
Safety and Efficacy of Moderate-Intensity Stereotactic Body Radiation Therapy for Ultra-Central Lung Tumor


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Evaluation and Statistics
2.3. SBRT Procedure
3. Results
3.1. Patient Characteristics
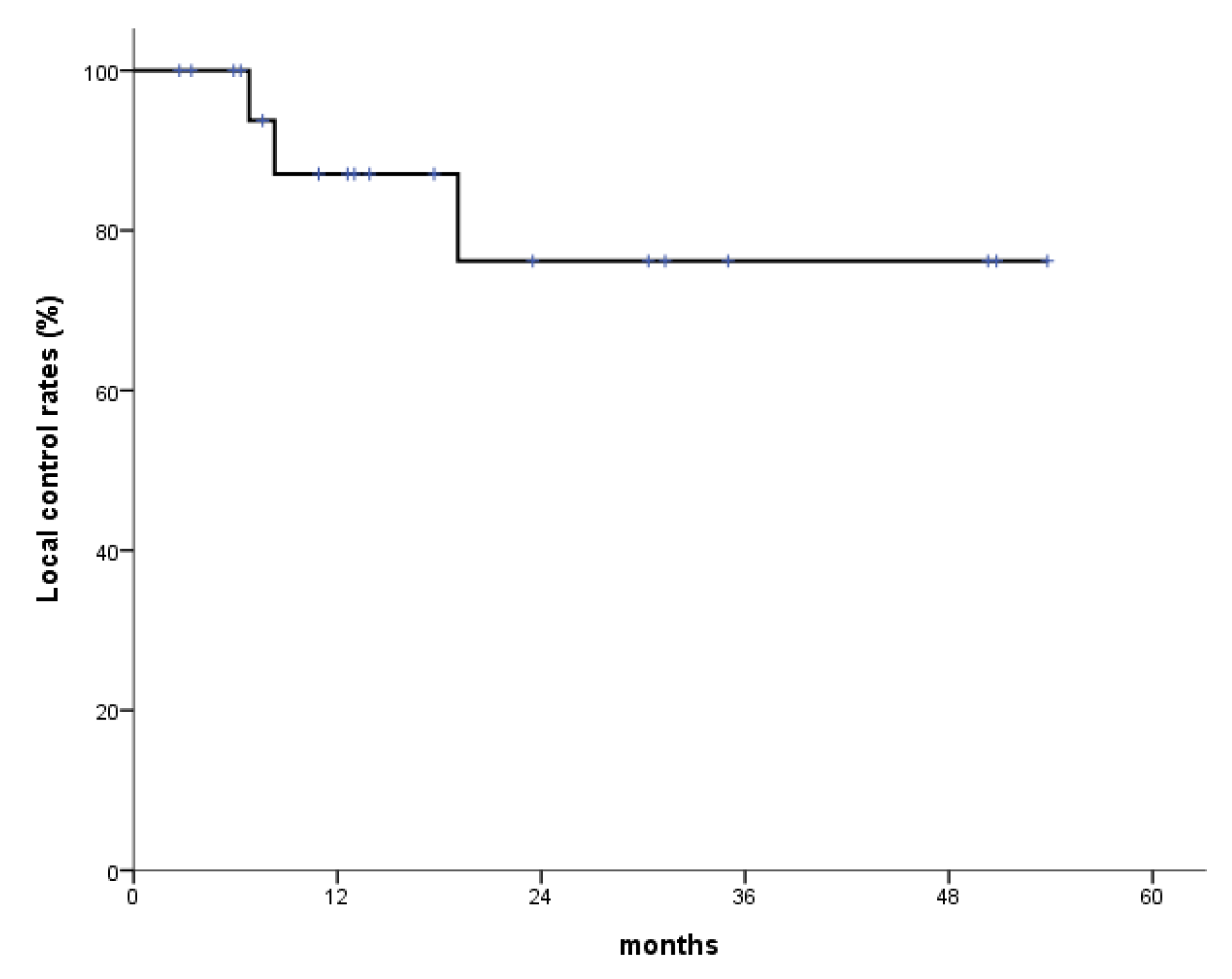
3.2. Local Control, OS, and Toxicities
3.3. Complete Response
3.4. Partial Response
3.5. PD and a Case of Fatal Hemoptysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guckenberger, M.; Andratschke, N.; Alheit, H.; Holy, R.; Moustakis, C.; Nestle, U.; Sauer, O.; Deutschen Gesellschaft für Radioonkologie (DEGRO). Definition of stereotactic body radiotherapy: Principles and practice for the treatment of stage I non-small cell lung cancer. Strahlenther. Onkol. 2014, 190, 26–33. [Google Scholar] [CrossRef]
- Chang, J.Y.; Senan, S.; Paul, M.A.; Mehran, R.J.; Louie, A.V.; Balter, P.; Groen, H.J.; McRae, S.E.; Widder, J.; Feng, L.; et al. Stereotactic ablative radiotherapy versus lobectomy for operable stage I non-small-cell lung cancer: A pooled analysis of two randomised trials. Lancet Oncol. 2015, 16, 630–637. [Google Scholar] [CrossRef]
- National Cancer Comprehensive Network (NCCN). Principles of Radiation Therapy (NSCL-C), Non-Small Cell Lung Cancer. NCCN Guidelines Version 1.2023. Available online: https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf (accessed on 11 January 2024).
