
Prognostic Value of Preoperative Lymphocyte-to-Monocyte Ratio in Patients with Recurrent Colorectal Cancer


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Statistical Analysis Methods
3. Results
3.1. Patient Characteristics
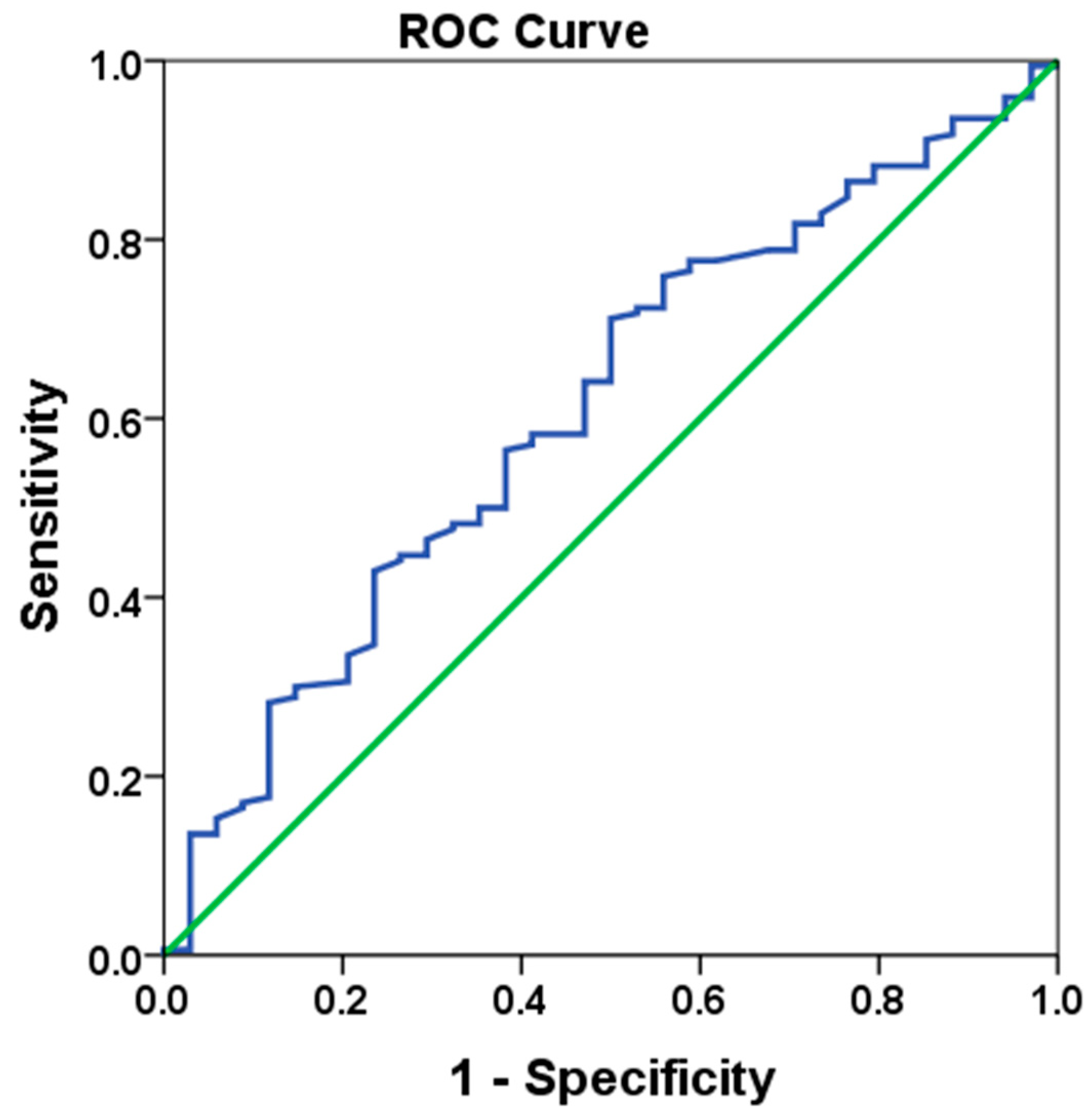
3.2. LMR Cut-Off Value
3.3. Comparison Between LMR-H and LMR-L Groups
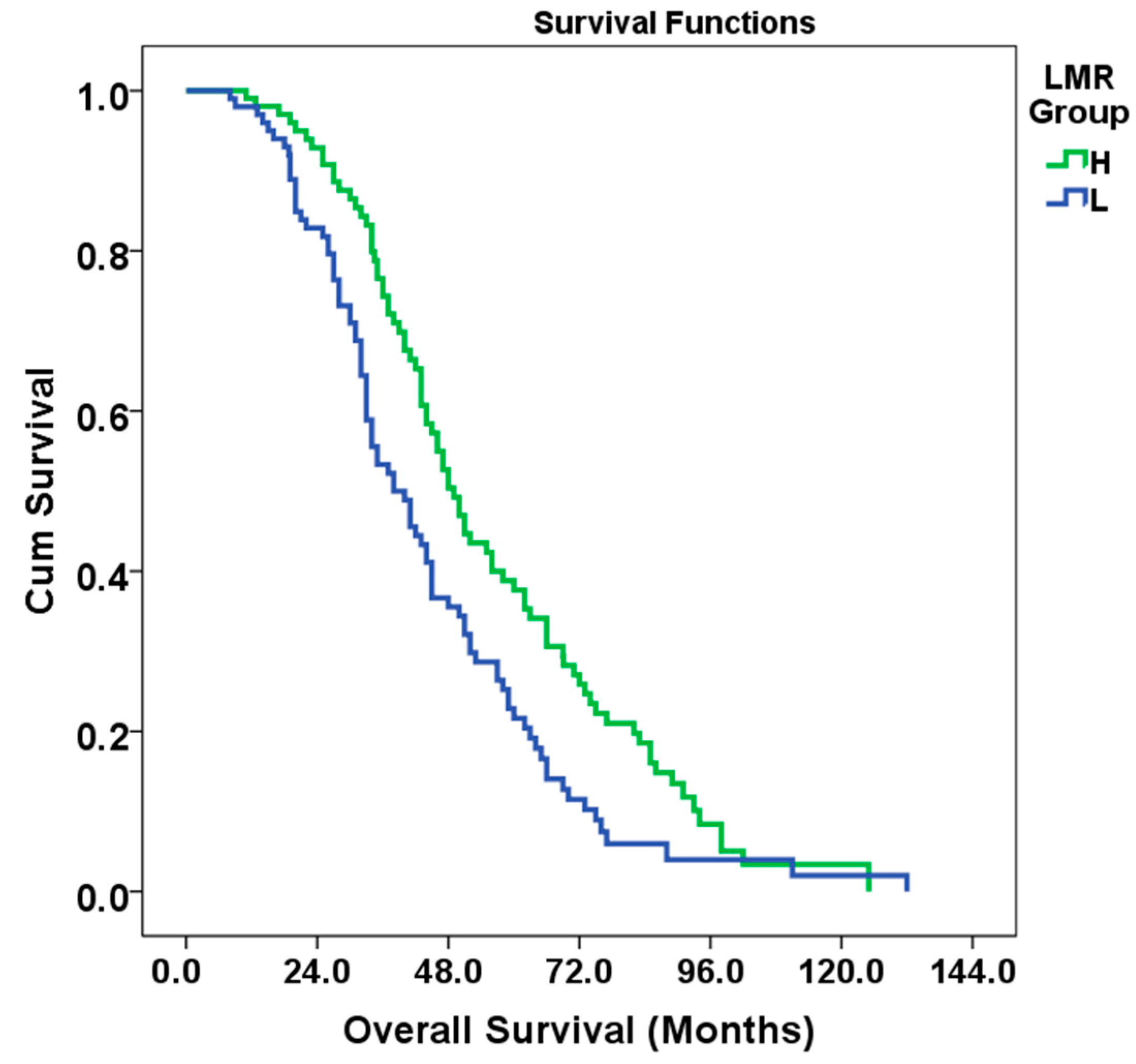
3.4. OS Assessment Results by LMR Groups
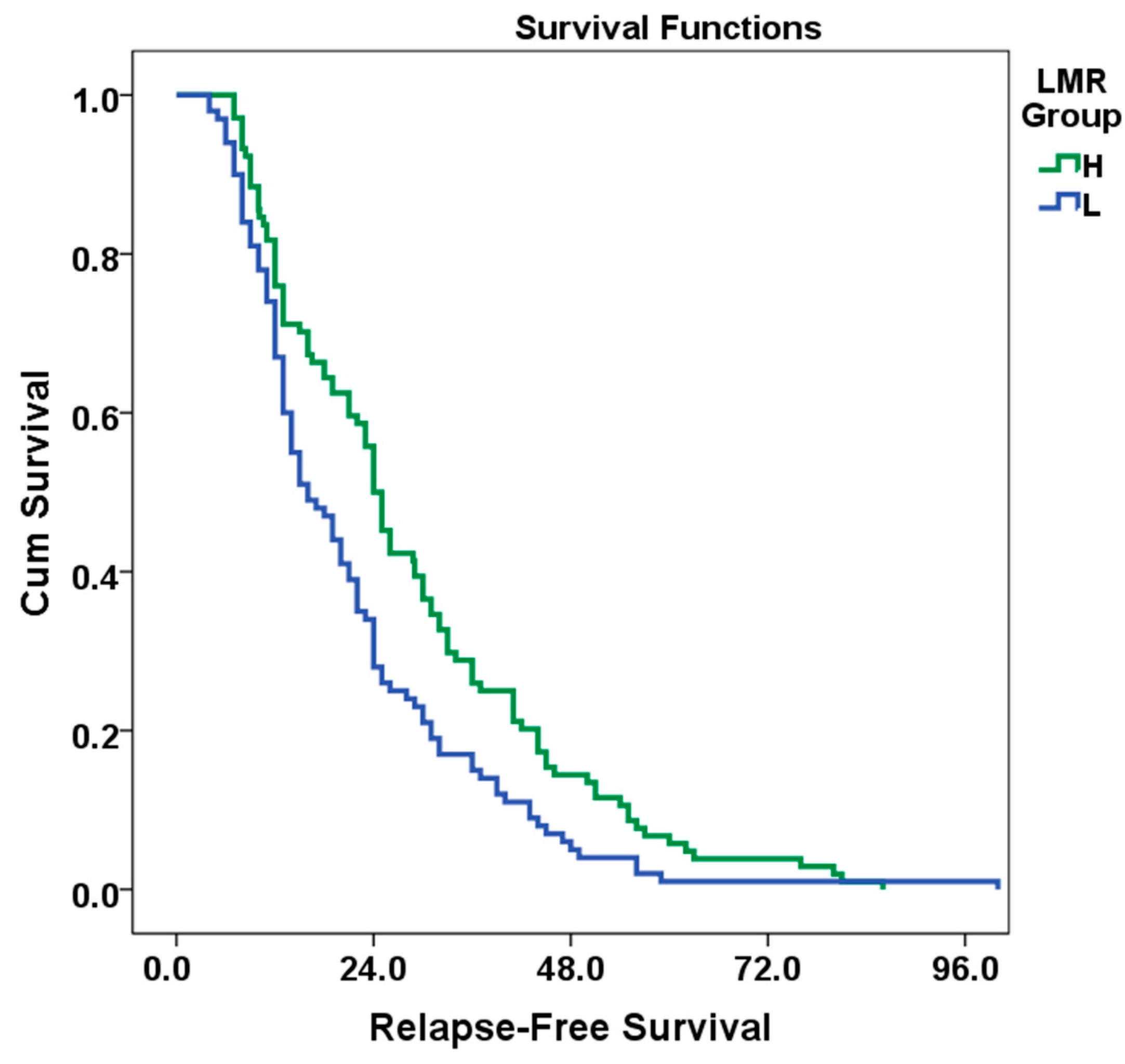
3.5. Results of Evaluation of RFS According to LMR Groups
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garzon-Muvdi, T.; Yang, W.; Lim, M.; Brem, H.; Huang, J. Atypical and anaplastic meningioma: Outcomes in a population based study. J. Neuro-Oncol. 2017, 133, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2020. CA A Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [PubMed]
- Dekker, E.; Tanis, P.J.; Vleugels, J.L.; Kasi, P.M.; Wallace, M.B. Colorectal cancer. Lancet 2019, 394, 1467–1480. [Google Scholar] [CrossRef] [PubMed]
- Keum, N.; Giovannucci, E. Global burden of colorectal cancer: Emerging trends, risk factors and prevention strategies. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 713–732. [Google Scholar] [CrossRef]
- Grivennikov, S.I.; Greten, F.R.; Karin, M. Immunity, inflammation, and cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Guthrie, G.J.; Charles, K.A.; Roxburgh, C.S.; Horgan, P.G.; McMillan, D.C.; Clarke, S.J. The systemic inflammation-based neutrophil–lymphocyte ratio: Experience in patients with cancer. Crit. Rev. Oncol./Hematol. 2013, 88, 218–230. [Google Scholar] [CrossRef]
- Jansson, H. Immunological Aspects on Prognosis in Resectable Cholangiocellular Cancer; Karolinska Institutet: Stockholm, Sweden, 2022. [Google Scholar]
