
Baricitinib Mitigates Methotrexate-Induced Liver Fibrosis Model via YAP Pathway

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Experimental Design
2.3. Biochemical Analysis of ALT and CK-18 Levels in Plasma
2.4. Lipid Peroxidation Analysis of Plasma
2.5. Biochemical Assessment of TGF-Beta and YAP1 in Liver Tissue
2.6. Histological Analysis
2.7. Statistical Analysis
3. Results
3.1. Effect of Baricitinib on Biochemical Parameters
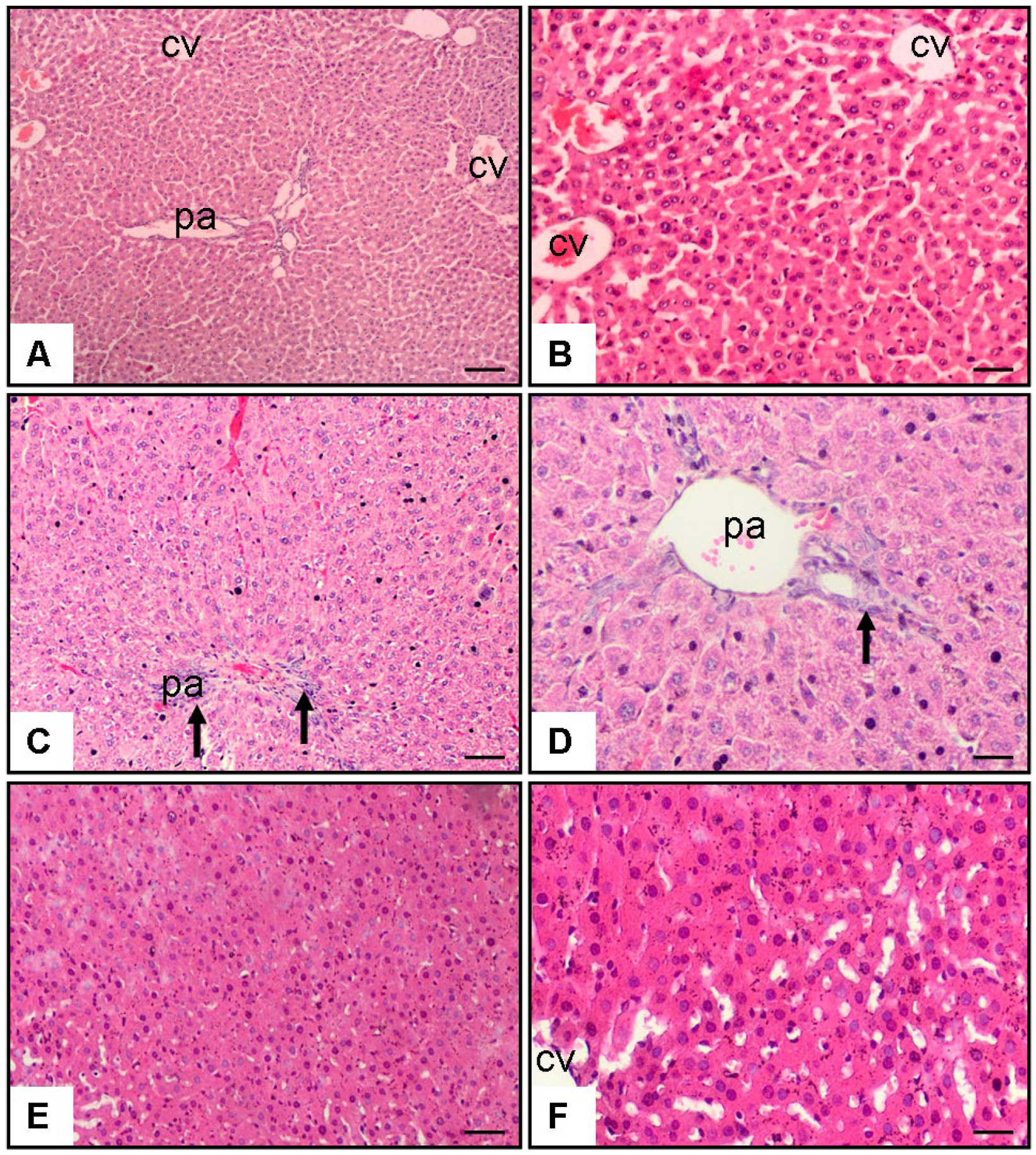
3.2. Effect of Baricitinib on Histopathological Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boyer-Diaz, Z.; Aristu-Zabalza, P.; Andrés-Rozas, M.; Robert, C.; Ortega-Ribera, M.; Fernández-Iglesias, A.; Broqua, P.; Junien, J.L.; Wettstein, G.; Bosch, J.; et al. Pan-PPAR agonist lanifibranor improves portal hypertension and hepatic fibrosis in experimental advanced chronic liver disease. J. Hepatol. 2021, 74, 1188–1199. [Google Scholar] [CrossRef] [PubMed]
- Caballeria, L.; Pera, G.; Arteaga, I.; Rodríguez, L.; Alumà, A.; Morillas, R.M.; de la Ossa, N.; Díaz, A.; Expósito, C.; Miranda, D.; et al. High prevalence of liver fibrosis among European adults with unknown liver disease: A population-based study. Clin. Gastroenterol. Hepatol. 2018, 16, 1138–1145.e5. [Google Scholar] [CrossRef] [PubMed]
- Vilar-Gomez, E.; Calzadilla-Bertot, L.; Wai-Sun, W.V.; Castellanos, M.; Aller-de, L.F.R.; Metwally, M.; Eslam, M.; Gonzalez-Fabian, L.; Sanz, M.A.-Q.; Conde-Martín, A.F.; et al. Fibrosis severity as a determinant of cause-specific mortality in patients with advanced nonalcoholic fatty liver disease: A multi-national cohort study. Gastroenterology 2018, 155, 443–457. [Google Scholar] [CrossRef]
- Langford, C.A. Management of systemic vasculitis. Best Pract. Res. Clin. Rheumatol. 2001, 15, 281–297. [Google Scholar] [CrossRef] [PubMed]
- Feagan, B.G.; Alfadhli, A. Methotrexate in inflammatory bowel disease. Gastroenterol. Clin. N. Am. 2004, 33, 407–420. [Google Scholar] [CrossRef]
- Wu, J.J.; Schiff, K.R. Sarcoidosis. Am. Fam. Physician 2004, 70, 312–322. [Google Scholar]
- Naldi, L.; Griffiths, C.E. Traditional therapies in the management of moderate to severe chronic plaque psoriasis: An assessment of the benefits and risks. Br. J. Dermatol. 2005, 152, 597–615. [Google Scholar] [CrossRef]
- ter Borg, E.J.; Seldenrijk, C.A.; Timmer, R. Liver cirrhosis due to methotrexate in a patient with rheumatoid arthritis. Neth. J. Med. 1996, 49, 244–246. [Google Scholar] [CrossRef]
- Bangert, C.A.; Costner, M.I. Methotrexate in dermatology. Dermatol. Ther. 2007, 20, 216–228. [Google Scholar] [CrossRef]
- Holliday, A.C.; Moody, M.N.; Berlingeri-Ramos, A. Methotrexate: Role of treatment in skin disease. Skin Ther. Lett. 2013, 18, 4–9. [Google Scholar]
