

Tuberculosis and Nontuberculous Mycobacterial Infections in Patients with Spondyloarthritis: A Population-Based Study


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
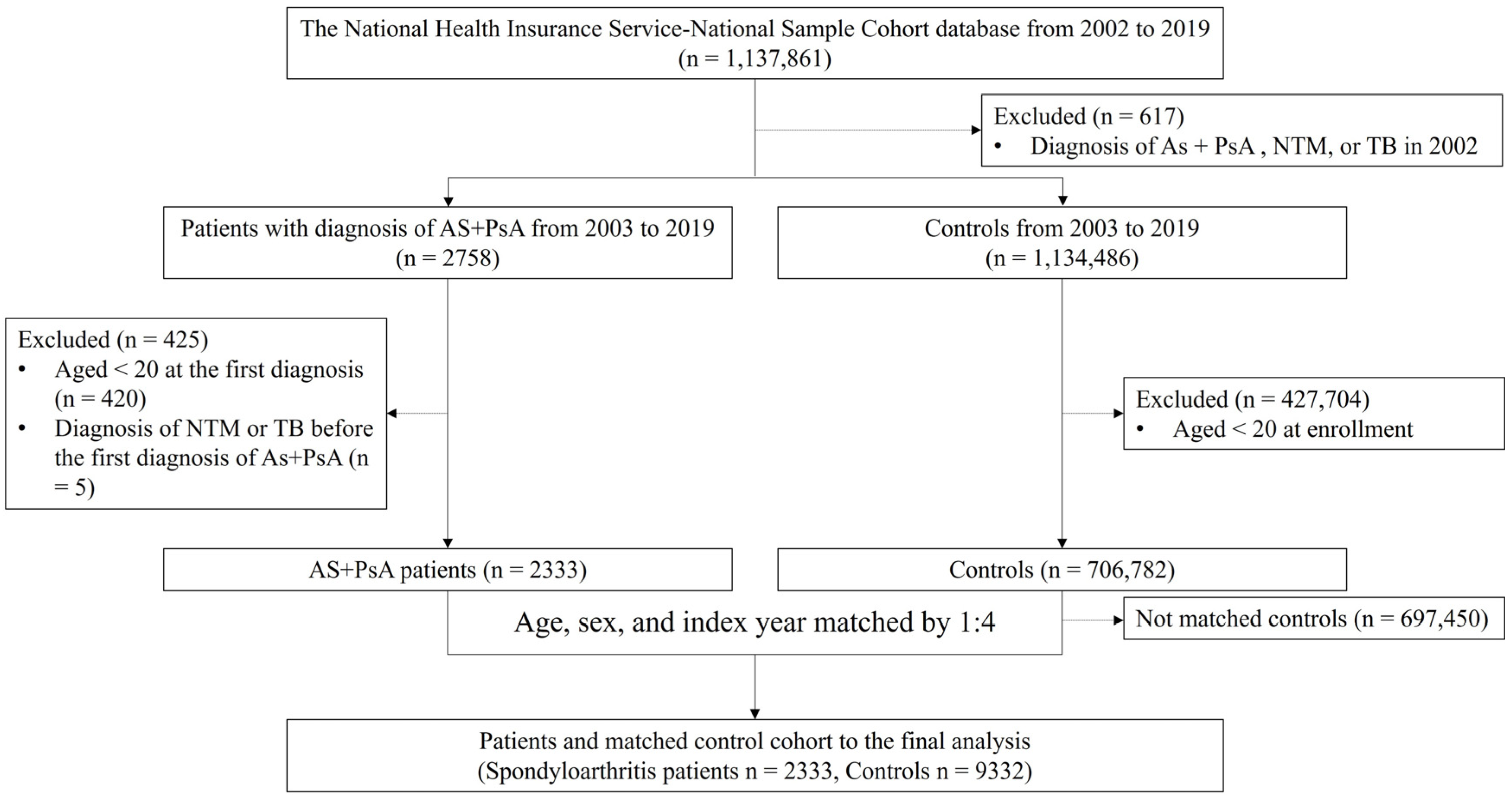
2.2. Study Population
2.3. Outcome Definition
2.4. Covariate Assessment
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cambau, E.; Drancourt, M. Steps towards the discovery of Mycobacterium tuberculosis by Robert Koch, 1882. Clin. Microbiol. Infect. 2014, 20, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Zaman, K. Tuberculosis: A global health problem. J. Health Popul. Nutr. 2010, 28, 111–113. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Tuberculosis Reports; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports (accessed on 23 August 2021).