- Liu, X.-C.; Dai, Y.-L.; Huang, F.; Zhong, Z.-J.; Liu, X.-F. Diagnostic Value of Carcinoembryonic Antigen Combined with Multi-Inflammatory Cell Ratios in Colorectal Cancer. Dis. Markers 2022, 2022, 4889616. [Google Scholar] [CrossRef]
- Roxburgh, C.S.; McMillan, D.C. Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol. 2010, 6, 149–163. [Google Scholar] [CrossRef] [PubMed]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef]
- Templeton, A.J.; Ace, O.; McNamara, M.G.; Al-Mubarak, M.; Vera-Badillo, F.E.; Hermanns, T.; Šeruga, B.; Ocana, A.; Tannock, I.F.; Amir, E. Prognostic role of platelet to lymphocyte ratio in solid tumors: A systematic review and meta-analysis. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1204–1212. [Google Scholar] [CrossRef] [PubMed]
- Chua, W.; Charles, K.A.; Baracos, V.E.; Clarke, S.J. Neutrophil/lymphocyte ratio predicts chemotherapy outcomes in patients with advanced colorectal cancer. Br. J. Cancer 2011, 104, 1288–1295. [Google Scholar] [CrossRef] [PubMed]
- Hamid, H.K.; Emile, S.H.; Davis, G.N. Prognostic significance of lymphocyte-to-monocyte and platelet-to-lymphocyte ratio in rectal cancer: A systematic review, meta-analysis, and meta-regression. Dis. Colon Rectum 2022, 65, 178–187. [Google Scholar] [CrossRef]
- Stojkovic Lalosevic, M.; Pavlovic Markovic, A.; Stankovic, S.; Stojkovic, M.; Dimitrijevic, I.; Radoman Vujacic, I.; Lalic, D.; Milovanovic, T.; Dumic, I.; Krivokapic, Z. Combined diagnostic efficacy of neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and mean platelet volume (MPV) as biomarkers of systemic inflammation in the diagnosis of colorectal cancer. Dis. Markers 2019, 2019, 6036979. [Google Scholar] [CrossRef]
- Lu, X.; Wan, J.; Shi, H. Platelet-to-lymphocyte and neutrophil-to-lymphocyte ratios are associated with the efficacy of immunotherapy in stage III/IV non-small cell lung cancer. Oncol. Lett. 2022, 24, 266. [Google Scholar] [CrossRef]
