
Prognostic Value of Procalcitonin in Febrile People Living with Human Immunodeficiency Virus (PLWH) Admitted to the Emergency Department

 , , ,
, , ,  ,
,  , , ,
, , ,  ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Characteristics and Clinical History
2.2. Laboratory Sampling and Group Definition
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Infective Diagnosis (Any Type of Infection)
Bloodstream Infection
3.3. Survival and Mortality
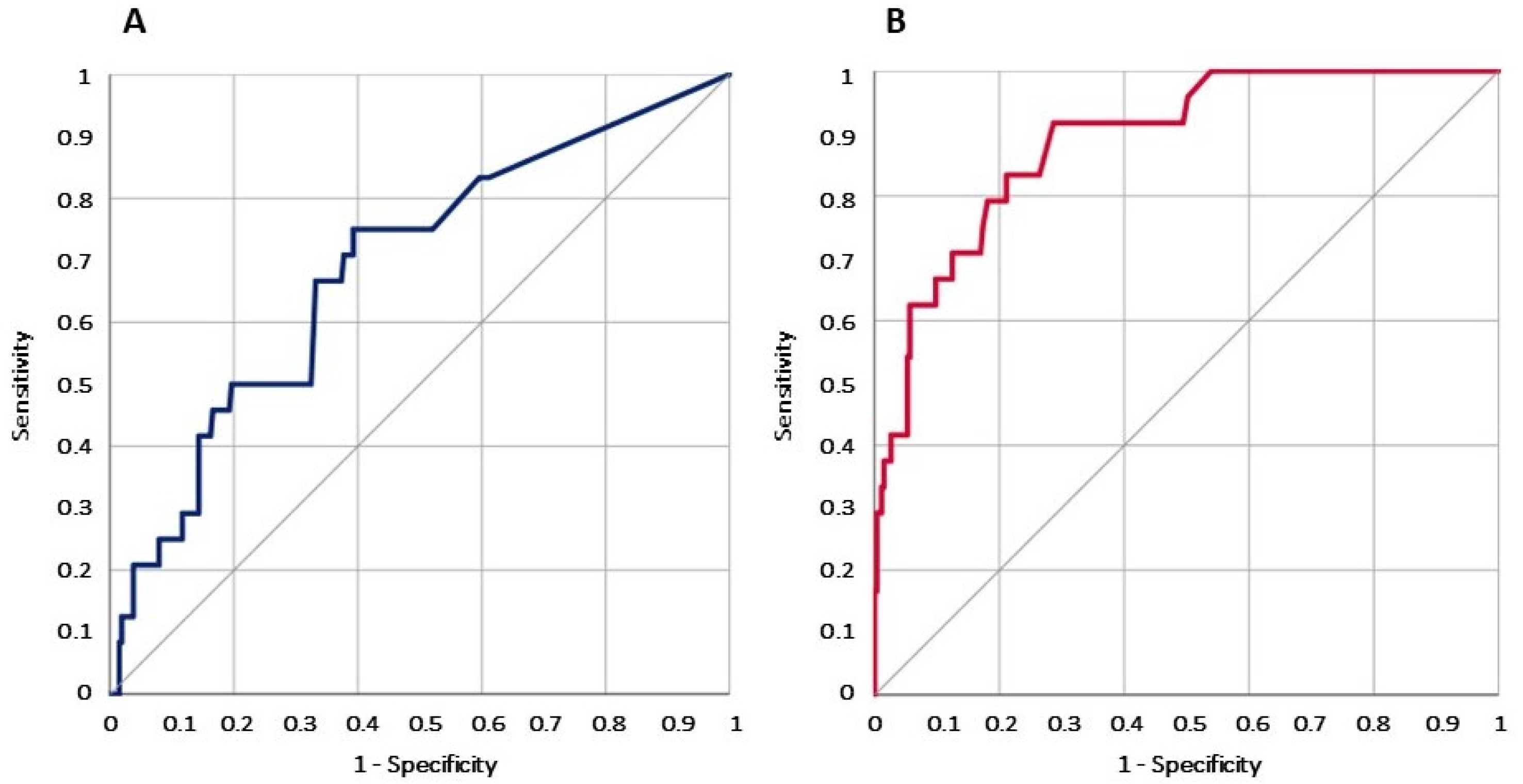
3.4. Receiver Operating Characteristic (ROC) Curve Analysis of Procalcitonin (PCT) Value for Blood Stream Infection (BSI) and Mortality
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- UNAIDS. 2024 UNAIDS Global Aids Update; UNAIDS: Geneva, Switzerland, 2024; Available online: https://www.unaids.org/sites/default/files/media_asset/2024-unaids-global-aids-update_en.pdf (accessed on 30 August 2024).