- Forbes, B.A. Mycobacterial taxonomy. J. Clin. Microbiol. 2017, 55, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Griffith, D.E.; Aksamit, T.; Brown-Elliott, B.A.; Catanzaro, A.; Daley, C.; Gordin, F.; Holland, S.M.; Horsburgh, R.; Huitt, G.; Iademarco, M.F.; et al. An official ATS/IDSA statement: Diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am. J. Respir. Crit. Care Med. 2007, 175, 367–416. [Google Scholar] [CrossRef] [PubMed]
- Stout, J.E.; Koh, W.J.; Yew, W.W. Update on pulmonary disease due to non-tuberculous mycobacteria. Int. J. Infect. Dis. 2016, 45, 123–134. [Google Scholar] [CrossRef] [PubMed]
- Prevots, D.R.; Marras, T.K. Epidemiology of human pulmonary infection with nontuberculous mycobacteria: A review. Clin. Chest Med. 2015, 36, 13–34. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.S.; Kim, J.K.; Choi, Q.; Kim, J.W. Distribution of Mycobacterium tuberculosis in Korea in the preceding decade. J. Clin. Lab. Anal. 2018, 32, e22325. [Google Scholar] [CrossRef] [PubMed]
- Park, S.C.; Kang, M.J.; Han, C.H.; Lee, S.M.; Kim, C.J.; Lee, J.M.; Kang, Y.A. Prevalence, incidence, and mortality of nontuberculous mycobacterial infection in Korea: A nationwide population-based study. BMC Pulm. Med. 2019, 19, 140. [Google Scholar] [CrossRef] [PubMed]
- Ozgocmen, S.; Khan, M.A. Current concept of spondyloarthritis: Special emphasis on early referral and diagnosis. Curr. Rheumatol. Rep. 2012, 14, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Burgos-Vargas, R. The assessment of the spondyloarthritis international society concept and criteria for the classification of axial spondyloarthritis and peripheral spondyloarthritis: A critical appraisal for the pediatric rheumatologist. Pediatr. Rheumatol. Online J. 2012, 10, 14. [Google Scholar] [CrossRef] [PubMed]
- Makos, A.; Kuiper, J.H.; Kehoe, O.; Amarasena, R. Psoriatic arthritis: Review of potential biomarkers predicting response to TNF inhibitors. Inflammopharmacology 2023, 31, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Sieper, J.; Poddubnyy, D. Axial spondyloarthritis. Lancet 2017, 390, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Sartori, N.S.; Picon, P.; Papke, A.; Neyeloff, J.L.; da Silva Chakr, R.M. A population-based study of tuerculosis incidence among rheumatic disease patients under anti-TNF treatment. PLoS ONE 2019, 14, e0224963. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Xu, Y.; Yang, L.; Guo, L.; Jiang, X. Short-term risk and long-term incidence rate of infection and malignancy with IL-17 and IL-23 inhibitors in adult patients with psoriasis and psoriatic arthritis: A systematic review and meta-analysis. Front. Immunol. 2023, 14, 1294416. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, M.; Warren, R.B.; Torres, T. Risk of tuberculosis reactivation with interleukin (IL)-17 and IL-23 inhibitors in psoriasis—time for a paradigm change. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 824–834. [Google Scholar] [CrossRef] [PubMed]