- Guo, G.; Chen, X.; Cai, X.; Chen, Y.; Wang, H.; Fan, L.; Bai, L.; Qiu, H.; Zhang, B. Inflammation-based markers can predict the prognosis of geriatric patients with metastatic colorectal cancer receiving first-line chemotherapy. Transl. Cancer Res. 2019, 8, 1137. [Google Scholar] [CrossRef]
- Gu, L.; Li, H.; Chen, L.; Ma, X.; Li, X.; Gao, Y.; Zhang, Y.; Xie, Y.; Zhang, X. Prognostic role of lymphocyte to monocyte ratio for patients with cancer: Evidence from a systematic review and meta-analysis. Oncotarget 2016, 7, 31926. [Google Scholar] [CrossRef]
- Tan, D.; Fu, Y.; Tong, W.; Li, F. Prognostic significance of lymphocyte to monocyte ratio in colorectal cancer: A meta-analysis. Int. J. Surg. 2018, 55, 128–138. [Google Scholar] [CrossRef]
- Song, W.; Wang, K.; Zhang, R.-j.; Zou, S.-b. Prognostic value of the lymphocyte monocyte ratio in patients with colorectal cancer: A meta-analysis. Medicine 2016, 95, e5540. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.C.; Chan, D.L.; Diakos, C.I.; Engel, A.; Pavlakis, N.; Gill, A.; Clarke, S.J. The lymphocyte-to-monocyte ratio is a superior predictor of overall survival in comparison to established biomarkers of resectable colorectal cancer. Ann. Surg. 2017, 265, 539–546. [Google Scholar] [CrossRef]
- Jia, W.; Yuan, L.; Ni, H.; Xu, B.; Zhao, P. Prognostic value of platelet-to-lymphocyte ratio, neutrophil-to-lymphocyte ratio, and lymphocyte-to-white blood cell ratio in colorectal cancer patients who received neoadjuvant chemotherapy. Technol. Cancer Res. Treat. 2021, 20, 15330338211034291. [Google Scholar] [CrossRef]
- Proctor, M.J.; Morrison, D.S.; Talwar, D.; Balmer, S.M.; Fletcher, C.D.; O’Reilly, D.S.J.; Foulis, A.K.; Horgan, P.G.; McMillan, D.C. A comparison of inflammation-based prognostic scores in patients with cancer. A Glasgow Inflammation Outcome Study. Eur. J. Cancer 2011, 47, 2633–2641. [Google Scholar] [CrossRef]
