31–39. [Google Scholar] [CrossRef]
- Nishimura, M. High-flow nasal cannula oxygen therapy in adults: Physiological benefits, indication, clinical benefits, and adverse effects. Respir. Care 2016, 61, 529–541. [Google Scholar] [CrossRef] [PubMed]
- Parke, R.L.; Eccleston, M.L.; McGuinness, S.P. The effects of flow on airway pressure during nasal high-flow oxygen therapy. Respir. Care 2011, 56, 1151–1155. [Google Scholar] [CrossRef] [PubMed]
- Lucangelo, U.; Vassallo, F.G.; Marras, E.; Ferluga, M.; Beziza, E.; Comuzzi, L.; Berlot, G.; Zin, W.A. High-flow nasal interface improves oxygenation in patients undergoing bronchoscopy. Crit. Care Res. Pract. 2012, 2012, 506382. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.C.; Liang, P.C.; Chuang, Y.H.; Huang, Y.J.; Lin, P.J.; Wu, C.Y. Effects of high-flow nasal oxygen during prolonged deep sedation on postprocedural atelectasis: A randomised controlled trial. Eur. J. Anaesthesiol. 2020, 37, 1025–1031. [Google Scholar] [CrossRef]
- Yang, H.; Huang, D.; Luo, J.; Liang, Z.; Li, J. The use of high-flow nasal cannula in patients with chronic obstructive pulmonary disease under exacerbation and stable phases: A systematic review and meta-analysis. Heart Lung 2023, 60, 116–126. [Google Scholar] [CrossRef]
- Mündel, T.; Feng, S.; Tatkov, S.; Schneider, H. Mechanisms of nasal high flow on ventilation during wakefulness and sleep. J. Appl. Physiol. 2013, 114, 1058–1065. [Google Scholar] [CrossRef]
