

The Impact of Platelet-Rich Plasma Application during Cesarean Section on Wound Healing and Postoperative Pain: A Single-Blind Placebo-Controlled Intervention Study

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
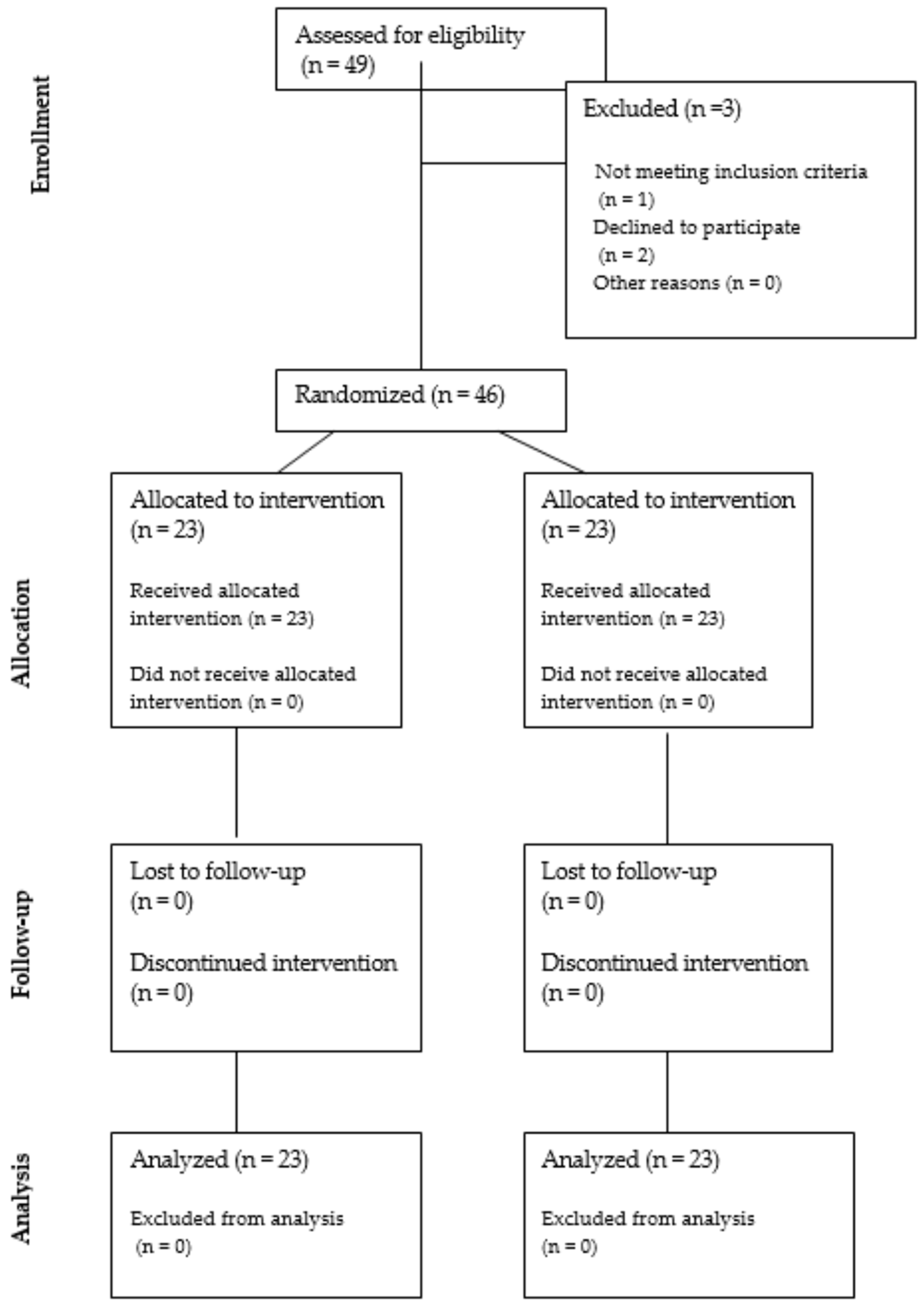
2.1. Study Population
2.2. Surgery and Postoperative Treatment
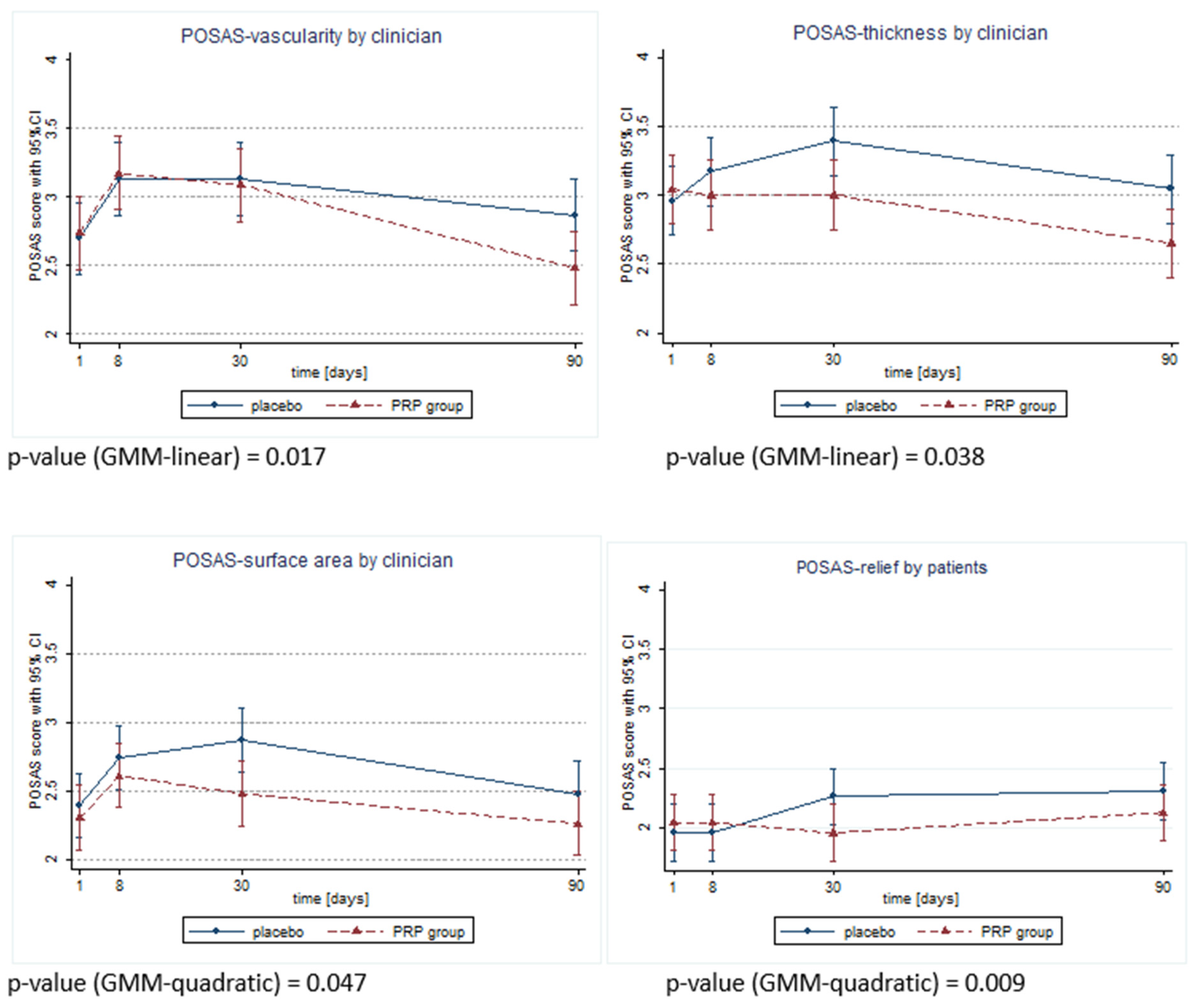
2.3. Scar Quality Assessment
2.4. Quality of Life Assessment
2.5. PRP Preparation
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dhurat, R.; Sukesh, M. Principles and Methods of Preparation of Platelet-Rich Plasma: A Review and Author’s Perspective. J. Cutan. Aesthetic Surg. 2014, 7, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.E. Platelet-Rich Plasma (PRP): What Is PRP and What Is Not PRP? Implant Dent. 2001, 10, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Everts, P.; Onishi, K.; Jayaram, P.; Lana, J.F.; Mautner, K. Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020. Int. J. Mol. Sci. 2020, 21, 7794. [Google Scholar] [CrossRef] [PubMed]
- Verma, R.; Kumar, S.; Garg, P.; Verma, Y.K. Platelet-Rich Plasma: A Comparative and Economical Therapy for Wound Healing and Tissue Regeneration. Cell Tissue Bank. 2023, 24, 285–306. [Google Scholar] [CrossRef] [PubMed]
- Lacci, K.M.; Dardik, A. Platelet-Rich Plasma: Support for Its Use in Wound Healing. Yale J. Biol. Med. 2010, 83, 1–9. [Google Scholar] [PubMed]
- Everts, P.A.; van Erp, A.; DeSimone, A.; Cohen, D.S.; Gardner, R.D. Platelet Rich Plasma in Orthopedic Surgical Medicine. Platelets 2021, 32, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Smith, O.J.; Jell, G.; Mosahebi, A. The Use of Fat Grafting and Platelet-Rich Plasma for Wound Healing: A Review of the Current Evidence. Int. Wound J. 2019, 16, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Sharara, F.I.; Lelea, L.-L.; Rahman, S.; Klebanoff, J.S.; Moawad, G.N. A Narrative Review of Platelet-Rich Plasma (PRP) in Reproductive Medicine. J. Assist. Reprod. Genet. 2021, 38, 1003–1012. [Google Scholar] [CrossRef] [PubMed]
