
Non-Invasive Monitoring of Intracranial Pressure Pulse Waves from Closed Eyelids in Patients with Normal-Tension Glaucoma

 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
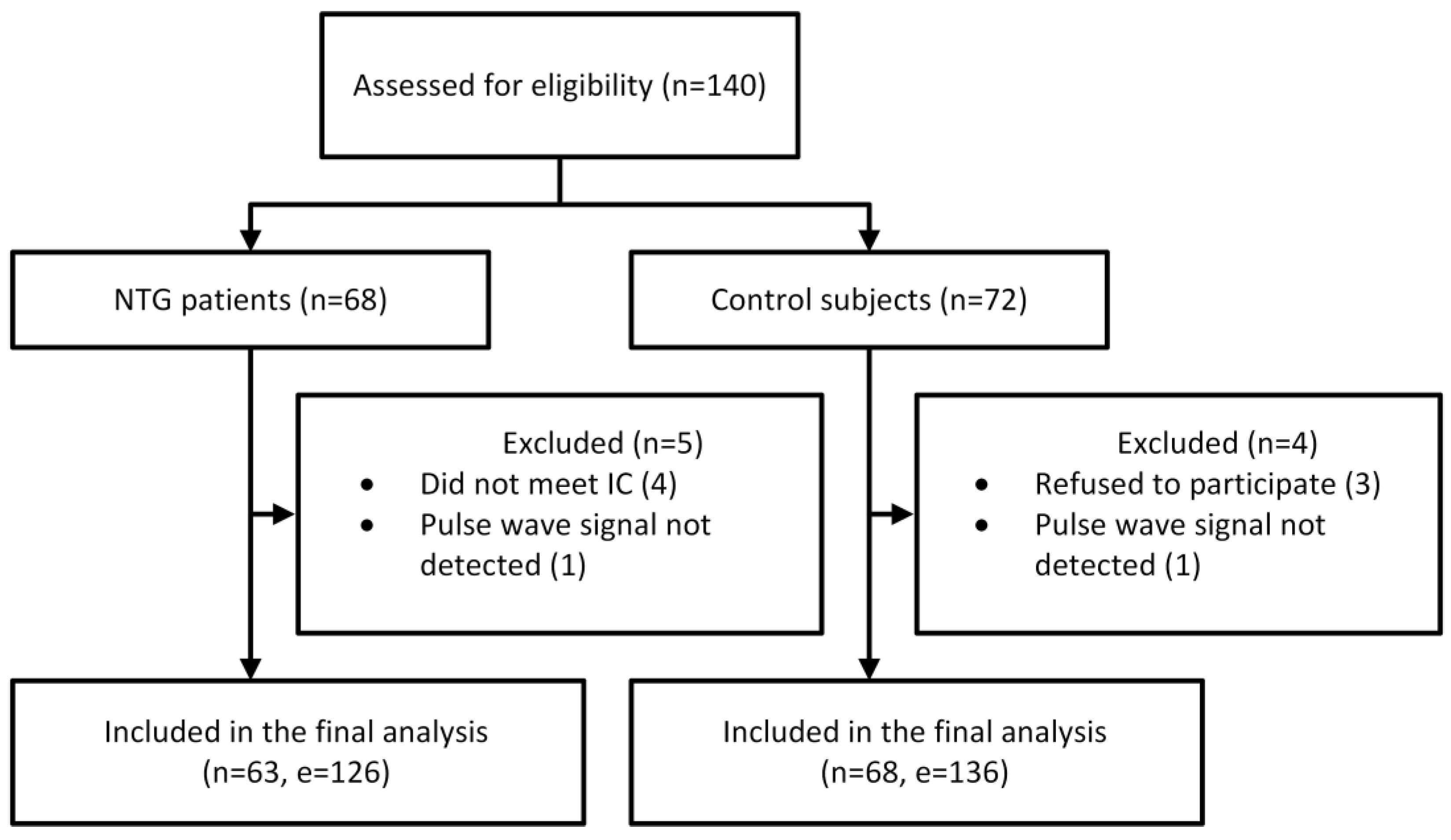
2.1. Study Design and Participants
- Refusal to participate;
- Age under 25 or over 85 years;
- Pregnancy or breastfeeding;
- Allergy or sensitivity to local anesthetics;
- Eye diseases that could distort study results;
- History of orbital or ocular trauma;
- Previous ocular surgery;
- Acute or chronic, currently exacerbated respiratory diseases;
- Decompensated cardiovascular diseases (e.g., a second- or third-degree atrioventricular block or cardiogenic shock);
- Decompensated diabetes mellitus;
- History of neurological disorders or mental illnesses.
