
Understanding of Stroke Risk Among Smokers in Saudi Arabia

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Measurement Tool
2.3. Setting and Ethical Consideration
2.4. Data Analysis
3. Results
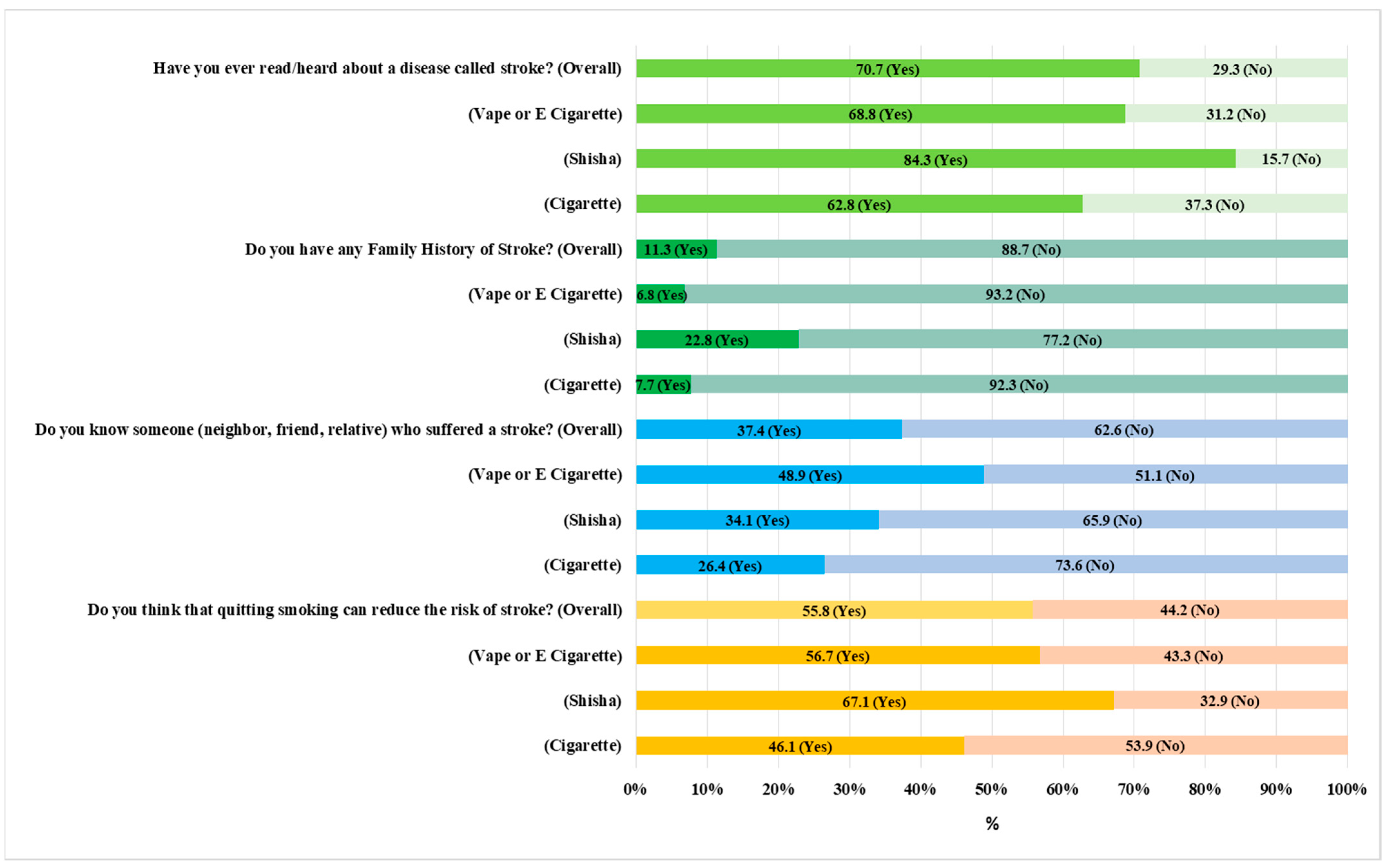
3.1. Familiarity with Stroke
3.2. Identification of Risk Factors of Stroke
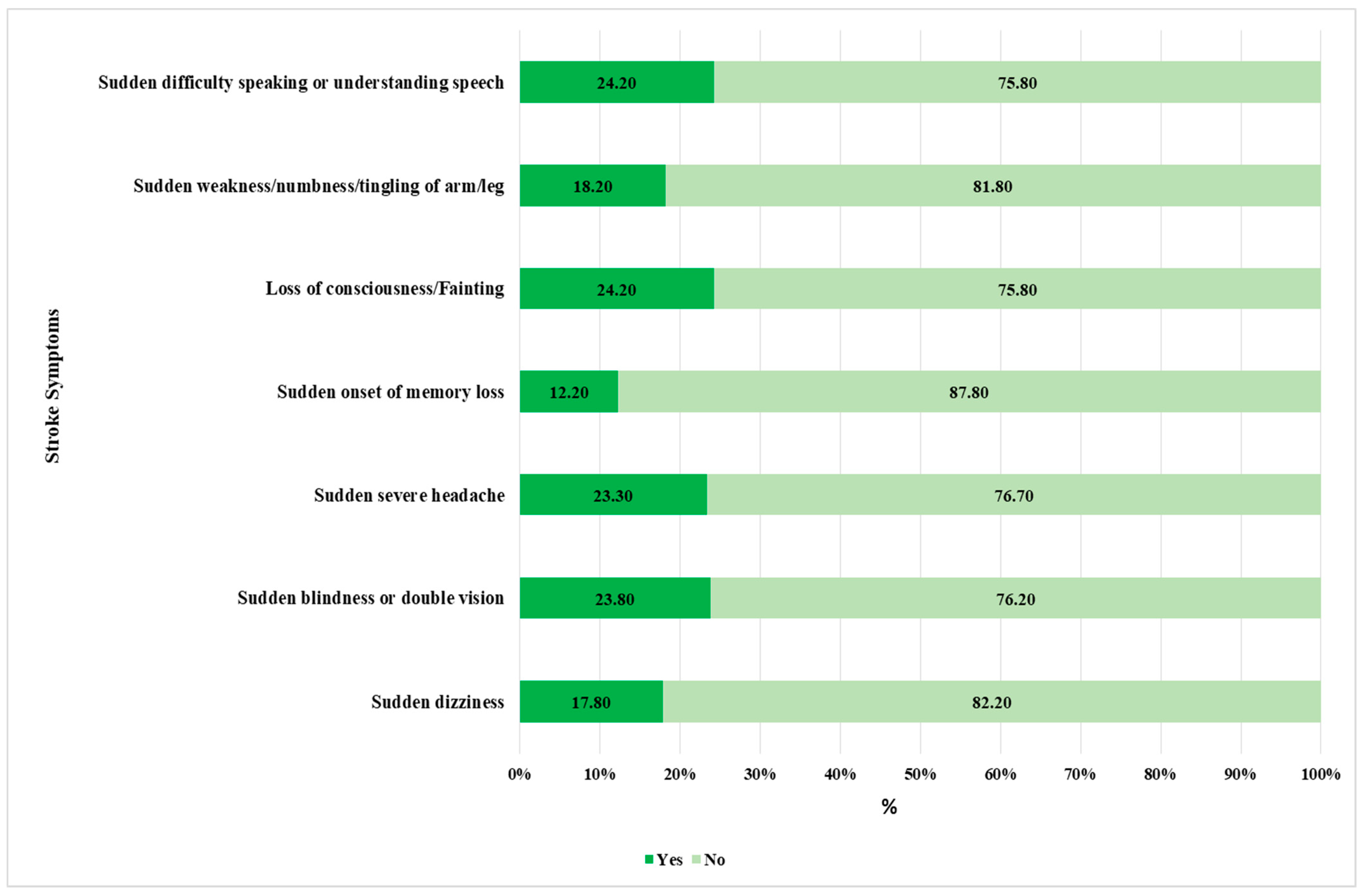
3.3. Identification of Stroke Symptoms
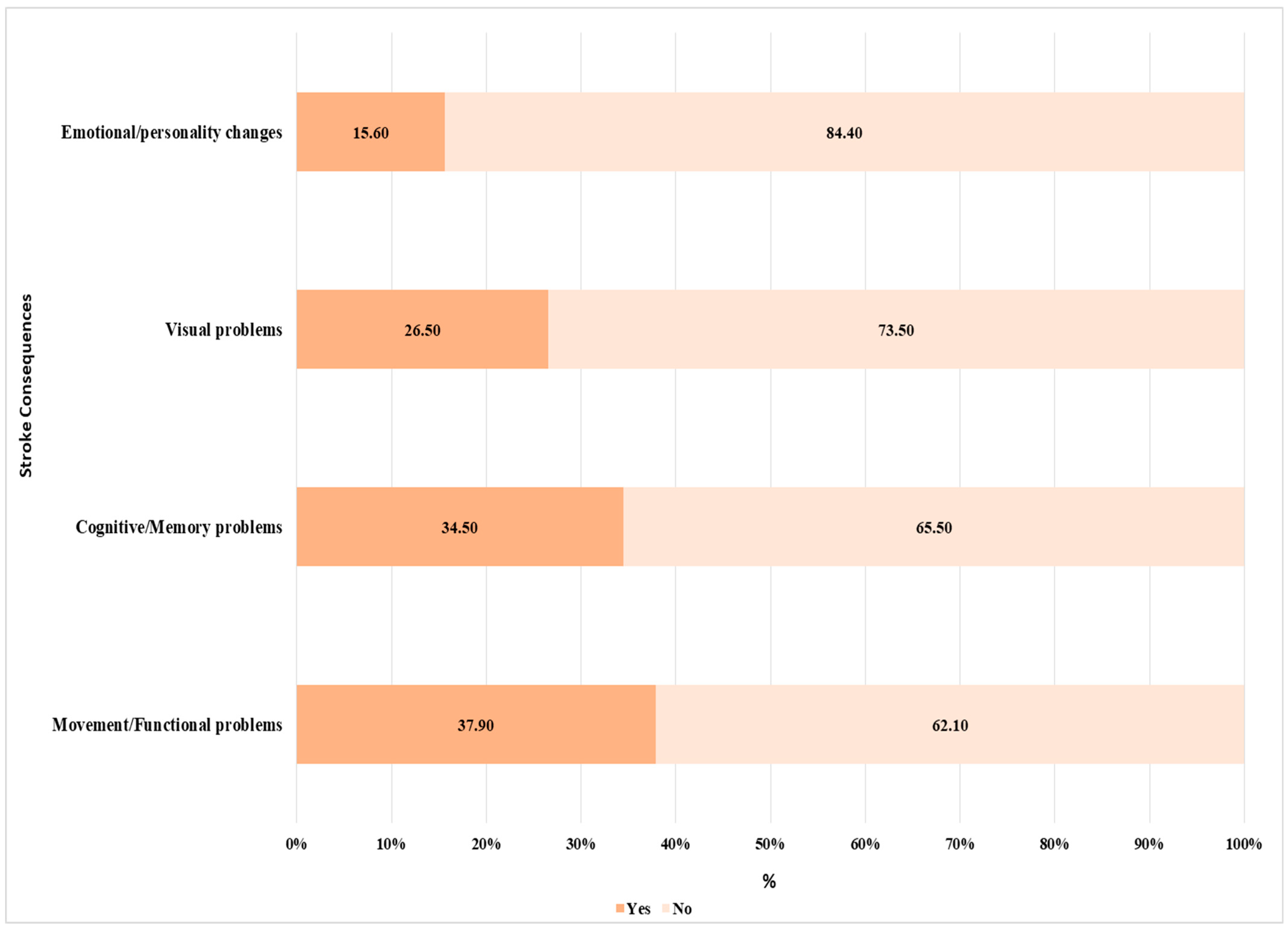
3.4. Awareness of Stroke Consequences
3.5. Association of Risk Factors, Symptoms, and Consequences of Stroke with the Socio-Demographic Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feigin, V.L.; Abate, M.D.; Abate, Y.H.; Abd ElHafeez, S.; Abd-Allah, F.; Abdelalim, A.; Abdelkader, A.; Abdelmasseh, M.; Abd-Elsalam, S.; Abdi, P.; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2021: A systematic analysis for the Global Burden of Disease Study 2021. Lancet Neurol. 2024, 23, 973–1003. [Google Scholar] [CrossRef] [PubMed]
- Niewada, M.; Michel, P. Lifestyle modification for stroke prevention: Facts and fiction. Curr. Opin. Neurol. 2016, 29, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Alluqmani, M.M.; Almshhen, N.R.; Alotaibi, R.A.; Aljardi, O.Y.; Zahid, H.M. Public Awareness of Ischemic Stroke in Medina city, Kingdom of Saudi Arabia. Neurosciences 2021, 26, 134–140. [Google Scholar] [CrossRef]
- Alqahtani, B.A.; Alenazi, A.M.; Hoover, J.C.; Alshehri, M.M.; Alghamdi, M.S.; Osailan, A.M.; Khunti, K. Incidence of stroke among Saudi population: A systematic review and meta-analysis. Neurol. Sci. 2020, 41, 3099–3104. [Google Scholar] [CrossRef]
- Boehme, A.K.; Esenwa, C.; Elkind, M.S. Stroke Risk Factors, Genetics, and Prevention. Circ. Res. 2017, 120, 472–495. [Google Scholar] [CrossRef]
- Mersal, F.A.; Tork, H.M. Stroke risk perception and its awareness among hypertensive patients in Qassim region Saudi Arabia. Majmaah J. Health Sci. 2020, 8, 9. [Google Scholar] [CrossRef]