- Varghese, J.; Acharya, N. Platelet-Rich Plasma: A Promising Regenerative Therapy in Gynecological Disorders. Cureus 2022, 14, e28998. [Google Scholar] [CrossRef]
- Dawood, A.S.; Salem, H.A. Current Clinical Applications of Platelet-Rich Plasma in Various Gynecological Disorders: An Appraisal of Theory and Practice. Clin. Exp. Reprod. Med. 2018, 45, 67–74. [Google Scholar] [CrossRef]
- Streit-Ciećkiewicz, D.; Kołodyńska, A.; Futyma-Gąbka, K.; Grzybowska, M.E.; Gołacki, J.; Futyma, K. Platelet Rich Plasma in Gynecology-Discovering Undiscovered-Review. Int. J. Environ. Res. Public Health 2022, 19, 5284. [Google Scholar] [CrossRef] [PubMed]
- Beitzel, K.; Allen, D.; Apostolakos, J.; Russell, R.P.; McCarthy, M.B.; Gallo, G.J.; Cote, M.P.; Mazzocca, A.D. US Definitions, Current Use, and FDA Stance on Use of Platelet-Rich Plasma in Sports Medicine. J. Knee Surg. 2015, 28, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Betran, A.P.; Ye, J.; Moller, A.-B.; Souza, J.P.; Zhang, J. Trends and Projections of Caesarean Section Rates: Global and Regional Estimates. BMJ Glob. Health 2021, 6, e005671. [Google Scholar] [CrossRef] [PubMed]
- Pinho, B.; Costa, A. Impact of Enhanced Recovery after Surgery (ERAS) Guidelines Implementation in Cesarean Delivery: A Systematic Review and Meta-Analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2024, 292, 201–209. [Google Scholar] [CrossRef]
- Betrán, A.P.; Ye, J.; Moller, A.-B.; Zhang, J.; Gülmezoglu, A.M.; Torloni, M.R. The Increasing Trend in Caesarean Section Rates: Global, Regional and National Estimates: 1990–2014. PLoS ONE 2016, 11, e0148343. [Google Scholar] [CrossRef] [PubMed]
- Clapp, M.A.; Barth, W.H. The Future of Cesarean Delivery Rates in the United States. Clin. Obstet. Gynecol. 2017, 60, 829–839. [Google Scholar] [CrossRef] [PubMed]
- Villar, J.; Carroli, G.; Zavaleta, N.; Donner, A.; Wojdyla, D.; Faundes, A.; Velazco, A.; Bataglia, V.; Langer, A.; Narváez, A.; et al. Maternal and Neonatal Individual Risks and Benefits Associated with Caesarean Delivery: Multicentre Prospective Study. BMJ 2007, 335, 1025. [Google Scholar] [CrossRef] [PubMed]