- Moore, R.D.; Keruly, J.C. CD4+ Cell Count 6 Years after Commencement of Highly Active Antiretroviral Therapy in Persons with Sustained Virologic Suppression. Clin. Infect. Dis. 2007, 44, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Robbins, G.K.; Spritzler, J.G.; Chan, E.S.; Asmuth, D.M.; Gandhi, R.T.; Rodriguez, B.A.; Skowron, G.; Skolnik, P.R.; Shafer, R.W.; Pollard, R.B.; et al. Incomplete Reconstitution of T Cell Subsets on Combination Antiretroviral Therapy in the AIDS Clinical Trials Group Protocol 384. Clin. Infect. Dis. 2009, 48, 350–361. [Google Scholar] [CrossRef] [PubMed]
- Aksak-Wąs, B.J.; Urbańska, A.; Scheibe, K.; Serwin, K.; Leszczyszyn-Pynka, M.; Rafalska-Kosior, M.; Gołąb, J.; Chober, D.; Parczewski, M. Factors Influencing Immune Restoration in People Living with HIV/AIDS. J. Clin. Med. 2022, 11, 1887. [Google Scholar] [CrossRef] [PubMed]
- Sogaard, O.S.; Lohse, N.; Gerstoft, J.; Kronborg, G.; Ostergaard, L.; Pedersen, C.; Pedersen, G.; Sørensen, H.T.; Obel, N. Hospitalization for Pneumonia among Individuals With and Without HIV Infection, 1995–2007: A Danish Population-Based, Nationwide Cohort Study. Clin. Infect. Dis. 2008, 47, 1345–1353. [Google Scholar] [CrossRef]
- Balakrishna, S.; Wolfensberger, A.; Kachalov, V.; Roth, J.A.; Kusejko, K.; Scherrer, A.U.; Furrer, H.; Hauser, C.; Calmy, A.; Cavassini, M.; et al. Decreasing Incidence and Determinants of Bacterial Pneumonia in HIV-Infected Individuals: The Swiss HIV Cohort Study. Lancet 2021. [Google Scholar] [CrossRef]
- Pecego, A.; Amâncio, R.; Costa, D.; Bozza, F.; Siqueira, M.; Oliveira, M.; Cerbino-Neto, J.; Japiassu, A. Etiology, clinical, and epidemiological characteristics of severe respiratory infection in people living with HIV. Int. J. STD AIDS 2020, 31, 100–108. [Google Scholar] [CrossRef]
- Nguyen, T.K.; Nguyen, Y.H.; Nguyen, H.T.; Khong, Q.M.; Tran, N.K. Etiologies of fever of unknown origin in HIV/AIDS patients, Hanoi, Vietnam. BMC Infect. Dis. 2022, 22, 61. [Google Scholar] [CrossRef]
- Hausfater, P.; Juillien, G.; Madonna-Py, B.; Haroche, J.; Bernard, M.; Riou, B. Serum procalcitonin measurement as diagnostic and prognostic marker in febrile adult patients presenting to the emergency department. Crit. Care 2007, 11, R60. [Google Scholar] [CrossRef]
- Tan, M.; Lu, Y.; Jiang, H.; Zhang, L. The diagnostic accuracy of procalcitonin and C-reactive protein for sepsis: A systematic review and meta-analysis. J. Cell. Biochem. 2019, 120, 5852–5859. [Google Scholar] [CrossRef]
- Doganci, M.; Eraslan Doganay, G.; Sazak, H.; Alagöz, A.; Cirik, M.O.; Hoşgün, D.; Cakiroglu, E.B.; Yildiz, M.; Ari, M.; Ozdemir, T.; et al. The Utility of C-Reactive Protein, Procalcitonin, and Leukocyte Values in Predicting the Prognosis of Patients with Pneumosepsis and Septic Shock. Med. Kaunas Lith. 2024, 60, 1560. [Google Scholar] [CrossRef]