- Mubaraki, A.A.; Alqahtani, A.S.; Almalki, A.A.; Almalki, A.H.; Alamri, H.M.; Aburass, M.K.; Althumali, Z.H. Public knowledge and awareness of stroke among adult population in Taif city, Saudi Arabia. Neurosciences 2021, 26, 339–345. [Google Scholar] [CrossRef]
- Alzahrani, F.A.; Alenzy, A.E.; Alghamdi, A.M. Stroke in Tabuk, KSA: Awareness and prevalence of risk factors. Life Sci. J. 2019, 16, 256. [Google Scholar]
- Alsubaie, F.; Alobaidallah, F.; Almustafa, S.; Alhazyim, B.; Ola Mousa, A. Assessing the knowledge of high school students about stroke as a leading cause of death in Saudi Arabia. South Asian Res. J. Nurs. Healthc. 2020, 2, 17–22. [Google Scholar] [CrossRef]
- Vangen-Lønne, A.M.; Wilsgaard, T.; Johnsen, S.H.; Løchen, M.L.; Njølstad, I.; Mathiesen, E.B. Declining Incidence of Ischemic Stroke: What Is the Impact of Changing Risk Factors? The Tromsø Study 1995 to 2012. Stroke 2017, 48, 544–550. [Google Scholar] [CrossRef]
- Tan, J.; Ramazanu, S.; Liaw, S.Y.; Chua, W.L. Effectiveness of Public Education Campaigns for Stroke Symptom Recognition and Response in Non-Elderly Adults: A Systematic Review and Meta-Analysis. J. Stroke Cerebrovasc. Dis. 2022, 31, 106207. [Google Scholar] [CrossRef] [PubMed]
- Basri, R.; Issrani, R.; Hua Gan, S.; Prabhu, N.; Khursheed Alam, M. Burden of stroke in the Kingdom of Saudi Arabia: A soaring epidemic. Saudi Pharm. J. 2021, 29, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.S.; Cole, J.W. Smoking and stroke: The more you smoke the more you stroke. Expert Rev. Cardiovasc. Ther. 2010, 8, 917–932. [Google Scholar] [CrossRef]
- Mantler, T. A systematic review of smoking Youths’ perceptions of addiction and health risks associated with smoking: Utilizing the framework of the health belief model. Addict. Res. Theory 2013, 21, 306–317. [Google Scholar] [CrossRef]
