
Prevalence of Sexual Dysfunction with Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS): An Updated Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection and Screening
2.3. Data Extraction
2.4. Quality of Studies and Risk of Bias
2.5. Assessment of Certainty in the Body of Evidence
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
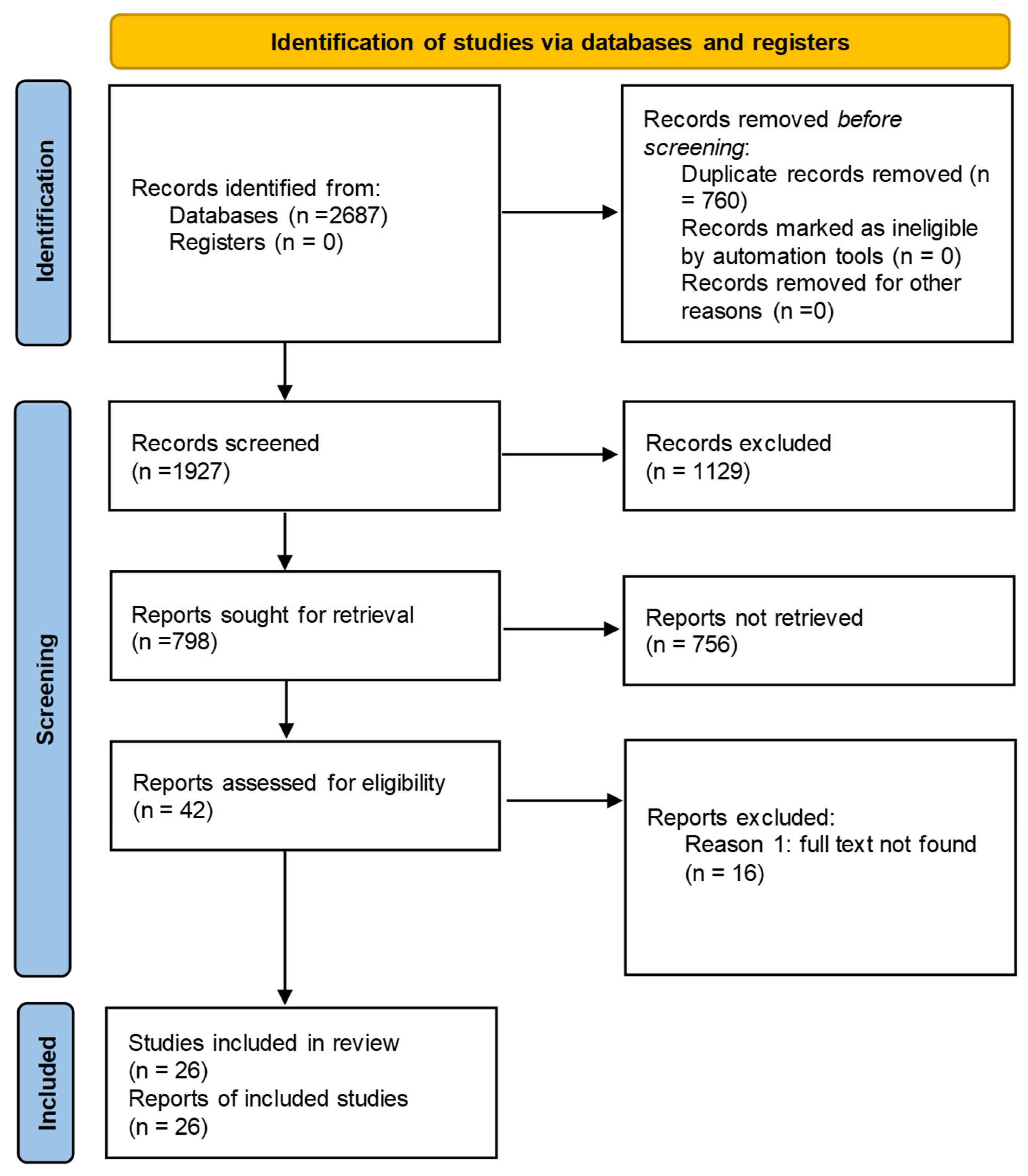
3.1. Flow of Studies
3.2. Characteristics of Observational Studies Included in Meta-Analysis
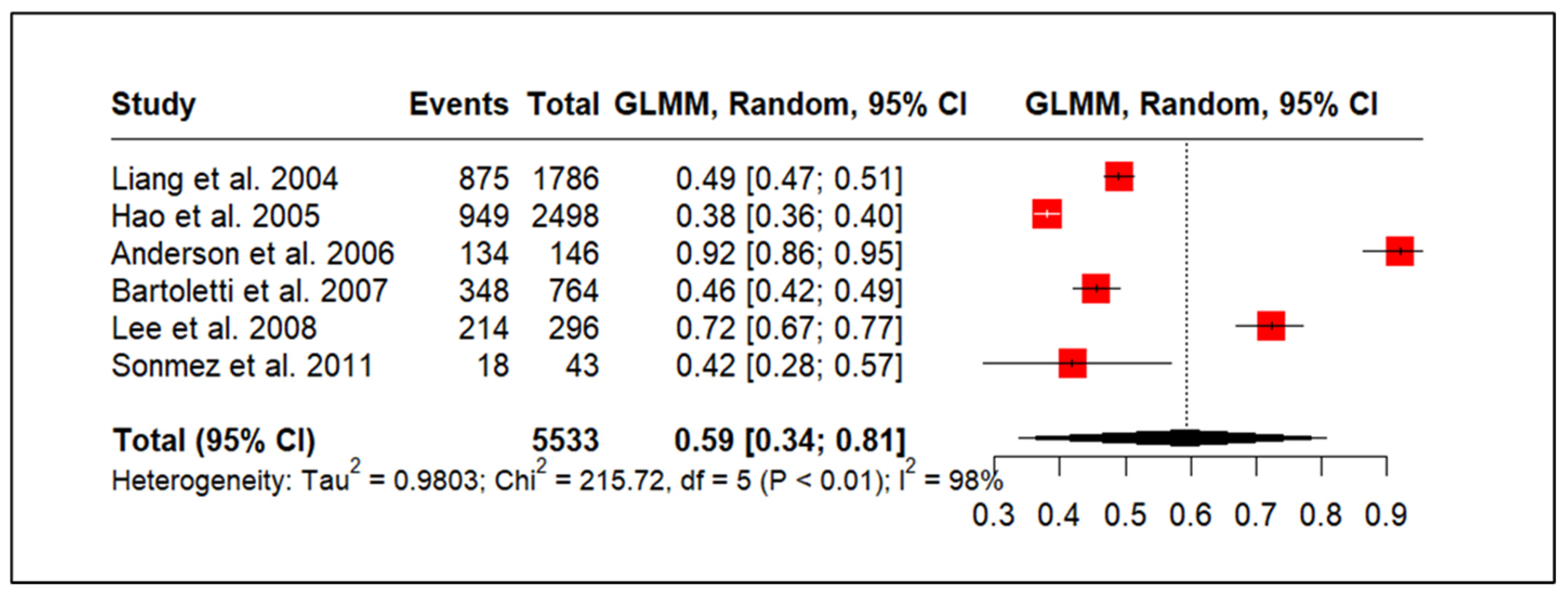
3.3. CP/CPPS and Sexual Dysfunction
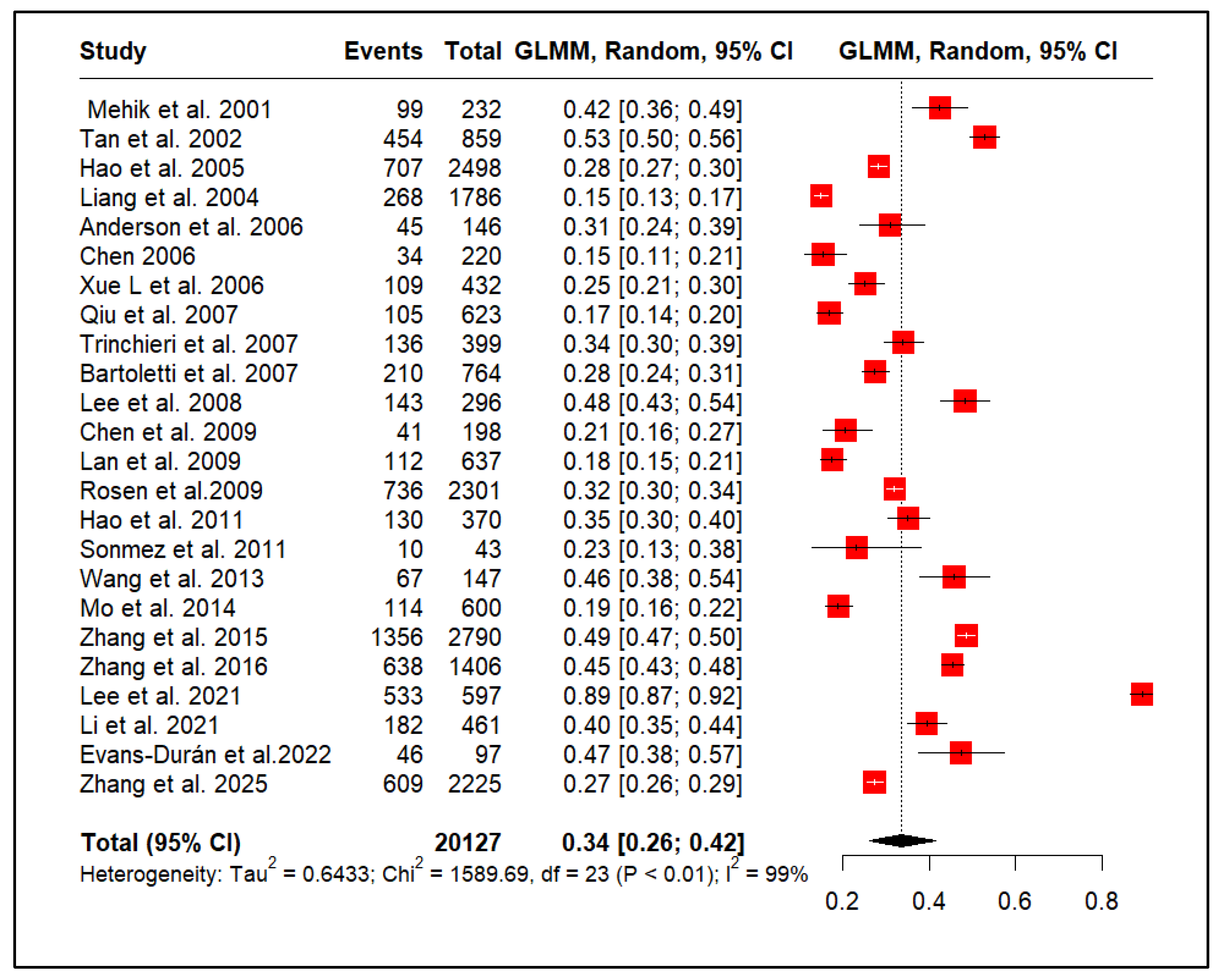
3.4. CP/CPPS and Premature Ejaculation
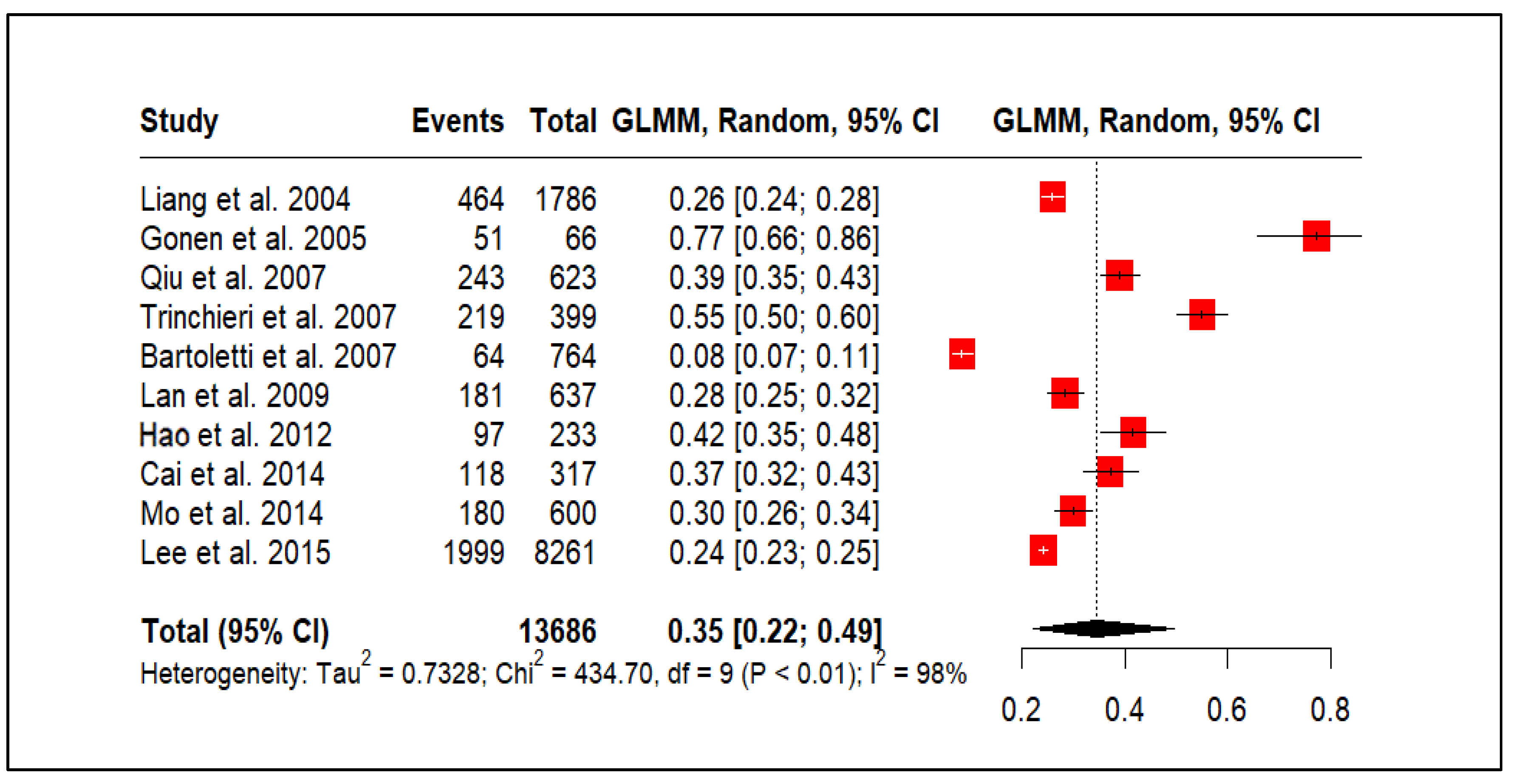
3.5. CP/CPPS and Erectile Dysfunction
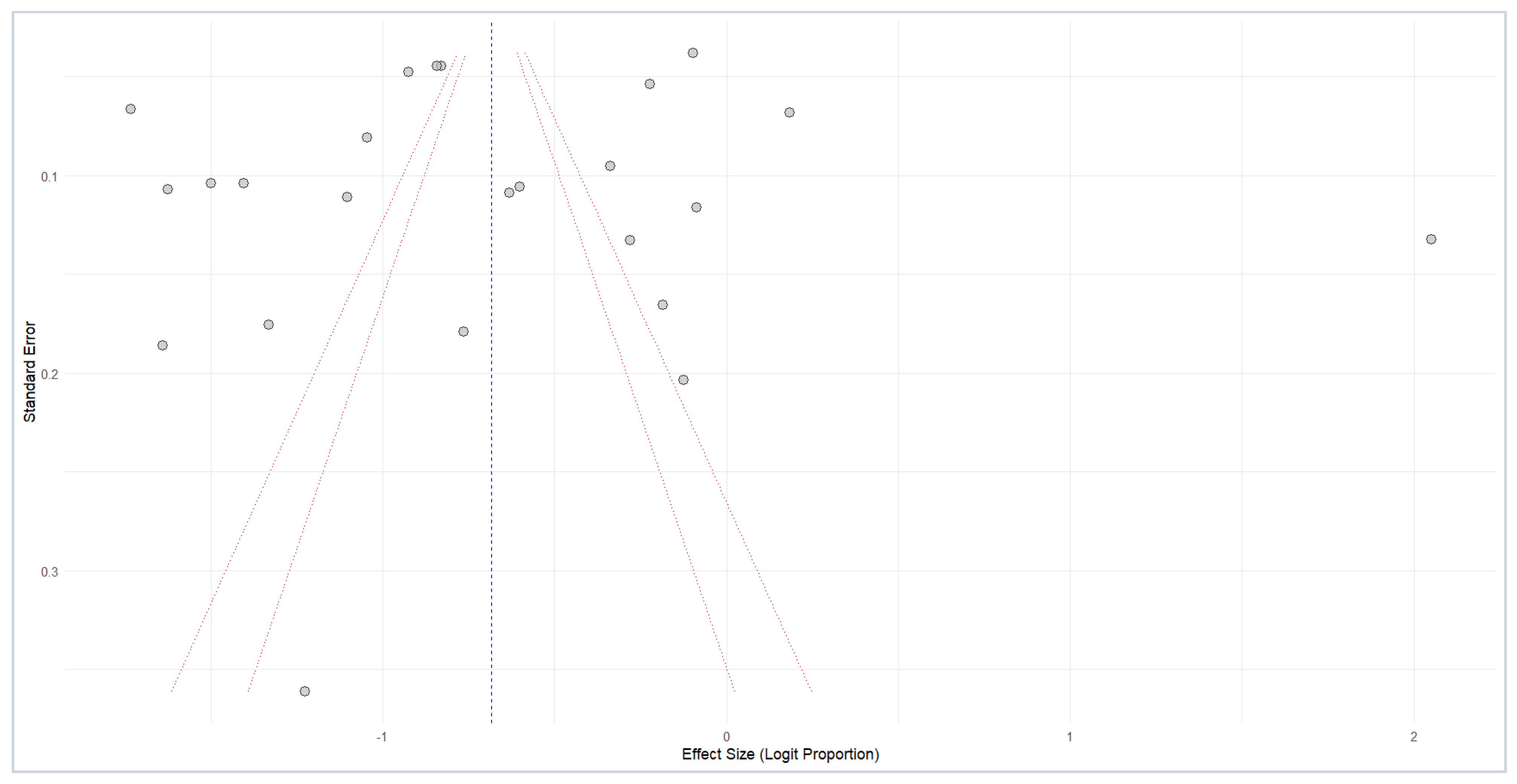
3.6. Publication Bias
3.7. Study Quality and Risk of Bias
3.8. Certainty of Evidence
4. Discussion
Strengths and Limitations
5. Conclusions
Implications for Future Research and Clinical Practice
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CP | Chronic prostatitis |
| CPPS | Chronic Pelvic Pain Syndrome |
| EAU | European Association of Urology |
| PE | Premature Ejaculation |
| ED | Erectile Dysfunction |
| MOOSE | Meta-analysis of Observational Studies in Epidemiology |
| PICO | Population, Intervention, Comparison, and Outcome |
References
- Healy, R.; Thorne, C.; Manjunath, A. Chronic prostatitis (chronic pelvic pain syndrome). BMJ 2023, 383, e073908. [Google Scholar] [CrossRef] [PubMed]
- Pendegast, H.; Leslie, S.; Rosario, D. Chronic Prostatitis and Chronic Pelvic Pain Syndrome in Men; StatPearls: St. Petersburg, FL, USA, 2024. [Google Scholar]
- Chen, J.; Zhang, H.; Niu, D.; Li, H.; Wei, K.; Zhang, L.; Yin, S.; Liu, L.; Zhang, X.; Zhang, M.; et al. The risk factors related to the severity of pain in patients with Chronic Prostatitis/Chronic Pelvic Pain Syndrome. BMC Urol. 2020, 20, 154. [Google Scholar] [CrossRef] [PubMed]
- Lam, J.C.; Stokes, W. Acute and Chronic Prostatitis. Am. Fam. Physician 2024, 110, 45–51. [Google Scholar] [PubMed]
- Ma, X.; Lao, Y.; Bai, Y.; Guan, X.; Jiang, J.; Cui, M.; Dong, Z. Study progress of etiologic mechanisms of chronic prostatitis/chronic pelvic pain syndrome. Int. Immunopharmacol. 2025, 148, 114128. [Google Scholar] [CrossRef]
- Li, A.S.-W.; Wong, A.L.Y.; Matthewson, M.; Van Niekerk, L.; Garry, M. Barriers in chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) management: Perspectives from health practitioners. Scand. J. Pain. 2023, 23, 518–530. [Google Scholar] [CrossRef]
- Yebes, A.; Toribio-Vazquez, C.; Martinez-Perez, S.; Quesada-Olarte, J.; Rodriguez-Serrano, A.; Álvarez-Maestro, M.; Martinez-Piñeiro, L. Prostatitis: A review. Curr. Urol. Rep. 2023, 24, 241–251. [Google Scholar] [CrossRef]