- Rittayamai, N.; Tscheikuna, J.; Rujiwit, P. High-flow nasal cannula versus conventional oxygen therapy after endotracheal extubation: A randomized crossover physiologic study. Respir. Care 2014, 59, 485–490. [Google Scholar] [CrossRef]
- Mauri, T.; Turrini, C.; Eronia, N.; Grasselli, G.; Volta, C.A.; Bellani, G.; Pesenti, A. Physiologic effects of high-flow nasal cannula in acute hypoxemic respiratory failure. Am. J. Respir. Crit. Care Med. 2017, 195, 1207–1215. [Google Scholar] [CrossRef]
- Wang, M.L.; Hung, M.H.; Chen, J.S.; Hsu, H.H.; Cheng, Y.J. Nasal high-flow oxygen therapy improves arterial oxygenation during one-lung ventilation in non-intubated thoracoscopic surgery. Eur. J. Cardiothorac. Surg. 2018, 53, 1001–1006. [Google Scholar] [CrossRef]
- Huang, X.; Du, Y.; Ma, Z.; Zhang, H.; Jun, L.; Wang, Z.; Lin, M.; Ni, F.; Li, X.; Tan, H.; et al. High-flow nasal cannula oxygen versus conventional oxygen for hypercapnic chronic obstructive pulmonary disease: A meta-analysis of randomized controlled trials. Clin. Respir. J. 2021, 15, 437–444. [Google Scholar] [CrossRef]
- Duan, L.; Xie, C.; Zhao, N. Effect of high-flow nasal cannula oxygen therapy in patients with chronic obstructive pulmonary disease: A meta-analysis. J. Clin. Nurs. 2022, 31, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Roy, A.; Khanna, P.; Chowdhury, S.R.; Haritha, D.; Sarkar, S. The impact of high-flow nasal cannula vs other oxygen delivery devices during bronchoscopy under sedation: A systematic review and meta-analyses. Indian. J. Crit. Care Med. 2022, 26, 1131–1140. [Google Scholar] [CrossRef] [PubMed]