- Malaeb, D.; Dia, N.; Haddad, C.; Hallit, S.; Sacre, H.; Barakat, M.; Mansour, S.; Salameh, P.; Hosseini, H. Factors associated with knowledge and awareness of stroke among the Lebanese population: A cross-sectional study. F1000Research 2022, 11, 425. [Google Scholar] [CrossRef]
- Barakat, M.; AlSalamat, H.A.; Jirjees, F.; Al-Obaidi, H.; Hussain, Z.K.; El Hadidi, S.; Mansour, S.; Malaeb, D.; Hosseini, H. Factors Associated with Knowledge and Awareness of Stroke Among the Jordanian Population: A Cross-Sectional Study. F1000Research 2021, 10, 1242. [Google Scholar] [CrossRef]
- Alzayer, R.; Barakat, M.; Jirjees, F.; Alhamdan, A.; Aloraifej, S.; Cherri, S.; Mansour, S.; El Khatib, S.; Kharaba, Z.; Rahal, M.; et al. Knowledge and awareness of stroke and associated factors in the Saudi general population: A cross-sectional study. Front. Neurol. 2023, 14, 1225980. [Google Scholar] [CrossRef]
- Elshatarat, R.A.; Stotts, N.A.; Engler, M.; Froelicher, E.S. Knowledge and beliefs about smoking and goals for smoking cessation in hospitalized men with cardiovascular disease. Heart Lung 2013, 42, 126–132. [Google Scholar] [CrossRef]
- Dawood, O.T.; Rashan, M.A.; Hassali, M.A.; Saleem, F. Knowledge and perception about health risks of cigarette smoking among Iraqi smokers. J. Pharm. Bioallied Sci. 2016, 8, 146–151. [Google Scholar] [CrossRef]
- Bajandouh, W.M.; Alotaibi, T.N.; Alharbi, A.R.; Alzahrani, S.A.; Alghamdi, G.A.; Aleissi, A.H.; Rashed, A.; Shatla, M. Stroke Knowledge and Response Among the General Population in Saudi Arabia: A Population-Based Survey. Cureus 2024, 16, e65587. [Google Scholar] [CrossRef]
