
Serum α-Synuclein in Pediatric Refractory Epilepsy: Correlation with Diagnosis and Clinical Severity

 , , , ,
, , , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Serum α-Synuclein Measurement
2.2. Sample Size
- Standardized blood collection methods included
- o
- Time of day samples were collected.
- o
- Time elapsed since the last seizure.
3. Results
4. Discussion
Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aaberg, K.M.; Gunnes, N.; Bakken, I.J.; Lund Søraas, C.; Berntsen, A.; Magnus, P.; Morten, I.L.; Camilla, S.; Richard, C.; Pål, S. Incidence and prevalence of childhood epilepsy: A nationwide cohort study. Pediatrics 2017, 139, e20163908. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-H.; Chou, I.-C.; Hong, S.-Y. Genetic factors and the risk of drug-resistant epilepsy in young children with epilepsy and neurodevelopment disability: A prospective study and updated meta-analysis. Medicine 2021, 100, e25277. [Google Scholar] [CrossRef] [PubMed]
- Löscher, W.; Potschka, H.; Sisodiya, S.M.; Vezzani, A. Drug resistance in epilepsy: Clinical impact, potential mechanisms, and new innovative treatment options. Pharmacol. Rev. 2020, 72, 606–638. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Gong, Y.; Wang, Y.; Chen, Z. New advances in pharmacoresistant epilepsy towards precise management-from prognosis to treatments. Pharmacol. Ther. 2022, 233, 108026. [Google Scholar] [CrossRef]
- Paudel, Y.N.; Shaikh, M.F.; Shah, S.; Kumari, Y.; Othman, I. Role of inflammation in epilepsy and neurobehavioral comorbidities: Implication for therapy. Eur. J. Pharmacol. 2018, 837, 145–155. [Google Scholar] [CrossRef]
- Vezzani, A.; Balosso, S.; Ravizza, T. Neuroinflammatory pathways as treatment targets and biomarkers in epilepsy. Nat. Rev. Neurol. 2019, 15, 459–472. [Google Scholar] [CrossRef]
- Łukawski, K.; Andres-Mach, M.; Czuczwar, M.; Łuszczki, J.J.; Kruszyński, K.; Czuczwar, S.J. Mechanisms of epileptogenesis and preclinical approach to antiepileptogenic therapies. Pharmacol. Rep. 2018, 70, 284–293. [Google Scholar] [CrossRef]
- van Loo, K.M.J.; Becker, A.J. Transcriptional Regulation of Channelopathies in Genetic and Acquired Epilepsies. Front. Cell. Neurosci. 2020, 13, 587. [Google Scholar] [CrossRef]