- Arora, S.; Singh, P.; Singh, P.M.; Trikha, A. Procalcitonin Levels in Survivors and Nonsurvivors of Sepsis: Systematic Review and Meta-Analysis. Shock Augusta Ga 2015, 43, 212–221. [Google Scholar] [CrossRef]
- Leroux, P.; De Ruffi, S.; Ramont, L.; Gornet, M.; Giordano Orsini, G.; Losset, X.; Kanagaratnam, L.; Gennai, S. Clinical Outcome Predictive Value of Procalcitonin in Patients Suspected with Infection in the Emergency Department. Emerg. Med. Int. 2021, 2021, 2344212. [Google Scholar] [CrossRef] [PubMed]
- Covino, M.; Manno, A.; De Matteis, G.; Taddei, E.; Carbone, L.; Piccioni, A.; Simeoni, B.; Fantoni, M.; Franceschi, F.; Murri, R. Prognostic Role of Serum Procalcitonin Measurement in Adult Patients Admitted to the Emergency Department with Fever. Antibiotics 2021, 10, 788. [Google Scholar] [CrossRef] [PubMed]
- Schleicher, G.K.; Herbert, V.; Brink, A.; Martin, S.; Maraj, R.; Galpin, J.S.; Feldman, C. Procalcitonin and C-reactive protein levels in HIV-positive subjects with tuberculosis and pneumonia. Eur. Respir. J. 2005, 25, 688–692. [Google Scholar] [CrossRef] [PubMed]
- Mikuła, T.; Cianciara, J.; Wiercińska-Drapało, A. Is there any influence of immune deficit on procalcitonin results? Hum. Immunol. 2011, 72, 1194–1197. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Covino, M.; Gallo, A.; Montalto, M.; De Matteis, G.; Burzo, M.L.; Simeoni, B.; Murri, R.; Candelli, M.; Ojetti, V.; Franceschi, F. The Role of Early Procalcitonin Determination in the Emergency Departiment in Adults Hospitalized with Fever. Medicina 2021, 57, 179. [Google Scholar] [CrossRef]
- Covino, M.; Piccioni, A.; Bonadia, N.; Onder, G.; Sabia, L.; Carbone, L.; Candelli, M.; Ojetti, V.; Murri, R.; Franceschi, F. Early procalcitonin determination in the emergency department and clinical outcome of community-acquired pneumonia in old and oldest old patients. Eur. J. Intern. Med. 2020, 79, 51–57. [Google Scholar] [CrossRef]
- Hausfater, P. Biomarkers and infection in the emergency unit. Med. Mal. Infect. 2014, 44, 139–145. [Google Scholar] [CrossRef]
- Russo, A.; Salini, S.; Gava, G.; Merra, G.; Piccioni, A.; De Matteis, G.; Tullo, G.; Novelli, A.; Petrucci, M.; Gasbarrini, A.; et al. Reduced Prognostic Role of Serum PCT Measurement in Very Frail Older Adults Admitted to the Emergency Department. Antibiotics 2023, 12, 1036. [Google Scholar] [CrossRef]
- Wirz, Y.; Meier, M.A.; Bouadma, L.; Luyt, C.E.; Wolff, M.; Chastre, J.; Tubach, F.; Schroeder, S.; Nobre, V.; Annane, D.; et al. Effect of procalcitonin-guided antibiotic treatment on clinical outcomes in intensive care unit patients with infection and sepsis patients: A patient-level meta-analysis of randomized trials. Crit. Care 2018, 22, 191. [Google Scholar] [CrossRef]