- Mascarello, K.C.; Horta, B.L.; Silveira, M.F. Maternal Complications and Cesarean Section without Indication: Systematic Review and Meta-Analysis. Rev. Saude Publica 2017, 51, 105. [Google Scholar] [CrossRef] [PubMed]
- Conner, S.N.; Verticchio, J.C.; Tuuli, M.G.; Odibo, A.O.; Macones, G.A.; Cahill, A.G. Maternal Obesity and Risk of Postcesarean Wound Complications. Am. J. Perinatol. 2014, 31, 299–304. [Google Scholar] [CrossRef]
- Temming, L.A.; Raghuraman, N.; Carter, E.B.; Stout, M.J.; Rampersad, R.M.; Macones, G.A.; Cahill, A.G.; Tuuli, M.G. Impact of Evidence-Based Interventions on Wound Complications after Cesarean Delivery. Am. J. Obstet. Gynecol. 2017, 217, 449.e1–449.e9. [Google Scholar] [CrossRef]
- Nunes, I.; Nicholson, W.; Theron, G.; FIGO Childbirth and Postpartum Hemorrhage Committee. FIGO Good Practice Recommendations on Surgical Techniques to Improve Safety and Reduce Complications during Cesarean Delivery. Int. J. Gynaecol. Obstet. 2023, 163 (Suppl. S2), 21–33. [Google Scholar] [CrossRef] [PubMed]
- Tehranian, A.; Esfehani-Mehr, B.; Pirjani, R.; Rezaei, N.; Sadat Heidary, S.; Sepidarkish, M. Application of Autologous Platelet-Rich Plasma (PRP) on Wound Healing After Caesarean Section in High-Risk Patients. Iran. Red Crescent Med. J. 2016, 18, e34449. [Google Scholar] [CrossRef] [PubMed]
- Elkhouly, N.I.; Elkilani, O.A.; Kolaib, H.A.; Elkhouly, R.M.; Morsi, D.I. Does Autologous Platelet-Rich Plasma Improve Wound Healing and Pain Perception after Cesarean Section in High-Risk Patients? Gynecol. Obstet. Investig. 2021, 86, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Expression of Concern. Gynecol. Obstet. Investig. 2021, 86, 554. [CrossRef] [PubMed]
- Holmgren, G.; Sjöholm, L. The Misgav Ladach Method of Caesarean Section: Evolved by Joel-Cohen and Michael Stark in Jerusalem. Trop. Doct. 1996, 26, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Holmgren, G.; Sjöholm, L.; Stark, M. The Misgav Ladach Method for Cesarean Section: Method Description. Acta Obstet. Gynecol. Scand. 1999, 78, 615–621. [Google Scholar] [CrossRef] [PubMed]