- Magnani, J.W.; Ning, H.; Wilkins, J.T.; Lloyd-Jones, D.M.; Allen, N.B. Educational Attainment and Lifetime Risk of Cardiovascular Disease. JAMA Cardiol. 2024, 9, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Kubota, Y.; Heiss, G.; MacLehose, R.F.; Roetker, N.S.; Folsom, A.R. Association of Educational Attainment With Lifetime Risk of Cardiovascular Disease: The Atherosclerosis Risk in Communities Study. JAMA Intern. Med. 2017, 177, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Sulo, G.; Nygård, O.; Vollset, S.E.; Igland, J.; Ebbing, M.; Sulo, E.; Egeland, G.M.; Tell, G.S. Higher education is associated with reduced risk of heart failure among patients with acute myocardial infarction: A nationwide analysis using data from the CVDNOR project. Eur. J. Prev. Cardiol. 2016, 23, 1743–1750. [Google Scholar] [CrossRef]
- Lee, H.Y.; Jin, S.W.; Henning-Smith, C.; Lee, J.; Lee, J. Role of Health Literacy in Health-Related Information-Seeking Behavior Online: Cross-sectional Study. J. Med. Internet Res. 2021, 23, e14088. [Google Scholar] [CrossRef]
- Appelros, P.; Stegmayr, B.; Terént, A. Sex differences in stroke epidemiology: A systematic review. Stroke 2009, 40, 1082–1090. [Google Scholar] [CrossRef]
- Appelros, P.; Åsberg, S. Sex differences in stroke. Handb. Clin. Neurol. 2020, 175, 299–312. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Characters | N (%) or | |
|---|---|---|
| Mean ± SD | ||
| Gender | ||
| Male | 904 | 87.9 |
| Female | 125 | 12.1 |
| Age group | ||
| 18–30 Year | 630 | 61.2 |
| 31–40 Year | 227 | 22.1 |
| 41–50 Year | 90 | 8.7 |
| >50 Year | 82 | 8 |
| Living Area | ||
| Rural | 52 | 5.1 |
| Urban | 977 | 94.9 |
| Marital Status | ||
| Married | 274 | 26.6 |
| Single | 755 | 73.4 |
| Regions | ||
| Western | 397 | 38.6 |
| Eastern | 348 | 33.8 |
| Central | 144 | 14 |
| Southern | 66 | 6.4 |
| Northern | 74 | 7.2 |
| Educational Status | ||
| School | 167 | 16.2 |
| University | 862 | 83.8 |
| Employment Status | ||
| Employed | 559 | 54.3 |
| Unemployed | 470 | 45.7 |
| Income Level | ||
| Less than 10,238 | 704 | 68.4 |
