
Update on the Efficacy and Safety of Sodium–Glucose Co-Transporter 2 Inhibitors in Patients with Chronic Diseases: A Systematic Review and Meta-Analysis

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
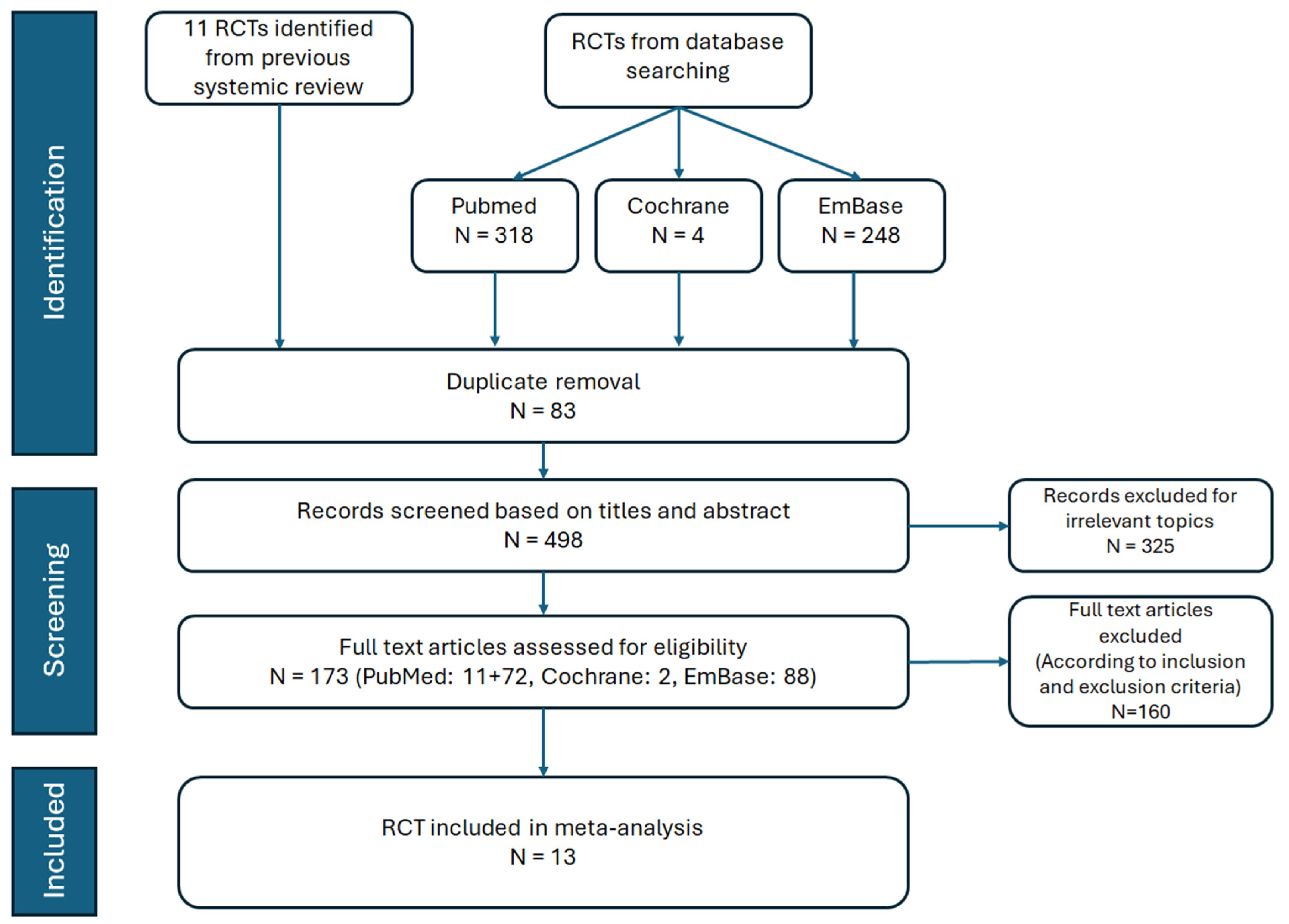
2.1. Database Searches and Identification of Eligible Papers
2.2. Inclusion and Exclusion Criteria
2.3. Data Screening and Extraction
2.4. Primary Outcomes
2.5. Safety Outcomes
2.6. Statistical Analysis and PROSPERO Registry
3. Results
3.1. Study Search and Characteristics of Included Patients
3.2. Type 2 Diabetic Mellitus
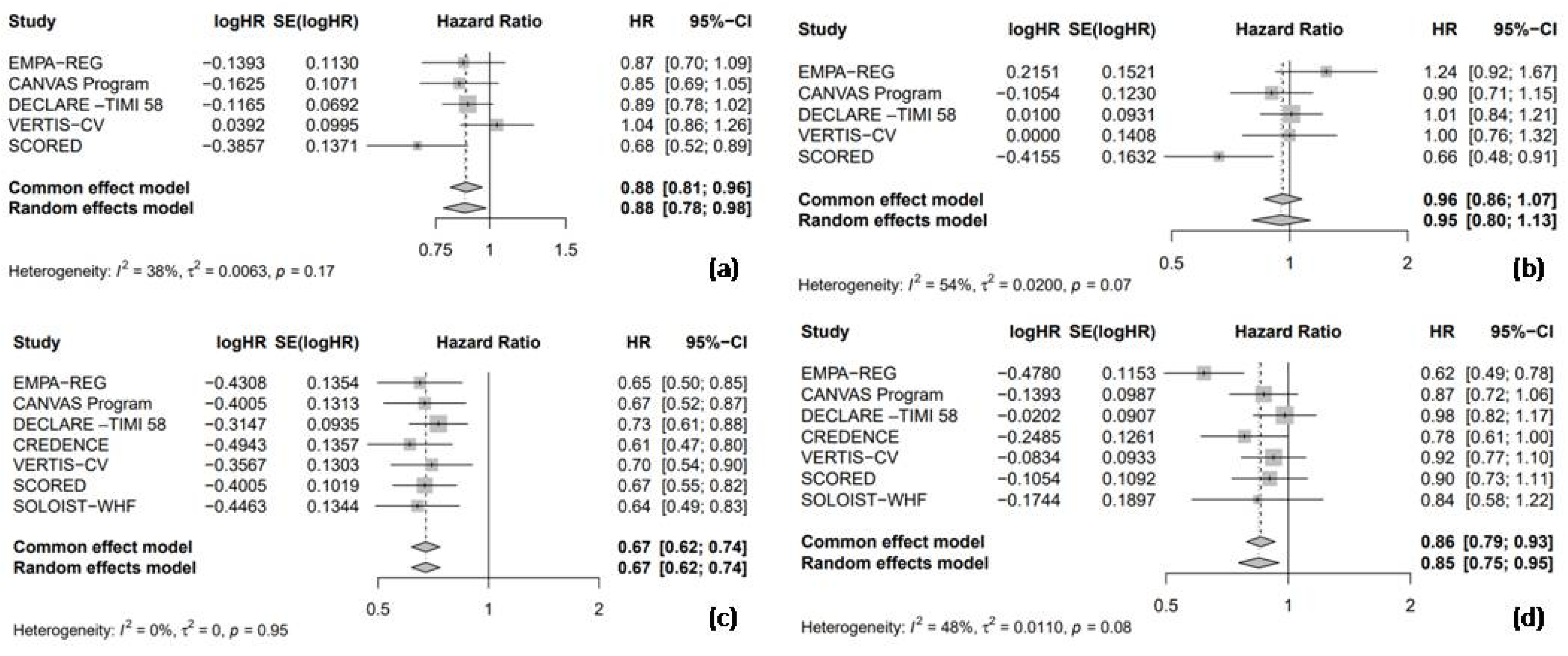
3.2.1. Nonfatal Myocardial Infarction, Nonfatal Stroke, and Hospitalization for Heart Failure and Cardiac Death
3.2.2. Safety Outcomes
3.3. Heart Failure
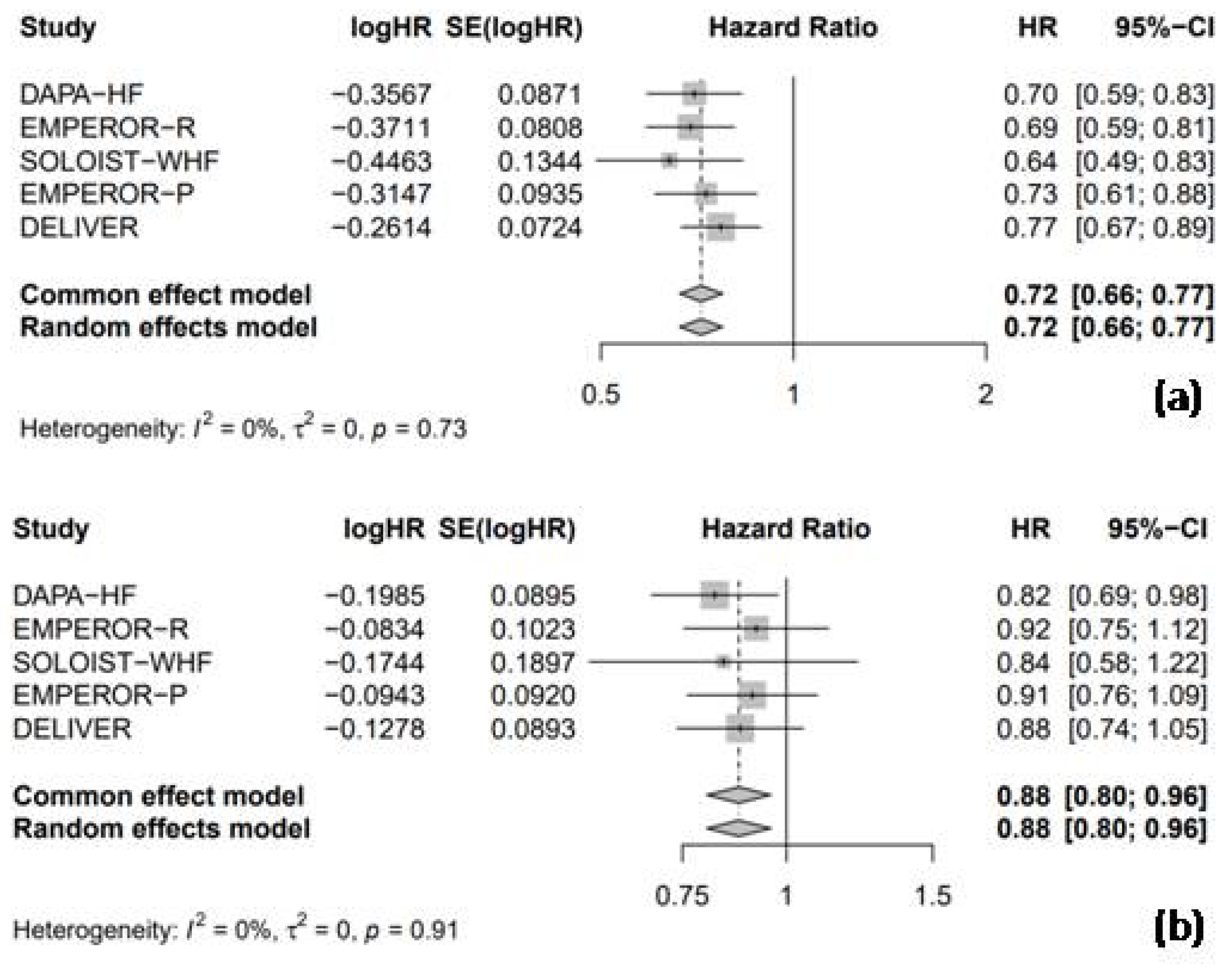
3.3.1. Hospitalization for Heart Failure and Cardiac Death
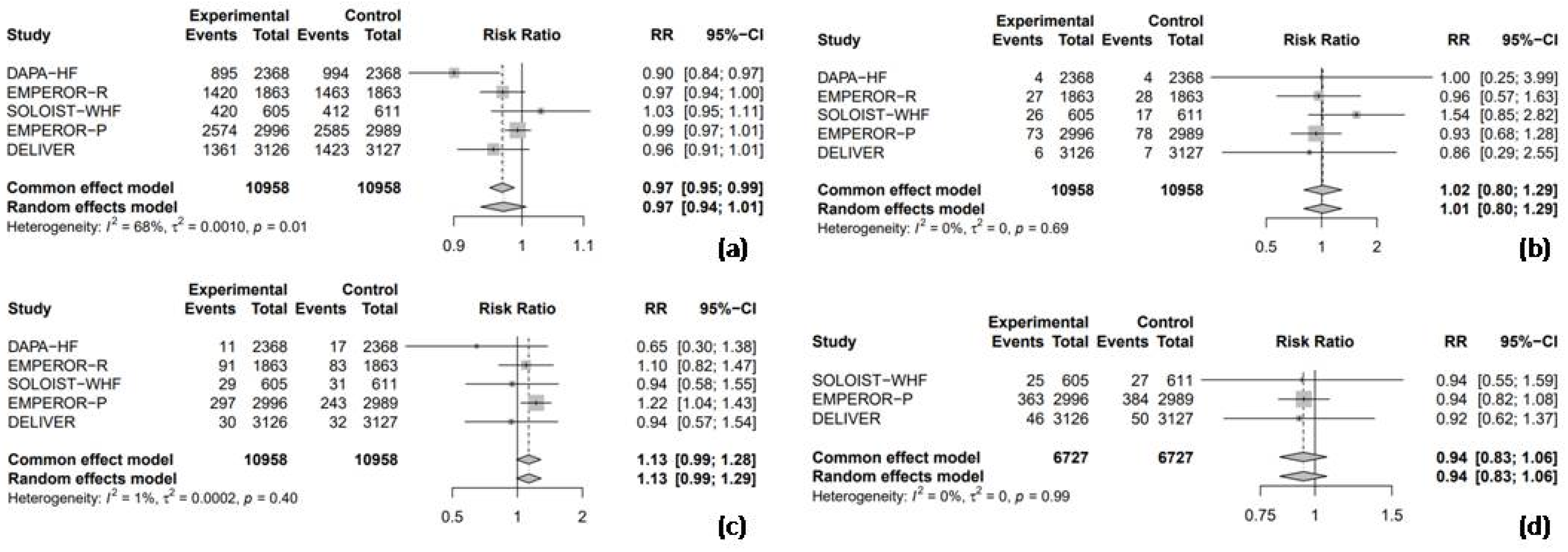
3.3.2. Safety Outcomes
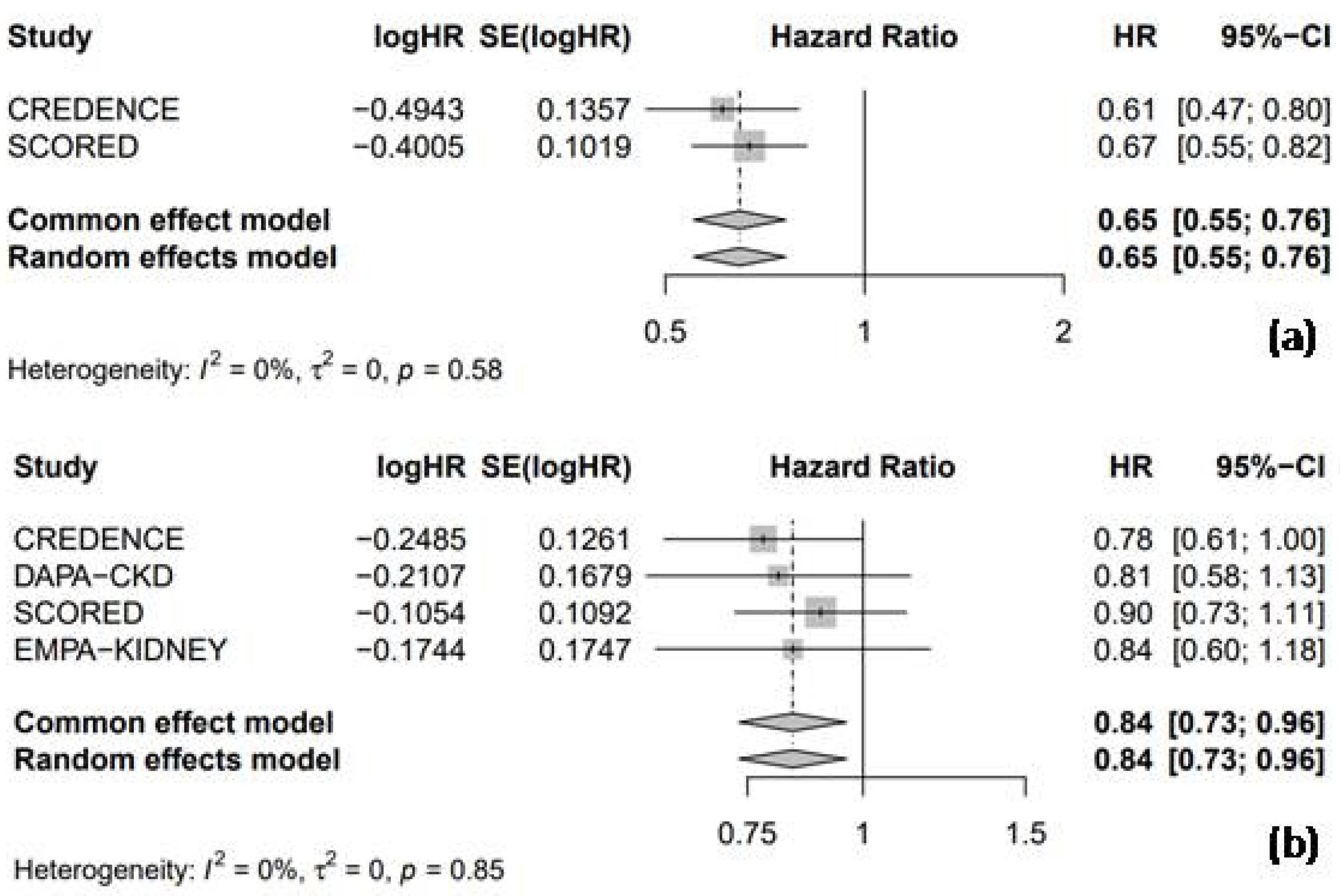
3.4. Chronic Kidney Disease
3.4.1. Hospitalization for Heart Failure and Cardiac Death
3.4.2. Safety Outcomes
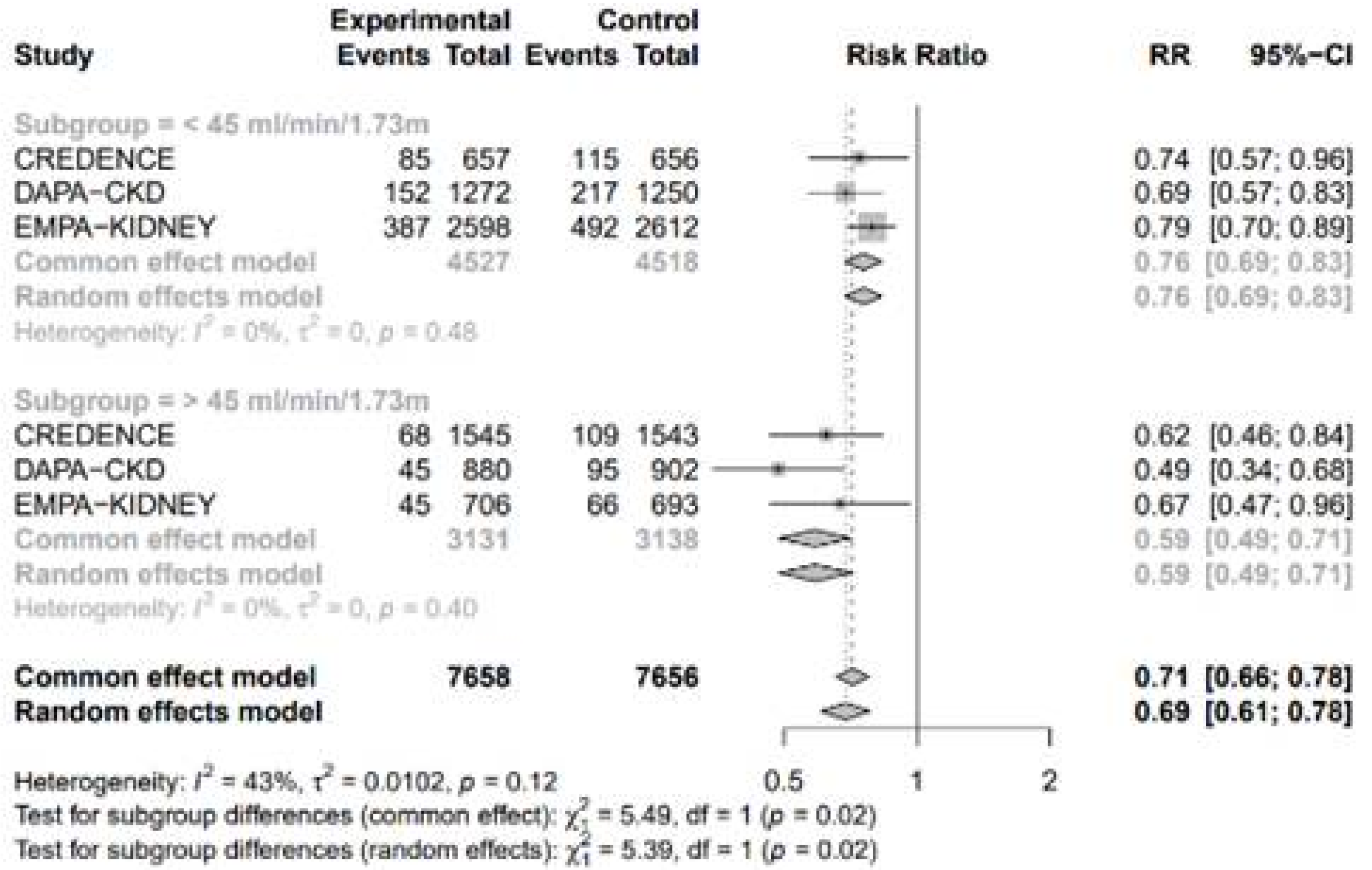
3.4.3. Subgroup Analysis by the Estimated Glomerular Filtration Rate
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| SGLT2 | sodium–glucose co-transporter-2 |
| T2DM | Type 2 diabetes mellitus |
| RCT | randomized controlled trials |
| HF | heart failure |
| CKD | chronic kidney disease |
| MI | myocardial infarction |
| HHF | hospitalization for heart failure |
| UTI | urinary tract infection |
| AKI | acute kidney injury |
| HR | hazard ratio |
| CI | confidence interval |
| RR | risk ratio |
| LVEF | left ventricular ejection fraction |
| PRISMA | preferred reporting items for systematic reviews and meta-analyses |
| eGFR | estimated glomerular filtration rate |
References
- Chew, N.W.; Ng, C.H.; Tan, D.J.H.; Kong, G.; Lin, C.; Chin, Y.H.; Lim, W.H.; Huang, D.Q.; Quek, J.; Fu, C.E.; et al. The global burden of metabolic disease: Data from 2000 to 2019. Cell Metab. 2023, 35, 414–428. [Google Scholar] [CrossRef] [PubMed]
- Ansah, J.P.; Chiu, C.-T. Projecting the chronic disease burden among the adult population in the United States using a multi-state population model. Front. Public Health 2023, 10, 1082183. [Google Scholar] [CrossRef] [PubMed]
- Martín-Timón, I.; Sevillano-Collantes, C.; Segura-Galindo, A.; del Cañizo-Gómez, F.J. Type 2 diabetes and cardiovascular disease: Have all risk factors the same strength? World J. Diabetes 2014, 5, 444. [Google Scholar] [CrossRef]
- Idris, I.; Donnelly, R. Sodium–glucose co-transporter-2 inhibitors: An emerging new class of oral antidiabetic drug. Diabetes Obes. Metab. 2009, 11, 79–88. [Google Scholar] [CrossRef]
- Rieg, T.; Vallon, V. Development of SGLT1 and SGLT2 inhibitors. Diabetologia 2018, 61, 2079–2086. [Google Scholar] [CrossRef]
- Haider, K.; Pathak, A.; Rohilla, A.; Haider, M.R.; Ahmad, K.; Yar, M.S. Synthetic strategy and SAR studies of C-glucoside heteroaryls as SGLT2 inhibitor: A review. Eur. J. Med. Chem. 2019, 184, 111773. [Google Scholar] [CrossRef]