- van de Kar, A.L.; Corion, L.U.M.; Smeulders, M.J.C.; Draaijers, L.J.; van der Horst, C.M.A.M.; van Zuijlen, P.P.M. Reliable and Feasible Evaluation of Linear Scars by the Patient and Observer Scar Assessment Scale. Plast. Reconstr. Surg. 2005, 116, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Słabuszewska-Jóźwiak, A.; Szymański, J.K.; Jóźwiak, Ł.; Sarecka-Hujar, B. A Systematic Review and Meta-Analysis of Wound Complications after a Caesarean Section in Obese Women. J. Clin. Med. 2021, 10, 675. [Google Scholar] [CrossRef] [PubMed]
- Krieger, Y.; Walfisch, A.; Sheiner, E. Surgical Site Infection Following Cesarean Deliveries: Trends and Risk Factors. J. Matern.-Fetal Neonatal Med. 2017, 30, 8–12. [Google Scholar] [CrossRef]
- Smid, M.C.; Kearney, M.S.; Stamilio, D.M. Extreme Obesity and Postcesarean Wound Complications in the Maternal-Fetal Medicine Unit Cesarean Registry. Am. J. Perinatol. 2015, 32, 1336–1341. [Google Scholar] [CrossRef]
- Shaikh, H.; Robinson, S.; Teoh, T.G. Management of Maternal Obesity Prior to and during Pregnancy. Semin. Fetal. Neonatal Med. 2010, 15, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Yong, W.; Wang, J.; Leng, Y.; Li, L.; Wang, H. Role of Obesity in Female Reproduction. Int. J. Med. Sci. 2023, 20, 366–375. [Google Scholar] [CrossRef]
- Darouiche, R.O.; Wall, M.J.; Itani, K.M.F.; Otterson, M.F.; Webb, A.L.; Carrick, M.M.; Miller, H.J.; Awad, S.S.; Crosby, C.T.; Mosier, M.C.; et al. Chlorhexidine-Alcohol versus Povidone-Iodine for Surgical-Site Antisepsis. N. Engl. J. Med. 2010, 362, 18–26. [Google Scholar] [CrossRef]
- Chelmow, D.; Rodriguez, E.J.; Sabatini, M.M. Suture Closure of Subcutaneous Fat and Wound Disruption after Cesarean Delivery: A Meta-Analysis. Obstet. Gynecol. 2004, 103, 974–980. [Google Scholar] [CrossRef]
- Baaqeel, H.; Baaqeel, R. Timing of Administration of Prophylactic Antibiotics for Caesarean Section: A Systematic Review and Meta-Analysis. BJOG 2013, 120, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Cho, E.B.; Park, G.S.; Park, S.S.; Jang, Y.J.; Kim, K.H.; Kim, K.J.; Park, E.J. Effect of Platelet-Rich Plasma on Proliferation and Migration in Human Dermal Fibroblasts. J. Cosmet. Dermatol. 2019, 18, 1105–1112. [Google Scholar] [CrossRef]
