


Genetic Patterns Related with the Development and Progression of Sarcopenia and Sarcopenic Obesity: A Systematic Review
 ,
,
Abstract

1. Introduction
2. Materials and Methods
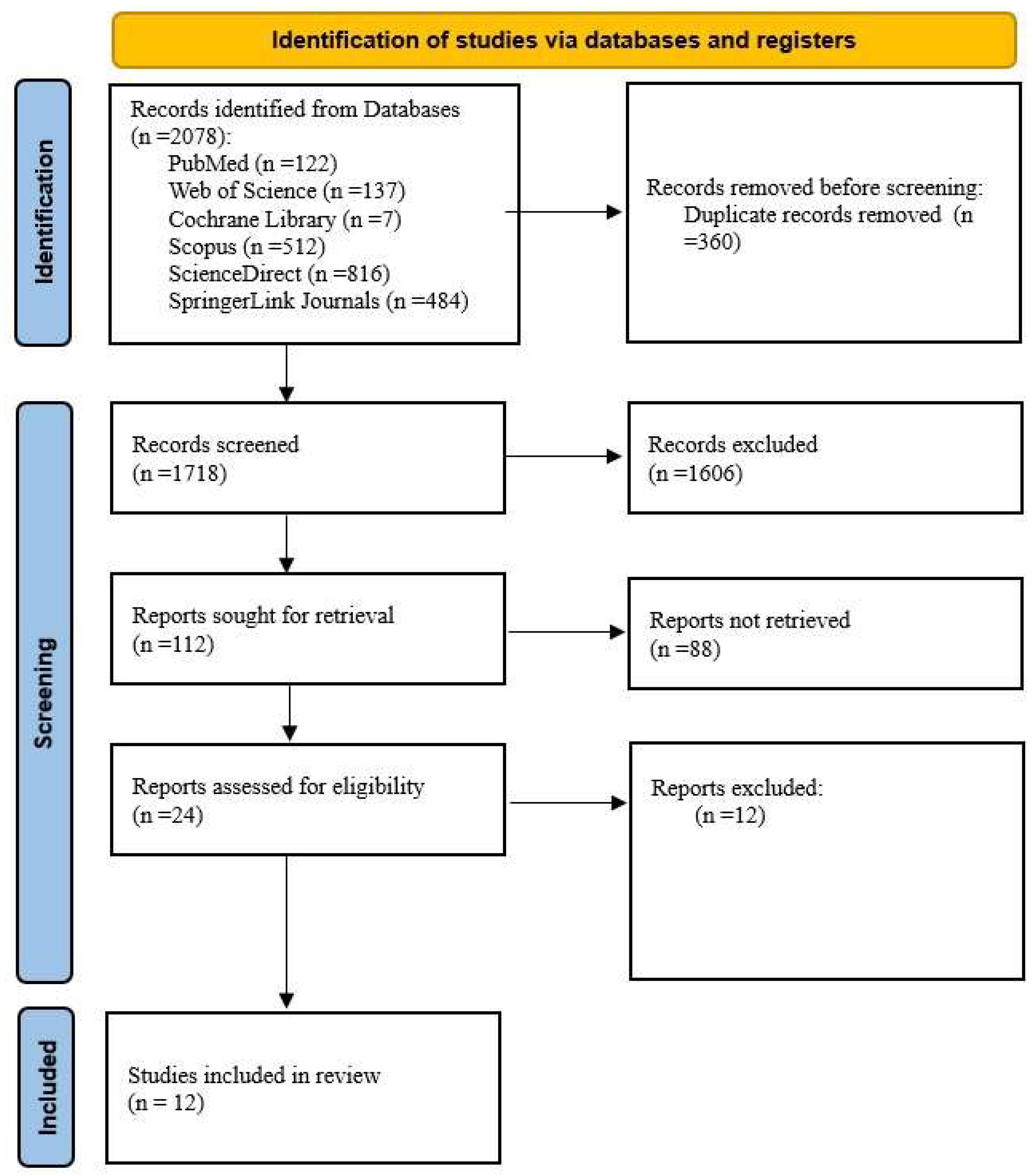
2.1. The Search Strategy
2.2. The Study Selection
- The Inclusion Criteria:
- -
- Original studies (randomized controlled trials, case–control studies, cohort studies, observational studies, trials) investigating SNPs associated with a predisposition to or the progression of sarcopenia and/or sarcopenic obesity;
- -
- The association of SNPs with muscle mass, muscle strength, muscle function, or body composition in the context of sarcopenia or sarcopenic obesity;
- -
- Studies conducted on adults, particularly older individuals, diagnosed with sarcopenia or sarcopenic obesity based on universally accepted criteria;
- -
- Studies published in English;
- -
- Studies published in the last 10 years.
- The Exclusion Criteria:
- -
- Systematic reviews, meta-analyses, books, book chapters, editorials, conference abstracts, and notes;
- -
- Studies not focused on SNPs associated with sarcopenia/sarcopenic obesity;
- -
- Studies analyzing environmental or lifestyle factors involved in the pathogenesis of sarcopenia and sarcopenic obesity without investigating the genetic component;
- -
- Studies examining the genetic context between sarcopenia/sarcopenic obesity and other pathologies;
- -
- Studies that did not provide a clear analysis of the associations between SNPs and muscle mass, muscle strength, or body composition;
- -
- Studies conducted on children, adolescents, or individuals with genetic disorders affecting muscle mass;
- -
- Animal studies or preclinical studies without clinical validation;
- -
- Studies published in languages other than English;
- -
- Studies published before 2015, ensuring the relevance and up-to-date nature of the data.