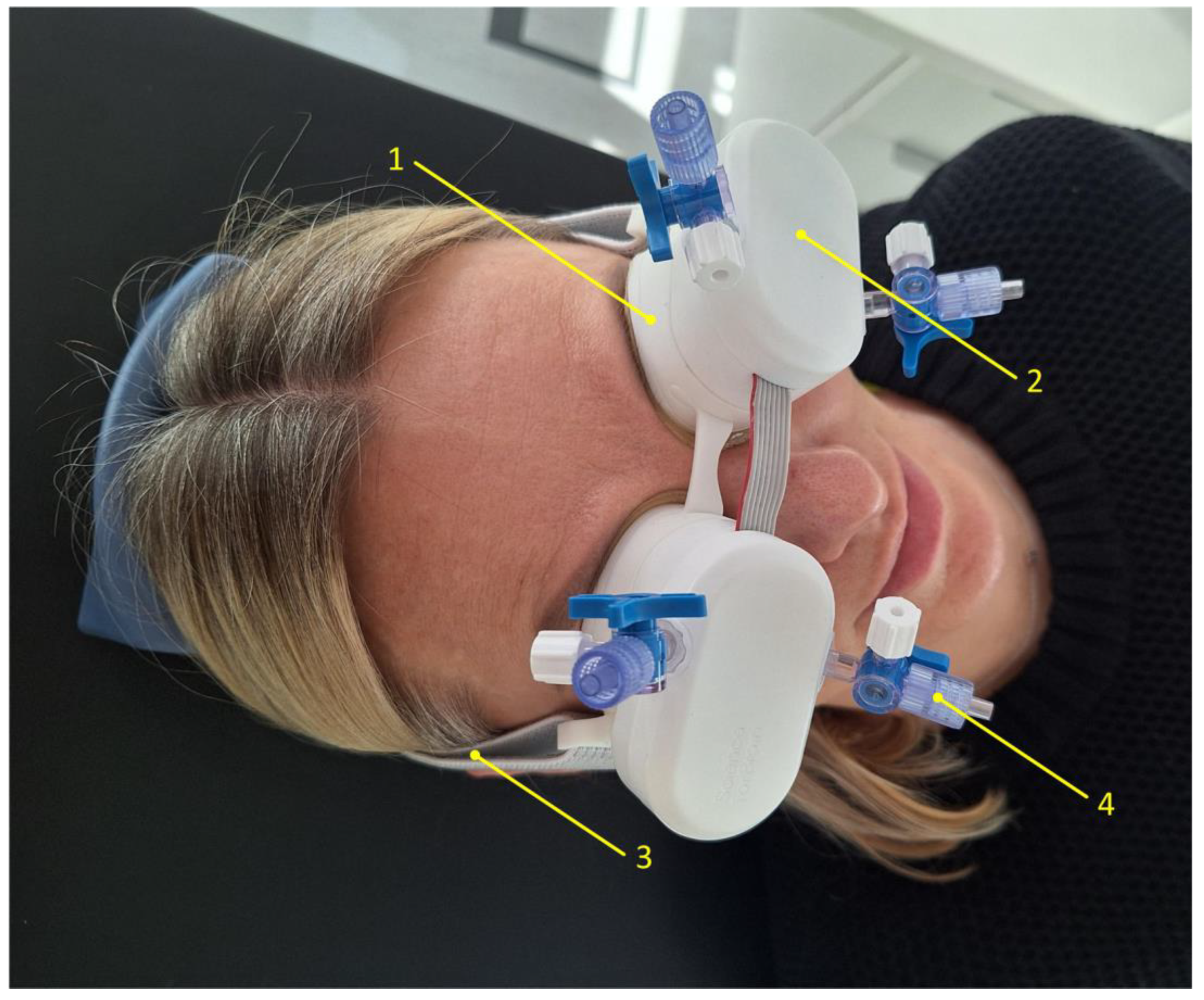
2.2. Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gupta, D.; Chen, P.P. Glaucoma. Am. Fam. Physician. 2016, 93, 668–674. [Google Scholar] [PubMed]
- Allison, K.; Patel, D.; Alabi, O. Epidemiology of Glaucoma: The Past, Present, and Predictions for the Future. Cureus. 2020, 12, e11686. [Google Scholar] [CrossRef] [PubMed]
- Siaudvytyte, L.; Januleviciene, I.; Ragauskas, A.; Bartusis, L.; Meiliuniene, I.; Siesky, B.; Harris, A. The difference in translaminar pressure gradient and neuroretinal rim area in glaucoma and healthy subjects. J. Ophthalmol. 2014, 2014, 937360. [Google Scholar] [CrossRef]
- Harasymowycz, P.; Birt, C.; Gooi, P.; Heckler, L.; Hutnik, C.; Jinapriya, D.; Shuba, L.; Yan, D.; Day, R. MedicaWl Management of Glaucoma in the 21st Century from a Canadian Perspective. J. Ophthalmol. 2016, 2016, 6509809. [Google Scholar] [CrossRef]
- Canadian Ophthalmological Society Glaucoma Clinical Practice Guideline Expert Committee; Canadian Ophthalmological Society. Canadian Ophthalmological Society evidence-based clinical practice guidelines for the management of glaucoma in the adult eye [published correction appears in Can. J. Ophthalmol. 2009, 44, 477]. Can. J. Ophthalmol. 2009, 44 (Suppl. S1), S7–S93. [Google Scholar] [CrossRef]
- Khalil, T.; Khalil, S.; Syed, A.M. Review of Machine Learning techniques for glaucoma detection and prediction. In Proceedings of the 2014 Science and Information Conference, Seoul, Republic of Korea, 6–9 May 2014; pp. 438–442. [Google Scholar]
- Srivastava, N.; Chandra, M.; Nitesh. A review exploring the dynamic of aqueous humor and glaucoma: Open & close angle perspective. Eur. J. Pharm. Med. Res. 2024, 11, 233–248. [Google Scholar]
- Johnson, M.; McLaren, J.W.; Overby, D.R. Unconventional aqueous humor outflow: A review. Exp. Eye Res. 2017, 158, 94–111. [Google Scholar] [CrossRef]
- Weinreb, R.N.; Aung, T.; Medeiros, F.A. The pathophysiology and treatment of glaucoma: A review. JAMA 2014, 311, 1901–1911. [Google Scholar] [CrossRef]