- Ali, N.H.; Al-Kuraishy, H.M.; Al-Gareeb, A.I.; Alnaaim, S.A.; Hetta, H.F.; Saad, H.M.; Batiha, G.E.-S. A Mutual Nexus Between Epilepsy and α-Synuclein: A Puzzle Pathway. Mol. Neurobiol. 2024, 61, 10198–10215. [Google Scholar] [CrossRef]
- Choi, J.; Kim, S.Y.; Kim, H.; Lim, B.C.; Hwang, H.; Chae, J.H.; Kim, K.J.; Oh, S.; Kim, E.Y.; Shin, J.-S. Serum α-synuclein and IL-1β are increased and correlated with measures of disease severity in children with epilepsy: Potential prognostic biomarkers? BMC Neurol. 2020, 20, 85. [Google Scholar] [CrossRef]
- Li, A.; Choi, Y.S.; Dziema, H.; Cao, R.; Cho, H.Y.; Jung, Y.J.; Obrietan, K. Proteomic profiling of the epileptic dentate gyrus. Brain Pathol. 2010, 20, 1077–1089. [Google Scholar] [CrossRef] [PubMed]
- Holopainen, I.E. Seizures in the Developing Brain: Cellular and Molecular Mechanisms of Neuronal Damage, Neurogenesis, and Cellular Reorganization. Neurochem. Int. 2008, 52, 935–947. [Google Scholar] [CrossRef] [PubMed]
- Ambrogini, P.; Torquato, P.; Bartolini, D.; Albertini, M.C.; Lattanzi, D.; Di Palma, M.; Marinelli, R.; Betti, M.; Minelli, A.; Cuppini, R.; et al. Excitotoxicity, neuroinflammation and oxidant stress as molecular bases of epileptogenesis and epilepsy-derived neurodegeneration: The role of vitamin E. Biochim. Biophys. Acta (BBA)-Mol. Basis Dis. 2019, 1865, 1098–1112. [Google Scholar] [CrossRef]
- Minic, R.; Zivkovic, I. Optimization, Validation and Standardization of ELISA. In Norovirus; IntechOpen: London, UK, 2021; p. 9. [Google Scholar]
- Liu, Q.; Ma, J.; Yu, G.; Zhang, Q.; Zhu, Y.; Wang, R.; Yu, H.; Liu, C.; Sun, Y.; Wang, W.; et al. Postoperative seizure and developmental outcomes of children with hemimegalencephaly and drug-resistant epilepsy. Seizure 2021, 92, 29–35. [Google Scholar] [CrossRef]
- Ascoli, M.; Mastroianni, G.; Gasparini, S.; Striano, P.; Cianci, V.; Neri, S.; Bova, V.; Mammì, A.; Gambardella, A.; Labate, A.; et al. Diagnostic and therapeutic approach to drug-resistant juvenile myoclonic epilepsy. Expert Rev. Neurother. 2021, 21, 1265–1273. [Google Scholar] [CrossRef]
- Idris, A.; Alabdaljabar, M.S.; Almiro, A.; Alsuraimi, A.; Dawalibi, A.; Abduljawad, S.; AlKhateeb, M. Prevalence, incidence, and risk factors of epilepsy in arab countries: A systematic review. Seizure 2021, 92, 40–50. [Google Scholar] [CrossRef]