2.3. Data Extraction
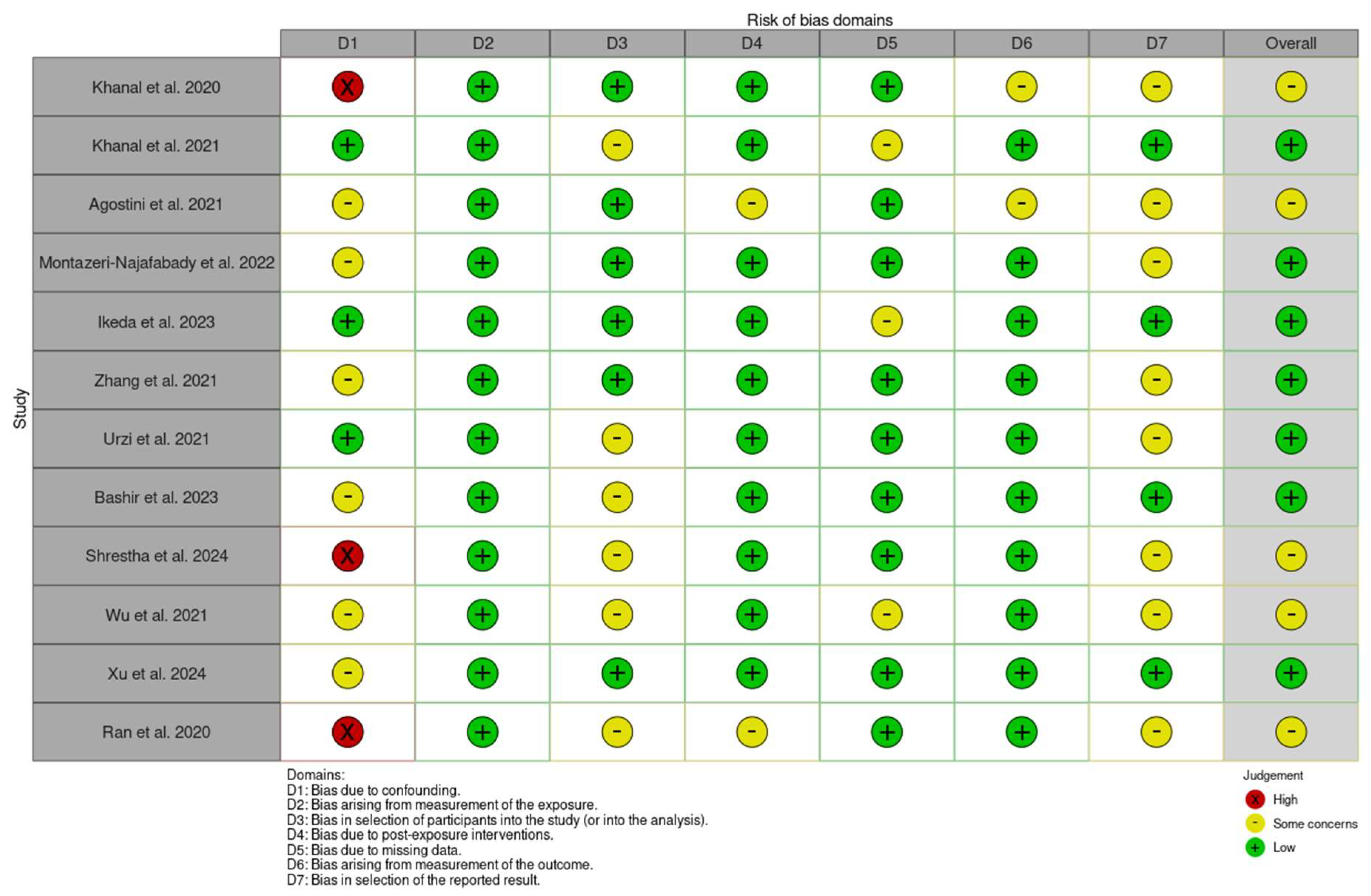
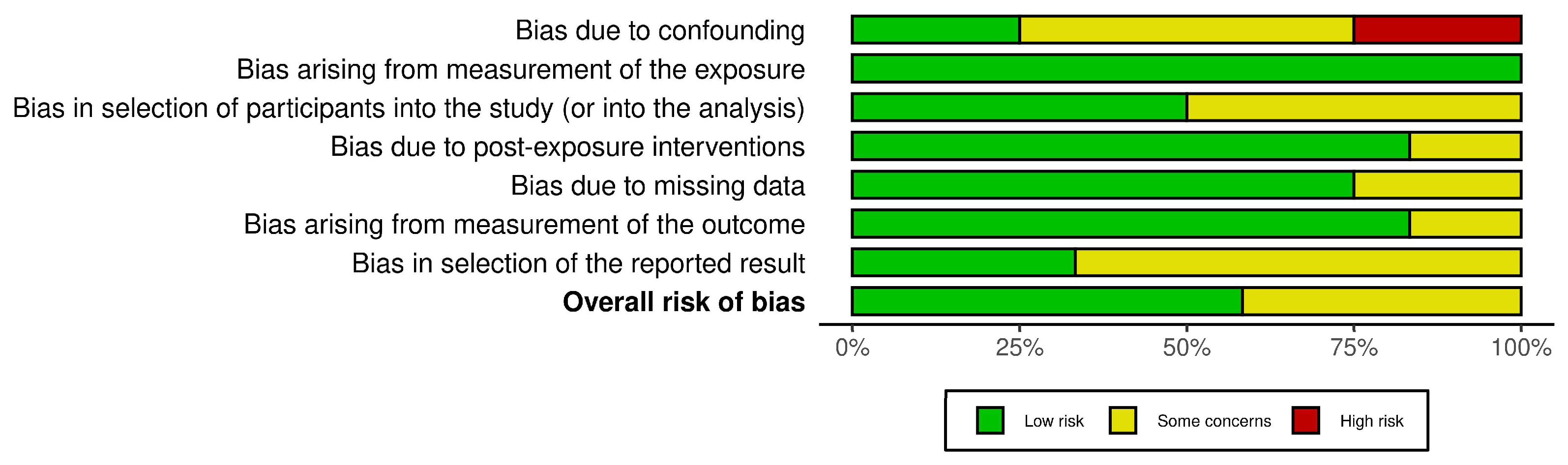
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. The Included Studies
3.2. The PICO Question
- -
- P (Population): Individuals affected by sarcopenia or sarcopenic obesity, specifically adults, with a focus on the elderly;
- -
- I (Intervention): The identification of SNPs associated with the development of sarcopenia and/or sarcopenic obesity;
- -
- C (Comparison): Healthy control groups without sarcopenia/sarcopenic obesity or individuals with different SNPs to assess variations and differences;
- -
- O (Outcome): The association between specific SNPs and the predisposition to or the progression of sarcopenia or sarcopenic obesity.
3.3. Risk of Bias
3.4. Detailed Study Descriptions of Identified SNPs
4. Discussion
4.1. The Functional Pathways of the Specific SNPs
4.1.1. Muscle Structure, Function, and Atrophy
4.1.2. Neurotransmission
4.1.3. Lipid Metabolism and Adipogenesis
4.1.4. Insulin Signaling and Glucose Metabolism
4.1.5. Oxidative Stress and Inflammation
4.1.6. Hormonal Regulation
4.1.7. The Cell Cycle and Regeneration
4.2. The Identification of Gaps in the Current Knowledge and Future Research Directions
4.3. The Strengths of This Study
4.4. Limitations of This Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
List of Abbreviations
| ACE | Angiotensin-Converting Enzyme |
| ACER2 | Alkaline ceramidase 2 |
| ACTN3 | Alpha actinin cardiac muscle 3 |
| ACVR1B | Activin receptor type-1B |
| ACVR2B | Activin receptor type-2B |
| ADIPOQ | Adiponectin |
| ALM/W | Appendicular lean mass adjusted for weight |
| ATXN8OS | Ataxin-8 opposite strand |
| AWGS | Asian Working Group for Sarcopenia |
| BDKRB2 | Bradykinin Receptor B2 |
| BIA | Bioelectrical impedance analysis |
| Del/Ins | Deletion/Insertion |
| DNA | Deoxyribonucleic acid |
| DXA | Dual-energy X-ray absorptiometry |
| EASO | European Association for the Study of Obesity |
| ESPEN | European Society for Clinical Nutrition and Metabolism |
| ESR1 | Estrogen receptor 1 |
| EWAS | Epigenome-wide association study |
| EWGSOP | European Working Group on Sarcopenia in Older People |
| FM% | Fat mass percentage |
| FTO | Fat mass and obesity-associated gene |
| FZR1 | Fizzy-related protein homolog |
| GM2A | Ganglioside activator |
| GS | Gait speed |
| GWAS | Genome-wide association study |
| HGS | Handgrip strength |
| IRS1 | Insulin receptor substrate 1 |
| IZUMO3 | IZUMO family member 3 |
| KASP | Kompetitive Allele-Specific PCR |
| LYPLAL1-AS1 | Lysophospholipase Like 1-Antisense RNA 1 |
| MiRNA | Microribonucleic acid |
| MTHFR | Methylenetetrahydrofolate reductase |
| 6MWD | Six-Minute Walk Distance |
| NIH | National Institutes of Health |
| NOS3 | Endothelial nitric oxide synthase 1 |
| NRF2 | Nuclear factor erythroid 2-related factor 2 |
| OR4A9P | Olfactory receptor, family 4, subfamily A, member 9 pseudogene |
| OR5D18 | Olfactory receptor family 5 subfamily D member 18 |
| OSBPL3 | Oxysterol binding protein-like |
| PCR | Polymerase chain reaction |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| qPCR | Quantitative PCR |
| RFLP | Restriction fragment length polymorphism |
| SGS | Sarcopenia genetic risk score |
| SMI | Skeletal muscle mass index |
| %SMM | %Skeletal muscle mass |
| SNAP-25 | Synaptosomal-associated protein of 25 kDa |
| SNPs | Single-nucleotide polymorphisms |
| SO | Sarcopenic obesity |