- Dietze, J.; Blair, K.; Zeppieri, M.; Havens, S.J. Glaucoma. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar] [PubMed]
- Zhang, N.; Wang, J.; Li, Y.; Jiang, B. Prevalence of primary open angle glaucoma in the last 20 years: A meta-analysis and systematic review. Sci Rep. 2021, 11, 13762. [Google Scholar] [CrossRef]
- Tham, Y.C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.-Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef]
- Mroczkowska, S.; Benavente-Perez, A.; Negi, A.; Sung, V.; Patel, S.R.; Gherghel, D. Primary open-angle glaucoma vs normal-tension glaucoma: The vascular perspective. JAMA Ophthalmol. 2013, 131, 36–43. [Google Scholar] [CrossRef]
- Mi, X.S.; Yuan, T.F.; So, K.F. The current research status of normal tension glaucoma. Clin. Interv. Aging 2014, 9, 1563–1571. [Google Scholar] [CrossRef] [PubMed]
- Killer, H.E.; Pircher, A. Normal tension glaucoma: Review of current understanding and mechanisms of the pathogenesis. Eye 2018, 32, 924–930. [Google Scholar] [CrossRef]
- Adeghate, J.; Rahmatnejad, K.; Waisbourd, M.; Katz, L.J. Intraocular pressure-independent management of normal tension glaucoma. Surv. Ophthalmol. 2019, 64, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Wiggs, J.L.; Pasquale, L.R. Genetics of glaucoma. Hum. Mol. Genet. 2017, 26, R21–R27. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.J. Normal tension glaucoma in Asia: Epidemiology, pathogenesis, diagnosis, and management. Taiwan J. Ophthalmol. 2020, 10, 250–254. [Google Scholar] [CrossRef]
- Bonomi, L.; Marchini, G.; Marraffa, M.; Bernardi, P.; De Franco, I.; Perfetti, S.; Varotto, A.; Tenna, V. Prevalence of glaucoma and intraocular pressure distribution in a defined population. The Egna-Neumarkt Study. Ophthalmology 1998, 105, 209–215. [Google Scholar] [CrossRef]
- Iwase, A.; Suzuki, Y.; Araie, M.; Yamamoto, T.; Abe, H.; Shirato, S.; Kuwayama, Y.; Mishima, H.K.; Shimizu, H.; Tomita, G.; et al. The prevalence of primary open-angle glaucoma in Japanese: The Tajimi Study. Ophthalmology 2004, 111, 1641–1648. [Google Scholar] [CrossRef]