| More than 10,238 | 325 | 31.6 |
| Smoking Status | ||
| Current Smoker | 698 | 67.8 |
| Ex-smoker | 331 | 32.2 |
| Types of smoking | ||
| Cigarette | 349 | 33.9 |
| Shisha | 267 | 25.9 |
| Vape or E-cigarette | 413 | 40.1 |
| Pack Per Year (Cigarette) | 13.26 ± 17.96 | |
| Pack Per Year (Shisha) | 24.92 ± 70.90 | |
| Nicotine used in E-cigarette liquid | ||
| 0 mg | 27 | 6.5 |
| 2 to 18 mg | 63 | 15.3 |
| 20 to 30 mg | 121 | 29.3 |
| 30 to 40 mg | 86 | 20.8 |
| 40 to 50 mg | 116 | 28.1 |
| Bottle of e-cigarette consumption (used ≥20 mg in a week) | ||
| In one week | 65 | 15.7 |
| 2 to 3 weeks | 96 | 23.2 |
| 3 to 4 weeks | 129 | 31.2 |
| Longer than one month | 123 | 29.8 |
| High Nicotine dependence for E-cigarette | 36 | 9% |
| Variables | N (%) | |
|---|---|---|
| Identification of risk factors for stroke | ||
| Zero | 270 | 26.2 |
| One risk Factor | 55 | 5.3 |
| Two risk Factors | 189 | 18.4 |
| Three risk Factors | 95 | 9.2 |
| Four risk Factors | 139 | 13.5 |
| Five risk Factors | 78 | 7.6 |
| Six risk Factors | 57 | 5.5 |
| Seven risk Factors | 43 | 4.2 |
| Eight risk Factors | 35 | 3.4 |
| Nine risk Factors | 22 | 2.1 |
| Ten risk Factors | 46 | 4.5 |
| Identification of Stroke symptoms | ||
| Zero | 593 | 57.6 |
| One symptom | 36 | 3.5 |
| Two symptoms | 13 | 1.3 |
| Three symptoms | 61 | 5.9 |
| Four symptoms | 74 | 7.2 |
| Five symptoms | 60 | 5.8 |
| Six symptoms | 51 | 5 |
| Seven symptoms | 141 | 13.7 |
| Consequences Identified | ||
| Zero | 450 | 43.7 |
| One Problem | 241 | 23.4 |
| Two Problems | 167 | 16.2 |
| Three problems | 88 | 8.6 |
| Four Problems | 83 | 8.1 |
| Variables | OR (95% CI) | p-Value |
|---|---|---|
| Risk factor(s) identified (≥1) | ||
| Gender (male versus female *) | 1.34 (0.81–2.23) | 0.26 |
| Residence area (rural versus urban *) | 1.60 (0.85–3.01) | 0.15 |