- Roca, O.; Hernández, G.; Díaz-Lobato, S.; Carratalá, J.M.; Gutiérrez, R.M.; Masclans, J.R.; Spanish Multidisciplinary Group of High Flow Supportive Therapy in Adults (HiSpaFlow). Current evidence for the effectiveness of heated and humidified high flow nasal cannula supportive therapy in adult patients with respiratory failure. Crit. Care 2016, 20, 109. [Google Scholar] [CrossRef] [PubMed]
- Maitra, S.; Som, A.; Bhattacharjee, S.; Arora, M.K.; Baidya, D.K. Comparison of high-flow nasal oxygen therapy with conventional oxygen therapy and noninvasive ventilation in adult patients with acute hypoxemic respiratory failure: A meta-analysis and systematic review. J. Crit. Care 2016, 35, 138–144. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mask (n = 25) | HFNC (n = 26) | p-Value | |
|---|---|---|---|
| Age (y) | 61.1 ± 8.5 | 63.2 ± 7.9 | 0.360 |
| Sex (male/female) | 21 (84.0)/4 (16.0) | 23 (88.5)/3 (11.5) | 0.703 |
| BMI (kg/m2) | 24.6 ± 3.6 | 24.9 ± 3.1 | 0.762 |
| Diabetes | 7 (28.0) | 10 (38.5) | 0.428 |
| Hypertension | 9 (36.0) | 9 (34.6) | 0.918 |
| COPD | 4 (16.0) | 2 (7.7) | 0.419 |
| ASA classification | 0.110 | ||
| I | 3 (12.0) | 0(0.0) | |
| II | 22 (88.0) | 26 (100.0) | |
| Tumor type | 1.000 | ||
| HCC | 24 (96.0) | 23 (88.5) | |
| Metastatic | 1 (4.0) | 2 (7.7) | |
| Cryptogenic LC | 0 (0.0) | 1 (3.8) | |
| Tumor size (cm) | 1.6 ± 0.5 | 1.5 ± 0.4 | 0.310 |
| Pre-procedure ABGA | |||
| pH (mmHg) | 7.4 (7.4, 7.4) | 7.4 (7.4, 7.4) | 0.572 |