| SOAT2 | Sterol O-acyltransferase |
| 2SPPB | Short Physical Performance Battery |
| TMEM14A | Transmembrane Protein 14A |
| TP53 | Tumor suppressor protein 53 |
| TRHR | Thyrotropin-releasing hormone receptor |
| VFA | Visceral fat area |
| WES | Whole-exome sequencing |
| WLBM | Whole lean body mass |
References
- Urzi, F.; Pokorny, B.; Buzan, E. Pilot Study on Genetic Associations with Age-Related Sarcopenia. Front. Genet. 2021, 11, 615238. [Google Scholar] [CrossRef]
- Agostini, S.; Mancuso, R.; Costa, A.S.; Guerini, F.R.; Trecate, F.; Miglioli, R.; Menna, E.; Arosio, B.; Clerici, M. Sarcopenia associates with SNAP-25 SNPs and a miRNAs profile which is modulated by structured rehabilitation treatment. J. Transl. Med. 2021, 19, 315. [Google Scholar] [CrossRef]
- Villa, O.; Stuhr, N.L.; Yen, C.-A.; Crimmins, E.M.; Arpawong, T.E.; Curran, S.P. Genetic variation in ALDH4A1 is associated with muscle health over the lifespan and across species. eLife 2022, 11, e74308. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Walston, J.D. Sarcopenia in older adults. Curr. Opin. Rheumatol. 2012, 24, 623–627. [Google Scholar] [CrossRef]
- Stanciu, L.-E.; Iliescu, M.-G.; Oprea, C.; Ionescu, E.-V.; Petcu, A.; Ciortea, V.M.; Petcu, L.C.; Apostol, S.; Nedelcu, A.-D.; Motoașcă, I.; et al. The Impact of Complex Rehabilitation Treatment on Sarcopenia—Pathology with an Endocrine Morphological Substrate and Musculoskeletal Implications. Medicina 2023, 59, 1238. [Google Scholar] [CrossRef]
- Wei, S.; Nguyen, T.T.; Zhang, Y.; Ryu, D.; Gariani, K. Sarcopenic obesity: Epidemiology, pathophysiology, cardiovascular disease, mortality, and management. Front. Endocrinol. 2023, 14, 1185221. [Google Scholar] [CrossRef]
- Donini, L.M.; Busetto, L.; Bischoff, S.C.; Cederholm, T.; Ballesteros-Pomar, M.D.; Batsis, J.A.; Bauer, J.M.; Boirie, Y.; Cruz-Jentoft, A.J.; Dicker, D.; et al. Definition and Diagnostic Criteria for Sarcopenic Obesity: ESPEN and EASO Consensus Statement. Obes. Facts 2022, 15, 321–335. [Google Scholar] [CrossRef]
- Prado, C.M.; Batsis, J.A.; Donini, L.M.; Gonzalez, M.C.; Siervo, M. Sarcopenic obesity in older adults: A clinical overview. Nat. Rev. Endocrinol. 2024, 20, 261–277. [Google Scholar] [CrossRef]
- Kalinkovich, A.; Livshits, G. Sarcopenic obesity or obese sarcopenia: A cross talk between age-associated adipose tissue and skeletal muscle inflammation as a main mechanism of the pathogenesis. Ageing Res. Rev. 2017, 35, 200–221. [Google Scholar] [CrossRef]
- Batsis, J.A.; Villareal, D.T. Sarcopenic obesity in older adults: Aetiology, epidemiology and treatment strategies. Nat. Rev. Endocrinol. 2018, 14, 513–537. [Google Scholar] [CrossRef] [PubMed]
- Aslam, M.A.; Ma, E.B.; Huh, J.Y. Pathophysiology of sarcopenia: Genetic factors and their interplay with environmental factors. Metabolism 2023, 149, 155711. [Google Scholar] [CrossRef]
- da Silva, J.R.D.; Freire, I.V.; Ribeiro, Í.J.; Dos Santos, C.S.; Casotti, C.A.; Dos Santos, D.B.; Barbosa, A.A.L.; Pereira, R. Improving the comprehension of sarcopenic state determinants: An multivariate approach involving hormonal, nutritional, lifestyle and genetic variables. Mech. Ageing Dev. 2018, 173, 21–28. [Google Scholar] [CrossRef]
- Semenova, E.A.; Pranckevičienė, E.; Bondareva, E.A.; Gabdrakhmanova, L.J.; Ahmetov, I.I. Identification and Characterization of Genomic Predictors of Sarcopenia and Sarcopenic Obesity Using UK Biobank Data. Nutrients 2023, 15, 758. [Google Scholar] [CrossRef]
