

Efficacy of Quadratus Lumborum Block for Postoperative Pain Management in Single-Port Total Laparoscopic Hysterectomy: A Randomized Observer-Blinded Controlled Trial

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
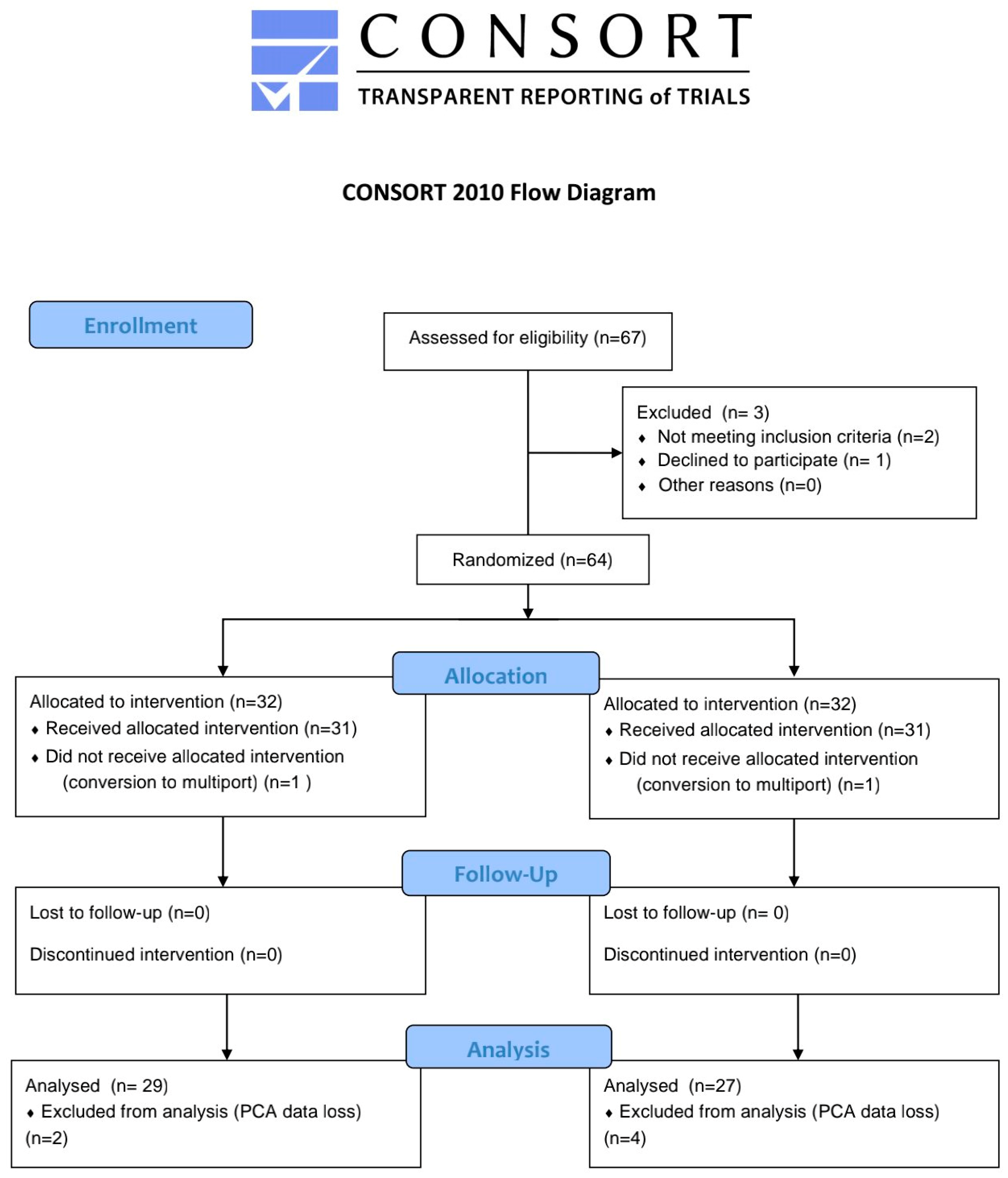
2.2. Randomization
2.3. Intraoperative Management
2.4. Surgical Technique
2.5. Block Technique
2.6. Postoperative Management
2.7. Outcomes
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Neill, A.; Lirk, P. Multimodal Analgesia. Anesth. Clin. 2022, 40, 455–468. [Google Scholar] [CrossRef] [PubMed]
- Wick, E.C.; Grant, M.C.; Wu, C.L. Postoperative Multimodal Analgesia Pain Management with Nonopioid Analgesics and Techniques: A Review. JAMA Surg. 2017, 152, 691–697. [Google Scholar] [CrossRef] [PubMed]
- Beverly, A.; Kaye, A.D.; Ljungqvist, O.; Urman, R.D. Essential Elements of Multimodal Analgesia in Enhanced Recovery After Surgery (ERAS) Guidelines. Anesth. Clin. 2017, 35, e115–e143. [Google Scholar] [CrossRef]
- Chen, Y.K.; Boden, K.A.; Schreiber, K.L. The role of regional anaesthesia and multimodal analgesia in the prevention of chronic postoperative pain: A narrative review. Anaesthesia 2021, 76 (Suppl. S1), 8–17. [Google Scholar] [CrossRef]
- Chin, K.J.; McDonnell, J.G.; Carvalho, B.; Sharkey, A.; Pawa, A.; Gadsden, J. Essentials of Our Current Understanding: Abdominal Wall Blocks. Reg. Anesth. Pain Med. 2017, 42, 133–183. [Google Scholar] [CrossRef]
- Ueshima, H.; Otake, H.; Lin, J.A. Ultrasound-Guided Quadratus Lumborum Block: An Updated Review of Anatomy and Techniques. Biomed Res. Int. 2017, 2017, 2752876. [Google Scholar] [CrossRef] [PubMed]
- Blanco, R.; McDonnell, J. Optimal point of injection: The quadratus lumborum type I and II blocks. Anesthesia 2013, 68, 4. [Google Scholar]
- Børglum, J.; Moriggl, B.; Jensen, K.; Lønnqvist, P.A.; Christensen, A.F.; Sauter, A.; Bendtsen, T.F. Ultrasound-guided transmuscular quadratus lumborum blockade. Br. J. Anaesth. 2013, 111. [Google Scholar] [CrossRef]
- Carline, L.; McLeod, G.A.; Lamb, C. A cadaver study comparing spread of dye and nerve involvement after three different quadratus lumborum blocks. Br. J. Anaesth. 2016, 117, 387–394. [Google Scholar] [CrossRef]
- Elsharkawy, H.; El-Boghdadly, K.; Barrington, M. Quadratus Lumborum Block: Anatomical Concepts, Mechanisms, and Techniques. Anesthesiology 2019, 130, 322–335. [Google Scholar] [CrossRef] [PubMed]
- Freys, J.C.; Bigalke, S.M.; Mertes, M.; Lobo, D.N.; Pogatzki-Zahn, E.M.; Freys, S.M. Perioperative pain management for appendicectomy: A systematic review and Procedure-specific Postoperative Pain Management recommendations. Eur. J. Anaesthesiol. 2024, 41, 174–187. [Google Scholar] [CrossRef]