| PaCO2 (mmHg) | 38.3 (35.6, 40.4) | 37.5 (31.8, 39.0) | 0.158 |
| PaO2 (mmHg) | 85.8 (77.9, 98.8) | 95.4 (86.2, 107.0) | 0.037 |
| HCO3− (mmol/l) | 24.3 ± 2.6 | 23.2 ± 3.0 | 0.173 |
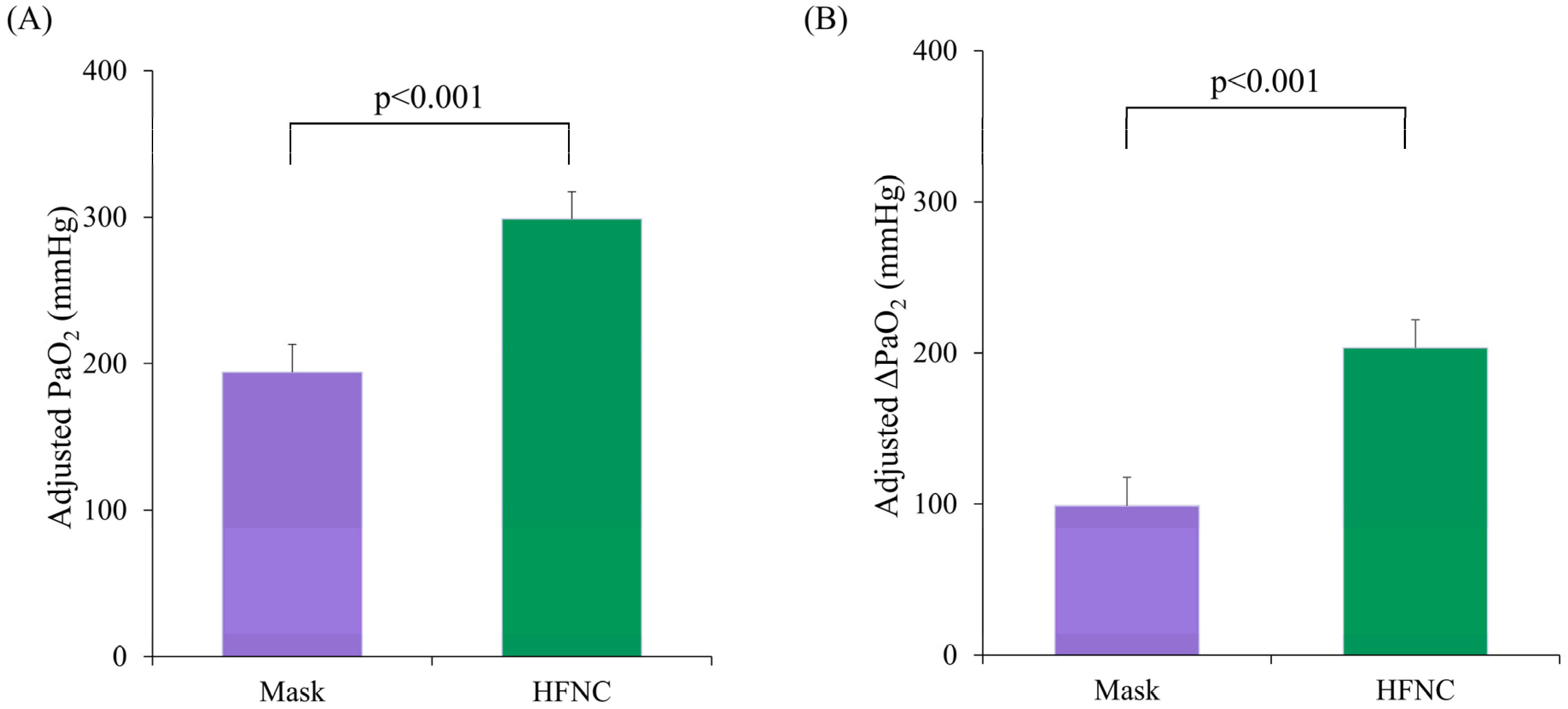
| P/F ratio | 171.6 (155.7, 197.6) | 95.4 (86.2 107.0) | <0.001 |
| Total ablation time (min) | 8.0 (6.0, 10.0) | 6.5 (5.0, 12.0) | 0.374 |
| Sedation time (min) | 34.0 (29.5, 47.5) | 28.0 (26.0, 40.5) | 0.262 |
| Total dose of propofol (mg) | 77.0 (67.0, 103.0) | 75.0 (57.1, 99.0) | 0.445 |
| Total dose of remifentanil (ng) | 88.7 (70.6, 108.0) | 76.1 (63.5, 96.3) | 0.366 |
| Type of procedure | 0.301 | ||
| Conventional | 17 (68.0) | 14 (53.8) | |
| Microwave | 8 (32.0) | 12 (46.2) | |
| Use of artificial ascites | 7 (28.0) | 7 (26.9) | 0.931 |
| Mask (n = 25) | HFNC (n = 26) | Crude p-Value | Bonferroni- Corrected p-Value | |
|---|---|---|---|---|
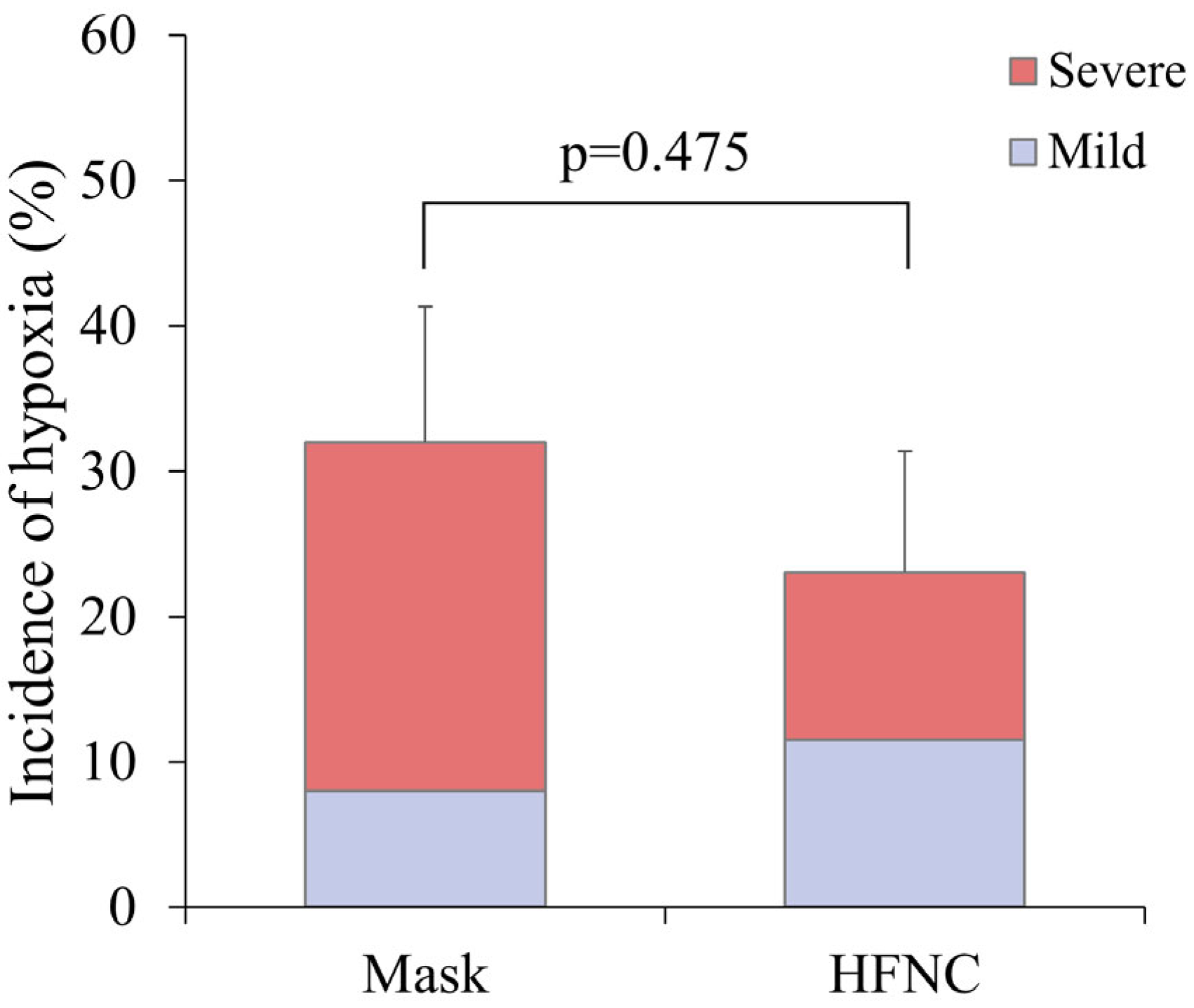
| Incidence of hypoxia (95% CI) | 32.0 ± 9.3 (13.7–50.3) | 23.1 ± 8.3 (6.9–39.3) | 0.475 | 1.000 |
| Intra-procedure ABGA | ||||
| ∆P/F ratio (95% CI) * | 246.1 ± 30.8 (184.2−308.0) | 158.6 ± 30.0 (98.3−218.9) | 0.084 | 0.336 |
| ∆PaCO2 (mmHg) (95% CI) † | 13.6 ± 4.59 (4.30–22.8) | 14.2 ± 5.00 (4.13–24.3) | 0.789 | 1.000 |
| Satisfaction | ||||
| Patient satisfaction (95% CI) | 25.0 ± 2.1 (20.7–29.4) | 21.1 ± 2.4 (16.1–26.1) | 0.270 | 1.000 |
| Variable | Group | Analysis for Repeated Measures | ||||
|---|---|---|---|---|---|---|