- Fu, Y.; Zhao, J.; Zhang, W.; Du, H. Comparison of economic burden of disease and quality of life in patients with premature ejaculation and erectile dysfunction. Sci. Rep. 2024, 14, 27374. [Google Scholar] [CrossRef]
- Meana, M.; Nobre, P.; Tavares, I. Sexual dysfunctions. In Tasman’s Psychiatry; Springer: Cham, Switzerland, 2023; pp. 1–45. [Google Scholar]
- Goerling, E.; Wolfe, E. Chapter 17–Sexual Dysfunction and Treatment. In Introduction to Human Sexuality; Pressbooks: Montreal, QC, Canada, 2024. [Google Scholar]
- Salonia, A.; Bettocchi, C.; Boeri, L.; Capogrosso, P.; Carvalho, J.; Cilesiz, N.C.; Cocci, A.; Corona, G.; Dimitropoulos, K.; Gül, M. European Association of Urology guidelines on sexual and reproductive health—2021 update: Male sexual dysfunction. Eur. Urol. 2021, 80, 333–357. [Google Scholar] [CrossRef]
- Sugimoto, M.; Hijikata, Y.; Tohi, Y.; Kuroda, H.; Takei, M.; Matsuki, T.; Kamitani, T.; Kakehi, Y.; Yamamoto, Y.; Fukuhara, S. Low quality of life in men with chronic prostatitis-like symptoms. Prostate Cancer Prostatic Dis. 2022, 25, 785–790. [Google Scholar] [CrossRef]
- Elterman, D.S.; Bhattacharyya, S.K.; Mafilios, M.; Woodward, E.; Nitschelm, K.; Burnett, A.L. The quality of life and economic burden of erectile dysfunction. Res. Rep. Urol. 2021, 13, 79–86. [Google Scholar] [CrossRef]
- Mohamadkhani Shahri, L.; Allameh, F.; Nasiri, M.; Keshavarz, Z. Sexual Quality of Life and Its Contributory Factors in Iranian Couples with Benign Prostatic Hyperplasia-Afflicted Spouses: A Cross-sectional Study. Crescent J. Med. Biol. Sci. 2023, 12, 42–53. [Google Scholar] [CrossRef]
- Chen, X.; Zhou, Z.; Qiu, X.; Wang, B.; Dai, J. The Effect of Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS) on Erectile Function: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0141447. [Google Scholar] [CrossRef] [PubMed]
- Li, H.-J.; Kang, D.-Y. Prevalence of sexual dysfunction in men with chronic prostatitis/chronic pelvic pain syndrome: A meta-analysis. World J. Urol. 2016, 34, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Brooke, B.S.; Schwartz, T.A.; Pawlik, T.M. MOOSE reporting guidelines for meta-analyses of observational studies. JAMA Surg. 2021, 156, 787–788. [Google Scholar] [CrossRef]
- Nishikawa-Pacher, A. Research questions with PICO: A universal mnemonic. Publications 2022, 10, 21. [Google Scholar] [CrossRef]
- Ghaferi, A.A.; Schwartz, T.A.; Pawlik, T.M. STROBE reporting guidelines for observational studies. JAMA Surg. 2021, 156, 577–578. [Google Scholar] [CrossRef]
- Schünemann, H.J. Using systematic reviews in guideline development: The GRADE approach. Syst. Rev. Health Res. Meta-Anal. Context 2022, 424–448. [Google Scholar] [CrossRef]