- Al Habbal, A.; AlSharif, A.; Almubark, A.; Fattouh, H.; Hamzeh, G.; Kakaje, A. Risk factors associated with epilepsy in children and adolescents: A case-control study from Syria. Epilepsy Behav. 2021, 114, 107596. [Google Scholar] [CrossRef]
- Fawi, G.; Abbas, M.A.; Gamea, A. Prevalence of Idiopathic Epilepsy Among Primary School Children in Qena City, Qena Governorate, Egypt. SVU-Int. J. Med. Sci. 2023, 6, 602–613. [Google Scholar] [CrossRef]
- Abokrysha, N.T.; Taha, N.; Shamloul, R.; Elsayed, S.; Osama, W.; Hatem, G. Clinical, radiological and electrophysiological predictors for drug-resistant epilepsy. Egypt. J. Neurol. Psychiat. Neurosurg. 2023, 59, 44. [Google Scholar] [CrossRef]
- Shah, A.K.; Mittal, S. Evaluation of magnetic resonance imaging-negative drug-resistant epilepsy. Ann. Indian Acad. Neurol. 2014, 17 (Suppl. S1), S80–S88. [Google Scholar] [CrossRef]
- Yang, S.; Li, S.; Wang, H.; Li, J.; Wang, C.; Liu, Q.; Zhong, J.; Jia, M. Early prediction of drug-resistant epilepsy using clinical and EEG features based on convolutional neural network. Seizure: Eur. J. Epilepsy 2024, 114, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Czech, T.; Felizardo, M.; Baumgartner, C.; Lubec, G. Aberrant expression of cytoskeleton proteins in hippocampus from patients with mesial temporal lobe epilepsy. Amino acids. 2006, 30, 477–493. [Google Scholar] [CrossRef] [PubMed]
- Şener, N.; Keti, D.B.; Güleç, A.; Canpolat, M.; Per, H.; Gümüş, H.; Muhtaroğlu, S. Biochemical risk factors associated with refractory epilepsy: Alpha synuclein and adenosine deaminase. Rev. Rom. Med. Lab. 2024, 32, 255–261. [Google Scholar] [CrossRef]
- Surguchov, A.; Surgucheva, I.; Sharma, M.; Sharma, R.; Singh, V. Pore-forming proteins as mediators of novel epigenetic mechanism of epilepsy. Front. Neurol. 2017, 8, 3. [Google Scholar] [CrossRef]
- Şimşek, F.; Ceylan, M.; Aşkın, S.; Kızıltunç, A. Serum myeloperoxidase, malondialdehyde, alpha-synuclein levels in patients with epilepsy. Malang Neurol. J. 2021, 7, 93–97. [Google Scholar] [CrossRef]
- Rong, H.; Jin, L.; Wei, W.; Wang, X.; Xi, Z. Alpha-synuclein is a potential biomarker in the serum and CSF of patients with intractable epilepsy. Seizure 2015, 27, 6–9. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | Drug-Resistant Epilepsy | Drug-Responsive Epilepsy | U | p Value | ||