- Póvoa, P.; Coelho, L.; Dal-Pizzol, F.; Ferrer, R.; Huttner, A.; Conway Morris, A.; Nobre, V.; Ramirez, P.; Rouze, A.; Salluh, J.; et al. How to use biomarkers of infection or sepsis at the bedside: Guide to clinicians. Intensive Care Med. 2023, 49, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-H.; Tsao, K.-C.; Hu, H.-C.; Huang, C.-C.; Kao, K.-C.; Chen, N.-H.; Yang, C.-T.; Tsai, Y.-H.; Hsieh, M.-J. Procalcitonin and C-reactive protein cannot differentiate bacterial or viral infection in COPD exacerbation requiring emergency department visits. Int. J. Chron. Obstruct. Pulmon. Dis. 2015, 10, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Watkins, R.R.; Lemonovich, T.L. Serum procalcitonin in the diagnosis and management of intra-abdominal infections. Expert Rev. Anti Infect. Ther. 2012, 10, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Drechsler, H.; Zhang, S.; Holodniy, M.; Bedimo, R. CD4 counts and mortality in virologically suppressed US veterans. J. Int. Assoc. Provid. AIDS Care 2014, 13, 120–126. [Google Scholar] [CrossRef]
- Nura, G.J.; Guyo, A.B.; Erango, M.A. Determinants of longitudinal changes of CD4 cell count and survival time to death of HIV/AIDS patients treated at Yabelo General Hospital, the case of pastoralist area: Using joint modelling approach. PLoS ONE 2024, 19, e0305519. [Google Scholar] [CrossRef]
- Huang, G.; Li, X.; Zhang, C.; Li, H.; Jian, M.; Huang, C.; Zhang, Y.; Xian, L.; Zeng, H.; Xia, Y.; et al. Evaluation of CD4+ T Lymphocyte Counts to Predict Survival of ICU Patients with Sepsis Using Sepsis-3 Criteria: A Prospective Cohort Study. Emerg. Med. Int. 2024, 2024, 4293700. [Google Scholar] [CrossRef]
- Park, L.S.; Tate, J.P.; Sigel, K.; Brown, S.T.; Crothers, K.; Gibert, C.; Goetz, M.B.; Rimland, D.; Rodriguez-Barradas, M.C.; Bedimo, R.J.; et al. Association of Viral Suppression With Lower AIDS-Defining and Non–AIDS-Defining Cancer Incidence in HIV-Infected Veterans. Ann. Intern. Med. 2018, 169, 87–96. [Google Scholar] [CrossRef]
- Delabays, B.; Cavassini, M.; Damas, J.; Beuret, H.; Calmy, A.; Hasse, B.; Bucher, H.C.; Frischknecht, M.; Mueller, O.; Mean, M.; et al. Cardiovascular risk assessment in people living with HIV compared to the general population. Eur. J. Prev. Cardiol. 2022, 29, 689–699. [Google Scholar] [CrossRef]
- Poorolajal, J.; Hooshmand, E.; Mahjub, H.; Esmailnasab, N.; Jenabi, E. Survival rate of AIDS disease and mortality in HIV-infected patients: A meta-analysis. Public Health 2016, 139, 3–12. [Google Scholar] [CrossRef]
- Orak, M.; Karakoç, Y.; Ustundag, M.; Yildirim, Y.; Celen, M.K.; Güloglu, C. An investigation of the effects of the mean platelet volume, platelet distribution width, platelet/lymphocyte ratio, and platelet counts on mortality in patents with sepsis who applied to the emergency department. Niger. J. Clin. Pract. 2018, 21, 667–671. [Google Scholar] [CrossRef]
- Cifci, M.; Halhalli, H.C. The Relationship Between Neutrophil-Lymphocyte and Platelet-Lymphocyte Ratios With Hospital Stays and Mortality in the Emergency Department. Cureus 2020, 12, e12179. [Google Scholar] [CrossRef] [PubMed]