- Kamonvarapitak, T.; Matsuda, A.; Matsumoto, S.; Jamjittrong, S.; Sakurazawa, N.; Kawano, Y.; Yamada, T.; Suzuki, H.; Miyashita, M.; Yoshida, H. Preoperative lymphocyte-to-monocyte ratio predicts postoperative infectious complications after laparoscopic colorectal cancer surgery. Int. J. Clin. Oncol. 2020, 25, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Verras, G.-I.; Mulita, F. Butyrylcholinesterase levels correlate with surgical site infection risk and severity after colorectal surgery: A prospective single-center study. Front. Surg. 2024, 11, 1379410. [Google Scholar] [CrossRef] [PubMed]
- Fridman, W.H.; Pagès, F.; Sautès-Fridman, C.; Galon, J. The immune contexture in human tumours: Impact on clinical outcome. Nat. Rev. Cancer 2012, 12, 298–306. [Google Scholar] [CrossRef]
- Ceze, N.; Thibault, G.; Goujon, G.; Viguier, J.; Watier, H.; Dorval, E.; Lecomte, T. Pre-treatment lymphopenia as a prognostic biomarker in colorectal cancer patients receiving chemotherapy. Cancer Chemother. Pharmacol. 2011, 68, 1305–1313. [Google Scholar] [CrossRef]
- Shibutani, M.; Maeda, K.; Nagahara, H.; Iseki, Y.; Ikeya, T.; Hirakawa, K. Prognostic significance of the preoperative lymphocyte-to-monocyte ratio in patients with colorectal cancer. Oncol. Lett. 2017, 13, 1000–1006. [Google Scholar] [CrossRef]
- You, J.-F.; Hsu, Y.-J.; Chern, Y.-J.; Cheng, C.-C.; Jong, B.-K.; Liao, C.-K.; Hsieh, P.-S.; Hsu, H.-C.; Tsai, W.-S. Preoperative cancer inflammation prognostic index as a superior predictor of short-and long-term outcomes in patients with stage I–III colorectal cancer after curative surgery. Cancers 2022, 14, 6232. [Google Scholar] [CrossRef]
- Shibutani, M.; Maeda, K.; Nagahara, H.; Ohtani, H.; Sakurai, K.; Yamazoe, S.; Kimura, K.; Toyokawa, T.; Amano, R.; Tanaka, H. Prognostic significance of the lymphocyte-to-monocyte ratio in patients with metastatic colorectal cancer. World J. Gastroenterol. WJG 2015, 21, 9966. [Google Scholar] [CrossRef] [PubMed]