- Ezhilarasan, D. Hepatotoxic potentials of methotrexate: Understanding the possible toxicological molecular mechanisms. Toxicology 2021, 458, 152840. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.L. Hepatic stellate cells: Protean, multifunctional, and enigmatic cells of the liver. Physiol. Rev. 2008, 88, 125–172. [Google Scholar] [CrossRef]
- Uraz, S.; Tahan, V.; Aygun, C.; Eren, F.; Unluguzel, G.; Yuksel, M.; Senturk, O.; Avsar, E.; Haklar, G.; Celikel, C.; et al. Role of ursodeoxycholic acid in prevention of methotrexate-induced liver toxicity. Dig. Dis. Sci. 2008, 53, 1071–1077. [Google Scholar] [CrossRef]
- Taskin, B.; Erdoğan, M.A.; Yiğittürk, G.; Günenç, D.; Erbaş, O. Antifibrotic effect of lactulose on a methotrexate-induced liver injury model. Gastroenterol. Res. Pract. 2017, 2017, 7942531. [Google Scholar] [CrossRef]
- Vogel, W.H.; Snyder, R.; Schulman, M.P. The inhibition of dehydrogenases by folic acid and several of its analogs. Biochem. Biophys. Res. Commun. 1963, 10, 97–101. [Google Scholar] [CrossRef]
- Lucas, M.; Solano, F. Coelenterazine is a superoxide anion-sensitive chemiluminescent probe: Its usefulness in the assay of respiratory burst in neutrophils. Anal. Biochem. 1992, 206, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Videla, L.A.; Correa, L.; Rivera, M.; Sir, T. Zymosan-induced luminol-amplified chemiluminescence of whole blood phagocytes in experimental and human hyperthyroidism. Free Radic. Biol. Med. 1993, 14, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Van Dyke, K.; Patel, S.; Vallyathan, V. Lucigenin chemiluminescence assay as an adjunctive tool for assessment of various stages of inflammation: A study of quiescent inflammatory cells. J. Biosci. 2003, 28, 115–119. [Google Scholar] [CrossRef]
- Verma, S.; Kaplowitz, N. Diagnosis, management and prevention of drug-induced liver injury. Gut 2009, 58, 1555–1564. [Google Scholar] [CrossRef]
- Abo-Haded, H.M.; Elkablawy, M.A.; Al-Johani, Z.; Al-Ahmadi, O.; El-Agamy, D.S. Hepatoprotective effect of sitagliptin against methotrexate-induced liver toxicity. PLoS ONE 2017, 12, e0174295. [Google Scholar] [CrossRef]
- Mehrzadi, S.; Fatemi, I.; Esmaeilizadeh, M.; Ghaznavi, H.; Kalantar, H.; Goudarzi, M. Hepatoprotective effect of berberine against methotrexate-induced liver toxicity in rats. Biomed. Pharmacother. 2018, 97, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Heyens, L.; Busschots, D.; Koek, G.H.; Robaeys, G.; Francque, S. Liver fibrosis in non-alcoholic fatty liver disease: From liver biopsy to non-invasive biomarkers in diagnosis and treatment. Front. Med. 2021, 8, 615978. [Google Scholar] [CrossRef] [PubMed]