- Camon, S.; Quiros, C.; Saubi, N.; Moreno, A.; Marcos, M.A.; Eto, Y.; Rofael, S.; Monclus, E.; Brown, J.; McHugh, T.D.; et al. Full blood count values as a predictor of poor outcome of pneumonia among HIV-infected patients. BMC Infect. Dis. 2018, 18, 189. [Google Scholar] [CrossRef] [PubMed]
- Laher, A.E.; Venter, W.D.F.; Richards, G.A.; Paruk, F. Profile of presentation of HIV-positive patients to an emergency department in Johannesburg, South Africa. South. Afr. J. HIV Med. 2021, 22, 1177. [Google Scholar] [CrossRef] [PubMed]
- Perelló, R.; Miró, O.; Marcos, M.A.; Almela, M.; Bragulat, E.; Sánchez, M.; Agustí, C.; Miro, J.M.; Moreno, A. Predicting bacteremic pneumonia in HIV-1-infected patients consulting the ED. Am. J. Emerg. Med. 2010, 28, 454–459. [Google Scholar] [CrossRef]
- Spierling, A.; Rao, S.; Kikano, E.G.; Smith, D.A.; Tirumani, S.H.; Ramaiya, N.H. Initial diagnosis of HIV/AIDS in patients presenting to the emergency department: Imaging and clinical findings at a single institution. Clin. Imaging 2021, 77, 230–241. [Google Scholar] [CrossRef]

{kind=link}
| Variables | All Patients | PCT < 0.5 | PCT > 0.5 | p Value |
|---|---|---|---|---|
| n = 289 | n = 220 | n = 69 | ||
| Age | 54 [43–62] | 50 [41–61] | 59 [54–64] | <0.001 |
| Charlson | 7 [6–8] | 6 [6–8] | 7 [6–9] | 0.006 |
| Sex (M%) | 214 (74) | 163 (74) | 51 (74) | 0.977 |
| Emergency Department Presentation (Laboratory tests) | ||||
| Creatinine (mg/dL) | 0.92 [0.72–1.21] | 0.89 [0.7125–1.08] | 1.13 [0.80–1.67] | <0.001 |
| Hb (g/dL) | 12.6 [10.75–14.3] | 13.05 [11.0–14.7] | 11.5 [9.6–13.8] | 0.002 |
| Fibrinogen (mg/dL) | 477 [364–663.5] | 446.5 [344–616.75] | 567 [463.5–811] | <0.001 |
| WBC (×109/L) | 7.6 [5.14–11.83] | 7.30 [4.62–10.25] | 9.18 [5.73–15.11] | 0.002 |
| Glucose (mg/dL) | 105 [92.25–131.75] | 103.5 [92–121] | 121 [101.5–169.25] | <0.001 |
| Procalcit. (ng/dL) | 0.1 [0.05–0.45] | 0.06 [0.05–0.13] | 1.95 [0.92–4.515] | <0.001 |
| Platelets (×109/L) | 200.5 [141.0–270.7] | 214 [152–285] | 174 [119–211] | 0.001 |
| CRP (mg/dL) | 51.0 [13.25–143.9] | 34.4 [9.6–95.15] | 163.4 [62.8–204.7] | <0.001 |
| NT-proBNP (ng/L) | 362 [96–1607] | 133 [66.25–454] | 1411 [592.75–4408.5] | <0.001 |
| HIV detectable | 100 (35) | 76 (34) | 24 (34) | 0.971 |
| CD4+ (cell/mm3) | 358 [104–531] | 378 [104–572.2] | 305 [91–511] | 0.371 |
| Emergency Department Presentation (Symptoms) | ||||
| QSOFA 2+ | 17 (5.9) | 5 (2.3) | 12 (17.3) | <0.001 |
| Fever > 38 °C | 204 (70.6) | 151 (68.6) | 53 (76.8) | 0.387 |
| Dyspnea | 104 (36) | 72 (32.7) | 32 (46.4) | 0.029 |
| Cough | 76 (26.3) | 65 (29.5) | 11 (15.9) | 0.016 |
| Hemoptysis | 4 (1.4) | 4 (1.8) | 0 | 0.334 |
| Syncope | 12 (4.2) | 10 (4.5) | 2 (3) | 0.423 |
| Diarrhea | 17 (5.9) | 17 (7.7) | 0 | 0.008 |
| Vomit | 30 (10.4) | 23 (10.5) | 7 (10) | 0.573 |
| Abdominal pain | 37 (12.8) | 27 (12) | 10 (14) | 0.68 |
| Chest pain | 18 (6.2) | 13 (6) | 5 (7.2) | 0.77 |
| Comorbidities | ||||
| COPD | 34 (11.8) | 25 (11.4) | 9 (13) | 0.424 |