- Bowen, R.C.; Little, N.A.B.; Harmer, J.R.; Ma, J.; Mirabelli, L.G.; Roller, K.D.; Breivik, A.M.; Signor, E.; Miller, A.B.; Khong, H.T. Neutrophil-to-lymphocyte ratio as prognostic indicator in gastrointestinal cancers: A systematic review and meta-analysis. Oncotarget 2017, 8, 32171. [Google Scholar] [CrossRef] [PubMed]
- Guo, G.; Hu, X.; Gao, T.; Zhou, H.; Li, B.; Zhou, C.; Yu, B.; Wang, G. Potential impact of platelet-to-lymphocyte ratio on prognosis in patients with colorectal cancer: A systematic review and meta-analysis. Front. Surg. 2023, 10, 1139503. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Guo, X.; Wu, T.; Niu, K.; Ma, X. Prognostic significance of inflammation-based indexes in patients with stage III/IV colorectal cancer after adjuvant chemoradiotherapy. Medicine 2019, 98, e14420. [Google Scholar] [CrossRef]
- Nishijima, T.F.; Muss, H.B.; Shachar, S.S.; Tamura, K.; Takamatsu, Y. Prognostic value of lymphocyte-to-monocyte ratio in patients with solid tumors: A systematic review and meta-analysis. Cancer Treat Rev. 2015, 41, 971–978. [Google Scholar] [CrossRef]
- Shimura, T.; Shibata, M.; Gonda, K.; Hayase, S.; Sakamoto, W.; Okayama, H.; Fujita, S.; Saito, M.; Momma, T.; Ohki, S.; et al. Prognostic impact of preoperative lymphocyte-to-monocyte ratio in patients with colorectal cancer with special reference to myeloid-derived suppressor cells. Fukushima J. Med. Sci. 2018, 64, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.N.; Liu, P.P.; Liu, D.Y.; Peng, J.W.; Xiao, J.J.; Xia, Z.J. Prognostic significance of the pre-chemotherapy lymphocyte-to-monocyte ratio in patients with previously untreated metastatic colorectal cancer receiving FOLFOX chemotherapy. Chin. J. Cancer 2016, 35, 1–9. [Google Scholar] [CrossRef]