- Wilkinson, D.; Piasecki, M.; Atherton, P. The age-related loss of skeletal muscle mass and function: Measurement and physiology of muscle fibre atrophy and muscle fibre loss in humans. Ageing Res. Rev. 2018, 47, 123–132. [Google Scholar] [CrossRef]
- Carmelli, D.; Reed, T. Stability and change in genetic and environmental influences on hand-grip strength in older male twins. J. Appl. Physiol. 2000, 89, 1879–1883. [Google Scholar] [CrossRef]
- Jin, H.; Yoo, H.J.; Kim, Y.A.; Lee, J.H.; Lee, Y.; Kwon, S.-H.; Seo, Y.J.; Lee, S.H.; Koh, J.-M.; Ji, Y.; et al. Unveiling genetic variants for age-related sarcopenia by conducting a genome-wide association study on Korean cohorts. Sci. Rep. 2022, 12, 3501. [Google Scholar] [CrossRef]
- Bilski, J.; Pierzchalski, P.; Szczepanik, M.; Bonior, J.; Zoladz, J.A. Multifactorial Mechanism of Sarcopenia and Sarcopenic Obesity. Role of Physical Exercise, Microbiota and Myokines. Cells 2022, 11, 160. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sohani, Z.N.; Meyre, D.; de Souza, R.J.; Joseph, P.G.; Gandhi, M.; Dennis, B.B.; Norman, G.; Anand, S.S. Assessing the quality of published genetic association studies in meta-analyses: The quality of genetic studies (Q-Genie) tool. BMC Genet. 2015, 16, 50. [Google Scholar] [CrossRef]
- Sohani, Z.N.; Sarma, S.; Alyass, A.; de Souza, R.J.; Robiou-du-Pont, S.; Li, A.; Mayhew, A.; Yazdi, F.; Reddon, H.; Lamri, A.; et al. Empirical evaluation of the Q-Genie tool: A protocol for assessment of effectiveness. BMJ Open 2016, 6, e010403. [Google Scholar] [CrossRef]
- Khanal, P.; He, L.; Stebbings, G.; Onambele-Pearson, G.L.; Degens, H.; Williams, A.; Thomis, M.; Morse, C.I. Prevalence and association of single nucleotide polymorphisms with sarcopenia in older women depends on definition. Sci. Rep. 2020, 10, 2913. [Google Scholar] [CrossRef]
- Khanal, P.; Williams, A.; He, L.; Stebbings, G.; Onambele-Pearson, G.; Thomis, M.; Degens, H.; Morse, C. Sarcopenia, Obesity, and Sarcopenic Obesity: Relationship with Skeletal Muscle Phenotypes and Single Nucleotide Polymorphisms. J. Clin. Med. 2021, 10, 4933. [Google Scholar] [CrossRef]
- Montazeri-Najafabady, N.; Dabbaghmanesh, M.H.; Nasimi, N.; Sohrabi, Z.; Estedlal, A.; Asmarian, N. Importance of TP53 codon 72 and intron 3 duplication 16 bp polymorphisms and their haplotypes in susceptibility to sarcopenia in Iranian older adults. BMC Geriatr. 2022, 22, 103. [Google Scholar] [CrossRef]
- Ikeda, Y.; Kawamura, R.; Takata, Y.; Tabara, Y.; Maruyama, K.; Takakado, M.; Hadate, T.; Ohashi, J.; Saito, I.; Ogawa, Y.; et al. Resistin G-A haplotype at SNP-420/-358 is associated with the latent sarcopenic obesity index in the toon genome study. J. Diabetes Investig. 2023, 14, 686–694. [Google Scholar] [CrossRef]
- Zhang, X.; Ye, L.; Li, X.; Chen, Y.; Jiang, Y.; Li, W.; Wen, Y. The association between sarcopenia susceptibility and polymorphisms of FTO, ACVR2B, and IRS1 in Tibetans. Mol. Genet. Genom. Med. 2021, 9, e1747. [Google Scholar] [CrossRef]
- Bashir, T.; Achison, M.; Adamson, S.; Akpan, A.; Aspray, T.; Avenell, A.; Band, M.M.; Burton, L.A.; Cvoro, V.; Donnan, P.T.; et al. Activin type I receptor polymorphisms and body composition in older individuals with sarcopenia-Analyses from the LACE randomised controlled trial. PLoS ONE 2023, 18, e0294330. [Google Scholar] [CrossRef]