| Average (n = 51) | Mask (n = 25) | HFNC (n = 26) | p | Source | p * | |
| Respiratory rate (breath/min) | ||||||
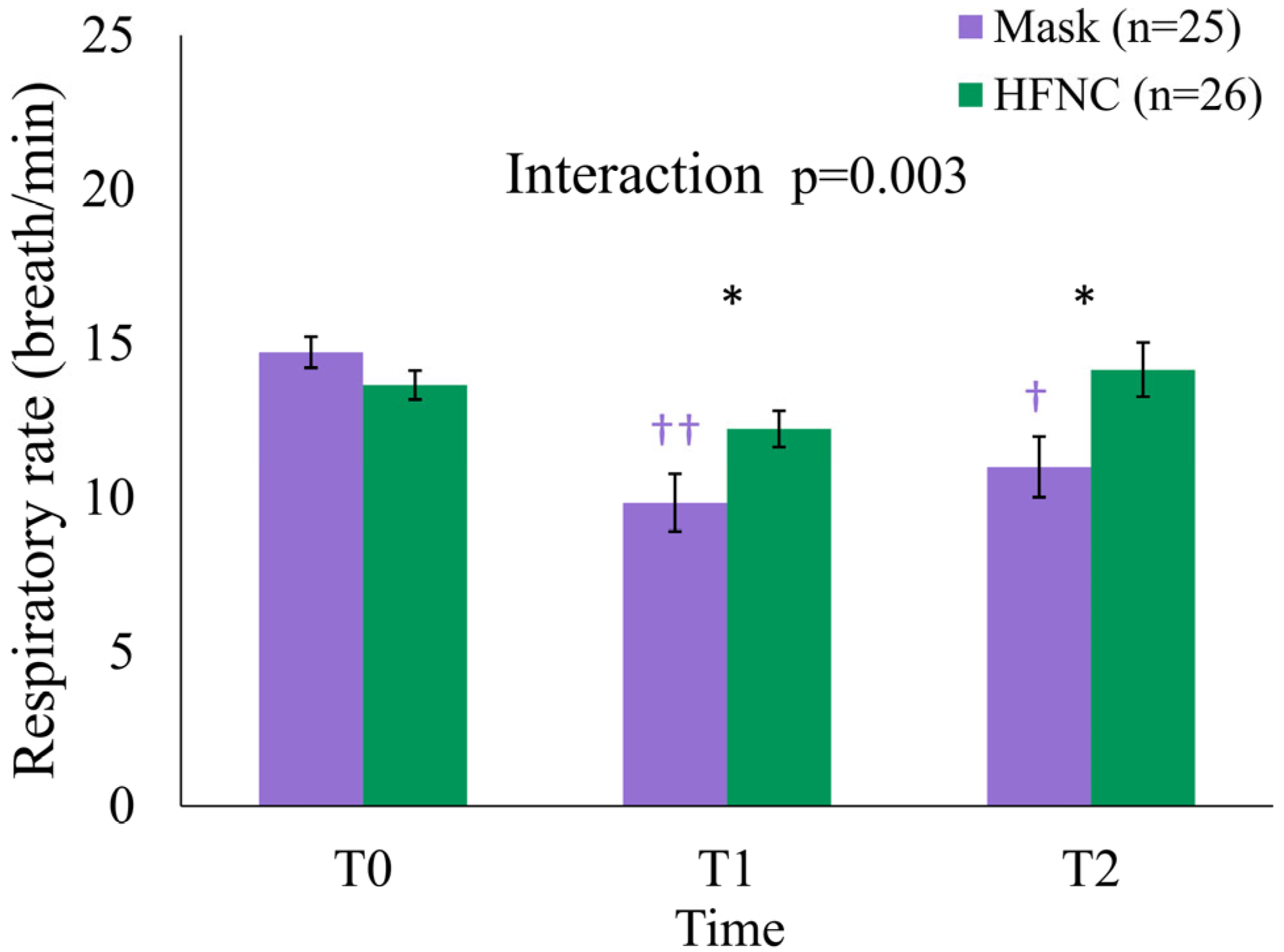
| T0 | 14.2 ± 2.5 | 14.7 ± 2.5 a | 13.7 ± 2.4 a | 0.131 1 | Group | 0.090 |
| T1 | 11.1 ± 4.1 | 9.8 ± 4.7 b | 12.2 ± 3.0 a | 0.036 1 | Time | 0.024 |
| T2 | 12.6 ± 4.9 | 11.0 ± 4.9 b | 14.2 ± 4.5 a | 0.031 2 | Group × Time | 0.003 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, J.-P.; Kim, G.W.; Yoon, J.-U.; Park, H.; Joung, K.-w. Effect of High-Flow Nasal Cannula vs. Facemask on Arterial Oxygenation During Liver Radiofrequency Ablation: Randomized Controlled Trial. Medicina 2025, 61, 1130. https://doi.org/10.3390/medicina61071130
Yoon J-P, Kim GW, Yoon J-U, Park H, Joung K-w. Effect of High-Flow Nasal Cannula vs. Facemask on Arterial Oxygenation During Liver Radiofrequency Ablation: Randomized Controlled Trial. Medicina. 2025; 61(7):1130. https://doi.org/10.3390/medicina61071130
Chicago/Turabian StyleYoon, Jung-Pil, Go Wun Kim, Ji-Uk Yoon, Hyeonsoo Park, and Kyoung-woon Joung. 2025. "Effect of High-Flow Nasal Cannula vs. Facemask on Arterial Oxygenation During Liver Radiofrequency Ablation: Randomized Controlled Trial" Medicina 61, no. 7: 1130. https://doi.org/10.3390/medicina61071130
APA StyleYoon, J.-P., Kim, G. W., Yoon, J.-U., Park, H., & Joung, K.-w. (2025). Effect of High-Flow Nasal Cannula vs. Facemask on Arterial Oxygenation During Liver Radiofrequency Ablation: Randomized Controlled Trial. Medicina, 61(7), 1130. https://doi.org/10.3390/medicina61071130