- Jin, Z.; Liu, J.; Li, R.; Gan, T.J.; He, Y.; Lin, J. Single injection Quadratus Lumborum block for postoperative analgesia in adult surgical population: A systematic review and meta-analysis. J. Clin. Anesth. 2020, 62, 109715. [Google Scholar] [CrossRef] [PubMed]
- Lirk, P.; Thiry, J.; Bonnet, M.P.; Joshi, G.P.; Bonnet, F. Pain management after laparoscopic hysterectomy: Systematic review of literature and PROSPECT recommendations. Reg. Anesth. Pain Med. 2019, 44, 425–436. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.P.; Davies, A.; McPherson, M.L.; Reddy, A.; Paice, J.A.; Roeland, E.; Walsh, D.; Mercadante, S.; Case, A.; Arnold, R.; et al. Opioid analgesic dose and route conversion ratio studies: A scoping review to inform an eDelphi guideline. Support. Care Cancer 2024, 32, 542. [Google Scholar] [CrossRef] [PubMed]
- Pereira, J.; Lawlor, P.; Vigano, A.; Dorgan, M.; Bruera, E. Equianalgesic dose ratios for opioids. a critical review and proposals for long-term dosing. J. Pain Symptom Manag. 2001, 22, 672–687. [Google Scholar] [CrossRef]
- She, H.; Jiang, P.; Zhu, J.; Zhou, Y.; Wang, Y.; Kan, M.; Wu, J. Comparison of the analgesic effect of quadratus lumborum block and epidural block in open uterine surgery: A randomized controlled trial. Minerva Anestesiol. 2021, 87, 414–422. [Google Scholar] [CrossRef]
- Bak, H.; Bang, S.; Yoo, S.; Kim, S.; Lee, S.Y. Continuous quadratus lumborum block as part of multimodal analgesia after total hip arthroplasty: A case report. Korean J. Anesthesiol. 2020, 73, 158–162. [Google Scholar] [CrossRef]
- Hansen, C.; Dam, M.; Nielsen, M.V.; Tanggaard, K.B.; Poulsen, T.D.; Bendtsen, T.F.; Børglum, J. Transmuscular quadratus lumborum block for total laparoscopic hysterectomy: A double-blind, randomized, placebo-controlled trial. Reg. Anesth. Pain Med. 2021, 46, 25–30. [Google Scholar] [CrossRef]
- She, H.; Qin, Y.; Peng, W.; Zhou, Y.; Dai, Y.; Wang, Y.; Jiang, P.; Wu, J. Anterior Quadratus Lumborum Block for Total Laparoscopic Hysterectomy: A Randomized, Double-Blind, Placebo-Controlled Trial. Clin. J. Pain 2023, 39, 571–579. [Google Scholar] [CrossRef]
- Choi, J.B.; Kang, K.; Song, M.K.; Seok, S.; Kim, Y.H.; Kim, J.E. Pain Characteristics after Total Laparoscopic Hysterectomy. Int. J. Med. Sci. 2016, 13, 562–568. [Google Scholar] [CrossRef]