- Yu, T.; Shin, I.S.; Yoon, W.S.; Rim, C.H. Stereotactic Body Radiotherapy for Centrally Located Primary Non-Small-Cell Lung Cancer: A Meta-Analysis. Clin. Lung Cancer 2019, 20, e452–e462. [Google Scholar] [CrossRef]
- Corradetti, M.N.; Haas, A.R.; Rengan, R. Central-airway necrosis after stereotactic body-radiation therapy. N. Engl. J. Med. 2012, 366, 2327–2329. [Google Scholar] [CrossRef]
- Rim, C.H.; Shin, I.S.; Yoon, W.S.; Park, S. Dose-response relationship of stereotactic body radiotherapy for ultracentral tumor and comparison of efficacy with central tumor: A meta-analysis. Transl. Lung Cancer Res. 2020, 9, 1268–1284. [Google Scholar] [CrossRef]
- Rim, C.H.; Kim, Y.; Kim, C.Y.; Yoon, W.S.; Yang, D.S. Is stereotactic body radiotherapy for ultra-central lung tumor a feasible option? A systemic review and meta-analysis. Int. J. Radiat. Biol. 2019, 95, 329–337. [Google Scholar] [CrossRef]
- Park, S.; Kim, Y.; Yoon, W.S.; Rim, C.H. A preliminary experience of moderate-intensity stereotactic body radiation therapy for ultra-central lung tumor. Int. J. Radiat. Biol. 2019, 95, 1287–1294. [Google Scholar] [CrossRef]
- Brown, J.M.; Carlson, D.J.; Brenner, D.J. The tumor radiobiology of SRS and SBRT: Are more than the 5 Rs involved? Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 254–262. [Google Scholar] [CrossRef]
- Bezjak, A.; Paulus, R.; Gaspar, L.; Timmerman, R.; Straube, W.; Ryan, W.; Garces, Y.; Pu, A.; Singh, A.; Videtic, G. Efficacy and toxicity analysis of NRG Oncology/RTOG 0813 trial of stereotactic body radiation therapy (SBRT) for centrally located non-small cell lung cancer (NSCLC). Int. J. Radiat. Oncol. 2016, 96, S8. [Google Scholar] [CrossRef]
- Timmerman, R.D.; Hu, C.; Michalski, J.; Straube, W.; Galvin, J.; Johnstone, D.; Bradley, J.; Barriger, R.; Bezjak, A.; Videtic, G.M.; et al. Long-term Results of RTOG 0236: A Phase II Trial of Stereotactic Body Radiation Therapy (SBRT) in the Treatment of Patients with Medically Inoperable Stage I Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, S30. [Google Scholar] [CrossRef]
- Timmerman, R.D.; Paulus, R.; Pass, H.I.; Gore, E.M.; Edelman, M.J.; Galvin, J.; Straube, W.L.; Nedzi, L.A.; McGarry, R.C.; Robinson, C.G.; et al. Stereotactic Body Radiation Therapy for Operable Early-Stage Lung Cancer: Findings From the NRG Oncology RTOG 0618 Trial. JAMA Oncol. 2018, 4, 1263–1266. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Tekatli, H.; Haasbeek, N.; Dahele, M.; De Haan, P.; Verbakel, W.; Bongers, E.; Hashemi, S.; Nossent, E.; Spoelstra, F.; de Langen, A.J.; et al. Outcomes of Hypofractionated High-Dose Radiotherapy in Poor-Risk Patients with “Ultracentral” Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2016, 11, 1081–1089. [Google Scholar] [CrossRef]