- Al-Sohaim, A.; Bawazir, A.S.; Al-Turki, T.; Alsafi, E.O.; Al-Roqy, A.; Layqah, L.; Baharoone, S.A. The risk of tuberculosis infection in 410 Saudipatients receiving adalimumab therapy. Ann. Saudi Med. 2021, 41, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.J.; Cho, S.K.; Kim, H.; Kim, H.W.; Nam, E.; Bae, S.C.; Yoo, D.H.; Sung, Y.K. Risk of tuberculosis development in patients with rheumatoid arthritis receiving targeted therapy: A prospective Single Center cohort study. J. Korean Med. Sci. 2021, 36, e70. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.W.; Kim, E.H.; Lee, M.; Jung, I.; Ahn, S.S. Risk of cancer, tuberculosis and serious infections in patients with ankylosing spondylitis, psoriatic arthritis and psoriasis treated with IL-17 and TNF-α inhibitors: A nationwide nested case-control analysis. Clin. Exp. Rheumatol. 2023, 41, 1491–1499. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Spondyloarthritis Patients | Controls | p-Value |
|---|---|---|---|
| N | 2333 | 9332 | |
| Female, N (%) | 1155 (49.51) | 4620 (49.51) | >0.999 |
| Age, years, N (%) | >0.999 | ||
| 20–29 | 164 (7.03) | 656 (7.03) | |
| 30–39 | 400 (17.15) | 1600 (17.15) | |
| 40–49 | 425 (18.22) | 1700 (18.22) | |
| 50–59 | 415 (17.79) | 1660 (17.79) | |
| 60–69 | 461 (19.76) | 1844 (19.76) | |
| 70–79 | 355 (15.22) | 1420 (15.22) | |
| ≥80 | 113 (4.84) | 452 (4.84) | |
| Morbidly obese (BMI ≥30.0), N (%) | 31 (1.33) | 108 (1.16) | 0.728 |
| Ever-smoker, N (%) | 616 (26.40) | 2501 (26.80) | <0.0001 |
| Level of health insurance fees, N (%) | 0.577 | ||
| 0–4 | 803 (34.42) | 3232 (34.63) | |
| 5–6 | 413 (17.70) | 1617 (17.33) | |
| 7–8 | 501 (21.47) | 2111 (22.62) | |
| 9–10 | 616 (26.40) | 2372 (25.42) | |
| Comorbidity (ICD-10 code), N (%) | |||
| Hypertension (I10–I15) | 898 (38.49) | 3137 (33.62) | <0.0001 |
| Diabetes (E10–E14) | 212 (9.09) | 775 (8.30) | 0.241 |
| Dyslipidemia (E78) | 9 (0.39) | 35 (0.38) | 0.999 |
| Renal failure (N17–N19) | 15 (0.64) | 73 (0.78) | 0.574 |
| Ischemic heart disease (I20–I25) | 78 (3.34) | 194 (2.08) | <0.0001 |
| Cerebrovascular disease (I60–I69) | 88 (3.77) | 259 (2.78) | 0.014 |
| Use of biological agents, N (%) | <0.0001 | ||
| TNF-α inhibitors | 224 (9.60) | 2 (0.02) | |
| IL-17 inhibitors | 1 (0.04) | 0 (0.00) |
| Variables | SpA (N = 2333) | Controls (N = 9332) | IRR (95% CI) of NTM | ||||
|---|---|---|---|---|---|---|---|
| N (%) | PY | IR | N (%) | PY | IR | ||
| Overall | 4 (0.002) | 24.837 | 0.161 | 9 (0.001) | 100.078 | 0.090 | 1.789 (0.396, 4.180) |
| Male | 1 (0.000) | 12.021 | 0.083 | 3 (0.000) | 48.305 | 0.062 | 1.339 (0.118, 10.912) |
| Female | 3 (0.001) | 12.825 | 0.234 | 6 (0.001) | 51.773 | 0.116 | 2.017 (0.339, 5.423) |
| Age, years | |||||||
| 20–29 | 0 (0.000) | 2.274 | 0.000 | 0 (0.000) | 9.180 | 0.000 | - |
| 30–39 | 0 (0.000) | 4.385 | 0.000 | 0 (0.000) | 17.511 | 0.000 | - |
| 40–49 | 1 (0.000) | 4.420 | 0.226 | 2 (0.000) | 17.600 | 0.114 | 1.982 (0.122, 14.846) |
| 50–59 | 2 (0.001) | 4.278 | 0.468 | 1 (0.000) | 17.156 | 0.058 | 8.069 (0.225, 27.312) |
| 60–69 | 1 (0.000) | 5.304 | 0.189 | 4 (0.000) | 21.215 | 0.189 | 1.000 (0.112, 8.947) |
| 70–79 | 0 (0.000) | 3.404 | 0.000 | 2 (0.000) | 14.174 | 0.141 | - |
| ≥80 | 0 (0.000) | 0.772 | 0.000 | 0 (0.000) | 3.242 | 0.000 | - |
| Variables | SpA (N = 2333) | Controls (N = 9332) | IRR (95% CI) of MTB | ||||
|---|---|---|---|---|---|---|---|