- Boezaart, A.P.; Smith, C.R.; Chembrovich, S.; Zasimovich, Y.; Server, A.; Morgan, G.; Theron, A.; Booysen, K.; Reina, M.A. Visceral versus somatic pain: An educational review of anatomy and clinical implications. Reg. Anesth. Pain Med. 2021, 46, 629–636. [Google Scholar] [CrossRef]
- Willard, F.H.; Schuenke, M.D. The neuroanatomy of female pelvic pain. In Pain in Women: A Clinical Guide; Springer: Berlin/Heidelberg, Germany, 2012; pp. 17–58. [Google Scholar]
- Astruc, A.; Roux, L.; Robin, F.; Sall, N.R.; Dion, L.; Lavoué, V.; Legendre, G.; Leveque, J.; Bessede, T.; Bertrand, M.; et al. Advanced Insights into Human Uterine Innervation: Implications for Endometriosis and Pelvic Pain. J. Clin. Med. 2024, 13, 1433. [Google Scholar] [CrossRef]
- Aurore, V.; Röthlisberger, R.; Boemke, N.; Hlushchuk, R.; Bangerter, H.; Bergmann, M.; Imboden, S.; Mueller, M.D.; Eppler, E.; Djonov, V. Anatomy of the female pelvic nerves: A macroscopic study of the hypogastric plexus and their relations and variations. J. Anat. 2020, 237, 487–494. [Google Scholar] [CrossRef]
- Struller, F.; Weinreich, F.J.; Horvath, P.; Kokkalis, M.K.; Beckert, S.; Königsrainer, A.; Reymond, M.A. Peritoneal innervation: Embryology and functional anatomy. Pleura Peritoneum 2017, 2, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Yan Zhao, Y.; Xin, W.; Luo, X. Post-laparoscopic Shoulder Pain Management: A Narrative Review. Curr. Pain Headache Rep. 2025, 29, 18. [Google Scholar] [CrossRef]
- Flynn, D.N.; Rojas, A.F.; Low, A.L.; Bullard, T.L.; Stearns, J.; Vishnevsky, B.M.; Armbruster, J.R.; Nanda, M.; Stander, S.; Schoenherr, J.W.; et al. The road not taken: An investigation of injectate spread between the thoracic paravertebral space and the quadratus lumborum. J. Clin. Anesth. 2022, 79, 110697. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Sadeghi, N.; Wahal, C.; Gadsden, J.; Grant, S.A. Quadratus Lumborum Spares Paravertebral Space in Fresh Cadaver Injection. Anesth. Analg. 2017, 125, 708–709. [Google Scholar] [CrossRef]
- Ishio, J.; Komasawa, N.; Kido, H.; Minami, T. Evaluation of ultrasound-guided posterior quadratus lumborum block for postoperative analgesia after laparoscopic gynecologic surgery. J. Clin. Anesth. 2017, 41, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Murouchi, T.; Iwasaki, S.; Yamakage, M. Quadratus Lumborum Block: Analgesic Effects and Chronological Ropivacaine Concentrations After Laparoscopic Surgery. Reg. Anesth. Pain Med. 2016, 41, 146–150. [Google Scholar] [CrossRef]
- Naaz, S.; Kumar, R.; Ozair, E.; Sahay, N.; Asghar, A.; Jha, S.; Akhil, V.P. Ultrasound Guided Quadratus Lumborum Block Versus Transversus Abdominis Plane Block for Post-operative Analgesia in Patients Undergoing Total Abdominal Hysterectomy. Turk. J. Anaesthesiol. Reanim. 2021, 49, 357–364. [Google Scholar] [CrossRef]