- LACE Study Group; Achison, M.; Adamson, S.; Akpan, A.; Aspray, T.; Avenell, A.; Band, M.M.; Bashir, T.; Burton, L.A.; Cvoro, V.; et al. Effect of perindopril or leucine on physical performance in older people with sarcopenia: The LACE randomized controlled trial. J. Cachex-Sarcopenia Muscle 2022, 13, 858–871. [Google Scholar] [CrossRef]
- Shrestha, A.; Bashir, T.; Achison, M.; Adamson, S.; Akpan, A.; Aspray, T.; Avenell, A.; Band, M.M.; Burton, L.A.; Cvoro, V.; et al. Association of bradykinin receptor 2 (BDKRB2) variants with physical performance and muscle mass: Findings from the LACE sarcopenia trial. PLoS ONE 2024, 19, e0307268. [Google Scholar] [CrossRef]
- Wu, S.; Chen, W. A Genome-Wide Association Study Identifies Novel Risk Loci for Sarcopenia in a Taiwanese Population. J. Inflamm. Res. 2021, 14, 5969–5980. [Google Scholar] [CrossRef]
- Xu, Q.; Zhao, Q.-G.; Ma, X.-L.; Yan, S.-S.; Han, B.-X.; Song, Z.-T.; Bu, F.; Li, K.; Zhang, L.; Pei, Y.-F. Exome-Wide Sequencing Study Identified Genetic Variants Associated With Sarcopenic Obesity. J. Gerontol. A Biol. Sci. Med. Sci. 2024, 79, glae025. [Google Scholar] [CrossRef] [PubMed]
- Ran, S.; He, X.; Jiang, Z.-X.; Liu, Y.; Zhang, Y.-X.; Zhang, L.; Gu, G.-S.; Pei, Y.; Liu, B.-L.; Tian, Q.; et al. Whole-exome sequencing and genome-wide association studies identify novel sarcopenia risk genes in Han Chinese. Mol. Genet. Genom. Med. 2020, 8, e1267. [Google Scholar] [CrossRef]
- Pratt, J.; Boreham, C.; Ennis, S.; Ryan, A.W.; De Vito, G. Genetic Associations with Aging Muscle: A Systematic Review. Cells 2019, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Morgan, R.L.; Rooney, A.A.; Taylor, K.W.; Thayer, K.A.; Silva, R.A.; Lemeris, C.; Akl, E.A.; Bateson, T.F.; Berkman, N.D.; et al. A tool to assess risk of bias in non-randomized follow-up studies of exposure effects (ROBINS-E). Environ. Int. 2024, 186, 108602. [Google Scholar] [CrossRef]
- Beaudart, C.; McCloskey, E.; Bruyère, O.; Cesari, M.; Rolland, Y.; Rizzoli, R.; Araujo de Carvalho, I.; Amuthavalli Thiyagarajan, J.; Bautmans, I.; Bertière, M.C.; et al. Sarcopenia in daily practice: Assessment and man-agement. BMC Geriatr. 2016, 16, 170. [Google Scholar] [CrossRef]
- Cawthon, P.M.; Visser, M.; Arai, H.; Ávila-Funes, J.A.; Barazzoni, R.; Bhasin, S.; Binder, E.; Bruyère, O.; Cederholm, T.; Chen, L.-K.; et al. Defining terms commonly used in sarcopenia research: A glossary proposed by the Global Leadership in Sarcopenia (GLIS) Steering Committee. Eur. Geriatr. Med. 2022, 13, 1239–1244. [Google Scholar] [CrossRef]
- Brinkmalm, A.; Brinkmalm, G.; Honer, W.G.; Frölich, L.; Hausner, L.; Minthon, L.; Hansson, O.; Wallin, A.; Zetterberg, H.; Blennow, K.; et al. SNAP-25 is a promising novel cerebrospinal fluid biomarker for synapse degeneration in Alzheimer’s disease. Mol. Neurodegener. 2014, 9, 53. [Google Scholar] [CrossRef] [PubMed]
- Al-Daghri, N.M.; Costa, A.S.; Alokail, M.S.; Zanzottera, M.; Alenad, A.M.; Mohammed, A.K.; Clerici, M.; Guerini, F.R. Synaptosomal Protein of 25 kDa (Snap25) Polymorphisms Associated with Glycemic Parameters in Type 2 Diabetes Patients. J. Diabetes Res. 2016, 2016, 8943092. [Google Scholar] [CrossRef]
- Tam, V.; Patel, N.; Turcotte, M.; Bossé, Y.; Paré, G.; Meyre, D. Benefits and limitations of genome-wide association studies. Nat. Rev. Genet. 2019, 20, 467–484. [Google Scholar] [CrossRef]