- Schwarzer, G. Meta-analysis. In Systematic Reviews in Health Research: Meta-Analysis in Context; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 2022; pp. 510–534. [Google Scholar]
- Langan, D. Assessing heterogeneity in random-effects meta-analysis. In Meta-Research: Methods and Protocols; Springer: Berlin/Heidelberg, Germany, 2021; pp. 67–89. [Google Scholar]
- Stroup, W.W.; Ptukhina, M.; Garai, J. Generalized Linear Mixed Models: Modern Concepts, Methods and Applications; Chapman and Hall/CRC: Boca Raton, FL, USA, 2024. [Google Scholar]
- Migliavaca, C.B.; Stein, C.; Colpani, V.; Barker, T.H.; Ziegelmann, P.K.; Munn, Z.; Falavigna, M.; Prevalence Estimates Reviews—Systematic Review Methodology Group. Meta-analysis of prevalence: I2 statistic and how to deal with heterogeneity. Res. Synth. Methods 2022, 13, 363–367. [Google Scholar] [CrossRef]
- Schulzke, S. Assessing and exploring heterogeneity. In Principles and Practice of Systematic Reviews and Meta-Analysis; Springer: Berlin/Heidelberg, Germany, 2021; pp. 33–41. [Google Scholar]
- Dowdy, A.; Hantula, D.A.; Travers, J.C.; Tincani, M. Meta-analytic methods to detect publication bias in behavior science research. Perspect. Behav. Sci. 2022, 45, 37–52. [Google Scholar] [CrossRef]
- Michael, H. The power functions of Begg’s and Egger’s tests for publication bias. Stat. Neerl. 2025, 79, e12364. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Sönmez, N.; Kiremit, M.; Güney, S.; Arisan, S.; Akca, O.; Dalkılıç, A. Sexual dysfunction in type III chronic prostatitis (CP) and chronic pelvic pain syndrome (CPPS) observed in Turkish patients. Int. Urol. Nephrol. 2011, 43, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lee, S.W. Relationship between premature ejaculation and chronic prostatitis/chronic pelvic pain syndrome. J. Sex. Med. 2015, 12, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Mehik, A.; Hellström, P.; Sarpola, A.; Lukkarinen, O.; Järvelin, M.R. Fears, sexual disturbances and personality features in men with prostatitis: A population-based cross-sectional study in Finland. BJU Int. 2001, 88, 35–38. [Google Scholar] [CrossRef]
- Tan, J.; Pug, D.; Liew, L.; Li, M.; Wong, M. Prevalence of prostatitis-like symptoms in Singapore: A population-based study. Singap. Med. J. 2002, 43, 189–193. [Google Scholar]
- Liang, C.Z.; Zhang, X.J.; Hao, Z.Y.; Shi, H.Q.; Wang, K.X. Prevalence of sexual dysfunction in Chinese men with chronic prostatitis. BJU Int. 2004, 93, 568–570. [Google Scholar] [CrossRef]
- Hao, Z.; Liang, C.; Wu, L.; Shi, H.; Liu, C. The impact of chronic prostatitis on the patient’s quality of life. Chin. J. Urol. 2005, 26, 367–370. [Google Scholar]
- Gonen, M.; Kalkan, M.; Cenker, A.; Ozkardes, H. Prevalence of premature ejaculation in Turkish men with chronic pelvic pain syndrome. J. Androl. 2005, 26, 601–603. [Google Scholar] [CrossRef]