- Gawiński, C.; Hołdakowska, A.; Wyrwicz, L. Correlation between Lymphocyte-to-Monocyte Ratio (LMR), Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR) and Extramural Vascular Invasion (EMVI) in Locally. Adv. Rectal Cancer Curr. Oncol. 2023, 30, 545–558. [Google Scholar] [CrossRef]
- Fülöp, Z.Z.; Fülöp, R.L.; Gurzu, S.; Bara, T., Jr.; Tímár, J.; Drágus, E.; Jung, I. Prognostic Impact of the Neutrophil-to-Lymphocyte and Lymphocyte-to-Monocyte Ratio, in Patients with Rectal Cancer: A Retrospective Study of 1052 Patients. J. Pers. Med. 2020, 10, 173. [Google Scholar] [CrossRef]
- Gawiński, C.; Michalski, W.; Mróz, A.; Wyrwicz, L. Correlation between Lymphocyte-to-Monocyte Ratio (LMR), Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR) and Tumor-Infiltrating Lymphocytes (TILs) in Left-Sided Colorectal Cancer Patients. Biology 2022, 11, 385. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| LMR Cut-off | Hazard Ratio (95% Cl) | p-Value | |
|---|---|---|---|
| ROC | 25.96 | 0.726 (0.535–0.986) | 0.041 |
| Median | 24.72 | 0.638 (0.470–0.867) | 0.004 |
| Overall, n, % | LMR-L, n, % | LMR-H, n, % | p-Value | |
|---|---|---|---|---|
| Gender | 0.575 | |||
| Male | 114, 55.9 | 42, 42 | 48, 46.2 | |
| Female | 90, 44.1 | 58, 58 | 56, 53.8 | |
| Age(years) | 0.108 | |||
| <65 | 132, 64.7 | 59, 59 | 73, 70.2 | |
| ≥65 | 72, 35.3 | 41, 41 | 31, 29.8 | |
| Histological subtype | 0.720 | |||
| Adenocarcinoma | 166, 81.4 | 80, 80 | 86, 82.7 | |
| Mucinous adenocarcinoma | 38, 18.6 | 20, 20 | 18, 17.3 | |
| Tumor location | 0.725 | |||
| Right-side | 40, 19.6 | 21, 21 | 19, 18.3 | |
| Left-side | 164, 80.4 | 79, 79 | 85, 81.7 | |
| RAS | 0.776 | |||
| Wild | 121, 59.3 | 58, 58 | 63, 60.6 | |
| Mutant | 83, 40.7 | 42, 42 | 41, 39.4 | |
| Histological grade | 0.938 | |||
| 1–2 | 187, 91.7 | 92, 92 | 95, 91.3 | |
| ≥3 | 17, 8.3 | 8, 8 | 9, 8.7 | |