- Ferrannini, E. Sodium–glucose transporter-2 inhibition as an antidiabetic therapy. Nephrol. Dial. Transplant. 2010, 25, 2041–2043. [Google Scholar] [CrossRef]
- Madaan, T.; Akhtar, M.; Najmi, A.K. Sodium glucose CoTransporter 2 (SGLT2) inhibitors: Current status and future perspective. Eur. J. Pharm. Sci. 2016, 93, 244–252. [Google Scholar] [CrossRef]
- Choi, C.-I. Sodium-glucose cotransporter 2 (SGLT2) inhibitors from natural products: Discovery of next-generation antihyperglycemic agents. Molecules 2016, 21, 1136. [Google Scholar] [CrossRef]
- Oranje, P.; Gouka, R.; Burggraaff, L.; Vermeer, M.; Chalet, C.; Duchateau, G.; van der Pijl, P.; Geldof, M.; de Roo, N.; Clauwaert, F.; et al. Novel natural and synthetic inhibitors of solute carriers SGLT1 and SGLT2. Pharmacol. Res. Perspect. 2019, 7, e00504. [Google Scholar] [CrossRef]
- Hsia, D.S.; Grove, O.; Cefalu, W.T. An update on sodium-glucose co-transporter-2 inhibitors for the treatment of diabetes mellitus. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Beghini, A.; Sammartino, A.M.; Papp, Z.; von Haehling, S.; Biegus, J.; Ponikowski, P.; Adamo, M.; Falco, L.; Lombardi, C.M.; Pagnesi, M.; et al. 2024 update in heart failure. ESC Heart Fail. 2024. [Google Scholar] [CrossRef] [PubMed]
- Qaseem, A.; Obley, A.J.; Shamliyan, T.; Hicks, L.A.; Harrod, C.S.; Crandall, C.J.; Clinical Guidelines Committee of the American College of Physicians; Balk, E.M.; Cooney, T.G.; Cross, J.T.; et al. Newer pharmacologic treatments in adults with type 2 diabetes: A clinical guideline from the American College of Physicians. Ann. Intern. Med. 2024, 177, 658–666. [Google Scholar] [CrossRef] [PubMed]
- O’hara, D.V.; Lam, C.S.P.; McMurray, J.J.V.; Yi, T.W.; Hocking, S.; Dawson, J.; Raichand, S.; Januszewski, A.S.; Jardine, M.J. Applications of SGLT2 inhibitors beyond glycaemic control. Nat. Rev. Nephrol. 2024, 20, 513–529. [Google Scholar] [CrossRef]
- Gajewska, A.; Wasiak, J.; Sapeda, N.; Młynarska, E.; Rysz, J.; Franczyk, B. SGLT2 Inhibitors in Kidney Diseases—A Narrative Review. Int. J. Mol. Sci. 2024, 25, 4959. [Google Scholar] [CrossRef]
- Dunlay, S.M.; Givertz, M.M.; Aguilar, D.; Allen, L.A.; Chan, M.; Desai, A.S.; Deswal, A.; Dickson, V.V.; Kosiborod, M.N.; Lekavich, C.L.; et al. Type 2 diabetes mellitus and heart failure: A scientific statement from the American Heart Association and the Heart Failure Society of America: This statement does not represent an update of the 2017 ACC/AHA/HFSA heart failure guideline update. Circulation 2019, 140, e294–e324. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Care in Diabetes—2024. Diabetes Care 2023, 47, S158–S178. [Google Scholar] [CrossRef]
- Bahari, H.; Shahraki Jazinaki, M.; Rahnama, I.; Aghakhani, L.; Amini, M.R.; Malekahmadi, M. The cardiometabolic benefits of okra-based treatment in prediabetes and diabetes: A systematic review and meta-analysis of randomized controlled trials. Front. Nutr. 2024, 11, 1454286. [Google Scholar] [CrossRef]