- Xue, L.; Renqian, W.; Jianjun, L. Relationship Analysis between Chronic Prostatitis and Sexual Dysfunction. Chin. J. Fam. Plan. 2006, 14, 432. [Google Scholar]
- Anderson, R.U.; Wise, D.; Sawyer, T.; Chan, C.A. Sexual dysfunction in men with chronic prostatitis/chronic pelvic pain syndrome: Improvement after trigger point release and paradoxical relaxation training. J. Urol. 2006, 176, 1534–1539. [Google Scholar] [CrossRef]
- Qiu, Y.; Xie, C.; Zeng, X.; Zhang, J. Investigation of sexual function in 623 patients with chronic prostatitis. Zhonghua Nan Ke Xue = Natl. J. Androl. 2007, 13, 524–526. [Google Scholar]
- Trinchieri, A.; Magri, V.; Cariani, L.; Bonamore, R.; Restelli, A.; Garlaschi, M.C.; Perletti, G. Prevalence of sexual dysfunction in men with chronic prostatitis/chronic pelvic pain syndrome. Arch. Ital. Di Urol. Androl. 2007, 79, 67. [Google Scholar]
- Bartoletti, R.; Cai, T.; Mondaini, N.; Dinelli, N.; Pinzi, N.; Pavone, C.; Gontero, P.; Gavazzi, A.; Giubilei, G.; Prezioso, D. Prevalence, incidence estimation, risk factors and characterization of chronic prostatitis/chronic pelvic pain syndrome in urological hospital outpatients in Italy: Results of a multicenter case-control observational study. J. Urol. 2007, 178, 2411–2415. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.H.; Liong, M.L.; Yuen, K.H.; Leong, W.S.; Cheah, P.Y.; Khan, N.A.K.; Krieger, J.N. Adverse impact of sexual dysfunction in chronic prostatitis/chronic pelvic pain syndrome. Urology 2008, 71, 79–84. [Google Scholar] [CrossRef]
- Chen, Z.-B.; Song, Y.-S.; Cui, J.; Zhang, H.; Fei, X. Influence of chronic prostatitis/chronic pelvic pain syndromes on male health. Zhonghua Nan Ke Xue = Natl. J. Androl. 2009, 15, 1108–1111. [Google Scholar]
- Lan, T.; Wang, Y.; Chen, Y. Investigation of sexual dysfunction among chronic prostatitis patients in high altitude area. Zhonghua Nan Ke Xue = Natl. J. Androl. 2009, 15, 886–890. [Google Scholar]
- Rosen, R.C.; Link, C.L.; O’Leary, M.P.; Giuliano, F.; Aiyer, L.P.; Mollon, P. Lower urinary tract symptoms and sexual health: The role of gender, lifestyle and medical comorbidities. BJU Int. 2009, 103, 42–47. [Google Scholar] [CrossRef]
- Hao, Z.Y.; Li, H.J.; Wang, Z.P.; Xing, J.P.; Hu, W.L.; Zhang, T.F.; Zhang, X.S.; Zhou, J.; Tai, S.; Liang, C.Z. The prevalence of erectile dysfunction and its relation to chronic prostatitis in Chinese men. J. Androl. 2011, 32, 496–501. [Google Scholar] [CrossRef]
- Wang, X.; Cui, S.; Gong, Z.; Tang, T.; Gu, J. The effects of chronic prostatitis/chronic pelvic pain syndromes on mental and sexual function. Chin. J. Androl. 2013, 27, 41–44. [Google Scholar]