| T-Stage | 0.655 | |||
| 1–3 | 138, 67.6 | 66, 66 | 72, 69.2 | |
| ≥4 | 66, 32.4 | 34, 34 | 32, 30.8 | |
| N Stage | 0.607 | |||
| Negative | 43, 21.1 | 23, 23 | 20, 19.2 | |
| Positive | 161, 78.9 | 77, 77 | 84, 80.8 | |
| LVI | 0.476 | |||
| No | 81, 39.7 | 37, 37 | 44, 42.3 | |
| Yes | 123, 60.3 | 63, 63 | 60, 57.7 | |
| PNI | 0.485 | |||
| No | 111, 54.4 | 57, 57 | 54, 51.9 | |
| Yes | 93, 45.6 | 43, 43 | 50, 48.1 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Variable | Hazard Ratio | 95% Cl | p Value | Hazard Ratio | 95% Cl | p Value |
| Gender | 0.98 | 0.727–1.337 | 0.928 | |||
| Male | ||||||
| Female | ||||||
| Age(years) | 1.45 | 1.060–1.997 | 0.020 | 1.57 | 1.127–2.199 | 0.008 |
| <65 | ||||||
| ≥65 | ||||||
| Histological subtype | 0.69 | 0.472–1.024 | 0.066 | |||
| Adenocarcinoma | ||||||
| Mucinous adenocarcinoma | ||||||
| Tumor location | 0.69 | 0.482–1.012 | 0.058 | |||
| Right-side | ||||||
| Left-side | ||||||
| RAS | 1.43 | 1.054–1.944 | 0.022 | 1.46 | 1.070–1.992 | 0.017 |
| Wild | ||||||
| Mutant | ||||||
| Histological grade | 1.98 | 1.143–3.452 | 0.015 | 2.07 | 1.174–3.657 | 0.012 |
| 1–2 | ||||||
| 3 | ||||||
| T Stage | 1.34 | 0.970–1.850 | 0.076 | |||
| 1–3 | ||||||
| ≥4 | ||||||
| N Stage | 1.52 | 1.039–2.239 | 0.031 | 1.65 | 1.104–2.481 | 0.015 |
| Negative | ||||||
| Positive | ||||||
| LVI | 1.42 | 1.037–1.951 | 0.029 | 1.30 | 0.947–1.808 | 0.103 |
| No | ||||||
| Yes | ||||||
| PNI | 1.34 | 0.985–1.824 | 0.062 | |||
| No | ||||||
| Yes | ||||||
| LMR | 0.63 | 0.470–0.867 | 0.004 | 0.66 | 0.488–0.916 | 0.012 |
| H | ||||||
| L |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Variable | Hazard Ratio | 95% Cl | p Value | Hazard Ratio | 95% Cl | p Value |
| Gender | 1.01 | 0.767–1.337 | 0.929 | |||
| Male | ||||||
| Female | ||||||
| Age (years) | 1.27 | 0.950–1.699 | 0.107 | |||
| <65 | ||||||