- Girgin, M.; Binnetoglu, K.; Duman, K.; Kanat, B.H.; Cetinkaya, Z.; Ayten, R.; Ilhan, Y.S.; Ilhan, N.; Seker, I.; Timurkaan, N. Effects of Platelet Rich Plasma on Fascial Healing in Rats with Fecal Peritonitis. Acta Cir. Bras. 2016, 31, 314–319. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zhou, B.; Ren, J.; Ding, C.; Wu, Y.; Hu, D.; Gu, G.; Li, J. Rapidly in Situ Forming Platelet-Rich Plasma Gel Enhances Angiogenic Responses and Augments Early Wound Healing after Open Abdomen. Gastroenterol. Res. Pract. 2013, 2013, 926764. [Google Scholar] [CrossRef]
- Ren, Z.-Q.; Du, B.; Dong, H.-J.; Duan, G.-H.; Du, A.-C.; Wang, Y.; Zhao, L.-X.; Shao, W. Autologous Platelet-Rich Plasma Repairs Burn Wound and Reduces Burn Pain in Rats. J. Burn Care Res. 2022, 43, 263–268. [Google Scholar] [CrossRef]
- Martinez-Zapata, M.J.; Martí-Carvajal, A.J.; Solà, I.; Expósito, J.A.; Bolíbar, I.; Rodríguez, L.; Garcia, J.; Zaror, C. Autologous Platelet-Rich Plasma for Treating Chronic Wounds. Cochrane Database Syst. Rev. 2016, 2016, CD006899. [Google Scholar] [CrossRef]
- Gerbershagen, H.J.; Aduckathil, S.; van Wijck, A.J.M.; Peelen, L.M.; Kalkman, C.J.; Meissner, W. Pain Intensity on the First Day after Surgery: A Prospective Cohort Study Comparing 179 Surgical Procedures. Anesthesiology 2013, 118, 934–944. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, D.; Fermanian, C.; Mardaye, A.; Aegerter, P.; Pain and Regional Anesthesia Committee of the French Anesthesia and Intensive Care Society (SFAR). A Patient-Based National Survey on Postoperative Pain Management in France Reveals Significant Achievements and Persistent Challenges. Pain 2008, 137, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Maier, C.; Nestler, N.; Richter, H.; Hardinghaus, W.; Pogatzki-Zahn, E.; Zenz, M.; Osterbrink, J. The Quality of Pain Management in German Hospitals. Dtsch. Arzteblatt Int. 2010, 107, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Kehlet, H.; Jensen, T.S.; Woolf, C.J. Persistent Postsurgical Pain: Risk Factors and Prevention. Lancet 2006, 367, 1618–1625. [Google Scholar] [CrossRef] [PubMed]