- Cai, T.; Pisano, F.; Magri, V.; Verze, P.; Mondaini, N.; D’Elia, C.; Malossini, G.; Mazzoli, S.; Perletti, G.; Gontero, P.; et al. Chlamydia trachomatis infection is related to premature ejaculation in chronic prostatitis patients: Results from a cross-sectional study. J. Sex. Med. 2014, 11, 3085–3092. [Google Scholar] [CrossRef]
- Mo, M.-Q.; Long, L.-L.; Xie, W.-L.; Chen, S.; Zhang, W.-H.; Luo, C.-Q.; Deng, L.-W. Sexual dysfunctions and psychological disorders associated with type IIIa chronic prostatitis: A clinical survey in China. Int. Urol. Nephrol. 2014, 46, 2255–2261. [Google Scholar] [CrossRef]
- Zhang, Z.; Li, Z.; Yu, Q.; Wu, C.; Lu, Z.; Zhu, F.; Zhang, H.; Liao, M.; Li, T.; Chen, W. The prevalence of and risk factors for prostatitis-like symptoms and its relation to erectile dysfunction in Chinese men. Andrology 2015, 3, 1119–1124. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zheng, T.; Tu, X.A.; Chen, X.; Wang, Z.; Chen, S.; Yang, Q.; Wan, Z.; Han, D.; Xiao, H. Erectile dysfunction in chronic prostatitis/chronic pelvic pain syndrome: Outcomes from a multi-center study and risk factor analysis in a single center. PLoS ONE 2016, 11, e0153054. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Yoo, T.K.; Kang, J.Y.; Cho, J.M.; Park, Y.W.; Lee, S.W.; Choi, J.D. Relationship between erectile dysfunction and moderate to severe prostatitis-like symptoms in middle-aged men: A propensity score–matched analysis. Int. Urol. Nephrol. 2021, 53, 2261–2266. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-C.; Zhang, X.-B.; Liao, Z.-C.; Tang, Z.-Y.; Li, D.-J. Is mild erectile dysfunction associated with severe psychological symptoms in Chinese patients with moderate-to-severe chronic prostatitis/chronic pelvic pain syndrome? Asian J. Androl. 2021, 23, 319–324. [Google Scholar] [CrossRef]
- Evans-Durán, B.; Tripp, D.A.; Campbell, J.; Doiron, R.C.; Nickel, J.C. Chronic prostatitis/chronic pelvic pain syndrome-related pain symptoms and their impact on sexual functioning. Can. Urol. Assoc. J. 2022, 16, 222. [Google Scholar] [CrossRef]
- Zhang, Y.; Zang, N.; Xiang, Y.; Lin, F.; Liu, X.; Zhang, J. A comprehensive analysis of erectile dysfunction prevalence and the impact of prostate conditions on ED among US adults: Evidence from NHANES 2001–2004. Front. Endocrinol. 2025, 15, 1412369. [Google Scholar] [CrossRef]
- Corona, G. Erectile dysfunction and premature ejaculation: A continuum movens supporting couple sexual dysfunction. J. Endocrinol. Investig. 2022, 45, 2029–2041. [Google Scholar] [CrossRef]
- Herkommer, K.; Meissner, V.H.; Dinkel, A.; Jahnen, M.; Schiele, S.; Kron, M.; Ankerst, D.P.; Gschwend, J.E. Prevalence, lifestyle, and risk factors of erectile dysfunction, premature ejaculation, and low libido in middle-aged men: First results of the Bavarian Men’s Health-Study. Andrology 2024, 12, 801–808. [Google Scholar] [CrossRef]