- Nikpayam, O.; Saghafi-Asl, M.; Safaei, E.; Bahreyni, N.; Sadra, V.; Asgharian, P. The effect of Abelmoschus esculentus L. (Okra) extract supplementation on glycaemic control, inflammation, kidney function and expression of PPAR-α, PPAR-γ, TGF-β and Nrf-2 genes in patients with diabetic nephropathy: A triple-blind, randomised, placebo-controlled trial. Br. J. Nutr. 2024, 131, 648–657. [Google Scholar]
- Sereno, A.B.; Pinto, C.D.; Andrade, F.A.; da Silva, M.A.B.; Garcia, A.C.; Krüger, C.C.H.; Reason, I.J.d.M. Effects of okra (Abelmoschus esculentus (L.) Moench) on glycemic markers in animal models of diabetes: A systematic review. J. Ethnopharmacol. 2022, 298, 115544. [Google Scholar] [CrossRef]
- Mokgalaboni, K.; Lebelo, S.L.; Modjadji, P.; Ghaffary, S. Okra ameliorates hyperglycaemia in pre-diabetic and type 2 diabetic patients: A systematic review and meta-analysis of the clinical evidence. Front. Pharmacol. 2023, 14, 1132650. [Google Scholar] [CrossRef] [PubMed]
- Adimadhyam, S.; Schumock, G.T.; Calip, G.S.; Smith Marsh, D.E.; Layden, B.T.; Lee, T.A. Increased risk of mycotic infections associated with sodium–glucose co-transporter 2 inhibitors: A prescription sequence symmetry analysis. Br. J. Clin. Pharmacol. 2019, 85, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, I.R.; Rose, S.C.P.; Freire, N.B.; Patrocínio, M.S.; Pierdoná, N.; Bittencourt, R.J. Use of sodium-glucose cotransporter-2 inhibitors and urinary tract infections in type 2 diabetes patients: A systematic review. Rev. Da Assoc. Médica Bras. 2019, 65, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar]
- Giugliano, D.; Longo, M.; Scappaticcio, L.; Bellastella, G.; Maiorino, M.I.; Esposito, K. SGLT-2 inhibitors and cardiorenal outcomes in patients with or without type 2 diabetes: A meta-analysis of 11 CVOTs. Cardiovasc. Diabetol. 2021, 20, 1–11. [Google Scholar] [CrossRef]
- Higgins, J. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. Cochrane Collab. 2011. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R.; et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N. Engl. J. Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Stefánsson, B.V.; Correa-Rotter, R.; Chertow, G.M.; Greene, T.; Hou, F.-F.; Mann, J.F.E.; McMurray, J.J.V.; Lindberg, M.; Rossing, P.; et al. Dapagliflozin in patients with chronic kidney disease. N. Engl. J. Med. 2020, 383, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Cannon, C.P.; Pratley, R.; Dagogo-Jack, S.; Mancuso, J.; Huyck, S.; Masiukiewicz, U.; Charbonnel, B.; Frederich, R.; Gallo, S.; Cosentino, F.; et al. Cardiovascular outcomes with ertugliflozin in type 2 diabetes. N. Engl. J. Med. 2020, 383, 1425–1435. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Szarek, M.; Pitt, B.; Cannon, C.P.; Leiter, L.A.; McGuire, D.K.; Lewis, J.B.; Riddle, M.C.; Inzucchi, S.E.; Kosiborod, M.N.; et al. Sotagliflozin in patients with diabetes and chronic kidney disease. N. Engl. J. Med. 2021, 384, 129–139. [Google Scholar] [CrossRef]