- Shukla, U.; Yadav, U.; Duggal, J. A Comparative Study of Ultrasound-Guided Quadratus Lumborum Block and Transversus Abdominis Plane Block for Postoperative Analgesia Following Total Abdominal Hysterectomy. Cureus 2023, 15, e36412. [Google Scholar] [CrossRef] [PubMed]
- Yousef, N.K. Quadratus Lumborum Block versus Transversus Abdominis Plane Block in Patients Undergoing Total Abdominal Hysterectomy: A Randomized Prospective Controlled Trial. Anesth. Essays. Res. 2018, 12, 742–747. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Zheng, L.; Zhang, J.; Zhu, X.; Pan, L.; Zhang, Y.; Wang, Q.; Shi, K. Transmuscular quadratus lumborum block versus oblique subcostal transversus abdominis plane block for analgesia in laparoscopic hysterectomy: A randomised single-blind trial. BMJ Open 2021, 11, e043883. [Google Scholar] [CrossRef]
- Jadon, A.; Ahmad, A.; Sahoo, R.K.; Sinha, N.; Chakraborty, S.; Bakshi, A. Efficacy of transmuscular quadratus lumborum block in the multimodal regimen for postoperative analgesia after total laparoscopic hysterectomy: A prospective randomised double-blinded study. Indian J. Anaesth. 2021, 65, 362–368. [Google Scholar] [CrossRef] [PubMed]
- Hebbard, P. Subcostal Transversus Abdominis Plane Block Under Ultrasound Guidance. Anesth. Analg. 2008, 106, 674–675. [Google Scholar] [CrossRef]

{kind=link}
| Control (n = 29) | QLB (n = 27) | |
|---|---|---|
| Age (yr) | 47.5 ± 4.6 | 48.5 ± 8.7 |
| Height (cm) | 158.1 ± 4.2 | 161.7 ± 5.4 |
| Weight (kg) | 62.2 ± 8.8 | 64.0 ± 9.8 |
| BMI (kg/m2) | 24.3 [22.3, 27.5] | 24.4 [22.0, 26.8] |
| Operation time (min) | 145 [112.5, 199] | 161 [140, 184] |
| Control Group (n = 29) | QLB Group (n = 27) | Mean Difference (95% CI) | p-Value | |
|---|---|---|---|---|
| Interval opioid consumption (mcg) | ||||
| 0 h–PACU | 55.5 [32, 79.1] | 33.7 [25, 74.5] | 21.3 (−15.1, 25.8) | 0.579 |
| PACU–2 h | 58.3 [31.8, 86.4] | 71.5 [27.5, 133.6] | −13.2 (−48.8, 10.4) | 0.206 |
| 2–4 h | 34 [0, 64.9] | 32.6 [0, 79.2] | 1.4 (−22.4, 15.4) | 0.686 |
| 4–8 h | 62.7 [0, 100.1] | 33.7 [0, 97.3] | 29 (−21.8, 53.3) | 0.462 |
| 8–12 h | 29.2 [0, 128.3] | 32.6 [0, 79.2] | −3.4 (−23.1, 60.2) | 0.410 |
| 12–18 h | 54.6 [0, 154.2] | 64 [0, 158.4] | −9.4 (−61.2, 45.8) | 0.841 |
| 18–24 h | 50.2 [0, 86.4] | 28.9 [0, 63.1] | 21.3 (−30.8, 87.9) | 0.373 |
| 24–32 h | 65.6 [0, 163.3] | 0 [0, 106.2] | 65.6 (−3.51, 87.5) | 0.104 |
| 32–48 h | 0 [0, 25.3] | 0 [0, 30.2] | 0 (−9.6, 20.2) | 0.517 |