- Lee, J.W.Y.; Chan, P.P.; Zhang, X.; Chen, L.J.; Jonas, J.B. Latest Developments in Normal-Pressure Glaucoma: Diagnosis, Epidemiology, Genetics, Etiology, Causes and Mechanisms to Management. Asia Pac. J. Ophthalmol. 2019, 8, 457–468. [Google Scholar] [CrossRef]
- Singh, K.; Dion, C.; Wajszilber, M.; Ozaki, T.; Lesk, M.R.; Costantino, S. Measurement of ocular fundus pulsation in healthy subjects using a novel Fourier-domain optical coherence tomography. Invest. Ophthalmol. Vis. Sci. 2011, 52, 8927–8932. [Google Scholar] [CrossRef]
- Singh, K.; Dion, C.; Godin, A.G.; Lorghaba, F.; Descovich, D.; Wajszilber, M.; Ozaki, T.; Costantino, S.; Lesk, M.R. Pulsatile movement of the optic nerve head and the peripapillary retina in normal subjects and in glaucoma. Invest. Ophthalmol. Vis. Sci. 2012, 53, 7819–7824. [Google Scholar] [CrossRef] [PubMed]
- Putnynaite, V.; Chaleckas, E.; Deimantavicius, M.; Bartusis, L.; Hamarat, Y.; Petkus, V.; Karaliunas, A.; Ragauskas, A. Prospective comparative clinical trials of novel non-invasive intracranial pressure pulse wave monitoring technologies: Preliminary clinical data. Interface Focus. 2024, 14, 20240027. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Participants. JAMA 2025, 333, 71–74. [Google Scholar] [CrossRef]
- Trivli, A.; Koliarakis, I.; Terzidou, C.; Siganos, C.S.; Dalianis, G.; Detorakis, E.T.; Goulielmos, G.N.; Spandidos, D.A. Normal-tension glaucoma: Pathogenesis and genetics. Exp. Ther. Med. 2019, 17, 563–574. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.X.; Xu, L.; Wei, W.B.; Jonas, J.B. Intraocular pressure and its normal range adjusted for ocular and systemic parameters. The Beijing Eye Study 2011. PLoS ONE 2018, 13, e0196926. [Google Scholar] [CrossRef]
- Lauwers, A.; Barbosa Breda, J.; Stalmans, I. The natural history of untreated ocular hypertension and glaucoma. Surv. Ophthalmol. 2023, 68, 388–424. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Age, Years | Gender | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean | ±SD | Min | Max | Male, n | Female, n | Male, % | Female, % | |