| Hepatopathy | 57 (19.7) | 42 (19) | 15 (22) | 0.372 |
| Cirrhosis | 23 (8.0) | 17 (7.7) | 6 (8.7) | 0.483 |
| Diabetes | 19 (6.6) | 15 (7) | 4 (6) | 0.509 |
| Heart failure | 7 (2.4) | 4 (2) | 3 (4) | 0.36 |
| CKD | 16 (5.5) | 11 (5) | 5 (7.2) | 0.55 |
| Infections | ||||
| BSI | 24 (8.3) | 5 (2.3) | 19 (27.5) | <0.001 |
| Pneumonia | 124 (42.9) | 99 (45) | 25 (36.2) | 0.21 |
| Abdominal inf. | 21 (7.3) | 16 (7) | 5 (7) | 1 |
| Urinary Tract inf. | 21 (7.3) | 16 (7) | 5 (7) | 1 |
| Cutaneous inf. | 6 (2) | 6 (3) | - | 0.35 |
| Outcomes | ||||
| Death | 24 (8.3) | 12 (5.5) | 12 (17.5) | 0.004 |
| LOS (days) | 14 [7.11–25.9] | 11.6 [6.57–24.55] | 16 [11.5–13.8] | 0.029 |
| Variables | No Infection n = 72 | Infection n = 217 | Univar. p Value | HR | Multiv. p Value |
|---|---|---|---|---|---|
| Age | 56 [44–62] | 53 [42–62] | 0.41 | ||
| Charlson | 7.5 [5.25–8.00] | 6.0 [6.0–8.0] | 0.3 | ||
| Emergency Department Presentation (Laboratory tests) | |||||
| PCT (ng/mL) | 0.12 [0.05–0.28] | 0.1 [0.05–0.49] | 0.48 | 0.98 [0.45–2.11] | 0.95 |
| Creatinine (mg/dL) | 0.96 [0.75–1.38] | 0.91 [0.71–1.19] | 0.12 | ||
| Hb (g/dL) | 11.35 [9.6–13.6] | 13.2 [11.1–14.8] | <0.001 | ||
| Fibrinogen (mg/dL) | 468.0 [359.5–677.0] | 477 [366.0–655.5] | 0.72 | ||
| WBC (×109/L) | 7.03 [2.91–9.60] | 7.69 [5.3–12.2] | 0.01 | 1.11 [1.03–1.18] | 0.003 |
| Glucose (mg/dL) | 106 [92.5–137.25] | 105 [92.25–129.75] | 0.70 | ||
| Platelets (×109/L) | 187 [115–251] | 209.5 [150–278.5] | 0.04 | ||
| CRP (mg/dL) | 42.2 [8.32–147.25] | 52.5 [14.7–140.0] | 0.38 | 1.00 [0.98–1.00] | 0.79 |
| HIV detectable | 17 (24) | 83 (38) | 0.31 | 2.67 [1.37–5.20] | 0.004 |
| CD4+ (cell/mm3) | 344.5 [135.0–478.0] | 358 [99–551] | 0.02 | ||
| Emergency Department Presentation (Symptoms) | |||||
| QSOFA 2+ | 7 (9.7) | 10 (4.6) | 0.01 | ||
| Fever > 38 °C | 52 (72.2) | 181 (83.4) | 0.03 | 0.62 [0.31–1.23] | 0.173 |
| Dispnea | 19 (26.4) | 85 (39.2) | 0.03 | ||
| Cough | 10 (13.9) | 66 (30.4) | 0.003 | 2.40 [1.12–5.16] | 0.024 |
| Hemoptysis | 0 (0) | 4 (1.8) | 0.32 | ||
| Syncope | 6 (8.3) | 6 (2.8) | 0.05 | ||
| Diarrhea | 5 (6.9) | 12 (5.5) | 0.42 | ||
| Vomit | 8 (11.1) | 22 (10.1) | 0.48 | ||
| Abdominal pain | 11 (15.3) | 26 (12) | 0.54 | ||
| Chest pain | 7 (9.7) | 11 (5.1) | 0.54 | ||
| Comorbidities | |||||
| COPD | 2 (2.8) | 32 (14.7) | 0.003 | ||
| Hepatopathy | 21 (29.2) | 36 (16.6) | 0.02 | ||
| Cirrhosis | 6 (8.3) | 17 (7.8) | 0.53 | ||
| Diabetes | 4 (5.6) | 15 (6.9) | 0.46 | ||
| Heart failure | 2 (2.8) | 5 (2.3) | 0.99 | ||
| CKD | 7 (9.7) | 9 (4.1) | 0.08 | ||
| Infections | |||||
| BSI | - | 24 (11) | |||
| Pneumonia | - | 124 (57.1) | |||
| Abdominal inf. | - | 21 (9.7) | |||
| Urinary Tract inf. | - | 21 (9.7) | |||
| Cutaneous inf. | - | 6 (2.8) | |||
| Outcomes | |||||
| Death | 7 (9.7) | 17 (7.8) | 0.62 | ||
| LOS (days) | 9.76 [6.5–17] | 15.4 [8.0–27.5] | 0.001 | ||
| Variables | BSI n = 24 | No BSI n = 265 | Univar. p Value | HR | Multiv. p Value |