- Yoon, K.J.; Yi, Y.; Do, J.G.; Kim, H.-L.; Lee, Y.-T.; Kim, H.-N. Variants in NEB and RIF1 genes on chr2q23 are associated with skeletal muscle index in Koreans: Genome-wide association study. Sci. Rep. 2021, 11, 2333. [Google Scholar] [CrossRef]
- Wei, S.; Tao, J.; Xu, J.; Chen, X.; Wang, Z.; Zhang, N.; Zuo, L.; Jia, Z.; Chen, H.; Sun, H.; et al. Ten Years of EWAS. Adv. Sci. 2021, 8, e2100727. [Google Scholar] [CrossRef]
- Iliescu, M.G.; Stanciu, L.-E.; Uzun, A.-B.; Cristea, A.-E.; Motoască, I.; Irsay, L.; Iliescu, D.M.; Vari, T.; Ciubean, A.D.; Caraban, B.M.; et al. Assessment of Integrative Therapeutic Methods for Improving the Quality of Life and Functioning in Cancer Patients—A Systematic Review. J. Clin. Med. 2024, 13, 1190. [Google Scholar] [CrossRef]
- Nasui, B.A.; Talaba, P.; Nasui, G.A.; Sirbu, D.M.; Borda, I.M.; Pop, A.L.; Ciortea, V.M.; Irsay, L.; Purcar-Popescu, A.I.; Cinteza, D.; et al. The Influence of Diet and Physical Activity on Oxidative Stress in Romanian Females with Osteoarthritis. Nutrients 2022, 14, 4159. [Google Scholar] [CrossRef]
- Pan, J.T.; See, K.C. Criteria for stopping high-flow nasal oxygen for acute hypoxemic respiratory failure: A systematic review of randomized controlled trials. Anesthesiol. Perioper. Sci. 2024, 2, 23. [Google Scholar] [CrossRef]
- Xu, Y.; Han, Y.; Zhuang, H.; Fei, F.; Zheng, T.; Yu, H. Effect of ultrasound-guided recruitment maneuver on atelectasis: A systematic review and meta-analysis of randomized controlled trials. Anesthesiol. Perioper. Sci. 2024, 2, 16. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Databases | Database Search Filters | Number of Results |
|---|---|---|
| PubMed, National Institutes of Health (NIH) | Publication years: 2015-present Language: English Species: humans Article types: all | 122 results |
| Web of Science | Publication years: 2015-present Language: English Article types: all | 137 results |
| Cochrane Library | Publication years: 2015-present Language: English | 7 results |
| Scopus | Publication years: 2015-present Language: English Species: humans Article types: articles, reviews | 512 results |
| ScienceDirect | Publication years: 2015-present Language: English Article types: research articles, case reports, reviews, mini-reviews | 816 results |
| SpringerLink Journals | Publication years: 2015-present Language: English Article types: articles, review articles, research articles | 484 results |
| TOTAL | 2078 results |
| Author’s Name and Year of Publication | Country | Pathology Studied | Study Design | Sample Size | Number of SNPs Identified | References |
|---|---|---|---|---|---|---|
| Khanal et al. [22] 2020 | United Kingdom | Sarcopenia | Cross-sectional study | 307 Caucasian female patients | 4 SNPs | 92 |
| Khanal et al. [23] 2021 | United Kingdom | Sarcopenia Sarcopenic Obesity and Obesity | Cross-sectional study | 307 Caucasian female patients | 3 SNPs | 97 |
| Agostini et al. [2] 2021 | Italy | Sarcopenia | Cross-sectional study | 358 Caucasian patients (177 sarcopenic patients and 181 controls) | 1 SNP | 55 |
| Montazeri-Najafabady et al. [24] 2022 | Iran | Sarcopenia | Cross-sectional study | 254 patients (65 sarcopenic patients and 189 controls) | 2 SNPs | 45 |
| Ikeda et al. [25] 2023 | Japan | Latent Sarcopenic Obesity | Cross-sectional study | 567 participants | 2 SNPs | 36 |
| Zhang et al. [26] 2021 | China | Sarcopenia | Cross-sectional study | 160 participants (all sarcopenic) | 4 SNPs | 50 |