| Control | 58.91 | ±12.76 | 25 | 84 | 17 | 51 | 25.0 | 75.0 |
| NTG | 66.63 | ±9.86 | 43 | 85 | 13 | 50 | 20.6 | 79.4 |
| Group | Control | NTG |
|---|---|---|
| NTG medication, n | No medication, 68 | No medication, 6 Pg analogues, 47 CAIs, 19 β blockers, 30 α2 agonists, 2 |
| Comorbidity, n | No comorbidities, 38 Arterial hypertension, 27 Diabetes mellitus, 4 Hypothyroidism, 3 Depression, 2 Gout (podagra), 3 Rheumatoid arthritis, 1 Psoriasis, 1 Asthma, 1 Ischemic heart disease, 3 Gastritis, 1 | No comorbidities, 23 Arterial hypertension, 33 Heart failure, 4 Hypercholesterolemia, 4 Parkinson’s disease, 1 Autoimmune thyroiditis, 1 Diabetes mellitus, 3 Depression, 1 Gout (podagra), 2 Osteoporosis, 1 Angina pectoris, 2 Chronic atrial fibrillation, 3 BPH, 1 Hyperlipidemia, 1 |
| Systemic medication, n | No systemic medication, 41 CCB, 9 ACE inhibitor, 11 Thyroid hormone, 2 Statin, 10 β-blockers, 13 SSRI, 2 XDH inhibitor, 2 Thiazide-like diuretic, 2 Biguanide, 2 ARB, 3 T4 hormone, 2 Other, 11 | No systemic medication, 22 ARB, 6 Thiazide diuretic, 2 Statin, 11 β-blockers, 22 ACE inhibitor, 13 BDZ, 3 NSAID, 6 SIRAs, 2 α2-agonist, 2 Thiazide-like diuretic, 2 XDH inhibitor, 2 Biguanide, 2 CCB, 6 Xa inhibitor, 3 Other, 14 |
| Analyzed Eyes | Left | Right | Both | |||
|---|---|---|---|---|---|---|
| Group | Control | NTG | Control | NTG | Control | NTG |
| Mean (±SD) | 15.39 (±3.20) | 14.80 (±2.78) | 15.39 (±3.15) | 14.43 (±2.93) | 15.39 (±3.16) | 14.62 (±2.85) |
| Median (IQR) | 15.15 (13.00–17.22) | 14.50 (12.70–17.00) | 15.30 (12.70–17.65) | 14.70 (12.30–16.70) | 15.30 (12.78–17.30) | 14.60 (12.70–16.70) |
| K-S test p-value | 0.200 | 0.200 | 0.200 | 0.200 | 0.052 | 0.200 |
| Significance between groups | t = 1.112, df = 129, p = 0.268 | t = 1.795, df = 129, p = 0.075 | F(1, 129) = 2.242, p = 0.137 | |||
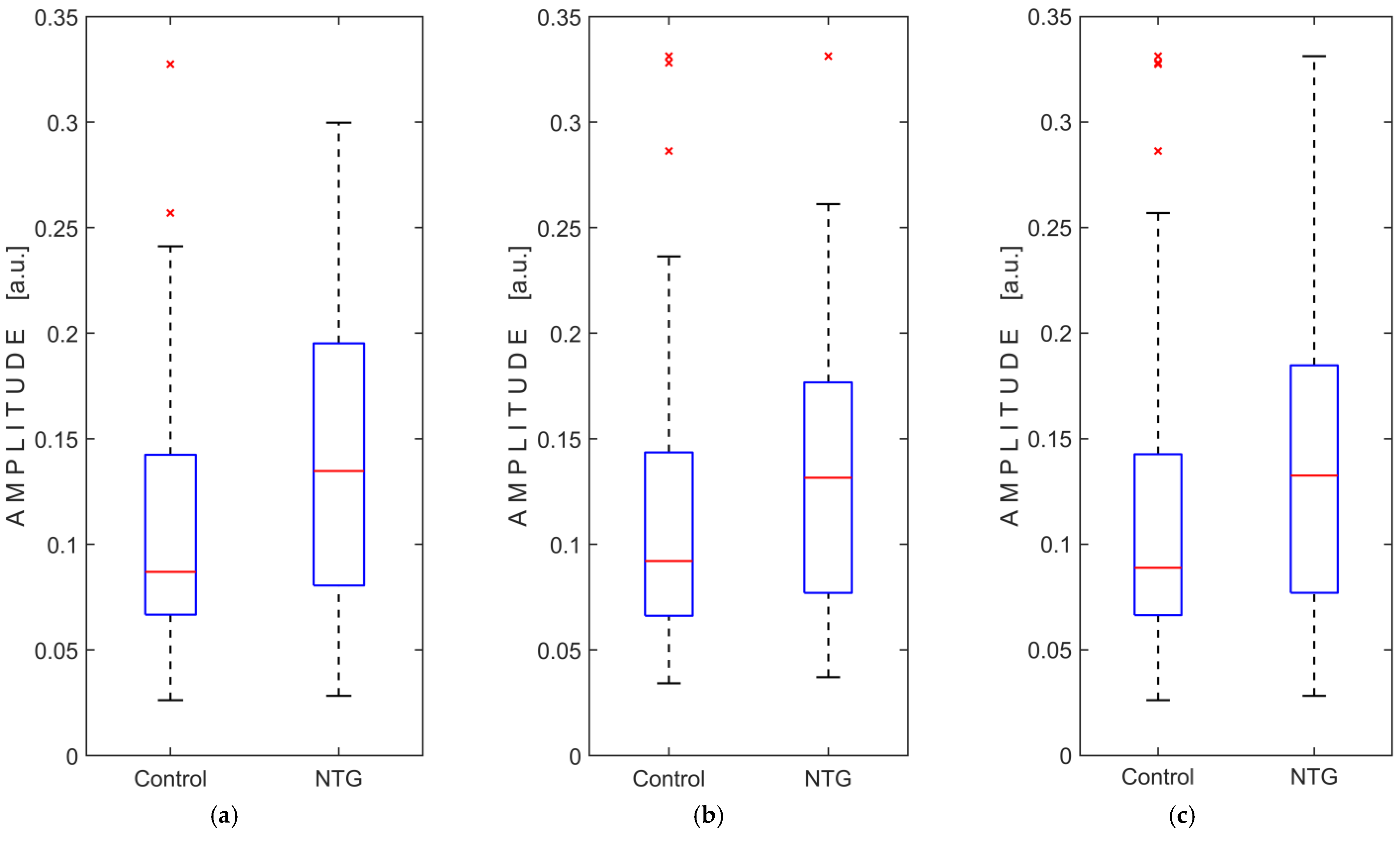
| Analyzed Eyes | Left | Right | Both | |||
|---|---|---|---|---|---|---|
| Group | Control | NTG | Control | NTG | Control | NTG |