|---|---|---|---|---|---|
| Age | 62 [55–66] | 53 [42–61] | 0.003 | 1.05 [1–1.1] | 0.02 |
| Charlson | 8 [6.25–11.75] | 6 [6–8] | 0.003 | ||
| Emergency Department Presentation (Laboratory tests) | |||||
| PCT (ng/mL) | 2.67 [0.53–21.6] | 0.09 [0.05–0.28] | <0.001 | 8.05 [2.54–25.46] | <0.001 |
| Creatinine (mg/dL) | 1.22 [1.06–3.86] | 0.91 [0.71–1.14] | <0.001 | ||
| Hb (g/dL) | 10.95 [9.2–14.0] | 12.9 [10.8–14.3] | 0.035 | ||
| Fibrinogen (mg/dL) | 529.5 [424–662] | 471 [360–663] | 0.172 | ||
| WBC (×109/L) | 8.74 [6.4–16.8] | 7.48 [4.9–11.5] | 0.058 | 1.06 [ 0.99–1.13] | 0.12 |
| Glucose (mg/dL) | 123 [93.0–173] | 104 [92–129] | 0.072 | ||
| Platelets (×109/L) | 142 [120–198] | 208 [150–273] | 0.011 | ||
| CRP (mg/L) | 147 [80–269] | 49 [11–136] | <0.001 | 1.00 [0.99–1.01] | 0.34 |
| HIV detectable | 10 (41.7) | 90 (34) | 0.503 | 1.88 [ 0.62–5.73] | 0.27 |
| CD4+ (cell/mm3) | 284 [69–503] | 360 [104–548] | 0.219 | ||
| Emergency Department Presentation (Symptoms) | |||||
| QSOFA 2+ | 2 (8.3) | 15 (5.7) | 0.422 | ||
| Fever > 38 °C | 21 (87.5) | 212 (80.0) | 0.278 | 0.45 [0.11–1.83] | 0.26 |
| Dispnea | 8 (33.3) | 96 (36.2) | 0.483 | ||
| Cough | 2 (8.3) | 74 (27.9) | 0.025 | 0.28 [0.05–1.4] | 0.28 |
| Hemoptysis | 0 | 4 (1.5) | 0.706 | ||
| Syncope | 0 | 12 (4.5) | 0.346 | ||
| Diarrhea | 0 | 17 (6.4) | 0.219 | ||
| Vomit | 2 (8.3) | 28 (10.6) | 0.535 | ||
| Abdominal pain | 2 (8.3) | 35 (13.2) | 0.75 | ||
| Chest pain | 1 (4.2) | 18 (6.8) | 0.38 | ||
| Comorbidities | |||||
| COPD | 6 (25.0) | 28 (10.6) | 0.047 | ||
| Hepatopathy | 5 (20.8) | 52 (19.6) | 0.531 | ||
| Cirrhosis | 4 (16.7) | 19 (7.2) | 0.110 | ||
| Diabetes | 3 (12.5) | 16 (6.0) | 0.201 | ||
| Heart failure | 2 (8.3) | 5 (1.9) | 0.10 | ||
| CKD | 3 (12.5) | 13 (4.9) | 0.13 | ||
| Infections | |||||
| BSI (primitive) | 20 (83) | - | <0.001 | ||
| Pneumonia | - | 124 (46.8) | <0.001 | ||
| Abdominal inf. | 1 (4.2) | 20 (7.5) | 1 | ||
| Urinary Tract inf. | 3 (12.5) | 18 (6.8) | 0.4 | ||
| Cutaneous inf. | - | 6 (2.3) | 1 | ||
| Outcomes | |||||
| Death | 3 (12.5) | 21 (7.9) | 0.43 | ||
| LOS (days) | 19.5 [12.5–30.4] | 13 [7.0–25] | 0.007 | ||
| Variables | Survivors n = 265 | Non-Survivors n = 24 | Univariate p Value | Hazard Ratio | Multiv. p Value |
|---|---|---|---|---|---|
| Age | 53 [42–62] | 59 [45.2–62.0] | 0.300 | 1.01 [0.97–1.05] | 0.66 |
| Charlson | 7 [6–8] | 8 [6–10] | 0.023 | 1.14 [0.95–1.36] | 0.17 |
| Emergency Department Presentation (Laboratory tests) | |||||
| PCT (ng/mL) | 0.1 [0.05–0.345] | 0.385 [0.098–2.34] | 0.002 | 3.1 [1.25–7.72] | 0.015 |
| Creatinine (mg/dL) | 0.93 [0.75–1.2175] | 0.68 [0.5525–1.220] | 0.013 | ||
| Hb (g/dL) | 12.7 [10.8–14.3] | 12.3 [10.2–13.8] | 0.39 | ||
| Fibrinogen (mg/dL) | 477 [374–673] | 448 [272–567] | 0.03 | ||
| WBC (×109/L) | 7.840 [5.22–12.0] | 5.3 [4.55–8.49] | 0.03 | ||
| Glucose (mg/dL) | 104 [92–128] | 113 [103–154] | 0.07 | ||