- Maggioni, C.; Margola, D.; Filippi, F. PTSD, Risk Factors, and Expectations among Women Having a Baby: A Two-Wave Longitudinal Study. J. Psychosom. Obstet. Gynaecol. 2006, 27, 81–90. [Google Scholar] [CrossRef]
- Kuffler, D.P. Platelet-Rich Plasma and the Elimination of Neuropathic Pain. Mol. Neurobiol. 2013, 48, 315–332. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| PRP Group n = 23 | Placebo Group n = 23 | p-Value | |
|---|---|---|---|
| Age (years) | 31.1 ± 5.2 | 31.1 ± 5.2 | 0.700 |
| BMI (kg/m2) | 26.6 ± 2.9 | 28.1 ± 3.4 | 0.191 |
| Nullipara | 18 (78.3%) | 20 (87.0%) | 0.699 |
| Multipara | 5 (21.7%) | 3 (13.0%) | |
| Hypothyroidism | 10 (43.5%) | 9 (39.1%) | 0.765 |
| GBS colonization | 10 (43.5%) | 3 (13.0%) | 0.022 |
| PRP Group n = 23 | Placebo Group n = 23 | p-Value | |
|---|---|---|---|
| Indications for cesarean section: | 0.957 | ||
| Breech presentation | 5 (21.7%) | 4 (17.4%) | |
| Psychiatric (tocophobia) | 6 (26.1%) | 5 (21.7%) | |
| Long infertility treatment | 4 (17.4%) | 3 (13%) | |
| Fetal macrosomia | 1 (4.3%) | 1 (4.3%) | |
| Previous CS because of lack of delivery progress | 2 (8.7%) | 2 (8.7%) | |
| Neurologic | 1 (4.3%) | 4 (17.4%) | |
| Ophthalmologic | 2 (8.7%) | 2 (8.7%) | |
| Orthopedic | 1 (4.3%) | 0 | |
| Cardiologic | 1 (4.3%) | 2 (8.7%) | |
| Gestational age at delivery (weeks) | 38.9 ± 0.29 | 39.0 ± 0.48 | 0.323 |
| Neonatal birth weight (g) | 3460 ± 391 | 3474 ± 343 | 0.930 |
| Blood loss: | 0.609 | ||
| 300 mL | 3 (13%) | 4 (17.4%) | |
| 350 mL | 17 (73.9%) | 13 (56.5%) | |
| 400 mL | 3 (13%) | 5 (21.7%) | |
| 450 mL | 0 | 1 (4.3%) | |
| Duration of patient’s hospitalization (days) | 5.61 ± 1.31 | 5.35 ± 1.27 | 0.299 |
| Parameter | PRP Group n = 23 | Placebo Group n = 23 | p-Value |
|---|---|---|---|
| Day 8 | |||
| Total amount | 16.96 ± 1.52 | 17.57 ± 1.85 | 0.230 |
| Vascularity | 3.57 ± 0.84 | 3.65 ± 0.94 | 0.732 |
| Pigmentation | 3.00 ± 0.6 | 2.83 ± 0.83 | 0.446 |
| Thickness | 2.61 ± 0.66 | 2.91 ± 0.6 | 0.099 |