- Bhatt, D.L.; Szarek, M.; Steg, P.G.; Cannon, C.P.; Leiter, L.A.; McGuire, D.K.; Lewis, J.B.; Riddle, M.C.; Voors, A.A.; Metra, M.; et al. Sotagliflozin in patients with diabetes and recent worsening heart failure. N. Engl. J. Med. 2021, 384, 117–128. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner–La Rocca, H.-P.; Choi, D.-J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in heart failure with a preserved ejection fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Solomon, S.D.; McMurray, J.J.; Claggett, B.; de Boer, R.A.; DeMets, D.; Hernandez, A.F.; Inzucchi, S.E.; Kosiborod, M.N.; Lam, C.S.; Martinez, F.; et al. Dapagliflozin in heart failure with mildly reduced or preserved ejection fraction. N. Engl. J. Med. 2022, 387, 1089. [Google Scholar] [CrossRef]
- EMPA-Kidney Collaborative Group. Empagliflozin in patients with chronic kidney disease. N. Engl. J. Med. 2023, 388, 117–127. [Google Scholar] [CrossRef]
- Borovac, J.A.; Kurir, T.; Mustapic, I.; Kumric, M.; Bozic, J.; Glavas, D.; D’amario, D. SGLT2 inhibitors and the risk of urinary tract infections in patients with heart failure: A pooled analysis examining safety endpoints. Pol. Heart J. 2022, 80, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, J.; Lin, Y.; Yao, K.; Xie, Y.; Zhou, T. Cardiovascular outcomes and safety of SGLT2 inhibitors in chronic kidney disease patients. Front. Endocrinol. 2023, 14, 1236404. [Google Scholar] [CrossRef] [PubMed]
- McGuire, D.K.; Shih, W.J.; Cosentino, F.; Charbonnel, B.; Cherney, D.Z.; Dagogo-Jack, S.; Pratley, R.; Greenberg, M.; Wang, S.; Huyck, S.; et al. Association of SGLT2 inhibitors with cardiovascular and kidney outcomes in patients with type 2 diabetes: A meta-analysis. JAMA Cardiol. 2021, 6, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.K.; Dhingra, N.K.; Hibino, M.; Gupta, V.; Verma, S. Sodium-glucose cotransporter 2 inhibitors in heart failure with reduced or preserved ejection fraction: A meta-analysis. ESC Heart Fail. 2022, 9, 942–946. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Zhou, G.; Zheng, Y.; Lv, D.; Zhu, X.; Wei, P.; Zheng, M.; Liu, S.; Zhou, E.; Sun, W.; et al. Effects of SGLT2 inhibitors on cardiovascular outcomes in patients with stage 3/4 CKD: A meta-analysis. PLoS ONE 2022, 17, e0261986. [Google Scholar] [CrossRef]
- Donnan, J.R.; Grandy, C.A.; Chibrikov, E.; Marra, C.A.; Aubrey-Bassler, K.; Johnston, K.; Swab, M.; Hache, J.; Curnew, D.; Nguyen, H.; et al. Comparative safety of the sodium glucose co-transporter 2 (SGLT2) inhibitors: A systematic review and meta-analysis. BMJ Open 2019, 9, e022577. [Google Scholar] [CrossRef]
- Thomas, M.C.; Cherney, D.Z.I. The actions of SGLT2 inhibitors on metabolism, renal function and blood pressure. Diabetologia 2018, 61, 2098–2107. [Google Scholar] [CrossRef]