| Platelets (×109/L) | 208.5 [150.25–271] | 120.5 [72–197] | 0.001 | ||
| PCR (mg/dL) | 50.9 [13.25–143.05] | 67.9 [14.6–194.6] | 0.50 | ||
| CD4+ (cell/mm3) | 369.5 [136.25–548.00] | 61 [14–186] | <0.001 | ||
| HIV detectable | 85 (32) | 15 (60) | 0.02 | 3.66 [1.41–9.48] | 0.007 |
| QSOFA 2+ | 14 (5.3) | 3 (12.5) | 0.16 | ||
| Emergency Department Presentation (Symptoms) | |||||
| Fever > 38 °C | 217 (81.9) | 16 (66.7) | 0.07 | ||
| Dispnea | 93 (35.1) | 11 (45.8) | 0.20 | ||
| Cough | 73 (27.5) | 3 (12.5) | 0.08 | ||
| Hemoptysis | 4 (1.5) | 0 (0) | 0.71 | ||
| Syncope | 12 (4.5) | 0 (0) | 0.35 | ||
| Diarrhea | 17 (6.4) | 0 (0) | 0.22 | ||
| Vomit | 30 (11.3) | 0 (0) | 0.06 | ||
| Abdominal pain | 36 (13.6) | 1 (4.2) | 0.33 | ||
| Chest pain | 18 (6.8) | 0 (0) | 0.38 | ||
| Comorbidities | |||||
| COPD | 32 (12.1) | 2 (8.3) | 0.44 | ||
| Hepatopathy | 54 (20.4) | 3 (12.5) | 0.26 | ||
| Cirrhosis | 21 (7.9) | 2 (8.3) | 0.59 | ||
| Diabetes | 15 (5.7) | 4 (16.7) | 0.06 | ||
| Heart failure | 5 (2) | 2 (8.3) | 0.11 | ||
| CKD | 13 (5) | 3 (12.5) | 0.14 | ||
| Infections | |||||
| BSI | 21 (7.9) | 3 (12) | 0.43 | ||
| Pneumonia | 64 (24) | 11 (45) | 0.02 | ||
| Abdominal inf. | 21 (8) | 0 (0) | 0.23 | ||
| Urinary Tract inf. | 21 (8) | 0 (0) | 0.23 | ||
| Cutaneous inf. | 6 (2.3) | 0 (0) | 1 | ||
| Outcomes | |||||
| LOS (days) | 13 [7–25] | 18 [15–29] | 0.021 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Celani, L.; Carbone, L.; Ceppa, F.; Piccioni, A.; Della Polla, D.A.; Chiuchiarelli, M.; Cingolani, A.; De Matteis, G.; Murri, R.; Gasbarrini, A.; et al. Prognostic Value of Procalcitonin in Febrile People Living with Human Immunodeficiency Virus (PLWH) Admitted to the Emergency Department. Medicina 2025, 61, 240. https://doi.org/10.3390/medicina61020240
Celani L, Carbone L, Ceppa F, Piccioni A, Della Polla DA, Chiuchiarelli M, Cingolani A, De Matteis G, Murri R, Gasbarrini A, et al. Prognostic Value of Procalcitonin in Febrile People Living with Human Immunodeficiency Virus (PLWH) Admitted to the Emergency Department. Medicina. 2025; 61(2):240. https://doi.org/10.3390/medicina61020240
Chicago/Turabian StyleCelani, Luigi, Luigi Carbone, Francesco Ceppa, Andrea Piccioni, Davide Antonio Della Polla, Marta Chiuchiarelli, Antonella Cingolani, Giuseppe De Matteis, Rita Murri, Antonio Gasbarrini, and et al. 2025. "Prognostic Value of Procalcitonin in Febrile People Living with Human Immunodeficiency Virus (PLWH) Admitted to the Emergency Department" Medicina 61, no. 2: 240. https://doi.org/10.3390/medicina61020240
APA StyleCelani, L., Carbone, L., Ceppa, F., Piccioni, A., Della Polla, D. A., Chiuchiarelli, M., Cingolani, A., De Matteis, G., Murri, R., Gasbarrini, A., Franceschi, F., & Covino, M. (2025). Prognostic Value of Procalcitonin in Febrile People Living with Human Immunodeficiency Virus (PLWH) Admitted to the Emergency Department. Medicina, 61(2), 240. https://doi.org/10.3390/medicina61020240