- Li, S.W. An Examination of Psychosocial Barriers in the Management of Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS): Informing Psychosocial Interventions. Ph.D. Thesis, University of Tasmania, Hobart, Australia, 2024. [Google Scholar]
- Juganavar, A.; Joshi, K.S. Chronic pelvic pain: A comprehensive review. Cureus 2022, 14, e30691. [Google Scholar] [CrossRef]
- Cai, T.; Alidjanov, J.; Palagin, I.; Medina-Polo, J.; Nickel, J.C.; Wagenlehner, F.M. Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS): Look to the future. Prostate Cancer Prostatic Dis. 2024, 27, 239–241. [Google Scholar] [CrossRef] [PubMed]
- Mazzilli, F. Erectile dysfunction: Causes, diagnosis and treatment: An update. J. Clin. Med. 2022, 11, 6429. [Google Scholar] [CrossRef] [PubMed]
- De Vincentis, S.; Tartaro, G.; Rochira, V.; Santi, D. HIV and sexual dysfunction in men. J. Clin. Med. 2021, 10, 1088. [Google Scholar] [CrossRef] [PubMed]
- Leeners, B.; Tschudin, S.; Wischmann, T.; Kalaitzopoulos, D.R. Sexual dysfunction and disorders as a consequence of infertility: A systematic review and meta-analysis. Hum. Reprod. Update 2023, 29, 95–125. [Google Scholar] [CrossRef]
- Chen, L.; Zhang, M.; Liang, C. Chronic prostatitis and pelvic pain syndrome: Another autoimmune disease? Arch. Immunol. Et. Ther. Exp. 2021, 69, 1–8. [Google Scholar] [CrossRef]
- Yitgin, Y.; Karakose, A. Correlation of resistive index of prostatic capsular artery to clinical symptoms in men with chronic prostatitis/chronic pelvic pain syndrome. LUTS Low. Urin. Tract. Symptoms 2023, 15, 180–184. [Google Scholar] [CrossRef]
- Meng, X.; Rao, K.; Chen, J. Metabolic factors in erectile dysfunction. Front. Endocrinol. 2023, 14, 1344191. [Google Scholar] [CrossRef]
- Yani, M.S.; Eckel, S.P.; Kirages, D.J.; Rodriguez, L.V.; Corcos, D.M.; Kutch, J.J. Impaired ability to relax pelvic floor muscles in men with chronic prostatitis/chronic pelvic pain syndrome. Phys. Ther. 2022, 102, pzac059. [Google Scholar] [CrossRef]
- Huang, X. A meta-analysis of psychological factors and pain catastrophizing of chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS). J. Sex. Med. 2022, 19, S182. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PICO Element | Search Terms/Keywords | Variations/Combinations | Example (PubMed) |
|---|---|---|---|
| P (Population/Participants) | Men | Male, Males | PubMed: “male” [MeSH Terms] OR “men” [Title/Abstract] |
| Chronic Prostatitis | Chronic Bacterial Prostatitis, Chronic Pelvic Pain Syndrome, CP/CPPS, Prostatitis-like syndrome | PubMed: “prostatitis” [MeSH Terms] OR “chronic prostatitis” [Title/Abstract] OR “CPPS” [Title/Abstract] | |
| I (Intervention/Exposure) | (Not directly applicable for prevalence studies. Focus is on the condition/problem.) | N/A | N/A |