- Garcia-Ropero, A.; Santos-Gallego, C.G.; Zafar, M.U.; Badimon, J.J. Metabolism of the failing heart and the impact of SGLT2 inhibitors. Expert Opin. Drug Metab. Toxicol. 2019, 15, 275–285. [Google Scholar] [CrossRef]
- Lopaschuk, G.D.; Verma, S. Mechanisms of cardiovascular benefits of sodium glucose co-transporter 2 (SGLT2) inhibitors: A state-of-the-art review. Basic Transl. Sci. 2020, 5, 632–644. [Google Scholar]
- Lopaschuk, G.D.; Ussher, J.R.; Folmes, C.D.; Jaswal, J.S.; Stanley, W.C. Myocardial fatty acid metabolism in health and disease. Physiol. Rev. 2010, 90, 207–258. [Google Scholar] [CrossRef]
- Neubauer, S. The failing heart—An engine out of fuel. N. Engl. J. Med. 2007, 356, 1140–1151. [Google Scholar] [CrossRef] [PubMed]
- Aubert, G.; Martin, O.J.; Horton, J.L.; Lai, L.; Vega, R.B.; Leone, T.C.; Koves, T.; Gardell, S.J.; Krüger, M.; Hoppel, C.L.; et al. The failing heart relies on ketone bodies as a fuel. Circulation 2016, 133, 698–705. [Google Scholar] [CrossRef] [PubMed]
- Bedi, K.C., Jr.; Snyder, N.W.; Brandimarto, J.; Aziz, M.; Mesaros, C.; Worth, A.J.; Wang, L.L.; Javaheri, A.; Ian, A.; Margulies, K.B.; et al. Evidence for intramyocardial disruption of lipid metabolism and increased myocardial ketone utilization in advanced human heart failure. Circulation 2016, 133, 706–716. [Google Scholar] [CrossRef] [PubMed]
- Ho, K.L.; Zhang, L.; Wagg, C.; Al Batran, R.; Gopal, K.; Levasseur, J.; Leone, T.; Dyck, J.R.B.; Ussher, J.R.; Muoio, D.M.; et al. Increased ketone body oxidation provides additional energy for the failing heart without improving cardiac efficiency. Cardiovasc. Res. 2019, 115, 1606–1616. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Rawat, S.; Ho, K.L.; Wagg, C.S.; Zhang, L.; Teoh, H.; Dyck, J.E.; Uddin, G.M.; Oudit, G.Y.; Mayoux, E.; et al. Empagliflozin increases cardiac energy production in diabetes: Novel translational insights into the heart failure benefits of SGLT2 inhibitors. JACC Basic Transl. Sci. 2018, 3, 575–587. [Google Scholar] [CrossRef]
- Verma, S.; McMurray, J.J. SGLT2 inhibitors and mechanisms of cardiovascular benefit: A state-of-the-art review. Diabetologia 2018, 61, 2108–2117. [Google Scholar] [CrossRef]
- Raskin, P. Sodium–glucose cotransporter inhibition: Therapeutic potential for the treatment of type 2 diabetes mellitus. Diabetes/Metab. Res. Rev. 2013, 29, 347–356. [Google Scholar] [CrossRef]
- Kaplan, A.; Abidi, E.; El-Yazbi, A.; Eid, A.; Booz, G.W.; Zouein, F.A. Direct cardiovascular impact of SGLT2 inhibitors: Mechanisms and effects. Heart Fail. Rev. 2018, 23, 419–437. [Google Scholar] [CrossRef]
- Fathi, A.; Vickneson, K.; Singh, J.S. SGLT2-inhibitors; more than just glycosuria and diuresis. Heart Fail. Rev. 2021, 26, 623–642. [Google Scholar] [CrossRef]
- Briasoulis, A.; Androulakis, E.; Christophides, T.; Tousoulis, D. The role of inflammation and cell death in the pathogenesis, progression and treatment of heart failure. Heart Fail. Rev. 2016, 21, 169–176. [Google Scholar] [CrossRef]