- Shan, L.; Wang, F.; Zhai, D.; Meng, X.; Liu, J.; Lv, X. New drugs for hepatic fibrosis. Front. Pharmacol. 2022, 13, 874408. [Google Scholar] [CrossRef]
- Al-Salama, Z.T.; Scott, L.J. Baricitinib: A review in rheumatoid arthritis. Drugs 2018, 78, 761–772. [Google Scholar] [CrossRef]
- Gu, S.; Liang, J.; Zhang, J.; Liu, Z.; Miao, Y.; Wei, Y.; Li, S.; Gu, J.; Cui, Y.; Xiao, T.; et al. Baricitinib attenuates bleomycin-induced pulmonary fibrosis in mice by inhibiting TGF-β1 signaling pathway. Medicina 2023, 28, 2195. [Google Scholar] [CrossRef]
- Hou, Z.; Su, X.; Han, G. JAK1/2 inhibitor baricitinib improves skin fibrosis and digital ulcers in systemic sclerosis. Front. Med. 2022, 9, 859330. [Google Scholar] [CrossRef] [PubMed]
- Bradford, M.M. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal. Biochem. 1976, 72, 248–254. [Google Scholar] [CrossRef]
- Lobenhofer, E.K.; Boorman, G.A.; Phillips, K.L.; Heinloth, A.N.; Malarkey, D.E.; Blackshear, P.E.; Houle, C.; Hurban, P. Application of visualization tools to the analysis of histopathological data enhances biological insight and interpretation. Toxicol. Pathol. 2006, 34, 921–928. [Google Scholar] [CrossRef]
- Sener, G.; Eksioglu-Demiralp, E.; Cetiner, M.; Ercan, F.; Yegen, B.C. Betaglucan ameliorates methotrexate-induced oxidative organ injury via its antioxidant and immunomodulatory effects. Eur. J. Pharmacol. 2006, 542, 170–178. [Google Scholar] [CrossRef]
- Dalaklioglu, S.; Genc, G.E.; Aksoy, N.H.; Akcit, F.; Gumuslu, S. Resveratrol ameliorates methotrexate-induced hepatotoxicity in rats via inhibition of lipid peroxidation. Hum. Exp. Toxicol. 2013, 32, 662–671. [Google Scholar] [CrossRef]
- Rosen, H.R.; Keeffe, E.B. Evaluation of abnormal liver enzymes, use of liver test, and the serology of viral hepatitis. In Liver Disease Diagnosis and Management; Bacon, B.R., Di Bisceglie, A.M., Eds.; Churchill: New York, NY, USA, 2000; pp. 24–35. [Google Scholar]
- Bozkurt, M.; Bodakci, M.N.; Turkcu, G.; Kuyumcu, M.; Akkurt, M.; Sula, B.; Em, S.; Oktayoglu, P.; Batmaz, I.; Yüksel, H. Protective effects of carvacrol against methotrexate-induced liver toxicity in rats. Acta Chir. Belg. 2014, 114, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Tunali-Akbay, T.; Sehirli, O.; Ercan, F.; Sener, G. Resveratrol protects against methotrexate-induced hepatic injury in rats. J. Pharm. Sci. 2010, 13, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Cusi, K.; Chang, Z.; Harrison, S.; Lomonaco, R.; Bril, F.; Orsak, B.; Ortiz-Lopez, C.; Hecht, J.; Feldstein, A.E.; Webb, A.; et al. Limited value of plasma cytokeratin-18 as a biomarker for NASH and fibrosis in patients with non-alcoholic fatty liver disease. J. Hepatol. 2014, 60, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Jahovic, N.; Cevik, H.; Sehirli, A.O.; Yeğen, B.C.; Sener, G. Melatonin prevents methotrexate-induced hepatorenal oxidative injury in rats. J. Pineal Res. 2003, 34, 282–287. [Google Scholar] [CrossRef]