| Urzi et al. [1] 2021 | Slovenia | Sarcopenia | Cross-sectional study | 190 participants (sarcopenic group: 45 participants; control group: 145 participants) | 3 SNPs | 75 |
| Bashir et al. [27] 2023 | United Kingdom | Sarcopenia | Post hoc sub-study of a randomized controlled trial [28] | 110 Caucasian patients (all sarcopenic) | 2 SNPs | 47 |
| Shrestha et al. [29] 2024 | United Kingdom | Sarcopenia | Post hoc sub-study of a randomized controlled trial [28] | 136 Caucasian patients (all sarcopenic) | 2 SNPs | 31 |
| Wu et al. [30] 2021 | China | Sarcopenia | Genome-wide association study (GWAS) | 96 participants | 8 SNPs were strongly associated | 52 |
| Xu et al. [31] 2024 | China | Sarcopenic Obesity | Exome-wide association study (EWAS) | 282,164 participants (6890 with sarcopenic obesity, 275,274 controls) | 14 SNPs | 50 |
| Ran et al. [32] 2020 | China | Sarcopenia | Whole-exome sequencing (WES) and genome-wide association study (GWAS) | 101 (Chinese Han), Replication: 217,822 (UK Biobank) | 4 significant SNPs | 39 |
| Studies | Items | Total Score | Quality Classification | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |||
| Khanal et al. [22] | 6 | 5 | 5 | 6 | 7 | 4 | 4 | 6 | 5 | 4 | 5 | 57/77 | Good |
| Khanal et al. [23] | 6 | 6 | 6 | 7 | 5 | 4 | 4 | 6 | 5 | 4 | 6 | 59/77 | Good |
| Agostini et al. [2] | 7 | 6 | 6 | 7 | 6 | 5 | 6 | 7 | 6 | 6 | 7 | 69/77 | Good |
| Montazeri-Najafabady et al. [24] | 6 | 5 | 5 | 6 | 4 | 5 | 4 | 5 | 4 | 4 | 6 | 54/77 | Good |
| Ikeda et al. [25] | 6 | 6 | 6 | 7 | 4 | 5 | 5 | 6 | 7 | 5 | 6 | 63/77 | Good |
| Zhang et al. [26] | 6 | 6 | 6 | 7 | 4 | 4 | 4 | 5 | 5 | 5 | 6 | 58/77 | Good |
| Urzi et al. [1] | 6 | 6 | 5 | 6 | 5 | 6 | 5 | 6 | 5 | 5 | 6 | 61/77 | Good |
| Bashir et al. [27] | 7 | 6 | 5 | 6 | 5 | 5 | 4 | 5 | 6 | 6 | 6 | 61/77 | Good |
| Shrestha et al. [29] | 6 | 7 | 4 | 5 | 4 | 5 | 4 | 4 | 4 | 5 | 5 | 53/77 | Good |
| Wu et al. [30] | 7 | 6 | 5 | 7 | 7 | 6 | 3 | 5 | 7 | 5 | 7 | 65/77 | Good |
| Xu et al. [31] | 7 | 6 | 6 | 6 | 7 | 6 | 7 | 6 | 7 | 6 | 7 | 71/77 | Good |
| Ran et al. [32] | 7 | 6 | 7 | 7 | 6 | 6 | 7 | 6 | 7 | 6 | 7 | 72/77 | Good |
| Author’s Name | Pathology Studied | SNPs Identified | Mentions |
|---|---|---|---|
| Khanal et al. [22] | Sarcopenia | FTO rs9939609, ESR1 rs4870044, NOS3 rs1799983, TRHR rs7832552 | -SNPs identified vary depending on the diagnostic criteria for sarcopenia; -Exclusive focus on female participants. |
| Khanal et al. [23] | Sarcopenia Sarcopenic obesity Obesity | ACTN3rs1815739, MTHFR rs1801131, MTHFR rs1537516 | -SNPs identified were only significantly associated with sarcopenic obesity; -Groups based on sarcopenia and obesity status were not equally distributed; -Exclusive focus on female participants. |
| Agostini et al. [2] | Sarcopenia | SNAP-25 rs363050 | -The SNP identified is associated with sarcopenia, but the assessment was based on physical performance and muscle strength, while muscle mass was not evaluated using imaging methods, which are considered the gold standard. |
| Montazeri-Najafabady et al. [24] | Sarcopenia | TP53 exon 4 Arg72pro rs1042522, Intron 3 16-bp Del/Ins rs17878362 | -TP53 codon 72 influences the risk of sarcopenia; -rs17878362 (16-bp Del/Ins) is technically a structural variation (Indel) rather than a traditional SNP, but it is considered a genetic polymorphism that affects gene function and has not been directly associated with sarcopenia. |