|---|---|---|---|---|---|---|
| Range | Median (Interquartile Range) | Range | Median (Interquartile Range) | |||
| Age (in years) | 2.0–12.0 | 5.0 (4.0–9.0) | 1.5–12.0 | 8.0 (5.0–10.0) | U = 366.0 | 0.213 |
| Age of onset of seizures (in years) | 0.01–8.00 | 0.75 (0.25–2.00) | 0.17–9.50 | 5.0 (0.50–6.44) | 261.5 | 0.005 * |
| Duration of epilepsy (in years) | 1.00–11.33 | 3.79 (2.96–6.69) | 1.4–7.0 | 3.25 (2.00–4.77) | 341.5 | 0.108 |
| Time from last attack of seizure (in years) | 0.00–0.50 | 0.08 (0.01–0.25) | 1.08–2.50 | 1.42 (1.17–1.67) | 465.0 # | <0.001 * |
| Numbers of hospital admissions due to seizures | 1.0–10.0 | 4.0 (2.0–5.0) | 0.0–5.0 | 2.0 (0.0–2.0) | 160.0 | <0.001 * |
| Variables | Drug-Resistant Epilepsy | Drug-Responsive Epilepsy | X2 | p Value |
|---|---|---|---|---|
| N (%) | N (%) | |||
| Psychomotor developmental disorders | X2 = 13.303 | <0.001 * | ||
| Normal | 6 (20.0%) | 20 (66.7%) | ||
| Delayed | 24 (80.0%) | 10 (33.3%) | ||
| Subtypes of seizures | X2 = 2.857 | 0.158 | ||
| Generalized | 18 (60.0%) | 24 (80.0%) | ||
| Focal | 12 (40.0%) | 6 (20.0%) | ||
| Seizure frequency per month | U = 465.0 | <0.001 * | ||
| Median (interquartile range) | 3 (2–4) | 0 | ||
| Etiology of epilepsy: | X2 = 2.848 | 0.461 | ||
| Structural | 13(43.3%) | 9(30%) | ||
| Genetic | 5(16.7%) | 8(26.7%) | ||
| Infectious | 3(10.0%) | 1(3.3%) | ||
| Unknown | 9(30%) | 12(40.0%) | ||
| EEG | 0.089 | 1.000 | ||
| Normal | 7 (23.3%) | 8 (26.7%) | ||
| Abnormal | 23 (76.7%) | 22 (73.3%) | ||
| MRI | 3.300 | 0.119 | ||
| Normal | 13 (43.3%) | 20 (66.7%) | ||
| Abnormal | 17 (56.7%) | 10 (33.3%) | ||
| Anti-epileptic drugs | 24.300 | <0.001 * | ||
| Monotherapy | 1 (3.3%) | 19 (63.3%) | ||
| Polytherapy | 29 (96.7%) | 11 (36.7%) |
| Control | Drug-Responsive Epilepsy | Drug-Resistant Epilepsy | p ** | p1 # | p2 # | p3 # | |
|---|---|---|---|---|---|---|---|
| Median (IQR Range) | Median (IQR Range) | Median (IQR Range) | |||||
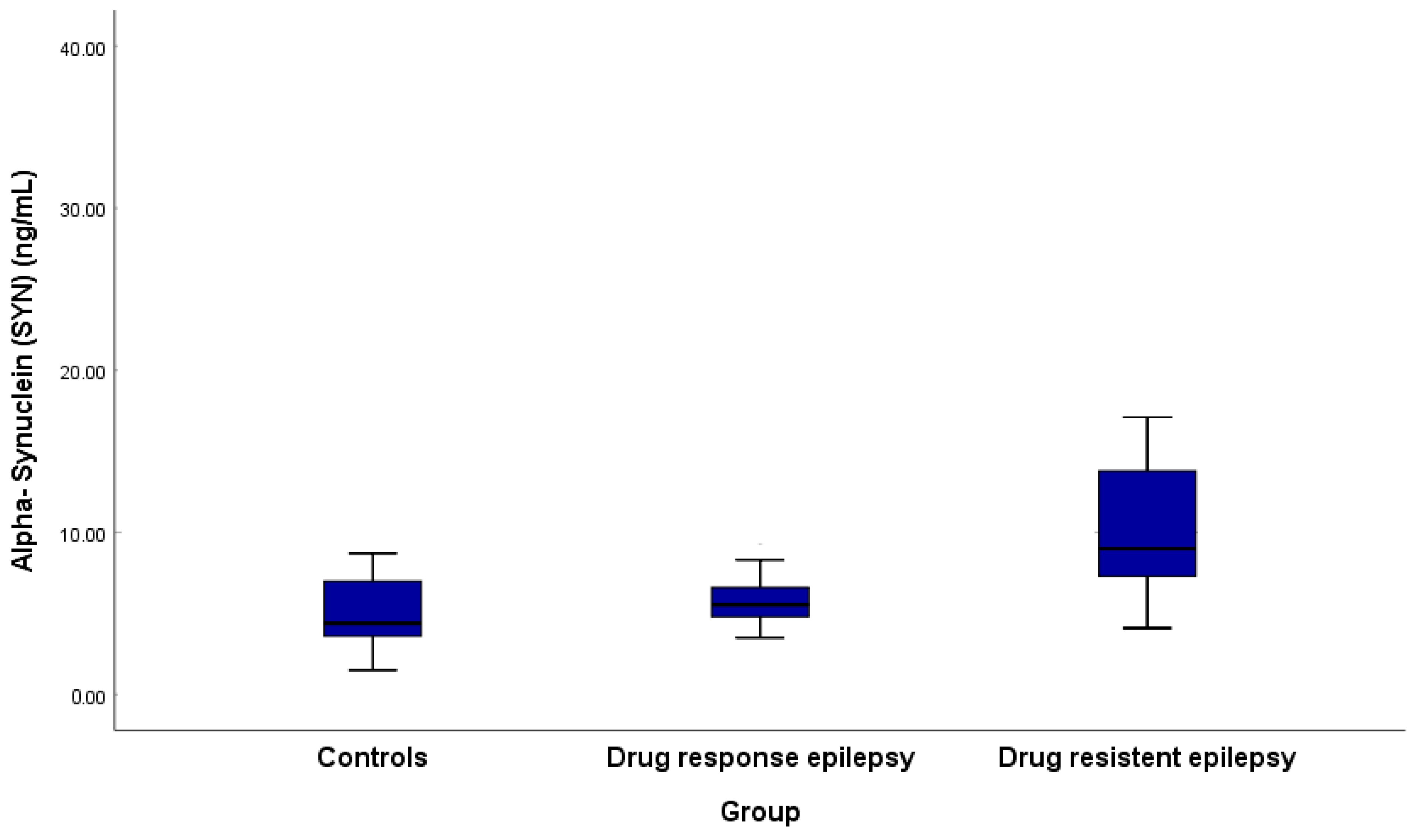
| α-syn (ng/mL) | 4.40 (3.58–7.05) | 5.55 (4.78–6.60) | 9.0 (7.23–14.58) | <0.001 * | 0.040 * | <0.001 * | <0.001 * |
| Variables | Alpha-Synuclein (ng/mL) Median (IQR) | U | p Value |
|---|---|---|---|