- Hadi, N.R.; Al-Amran, F.G.; Swadi, A. Metformin ameliorates methotrexate-induced hepatotoxicity. J. Pharmacol. Pharmacother. 2012, 3, 248–253. [Google Scholar] [CrossRef]
- Elsawy, H.; Algefare, A.I.; Alfwuaires, M.; Khalil, M.; Elmenshawy, O.M.; Sedky, A.; Abdel-Moneim, A.M. Naringin alleviates methotrexate-induced liver injury in male albino rats and enhances its antitumor efficacy in HepG2 cells. Biosci. Rep. 2020, 40, BSR20193686. [Google Scholar] [CrossRef]
- Dooley, S.; Ten Dijke, P. TGF-β in progression of liver disease. Cell Tissue Res. 2012, 347, 245–256. [Google Scholar] [CrossRef]
- Haak, A.J.; Kostallari, E.; Sicard, D.; Ligresti, G.; Choi, K.M.; Caporarello, N.; Jones, D.L.; Tan, Q.; Meridew, J.; Diaz Espinosa, A.M.; et al. Selective YAP/TAZ inhibition in fibroblasts via dopamine receptor D1 agonism reverses fibrosis. Sci. Transl. Med. 2019, 11, eaau6296. [Google Scholar] [CrossRef]
- Yu, H.X.; Yao, Y.; Bu, F.T.; Chen, Y.; Jiang, S.; He, Z. Mitochondrial reactive oxygen species-regulated Nrf2 and apoptosis induction protect against mitochondrial dysfunction in methotrexate-induced hepatotoxicity. Eur. J. Pharmacol. 2021, 893, 173818. [Google Scholar]
- Alsamman, S.; Christenson, S.A.; Yu, A.; Ayad, N.M.E.; Mooring, M.S.; Segal, J.M.; Hu, J.K.; Schaub, J.R.; Ho, S.S.; Rao, V.; et al. Targeting acid ceramidase inhibits YAP/TAZ signaling to reduce fibrosis in mice. Sci. Transl. Med. 2020, 12, eaay8798. [Google Scholar] [CrossRef]
- Mooring, M.; Fowl, B.H.; Lum, S.Z.C.; Liu, Y.; Yao, K.; Softic, S.; Kirchner, R.; Bernstein, A.; Singhi, A.D.; Jay, D.G.; et al. Hepatocyte stress increases expression of Yes-associated protein and transcriptional coactivator with PDZ-binding motif in hepatocytes to promote parenchymal inflammation and fibrosis. Hepatology 2020, 71, 1813–1830. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Cai, B.; Yang, X.; Sonubi, O.O.; Zheng, Z.; Ramakrishnan, R.; Shi, H.; Valenti, L.; Pajvani, U.B.; Sandhu, J.; et al. Cholesterol stabilizes TAZ in hepatocytes to promote experimental non-alcoholic steatohepatitis. Cell Metab. 2020, 31, 969–986.e7. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Zhang, R.; Zhan, Y.; Zheng, J. Resveratrol inhibits hepatic stellate cell activation via the Hippo pathway. Mediat. Inflamm. 2021, 2021, 3399357. [Google Scholar] [CrossRef]