| C (Comparison/Control) | (Often not applicable for prevalence studies. Could be men without prostatitis if comparing prevalence rates, but our focus is on men with prostatitis.) | Men without CP/CPPS (if a comparative prevalence is sought) | PubMed: “healthy men” [Title/Abstract] (Use with Population terms if comparing) |
| O (Outcome) | Sexual Dysfunction | Erectile Dysfunction, Premature Ejaculation, Ejaculatory Dysfunction, Decreased Libido, Painful Ejaculation, Sexual Problems, Sexual Health, Sexual Function | PubMed: “sexual dysfunction” [MeSH Terms] OR “erectile dysfunction” [MeSH Terms] OR “premature ejaculation” [MeSH Terms] OR “sexual health” [MeSH Terms] |
| Scope | Prevalence | Frequency, Occurrence, Epidemiology, Survey, Questionnaire, Cross-sectional | PubMed: “prevalence” [MeSH Terms] OR “epidemiology” [MeSH Terms] OR “survey” [Title/Abstract] |
| Author | Year | Country | n | Age | Tools | Outcomes | SD | ED | PE |
|---|---|---|---|---|---|---|---|---|---|
| Mehik et al., 2001 [31] | 2001 | Finland | 232 | 20–59 | Self-reported | ED | NR | 42.5% | NR |
| Tan et al., 2002 [32] | 2002 | Singapore | 859 | 43.14 | NIH-CPSI and IIEF-5 | ED | NR | 52.9% | NR |
| Liang et al., 2004 [33] | 2004 | China | 1786 | 20–59 | NIH-CPSI and IIEF-5 | SD and ED | 49.0% | 15.0% | 26.0% |
| Hao et al., 2005 [34] | 2005 | China | 2498 | 20–59 | NIH-CPSI and IIEF-5 | SD and ED | 38.0% | 28.3% | NR |
| Gonen et al., 2005 [35] | 2005 | Turkey | 66 | 21–55 | NIH-CPSI | PE | NR | NR | 77.3% |
| Xue L et al., 2006 [36] | 2006 | China | 432 | 22–45 | NIH-CPSI and IIEF-5 | ED | NR | 25.2% | NR |
| Anderson et al., 2006 [37] | 2006 | USA | 146 | 18–77 | NIH-CPSI and PPSS | SD and ED | 92.0% | 31% | NR |
| Qiu et al., 2007 [38] | 2007 | China | 623 | 18–57 | CISFPE and IIEF-5 | ED and PE | NR | 16.9% | 39.0% |
| Trinchieri et al., 2007 [39] | 2007 | Italy | 399 | <50 | NIH-CPSI | ED and PE | NR | 34% | 55.0% |
| Bartoletti et al., 2007 [40] | 2007 | Italy | 764 | 25–50 | NIH-CPSI and IIEF-5 | SD, ED, and PE | 45.5% | 27.5% | 8.4% |
| Lee et al., 2008 [41] | 2008 | Malaysia | 296 | 20–69 | NIH-CPSI and IIEF-5 | SD and ED | 72.3% | 48.3% | NR |
| Chen et al., 2009 [42] | 2009 | China | 198 | 20–59 | NIH-CPSI and IIEF-5 | ED | NR | 20.7% | NR |
| Lan et al., 2009 [43] | 2009 | China | 637 | 25–61 | CISFPE and IIEF-5 | ED and PE | NR | 17.6% | 28.4% |
| Rosen et al., 2009 [44] | 2009 | USA | 2301 | 30–79 | NIH-CPSI, IPSS, and IIEF-5 | ED | NR | 32.0% | NR |
| Hao et al., 2011 [45] | 2011 | China | 370 | 15–60 | NIH-CPSI and IIEF-5 | ED | NR | 35.1% | NR |
| Sonmez et al., 2011 [29] | 2011 | Turkey | 43 | 22–48 | NIH-CPSI and IIEF | SD and ED | 41.9% | 23.3% | NR |
| Wang et al., 2013 [46] | 2013 | China | 147 | 18–64 | NIH-CPSI and IIEF-5 | ED | NR | 45.8% | NR |