| Ikeda et al. [25] | Latent sarcopenic obesity | SNP-420 rs1862513, SNP-358 rs3219175 | -SNPs identified are associated with an increased risk of latent sarcopenic obesity; -The definition of latent sarcopenic obesity requires further validation. |
| Zhang et al. [26] | Sarcopenia | FTO rs9939609, FTO rs9936385, ACVR2B rs2276541, IRS1 rs294365 | -FTO rs9939609 and rs9936385 were significantly associated with lower limb skeletal muscle mass and sarcopenia, particularly in Tibetan women; -ACVR2B rs2276541 and IRS1 rs2943656 showed no significant association with sarcopenia. |
| Urzi et al. [1] | Sarcopenia | MTHFR rs1801131, ACTN3 rs1815739, NRF2 rs12594956 | -The SNPs identified were significantly associated with sarcopenia risk. |
| Bashir et al. [27] | Sarcopenia | ACVR1B rs10783486, ACVR1B rs2854464 | -The SNPs were linked to height and limb fat mass, rather than muscle mass or strength, in older men with sarcopenia. |
| Shrestha et al. [29] | Sarcopenia | BDKRB2 rs1799722, BDKRB2 rs5810761 | -BDKRB2 polymorphisms are associated with physical performance and muscle mass. |
| Wu et al. [30] | Sarcopenia | OSBPL3 rs10282247, ACER2 rs7022373, GM2A rs60274968, TMEM14A rs6905523, IZUMO3 rs57247929, OR5D18 rs11231180, OR4A9P rs118154365, ATXN8OS rs9572533 | -Notably, OSBPL3 rs10282247 (influencing cholesterol metabolism) and ACER2 rs7022373 (involved in cellular apoptosis) were identified as key genetic markers. |
| Xu et al. [31] | Sarcopenic obesity | LYPLAL1-AS1 rs1417066, LYPLAL1-AS1 rs11205303, LYPLAL1-AS1 rs12138590, LYPLAL1-AS1 rs13374518, LYPLAL1-AS1 rs147871, LYPLAL1-AS1 rs188491278, LYPLAL1-AS1 rs34360, LYPLAL1-AS1 rs34594323, LYPLAL1-AS1 rs35706747, LYPLAL1-AS1 rs3736533, LYPLAL1-AS1 rs4980745, LYPLAL1-AS1 rs55687493, LYPLAL1-AS1 rs6670062, LYPLAL1-AS1 rs76293177 | -The lead variant, rs1417066, in the LYPLAL1-AS1 gene was the most significant genetic marker for SO. |
| Ran et al. [32] | Sarcopenia | FZR1 rs740681, SOAT2 rs2272303, SOAT2 rs11170413, SOAT2 rs2272302 | -Additionally, FZR1 plays a key role in cell cycle regulation and muscle differentiation, while SOAT2 is involved in cholesterol metabolism and obesity. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nedelcu, A.-D.; Uzun, A.-B.; Ciortea, V.-M.; Irsay, L.; Stanciu, L.-E.; Iliescu, D.M.; Popa, F.L.; Iliescu, M.-G. Genetic Patterns Related with the Development and Progression of Sarcopenia and Sarcopenic Obesity: A Systematic Review. Medicina 2025, 61, 866. https://doi.org/10.3390/medicina61050866
Nedelcu A-D, Uzun A-B, Ciortea V-M, Irsay L, Stanciu L-E, Iliescu DM, Popa FL, Iliescu M-G. Genetic Patterns Related with the Development and Progression of Sarcopenia and Sarcopenic Obesity: A Systematic Review. Medicina. 2025; 61(5):866. https://doi.org/10.3390/medicina61050866
Chicago/Turabian StyleNedelcu, Andreea-Dalila, Andreea-Bianca Uzun, Viorela-Mihaela Ciortea, Laszlo Irsay, Liliana-Elena Stanciu, Dan Marcel Iliescu, Florina Ligia Popa, and Mădălina-Gabriela Iliescu. 2025. "Genetic Patterns Related with the Development and Progression of Sarcopenia and Sarcopenic Obesity: A Systematic Review" Medicina 61, no. 5: 866. https://doi.org/10.3390/medicina61050866
APA StyleNedelcu, A.-D., Uzun, A.-B., Ciortea, V.-M., Irsay, L., Stanciu, L.-E., Iliescu, D. M., Popa, F. L., & Iliescu, M.-G. (2025). Genetic Patterns Related with the Development and Progression of Sarcopenia and Sarcopenic Obesity: A Systematic Review. Medicina, 61(5), 866. https://doi.org/10.3390/medicina61050866