- Gui, Y.; Li, J.; Lu, Q.; Feng, Y.; Wang, M.; He, W.; Yang, J.; Dai, C. Yap/Taz mediates mTORC2-stimulated fibroblast activation and kidney fibrosis. J. Biol. Chem. 2018, 293, 16364–16375. [Google Scholar] [CrossRef] [PubMed]
- Francisco, J.; Zhang, Y.; Jeong, J.I.; Mizushima, W.; Ikeda, S.; Ivessa, A.; Oka, S.; Zhai, P.; Tallquist, M.D.; Del Re, D.P. Blockade of fibroblast YAP attenuates cardiac fibrosis and dysfunction through MRTF-A inhibition. JACC Basic Transl. Sci. 2020, 5, 931–945. [Google Scholar] [CrossRef]
- Mannaerts, I.; Leite, S.B.; Verhulst, S.; Claerhout, S.; Eysackers, N.; Thoen, L.F.; Hoorens, A.; Reynaert, H.; Halder, G.; van Grunsven, L.A. The Hippo pathway effector YAP controls mouse hepatic stellate cell activation. J. Hepatol. 2015, 63, 679–688. [Google Scholar] [CrossRef]

{kind=link}
| Group | Body Weight (g) | Age (Weeks) |
|---|---|---|
| Control | 176.5 ± 9.4 | 11.2 ± 0.4 |
| MTX + Saline | 178.1 ± 10.2 | 11.3 ± 0.5 |
| MTX + Baricitinib | 177.3 ± 8.9 | 11.1 ± 0.6 |
| Control | MTX + Saline | MTX + Baricitinib | |
|---|---|---|---|
| Liver TGF-β level (pg/g) | 0.58 ± 0.2 | 2.6 ± 0.1 * | 1.15 ± 0.1 # |
| Liver MDA level (nmol/g tissue) | 30.8 ± 0.6 | 68.2 ± 3.5 ** | 45.4 ± 1.8 ## |
| Liver YAP1 level (pg/g) | 635.1 ± 4.6 | 958.2 ± 2.4 * | 715.9 ± 1.8 # |
| Plasma cytokeratin-18 level (ng/mL) | 1.2 ± 0.1 | 2.75 ± 0.6 ** | 1.9 ± 0.3 ## |
| Plasma MDA level (nM) | 32.5 ± 1.8 | 122.4 ± 6.5 ** | 106.8 ± 3.1 # |
| Plasma ALT (IU/L) | 16.5 ± 0.8 | 44.2 ± 1.5 * | 32.3 ± 1.6 # |
| Control | MTX + Saline | MTX + Baricitinib | |
|---|---|---|---|
| Hepatic necrosis | 0 [0–1] | 2 [2,3] * | 1 [0–2] # |
| Fibrosis | 0 [0–1] | 2 [1,2,3] * | 1 [0–2] # |
| Cellular infiltration | 0 [0–1] | 2 [1,2,3] * | 1 [0–2] # |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ulusan, M.; Erdogan, M.A.; Simsek, O.; Dogan, Z.; Ciftci, B.B.; Atalan, G.; Erbas, O. Baricitinib Mitigates Methotrexate-Induced Liver Fibrosis Model via YAP Pathway. Medicina 2025, 61, 857. https://doi.org/10.3390/medicina61050857
Ulusan M, Erdogan MA, Simsek O, Dogan Z, Ciftci BB, Atalan G, Erbas O. Baricitinib Mitigates Methotrexate-Induced Liver Fibrosis Model via YAP Pathway. Medicina. 2025; 61(5):857. https://doi.org/10.3390/medicina61050857
Chicago/Turabian StyleUlusan, Mehmet, Mumin Alper Erdogan, Ozkan Simsek, Zafer Dogan, Bertug Bekir Ciftci, Gultekin Atalan, and Oytun Erbas. 2025. "Baricitinib Mitigates Methotrexate-Induced Liver Fibrosis Model via YAP Pathway" Medicina 61, no. 5: 857. https://doi.org/10.3390/medicina61050857
APA StyleUlusan, M., Erdogan, M. A., Simsek, O., Dogan, Z., Ciftci, B. B., Atalan, G., & Erbas, O. (2025). Baricitinib Mitigates Methotrexate-Induced Liver Fibrosis Model via YAP Pathway. Medicina, 61(5), 857. https://doi.org/10.3390/medicina61050857