| Cai et al., 2014 [47] | 2014 | Italy | 317 | 33.8 ± 5.1 | NIH-CPSI and PEDT | PE | NR | NR | 37.2% |
| Mo et al., 2014 [48] | 2014 | China | 600 | 28.95 ± 4.98 | NIH-CPSI and IIEF-5 | ED and PE | NR | 19.0% | 30.0% |
| Lee et al., 2015 [30] | 2015 | Korea | 8261 | 50.4 ± 5.5 | NIH-CPSI and IIEF-5 | PE | NR | NR | 24.2% |
| Zhang et al., 2015 [49] | 2015 | China | 2790 | 40.10 ± 0.58 | NIH-CPSI and IIEF-5 | ED | NR | 48.6% | NR |
| Zhang et al., 2016 [50] | 2016 | China | 1406 | 32.18 (18–60) | NIH-CPSI and IIEF-5 | ED | NR | 45.4% | NR |
| Lee et al., 2021 [51] | 2021 | Republic of Korea | 597 | 50.9 ± 5.6 | NIH-CPSI, PEDT, and IIEF-5 | ED | NR | 89.3% | NR |
| Li et al., 2021 [52] | 2021 | China | 461 | 33.86 ± 8.36 | NIH-CPSI, PEDT, and IIEF-6 | ED | NR | 39.5% | NR |
| Evans-Durán et al., 2022 [53] | 2022 | Multi-country | 97 | 44.22 ±11.25 | NIH-CPSI and IIEF-5 | ED | NR | 47.4% | NR |
| Zhang et al., 2025 [54] | 2025 | USA | 2225 | 40–80 | Self-reported | ED | NR | 27.5% | NR |
| Outcome | No. of Studies | Participants | Risk of Bias | Inconsistency (I2) | Indirectness | Imprecision | Publication Bias | Certainty of Evidence |
|---|---|---|---|---|---|---|---|---|
| Sexual Dysfunction | 6 | 5533 | Serious | Very serious (98%) | Not serious | Serious | Not detected | Very Low |
| Erectile Dysfunction | 10 | 13,686 | Serious | Very serious (98%) | Not serious | Not serious | Not detected | Low |
| Premature Ejaculation | 24 | 20,127 | Serious | Very serious (99%) | Not serious | Not serious | Not detected | Low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshahrani, S.; Fathi, B.A.; Abouelgreed, T.A.; El-Metwally, A. Prevalence of Sexual Dysfunction with Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS): An Updated Systematic Review and Meta-Analysis. Medicina 2025, 61, 1110. https://doi.org/10.3390/medicina61061110
Alshahrani S, Fathi BA, Abouelgreed TA, El-Metwally A. Prevalence of Sexual Dysfunction with Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS): An Updated Systematic Review and Meta-Analysis. Medicina. 2025; 61(6):1110. https://doi.org/10.3390/medicina61061110
Chicago/Turabian StyleAlshahrani, Saad, Basem A. Fathi, Tamer A. Abouelgreed, and Ashraf El-Metwally. 2025. "Prevalence of Sexual Dysfunction with Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS): An Updated Systematic Review and Meta-Analysis" Medicina 61, no. 6: 1110. https://doi.org/10.3390/medicina61061110
APA StyleAlshahrani, S., Fathi, B. A., Abouelgreed, T. A., & El-Metwally, A. (2025). Prevalence of Sexual Dysfunction with Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS): An Updated Systematic Review and Meta-Analysis. Medicina, 61(6), 1110. https://doi.org/10.3390/medicina61061110