| Region (Central Region versus Western Region *) | 2.42 (1.56–3.75) | 0.001 |
| Region (Eastern Region versus Western Region *) | 0.69 (0.47–1.03) | 0.07 |
| Region (Northern Region versus Western Region *) | 1.57 (0.89–2.77) | 0.12 |
| Region (Southern Region versus Western Region *) | 1.45 (0.78–2.69) | 0.25 |
| Educational level (school versus university *) | 0.92 (0.61–1.37) | 0.68 |
| Employment status (employed versus unemployed *) | 1.06 (0.75–1.49) | 0.74 |
| History of smoking (Current smoker versus Ex-smoker *) | 1.95 (1.38–2.75) | 0.001 |
| Type of Smoking (Cigarette versus E-cigarette *) | 1.40 (0.98–2.00) | 0.07 |
| Type of Smoking (Shisha versus E-cigarette *) | 1.16 (0.79–1.72) | 0.45 |
| Identified Stroke Symptoms (≥1) | ||
| Gender (male versus female *) | 2.88 (1.86–4.47) | 0.001 |
| Residence area (rural versus urban *) | 1.18 (0.63–2.20) | 0.61 |
| Region (Central Region versus Western Region *) | 0.71 (0.46–1.09) | 0.11 |
| Region (Eastern Region versus Western Region *) | 1.14 (0.81–1.61) | 0.45 |
| Region (Northern Region versus Western Region *) | 0.65 (0.38–1.11) | 0.11 |
| Region (Southern Region versus Western Region *) | 0.78 (0.44–1.39) | 0.41 |
| Educational level (school versus university *) | 0.53 (0.37–0.76) | 0.001 |
| Employment status (employed versus unemployed *) | 1.09 (0.80–1.48) | 0.59 |
| History of smoking (Current smoker versus Ex-smoker *) | 2.68 (2.00–3.59) | 0.001 |
| Type of Smoking (Cigarette versus E-cigarette *) | 0.99 (0.71–1.38) | 0.96 |
| Type of Smoking (Shisha versus E-cigarette *) | 0.93 (0.65–1.32) | 0.68 |
| Identified consequences (≥1) | ||
| Gender (male versus female *) | 0.76 (0.49–1.17) | 0.21 |
| Residence area (rural versus urban *) | 1.12 (0.60–2.09) | 0.72 |
| Region (Central Region versus Western Region *) | 3.16 (2.05–4.88) | 0.001 |
| Region (Eastern Region versus Western Region *) | 1.52 (1.08–2.14) | 0.02 |