| Epilepsy Subtype | |||
| Focal epilepsy | 6.8 (5.7–9.4) | U = 356.0 | 0.723 |
| Generalized epilepsy | 6.65 (5.28–9.55) | ||
| Epilepsy etiology | |||
| Structural epilepsy | 7.90 (5.65–11.08) | ||
| Genetic epilepsy | 6.6 (5.3–8.5) | H = 2.522 | 0.471 |
| Infectious epilepsy | 5.75 (4.53–11.85) | ||
| Epilepsy of unknown cause | 6.70 (4.85–7.90) | ||
| MRI | |||
| Normal | 6.10 (5.20–7.50) | U = 329.0 | 0.083 |
| Abnormal | 8.30 (5.60–11.55) | ||
| EEG | |||
| Focal | 6.00 (5.70–9.00) | U = 196.5 | 0.331 |
| Generalized | 7.50 (5.45–10.95) |
| Variables | Alpha-Synuclein | |
|---|---|---|
| R | p Value | |
| Age | −0.222 | 0.088 |
| Numbers of hospital admissions due to seizures | 0.304 | 0.018 * |
| Duration of epilepsy (in years) | 0.040 | 0.761 |
| Time of last attack of seizure (in years) | −0.417 | 0.001 * |
| Age of onset of seizures (in years) | −0.310 | 0.016 * |
| Number of AEDs | 0.336 | 0.009 * |
| Frequency of seizures per month | 0.505 | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salem, A.M.S.; Morgan, D.S.; Elgendy, M.O.; Abdelrahim, M.E.A.; Mohamed Mostafa, N.M.; Saleh, A.; Abdel-Aziz, M.M.; Ramadan, A.K. Serum α-Synuclein in Pediatric Refractory Epilepsy: Correlation with Diagnosis and Clinical Severity. Medicina 2025, 61, 818. https://doi.org/10.3390/medicina61050818
Salem AMS, Morgan DS, Elgendy MO, Abdelrahim MEA, Mohamed Mostafa NM, Saleh A, Abdel-Aziz MM, Ramadan AK. Serum α-Synuclein in Pediatric Refractory Epilepsy: Correlation with Diagnosis and Clinical Severity. Medicina. 2025; 61(5):818. https://doi.org/10.3390/medicina61050818
Chicago/Turabian StyleSalem, Aida M. S., Dalia Saber Morgan, Marwa O. Elgendy, Mohamed E. A. Abdelrahim, Noura Mostafa Mohamed Mostafa, Asmaa Saleh, Manar M. Abdel-Aziz, and Asmaa K. Ramadan. 2025. "Serum α-Synuclein in Pediatric Refractory Epilepsy: Correlation with Diagnosis and Clinical Severity" Medicina 61, no. 5: 818. https://doi.org/10.3390/medicina61050818
APA StyleSalem, A. M. S., Morgan, D. S., Elgendy, M. O., Abdelrahim, M. E. A., Mohamed Mostafa, N. M., Saleh, A., Abdel-Aziz, M. M., & Ramadan, A. K. (2025). Serum α-Synuclein in Pediatric Refractory Epilepsy: Correlation with Diagnosis and Clinical Severity. Medicina, 61(5), 818. https://doi.org/10.3390/medicina61050818