| Cumulative opioid consumption (mcg) | ||||
| PACU | 55.5 [32, 79.1] | 33.7 [25, 74.5] | 21.3 (−15.1, 25.8) | 0.579 |
| 2 h | 108 [69.4, 163.6] | 107.2 [40.5, 196.6] | 0.8 (−54.8, 27) | 0.529 |
| 4 h | 144.4 [109.4, 228.1] | 153.5 [106.1, 252.4] | −9.1 (−67.6, 24.8) | 0.406 |
| 8 h | 208.5 [120, 315.9] | 239.9 [106.1, 377.6] | −31.4 (−76.2, 66.7) | 0.850 |
| 12 h | 305.5 [145, 412] | 239.9 [128, 441.2] | 65.6 (−85.5, 110.3) | 0.836 |
| 18 h | 404.5 [163.5, 508.2] | 317.8 [195.3, 475.4] | 86.7 (−135.5, 143.5) | 0.911 |
| 24 h | 470 [191.6, 648.1] | 342.8 [220, 651] | 127.2 (−151.8, 204.1) | 0.714 |
| 32 h | 548.7 [200.4, 878.9] | 396.7 [228.5, 712.8] | 152 (−126.7, 267.1) | 0.456 |
| 48 h | 548.7 [200.4, 961.8] | 424.1 [228.5, 712.8] | 124.6 (−128.6, 297.3) | 0.441 |
| Control Group (n = 29) | QLB Group (n = 27) | p-Value | |
|---|---|---|---|
| Pain score (VAS) | |||
| PACU | 3 [2, 3] | 2 [2, 3] | 0.395 |
| 2 h | 2 [2, 3] | 2 [2, 3] | 0.919 |
| 4 h | 2 [2, 3] | 2 [2, 3] | 0.723 |
| 8 h | 2 [2, 2] | 2 [2, 3] | 0.772 |
| 12 h | 2 [2, 3] | 2 [2, 2] | 0.623 |
| 18 h | 2 [2, 3] | 2 [2, 3] | 0.538 |
| 24 h | 2 [2, 2] | 2 [2, 3] | 0.755 |
| 32 h | 2 [2, 3] | 2 [2, 2] | 0.529 |
| 48 h | 2 [2, 2] | 2 [2, 2] | 0.791 |
| Time to first bolus (min) | 16 [10, 26.5] | 14 [10, 26] | 0.204 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, J.; Bang, S.; Lee, S.; Lee, Y.; Shin, H.-J.; Park, Y. Efficacy of Quadratus Lumborum Block for Postoperative Pain Management in Single-Port Total Laparoscopic Hysterectomy: A Randomized Observer-Blinded Controlled Trial. Medicina 2025, 61, 702. https://doi.org/10.3390/medicina61040702
Chung J, Bang S, Lee S, Lee Y, Shin H-J, Park Y. Efficacy of Quadratus Lumborum Block for Postoperative Pain Management in Single-Port Total Laparoscopic Hysterectomy: A Randomized Observer-Blinded Controlled Trial. Medicina. 2025; 61(4):702. https://doi.org/10.3390/medicina61040702
Chicago/Turabian StyleChung, Jihyun, Seunguk Bang, Sangmook Lee, Youngin Lee, Hyun-Jung Shin, and Yoonji Park. 2025. "Efficacy of Quadratus Lumborum Block for Postoperative Pain Management in Single-Port Total Laparoscopic Hysterectomy: A Randomized Observer-Blinded Controlled Trial" Medicina 61, no. 4: 702. https://doi.org/10.3390/medicina61040702
APA StyleChung, J., Bang, S., Lee, S., Lee, Y., Shin, H.-J., & Park, Y. (2025). Efficacy of Quadratus Lumborum Block for Postoperative Pain Management in Single-Port Total Laparoscopic Hysterectomy: A Randomized Observer-Blinded Controlled Trial. Medicina, 61(4), 702. https://doi.org/10.3390/medicina61040702