| Region (Northern Region versus Western Region *) | 0.80 (0.45–1.41) | 0.43 |
| Region (Southern Region versus Western Region *) | 1.81 (1.01–3.25) | 0.05 |
| Educational level (school versus university *) | 0.64 (0.43–0.93) | 0.02 |
| Employment status (employed versus unemployed *) | 1.40 (1.03–1.91) | 0.03 |
| History of smoking (Current smoker versus Ex-smoker *) | 2.36 (1.73–3.21) | 0.001 |
| Type of Smoking (Cigarette versus E-cigarette *) | 2.01 (1.45–2.79) | 0.001 |
| Type of Smoking (Shisha versus E-cigarette *) | 0.63 (0.44–0.91) | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alqahtani, J.S.; Aldhahir, A.M.; Alqarni, A.A.; Alghamdi, S.M.; Oyelade, T.; Alzaidi, F.N.; Alamri, M.A.; Kheder, A.M.; Alsamdani, H.I.; AlAyadi, A.Y.; et al. Understanding of Stroke Risk Among Smokers in Saudi Arabia. Medicina 2025, 61, 1006. https://doi.org/10.3390/medicina61061006
Alqahtani JS, Aldhahir AM, Alqarni AA, Alghamdi SM, Oyelade T, Alzaidi FN, Alamri MA, Kheder AM, Alsamdani HI, AlAyadi AY, et al. Understanding of Stroke Risk Among Smokers in Saudi Arabia. Medicina. 2025; 61(6):1006. https://doi.org/10.3390/medicina61061006
Chicago/Turabian StyleAlqahtani, Jaber S., Abdulelah M. Aldhahir, Abdullah A. Alqarni, Saeed M. Alghamdi, Tope Oyelade, Fahad Nawar Alzaidi, Muath Abdulrahman Alamri, Ali Mohammad Kheder, Hussain Ibrahim Alsamdani, Ayadh Yahya AlAyadi, and et al. 2025. "Understanding of Stroke Risk Among Smokers in Saudi Arabia" Medicina 61, no. 6: 1006. https://doi.org/10.3390/medicina61061006
APA StyleAlqahtani, J. S., Aldhahir, A. M., Alqarni, A. A., Alghamdi, S. M., Oyelade, T., Alzaidi, F. N., Alamri, M. A., Kheder, A. M., Alsamdani, H. I., AlAyadi, A. Y., Siraj, R. A., Aldabayan, Y. S., & Al Rajeh, A. M. (2025). Understanding of Stroke Risk Among Smokers in Saudi Arabia. Medicina, 61(6), 1006. https://doi.org/10.3390/medicina61061006