- Iannantuoni, F.; de Marañon, A.M.; Diaz-Morales, N.; Falcon, R.; Bañuls, C.; Abad-Jimenez, Z.; Victor, V.M.; Hernandez-Mijares, A.; Rovira-Llopis, S. The SGLT2 inhibitor empagliflozin ameliorates the inflammatory profile in type 2 diabetic patients and promotes an antioxidant response in leukocytes. J. Clin. Med. 2019, 8, 1814. [Google Scholar] [CrossRef] [PubMed]
- Heerspink, H.J.L.; Perco, P.; Mulder, S.; Leierer, J.; Hansen, M.K.; Heinzel, A.; Mayer, G. Canagliflozin reduces inflammation and fibrosis biomarkers: A potential mechanism of action for beneficial effects of SGLT2 inhibitors in diabetic kidney disease. Diabetologia 2019, 62, 1154–1166. [Google Scholar] [CrossRef] [PubMed]
- Leng, W.; Wu, M.; Pan, H.; Lei, X.; Chen, L.; Wu, Q.; Ouyang, X.; Liang, Z. The SGLT2 inhibitor dapagliflozin attenuates the activity of ROS-NLRP3 inflammasome axis in steatohepatitis with diabetes mellitus. Ann. Transl. Med. 2019, 7, 429. [Google Scholar] [CrossRef]
- Youm, Y.-H.; Nguyen, K.Y.; Grant, R.W.; Goldberg, E.L.; Bodogai, M.; Kim, D.; D’Agostino, D.; Planavsky, N.; Lupfer, C.; Kanneganti, T.-D.; et al. The ketone metabolite β-hydroxybutyrate blocks NLRP3 inflammasome–mediated inflammatory disease. Nat. Med. 2015, 21, 263–269. [Google Scholar] [CrossRef]
- Sano, M.; Takei, M.; Shiraishi, Y.; Suzuki, Y. Increased hematocrit during sodium-glucose cotransporter 2 inhibitor therapy indicates recovery of tubulointerstitial function in diabetic kidneys. J. Clin. Med. Res. 2016, 8, 844. [Google Scholar] [CrossRef]
- Lee, H.K. Cardiorenal protective effect of sodium–glucose cotransporter 2 inhibitors and mitochondrial function. J. Diabetes Investig. 2019, 10, 557–559. [Google Scholar] [CrossRef] [PubMed]
- Vallon, V.; Thomson, S.C. The tubular hypothesis of nephron filtration and diabetic kidney disease. Nat. Rev. Nephrol. 2020, 16, 317–336. [Google Scholar] [CrossRef]
- Fujita, Y.; Inagaki, N. Renal sodium glucose cotransporter 2 inhibitors as a novel therapeutic approach to treatment of type 2 diabetes: Clinical data and mechanism of action. J. Diabetes Investig. 2014, 5, 265–275. [Google Scholar] [CrossRef]
- Nishiyama, A.; Kitada, K. Possible renoprotective mechanisms of SGLT2 inhibitors. Front. Med. 2023, 10, 1115413. [Google Scholar] [CrossRef]
- Miyoshi, H.; Kameda, H.; Yamashita, K.; Nakamura, A.; Kurihara, Y. Protective effect of sodium–glucose cotransporter 2 inhibitors in patients with rapid renal function decline, stage G3 or G4 chronic kidney disease and type 2 diabetes. J. Diabetes Investig. 2019, 10, 1510–1517. [Google Scholar] [CrossRef]
- Ito, M.; Tanaka, T. The anticipated renoprotective effects of sodium-glucose cotransporter 2 inhibitors. Intern. Med. 2018, 57, 2105–2114. [Google Scholar] [CrossRef] [PubMed]