| Mean (±SD) | 0.1106 (±0.0746) | 0.1539 (±0.1068) | 0.1176 (±0.0771) | 0.1466 (±0.0875) | 0.1141 (±0.0757) | 0.1503 (±0.0973) |
| Median (IQR) | 0.0869 (0.0664–0.1433) | 0.1347 (0.0798–0.1967) | 0.0921 (0.0659–0.1447) | 0.1315 (0.0769–0.1775) | 0.0889 (0.0663–0.1434) | 0.1326 (0.0769–0.0185) |
| K-S test p-value | <0.001 | 0.007 | <0.001 | 0.006 | <0.001 | <0.001 |
| Significance between groups | U = 1501.0, Z = −2.953, p = 0.003 | U = 1620.4, Z = −2.402, p = 0.016 | F(1, 129) = 6.901, p = 0.01 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartusis, L.; Krakauskaite, S.; Kevalaite, U.; Judickaite, A.; Zizas, A.; Stoskuviene, A.; Chaleckas, E.; Deimantavicius, M.; Hamarat, Y.; Scalzo, F.; et al. Non-Invasive Monitoring of Intracranial Pressure Pulse Waves from Closed Eyelids in Patients with Normal-Tension Glaucoma. Medicina 2025, 61, 566. https://doi.org/10.3390/medicina61040566
Bartusis L, Krakauskaite S, Kevalaite U, Judickaite A, Zizas A, Stoskuviene A, Chaleckas E, Deimantavicius M, Hamarat Y, Scalzo F, et al. Non-Invasive Monitoring of Intracranial Pressure Pulse Waves from Closed Eyelids in Patients with Normal-Tension Glaucoma. Medicina. 2025; 61(4):566. https://doi.org/10.3390/medicina61040566
Chicago/Turabian StyleBartusis, Laimonas, Solventa Krakauskaite, Ugne Kevalaite, Austeja Judickaite, Arminas Zizas, Akvile Stoskuviene, Edvinas Chaleckas, Mantas Deimantavicius, Yasin Hamarat, Fabien Scalzo, and et al. 2025. "Non-Invasive Monitoring of Intracranial Pressure Pulse Waves from Closed Eyelids in Patients with Normal-Tension Glaucoma" Medicina 61, no. 4: 566. https://doi.org/10.3390/medicina61040566
APA StyleBartusis, L., Krakauskaite, S., Kevalaite, U., Judickaite, A., Zizas, A., Stoskuviene, A., Chaleckas, E., Deimantavicius, M., Hamarat, Y., Scalzo, F., Berskiene, K., Januleviciene, I., & Ragauskas, A. (2025). Non-Invasive Monitoring of Intracranial Pressure Pulse Waves from Closed Eyelids in Patients with Normal-Tension Glaucoma. Medicina, 61(4), 566. https://doi.org/10.3390/medicina61040566