| N (%) | PY | IR | N (%) | PY | IR | ||
| Overall | 37 (0.016) | 24.664 | 1.500 | 101 (0.011) | 99.727 | 1.013 | 1.481 (0.814, 1.728) |
| Male | 24 (0.010) | 11.888 | 2.019 | 48 (0.005) | 48.143 | 0.997 | 2.025 (0.832, 2.218) |
| Female | 13 (0.006) | 12.776 | 1.018 | 53 (0.006) | 51.584 | 1.027 | 0.991 (0.543, 1.827) |
| Age, years | |||||||
| 20–29 | 2 (0.001) | 2.262 | 0.884 | 2 (0.000) | 9.176 | 0.218 | 4.055 (0.259, 13.040) |
| 30–39 | 3 (0.001) | 4.360 | 0.688 | 4 (0.000) | 17.486 | 0.229 | 3.004 (0.361, 7.205) |
| 40–49 | 3 (0.001) | 4.401 | 0.682 | 14 (0.002) | 17.529 | 0.799 | 0.854 (0.268, 3.249) |
| 50–59 | 7 (0.003) | 4.238 | 1.652 | 15 (0.002) | 17.081 | 0.878 | 1.882 (0.537, 3.227) |
| 60–69 | 13 (0.006) | 5.258 | 2.472 | 33 (0.004) | 21.120 | 1.563 | 1.582 (0.642, 2.318) |
| 70–79 | 8 (0.003) | 3.382 | 2.365 | 25 (0.003) | 14.120 | 1.771 | 1.335 (0.511, 2.514) |
| ≥80 | 1 (0.000) | 0.763 | 1.311 | 8 (0.001) | 3.215 | 2.488 | 0.527 (0.095, 6.054) |
| Variables | SpA Treated with Biologics | Controls (N = 9332) | IRR (95% CI) | ||||
|---|---|---|---|---|---|---|---|
| N (%) | PY | IR | N (%) | PY | IR | ||
| NTM | |||||||
| Overall | 1 (0.004) | 1.965 | 0.509 | 9 (0.001) | 100.078 | 0.090 | 5.656 (0.269, 16.752) |
| Male | 1 (0.004) | 1.588 | 0.630 | 3 (0.000) | 48.305 | 0.062 | 10.161 (0.285, 26.316) |
| Female | 0 (0.000) | 0.377 | 0.000 | 6 (0.001) | 51.773 | 0.116 | - |
| MTB | |||||||
| Overall | 6 (0.027) | 1.930 | 3.109 | 101 (0.011) | 99.727 | 1.013 | 3.069 (0.714, 3.708) |
| Male | 6 (0.027) | 1.553 | 3.863 | 48 (0.005) | 48.143 | 0.997 | 3.875 (0.771, 4.208) |
| Female | 0 (0.000) | 0.377 | 0.0 00 | 53 (0.006) | 51.584 | 1.027 | - |
| Outcomes | No. of Events | Unadjusted HR (95% CI) | p-Value | Adjusted Model 1 HR (95% CI) 1 | p-Value | Adjusted Model 2 HR (95% CI) 2 | p-Value | |
|---|---|---|---|---|---|---|---|---|
| SpA (N = 2333, 24,650 PY) | Control (N = 9332, 99,694 PY) | |||||||
| NTM | 4 | 9 | 1.793 (0.552, 5.821) | 0.332 | 1.753 (0.538, 5.712) | 0.352 | 1.373 (0.378, 4.989) | 0.630 |
| MTB | 37 | 101 | 1.482 (1.017, 2.160) | 0.041 * | 1.479 (1.013, 2.158) | 0.043 * | 1.303 (0.872, 1.947) | 0.196 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.; Jang, H.-a.; Cho, H.; Im, Y.H.; Kim, J.H. Tuberculosis and Nontuberculous Mycobacterial Infections in Patients with Spondyloarthritis: A Population-Based Study. Medicina 2024, 60, 579. https://doi.org/10.3390/medicina60040579
Yang J, Jang H-a, Cho H, Im YH, Kim JH. Tuberculosis and Nontuberculous Mycobacterial Infections in Patients with Spondyloarthritis: A Population-Based Study. Medicina. 2024; 60(4):579. https://doi.org/10.3390/medicina60040579
Chicago/Turabian StyleYang, Jiyoul, Hyun-a Jang, Hyunjeong Cho, Yo Han Im, and Ji Hyoun Kim. 2024. "Tuberculosis and Nontuberculous Mycobacterial Infections in Patients with Spondyloarthritis: A Population-Based Study" Medicina 60, no. 4: 579. https://doi.org/10.3390/medicina60040579
APA StyleYang, J., Jang, H.-a., Cho, H., Im, Y. H., & Kim, J. H. (2024). Tuberculosis and Nontuberculous Mycobacterial Infections in Patients with Spondyloarthritis: A Population-Based Study. Medicina, 60(4), 579. https://doi.org/10.3390/medicina60040579