| Relief | 2.04 ± 0.64 | 1.96 ± 0.64 | 0.610 |
| Pliability | 3.17 ± 0.58 | 3.22 ± 0.85 | 0.842 |
| Surface area | 2.57 ± 0.59 | 3.00 ± 0.6 | 0.015 |
| Day 30 | |||
| Total amount | 17.00 ± 1.76 | 18.09 ± 2.00 | 0.033 |
| Vascularity | 3.57 ± 0.84 | 3.65 ± 0.94 | 0.732 |
| Pigmentation | 3.22 ± 0.6 | 3.04 ± 0.83 | 0.446 |
| Thickness | 2.74 ± 0.62 | 3.13 + 0.69 | 0.035 |
| Relief | 1.96 ± 0.37 | 2.26 ± 0.54 | 0.076 |
| Pliability | 3.17 ± 0.65 | 3.26 ± 0.81 | 0.691 |
| Surface area | 2.35 ± 0.71 | 2.74 ± 0.69 | 0.028 |
| Day 90 | |||
| Total amount | 14.91 ± 1.54 | 16.09 ± 1.68 | 0.021 |
| Vascularity | 2.65 ± 0.65 | 2.78 ± 0.85 | 0.607 |
| Pigmentation | 2.48 ± 0.59 | 2.48 ± 0.90 | 0.999 |
| Thickness | 2.57 ± 0.73 | 3.00 ± 0.52 | 0.019 |
| Relief | 2.13 ± 0.55 | 2.30 ± 0.56 | 0.309 |
| Pliability | 2.74 ± 0.75 | 2.74 ± 0.69 | 0.999 |
| Surface area | 2.35 ± 0.49 | 2.78 ± 0.52 | 0.015 |
| Parameter | PRP Group n = 23 | Placebo Group n = 23 | p-Value |
|---|---|---|---|
| Day 8 | |||
| Total amount | 15.61 ± 1.08 | 16.17 ± 1.44 | 0.180 |
| Vascularity | 3.17 ± 0.58 | 3.13 ± 0.63 | 0.820 |
| Pigmentation | 2.52 ± 0.59 | 2.65 ± 0.57 | 0.491 |
| Thickness | 3.00 ± 0.60 | 3.17 ± 0.49 | 0.333 |
| Relief | 1.65 ± 0.49 | 1.65 ± 0.57 | 0.999 |
| Pliability | 2.65 ± 0.65 | 2.83 ± 0.72 | 0.340 |
| Surface area | 2.61 ± 0.72 | 2.74 ± 0.54 | 0.437 |
| Day 30 | |||
| Total amount | 15.91 ± 1.24 | 17.13 ± 1.58 | 0.004 |
| Vascularity | 3.09 ± 0.60 | 3.13 ± 0.63 | 0.820 |
| Pigmentation | 2.87 ± 0.69 | 3.13 ± 0.69 | 0.169 |
| Thickness | 3.00 ± 0.60 | 3.39 + 0.72 | 0.030 |
| Relief | 1.83 ± 0.49 | 1.78 ± 0.60 | 0.806 |
| Pliability | 2.65 ± 0.65 | 2.83 ± 0.72 | 0.340 |
| Surface area | 2.48 ± 0.67 | 2.87 ± 0.63 | 0.021 |
| Day 90 | |||
| Total amount | 13.39 ± 1.53 | 14.74 ± 2.11 | 0.002 |
| Vascularity | 2.48 ± 0.59 | 2.87 ± 0.69 | 0.042 |
| Pigmentation | 1.87 ± 0.69 | 1.96 ± 0.56 | 0.646 |
| Thickness | 2.65 ± 0.71 | 3.04 ± 0.64 | 0.030 |
| Relief | 1.83 ± 0.58 | 2.00 ± 0.91 | 0.327 |
| Pliability | 2.30 ± 0.56 | 2.39 ± 0.50 | 0.633 |