- Han, J.H.; Oh, T.J.; Lee, G.; Maeng, H.J.; Lee, D.H.; Kim, K.M.; Choi, S.H.; Jang, H.C.; Lee, H.S.; Park, K.S.; et al. The beneficial effects of empagliflozin, an SGLT2 inhibitor, on atherosclerosis in ApoE−/− mice fed a western diet. Diabetologia 2017, 60, 364–376. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.-Z.; Ye, Y.-J.; Cheng, Z.-Y.; Hu, J.-J.; Zhang, C.-B.; Qian, L.; Lu, X.-H.; Cai, X.-R. Non-invasive assessment of early stage diabetic nephropathy by DTI and BOLD MRI. Br. J. Radiol. 2020, 93, 20190562. [Google Scholar] [CrossRef]
- Packer, M. Mechanisms leading to differential hypoxia-inducible factor signaling in the diabetic kidney: Modulation by SGLT2 inhibitors and hypoxia mimetics. Am. J. Kidney Dis. 2021, 77, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Cai, T.; Ke, Q.; Fang, Y.; Wen, P.; Chen, H.; Yuan, Q.; Luo, J.; Zhang, Y.; Sun, Q.; Lv, Y.; et al. Sodium–glucose cotransporter 2 inhibition suppresses HIF-1α-mediated metabolic switch from lipid oxidation to glycolysis in kidney tubule cells of diabetic mice. Cell Death Dis. 2020, 11, 390. [Google Scholar] [CrossRef]
- Bailey, C.J. Renal glucose reabsorption inhibitors to treat diabetes. Trends Pharmacol. Sci. 2011, 32, 63–71. [Google Scholar] [CrossRef]
- Nadkarni, G.N.; Ferrandino, R.; Chang, A.; Surapaneni, A.; Chauhan, K.; Poojary, P.; Saha, A.; Ferket, B.; Grams, M.E.; Coca, S.G. Acute kidney injury in patients on SGLT2 inhibitors: A propensity-matched analysis. Diabetes Care 2017, 40, 1479–1485. [Google Scholar] [CrossRef]
- Sridhar, V.S.; Tuttle, K.R.; Cherney, D.Z. We can finally stop worrying about SGLT2 inhibitors and acute kidney injury. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2020, 76, 454–456. [Google Scholar] [CrossRef]
- Bailey, C.J.; Day, C.; Bellary, S. Renal protection with SGLT2 inhibitors: Effects in acute and chronic kidney disease. Curr. Diabetes Rep. 2022, 22, 39–52. [Google Scholar] [CrossRef]
- Salvatore, T.; Galiero, R.; Caturano, A.; Rinaldi, L.; Di Martino, A.; Albanese, G.; Di Salvo, J.; Epifani, R.; Marfella, R.; Docimo, G.; et al. An overview of the cardiorenal protective mechanisms of SGLT2 inhibitors. Int. J. Mol. Sci. 2022, 23, 3651. [Google Scholar] [CrossRef]
- Gao, Y.; Feng, S.; Wen, Y.; Tang, T.; Wang, B.; Liu, B. Cardiorenal protection of SGLT2 inhibitors-perspectives from metabolic reprogramming. EBioMedicine 2022, 83, 104215. [Google Scholar] [CrossRef]
- Paolisso, P.; Bergamaschi, L.; Cesaro, A.; Gallinoro, E.; Gragnano, F.; Sardu, C.; Mileva, N.; Foà, A.; Armillotta, M.; Sansonetti, A.; et al. Impact of SGLT2-inhibitors on contrast-induced acute kidney injury in diabetic patients with acute myocardial infarction with and without chronic kidney disease: Insight from SGLT2-I AMI PROTECT registry. Diabetes Res. Clin. Pract. 2023, 202, 110766. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Drug | Patient Number | Mean Age (Years Old) | Follow Up (Years) |
|---|---|---|---|---|
| EMPA-REG, 2015, Zinman et al. [28] | Empagliflozin | 7020 | 63.2 | 3.1 |
| CANVAS Program, 2017, Neal et al. [29] | Canagliflozin | 10,142 | 63.3 | 3.6 |
| DECLARE-TIMI 58, 2019, Wiviott et al. [30] | Dapagliflozin | 17,160 | 63.9 | 4.2 |