| ≥65 | ||||||
| Histological subtype | 0.86 | 0.606–1.237 | 0.429 | |||
| Adenocarcinoma | ||||||
| Mucinous adenocarcinoma | ||||||
| Tumor location | 0.79 | 0.559–1.121 | 0.188 | |||
| Right-side | ||||||
| Left-side | ||||||
| RAS | 1.37 | 1.037–1.823 | 0.027 | 1.31 | 0.984–1.745 | 0.064 |
| Wild | ||||||
| Mutant | ||||||
| Histological grade | 2.16 | 1.309–3.594 | 0.003 | 1.81 | 1.073–3.067 | 0.026 |
| 1–2 | ||||||
| 3 | ||||||
| T Stage | 1.57 | 1.164–2.125 | 0.003 | 1.58 | 1.154–2.163 | 0.004 |
| 1–3 | ||||||
| ≥4 | ||||||
| N Stage | 1.49 | 1.058–2.120 | 0.023 | 1.51 | 1.061–2.173 | 0.022 |
| Negative | ||||||
| Positive | ||||||
| LVI | 1.39 | 1.046–1.848 | 0.023 | 1.26 | 0.942–1.695 | 0.118 |
| No | ||||||
| Yes | ||||||
| PNI | 1.24 | 0.939–1.645 | 0.128 | |||
| No | ||||||
| Yes | ||||||
| LMR | 0.66 | 0.506–0.885 | 0.005 | 0.68 | 0.518–0.909 | 0.009 |
| H | ||||||
| L |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Özkan, O.; Peker, P.; Geçgel, A.; Göker, E. Prognostic Value of Preoperative Lymphocyte-to-Monocyte Ratio in Patients with Recurrent Colorectal Cancer. Medicina 2025, 61, 707. https://doi.org/10.3390/medicina61040707
Özkan O, Peker P, Geçgel A, Göker E. Prognostic Value of Preoperative Lymphocyte-to-Monocyte Ratio in Patients with Recurrent Colorectal Cancer. Medicina. 2025; 61(4):707. https://doi.org/10.3390/medicina61040707
Chicago/Turabian StyleÖzkan, Oğuzcan, Pınar Peker, Aslı Geçgel, and Erdem Göker. 2025. "Prognostic Value of Preoperative Lymphocyte-to-Monocyte Ratio in Patients with Recurrent Colorectal Cancer" Medicina 61, no. 4: 707. https://doi.org/10.3390/medicina61040707
APA StyleÖzkan, O., Peker, P., Geçgel, A., & Göker, E. (2025). Prognostic Value of Preoperative Lymphocyte-to-Monocyte Ratio in Patients with Recurrent Colorectal Cancer. Medicina, 61(4), 707. https://doi.org/10.3390/medicina61040707