| Surface area | 2.26 ± 0.45 | 2.48 ± 0.51 | 0.196 |
| PRP Group n = 23 | Placebo Group n = 23 | p-Value | |
|---|---|---|---|
| Morphine: | |||
| Mean number of doses | 9.57 ± 2.86 | 10.09 ± 1.95 | 0.738 |
| Total dose number | 30.87 ± 9.2 | 35.43 ± 10.5 | 0.132 |
| Paracetamol: | 0.006 | ||
| 1 dose per day | 11 (47.8%) | 3 (13%) | |
| 2 doses per day | 12 (52.2%) | 15 (65.2%) | |
| 3 doses per day | 0 | 5 (21.7%) | |
| The additional use of ketoprofen | 0 | 6 (26.1%) | 0.096 |
| VAS score (mean ± SD): | |||
| Immediately after surgery | 3.3 ± 2.23 | 3.96 ± 2.08 | 0.299 |
| 6 h after surgery | 4.96 ± 1.49 | 5.3 ± 1.52 | 0.465 |
| 12 h after surgery | 4.96 ± 1.36 | 5.13 ± 1.36 | 0.657 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barwijuk, M.; Pankiewicz, K.; Gałaś, A.; Nowakowski, F.; Gumuła, P.; Jakimiuk, A.J.; Issat, T. The Impact of Platelet-Rich Plasma Application during Cesarean Section on Wound Healing and Postoperative Pain: A Single-Blind Placebo-Controlled Intervention Study. Medicina 2024, 60, 628. https://doi.org/10.3390/medicina60040628
Barwijuk M, Pankiewicz K, Gałaś A, Nowakowski F, Gumuła P, Jakimiuk AJ, Issat T. The Impact of Platelet-Rich Plasma Application during Cesarean Section on Wound Healing and Postoperative Pain: A Single-Blind Placebo-Controlled Intervention Study. Medicina. 2024; 60(4):628. https://doi.org/10.3390/medicina60040628
Chicago/Turabian StyleBarwijuk, Michał, Katarzyna Pankiewicz, Aleksander Gałaś, Filip Nowakowski, Patrycja Gumuła, Artur J. Jakimiuk, and Tadeusz Issat. 2024. "The Impact of Platelet-Rich Plasma Application during Cesarean Section on Wound Healing and Postoperative Pain: A Single-Blind Placebo-Controlled Intervention Study" Medicina 60, no. 4: 628. https://doi.org/10.3390/medicina60040628
APA StyleBarwijuk, M., Pankiewicz, K., Gałaś, A., Nowakowski, F., Gumuła, P., Jakimiuk, A. J., & Issat, T. (2024). The Impact of Platelet-Rich Plasma Application during Cesarean Section on Wound Healing and Postoperative Pain: A Single-Blind Placebo-Controlled Intervention Study. Medicina, 60(4), 628. https://doi.org/10.3390/medicina60040628