| CREDENCE, 2019, Perkovic et al. [31] | Canagliflozin | 4401 | 63 | 2.62 |
| DAPA-HF, 2019, McMurray et al. [32] | Dapagliflozin | 4744 | 66 | 1.5 |
| DAPA-CKD, 2020, Heerspink et al. [33] | Dapagliflozin | 4304 | 61.8 | 2.4 |
| VERTIS-CV, 2020, Cannon et al. [34] | Ertugliflozin | 8246 | 64.4 | 3.5 |
| EMPEROR-R, 2020, Packer et al. [35] | Empagliflozin | 3730 | 66.9 | 1.3 |
| SCORED, 2021, Bhatt et al. [36] | Sotagliflozin | 10,584 | 69 | 1.3 |
| SOLOIST-WHF, 2021, Bhatt et al. [37] | Sotagliflozin | 1222 | 70 | 0.75 |
| EMPEROR-P, 2021, Anker et al. [38] | Empagliflozin | 5988 | 71.9 | 2.2 |
| DELIVER, 2022, Solomon et al. [39] | Dapagliflozin | 6263 | 71.7 | 2.3 |
| EMPA-KIDNEY, 2023, The Empa-Kidney Collaboration Group [40] | Empagliflozin | 6609 | 63.8 | 2 |
| Study | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting |
|---|---|---|---|---|---|---|
| EMPA-REG, 2015, Zinman et al. [28] | L | L | L | L | L | L |
| L | L | L | L | L | L | |
| CANVAS Program, 2017, Neal et al. [29] | L | L | L | L | L | L |
| L | L | L | L | L | L | |
| DECLARE-TIMI 58, 2019, Wiviott et al. [30] | L | L | L | L | L | L |
| L | L | L | L | L | L | |
| CREDENCE, 2019, Perkovic et al. [31] | L | L | L | L | L | L |
| L | L | L | L | L | L | |
| DAPA-HF, 2019, McMurray et al. [32] | L | L | L | L | L | L |
| L | L | L | L | L | L | |
| DAPA-CKD, 2020, Heerspink et al. [33] | L | L | L | L | L | L |
| L | L | L | L | L | L | |
| VERTIS-CV, 2020, Cannon et al. [34] | L | L | L | L | L | L |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, I.-C.; Chang, H.-H.; Lai, Y.-J.; Chan, C.-M.; Sung, C.-H.; Pu, C.-M.; Chang, D.-C.; Ho, C.-C.; Hung, C.-F. Update on the Efficacy and Safety of Sodium–Glucose Co-Transporter 2 Inhibitors in Patients with Chronic Diseases: A Systematic Review and Meta-Analysis. Medicina 2025, 61, 202. https://doi.org/10.3390/medicina61020202
Liang I-C, Chang H-H, Lai Y-J, Chan C-M, Sung C-H, Pu C-M, Chang D-C, Ho C-C, Hung C-F. Update on the Efficacy and Safety of Sodium–Glucose Co-Transporter 2 Inhibitors in Patients with Chronic Diseases: A Systematic Review and Meta-Analysis. Medicina. 2025; 61(2):202. https://doi.org/10.3390/medicina61020202
Chicago/Turabian StyleLiang, I-Chia, Hsun-Hao Chang, Yu-Jou Lai, Chi-Ming Chan, Chao-Hsien Sung, Chi-Ming Pu, Der-Chen Chang, Ching-Chih Ho, and Chi-Feng Hung. 2025. "Update on the Efficacy and Safety of Sodium–Glucose Co-Transporter 2 Inhibitors in Patients with Chronic Diseases: A Systematic Review and Meta-Analysis" Medicina 61, no. 2: 202. https://doi.org/10.3390/medicina61020202
APA StyleLiang, I.-C., Chang, H.-H., Lai, Y.-J., Chan, C.-M., Sung, C.-H., Pu, C.-M., Chang, D.-C., Ho, C.-C., & Hung, C.-F. (2025). Update on the Efficacy and Safety of Sodium–Glucose Co-Transporter 2 Inhibitors in Patients with Chronic Diseases: A Systematic Review and Meta-Analysis. Medicina, 61(2), 202. https://doi.org/10.3390/medicina61020202