- Haseltine, J.M.; Rimner, A.; Gelblum, D.Y.; Modh, A.; Rosenzweig, K.E.; Jackson, A.; Yorke, E.D.; Wu, A.J. Fatal complications after stereotactic body radiation therapy for central lung tumors abutting the proximal bronchial tree. Pract. Radiat. Oncol. 2016, 6, e27–e33. [Google Scholar] [CrossRef]
- Lenglet, A.; Campeau, M.P.; Mathieu, D.; Bahig, H.; Lambert, L.; Vu, T.; Roberge, D.; Bilodeau, L.; Filion, E. Risk-adapted stereotactic ablative radiotherapy for central and ultra-central lung tumours. Radiother. Oncol. 2019, 134, 178–184. [Google Scholar] [CrossRef]
- Meng, M.B.; Wang, H.H.; Zaorsky, N.G.; Sun, B.S.; Zhu, L.; Song, Y.C.; Li, F.T.; Dong, Y.; Wang, J.S.; Chen, H.M.; et al. Risk-adapted stereotactic body radiation therapy for central and ultra-central early-stage inoperable non-small cell lung cancer. Cancer Sci. 2019, 110, 3553–3564. [Google Scholar] [CrossRef]
- Chang, J.H.; Poon, I.; Erler, D.; Zhang, L.; Cheung, P. The safety and effectiveness of stereotactic body radiotherapy for central versus ultracentral lung tumors. Radiother. Oncol. 2018, 129, 277–283. [Google Scholar] [CrossRef]
- Fukuda, Y.; Homma, T.; Uno, T.; Murata, Y.; Suzuki, S.; Shiozawa, E.; Takimoto, M.; Sagara, H. Fatal rupture of pulmonary artery pseudoaneurysm after thoracic radiation therapy against lung squamous cell carcinoma: A case report and literature review. Clin. Case Rep. 2021, 9, 737–741. [Google Scholar] [CrossRef]
- Razazi, K.; Parrot, A.; Khalil, A.; Djibre, M.; Gounant, V.; Assouad, J.; Carette, M.F.; Fartoukh, M.; Cadranel, J. Severe haemoptysis in patients with nonsmall cell lung carcinoma. Eur. Respir. J. 2015, 45, 756–764. [Google Scholar] [CrossRef]
- Langendijk, J.A.; Tjwa, M.K.; de Jong, J.M.; ten Velde, G.P.; Wouters, E.F. Massive haemoptysis after radiotherapy in inoperable non-small cell lung carcinoma: Is endobronchial brachytherapy really a risk factor? Radiother. Oncol. 1998, 49, 175–183. [Google Scholar] [CrossRef]
- Huber, R.M.; Fischer, R.; Hautmann, H.; Pöllinger, B.; Häussinger, K.; Wendt, T. Does additional brachytherapy improve the effect of external irradiation? A prospective, randomized study in central lung tumors. Int. J. Radiat. Oncol. Biol. Phys. 1997, 38, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Kim, E.Y.; Ban, H.J.; Oh, I.J.; Kim, K.S.; Kim, Y.C.; Ahn, S.J. Risk factors for fatal hemoptysis after concurrent chemoradiation therapy in patients with non-small cell lung carcinoma. Chonnam Med. J. 2010, 46, 19–24. [Google Scholar] [CrossRef]
- Cong, Y.; Sun, B.; Wang, J.; Meng, X.; Xuan, L.; Zhang, J.; Liu, J.; Shen, G.; Wu, S. Outcomes and toxicity of stereotactic body radiation therapy for advanced stage ultra-central non-small cell lung cancer. Thorac. Cancer 2019, 10, 1567–1575. [Google Scholar] [CrossRef] [PubMed]
- Lodeweges, J.E.; van Rossum, P.S.N.; Bartels, M.; van Lindert, A.S.R.; Pomp, J.; Peters, M.; Verhoeff, J.J.C. Ultra-central lung tumors: Safety and efficacy of protracted stereotactic body radiotherapy. Acta Oncol. 2021, 60, 1061–1068. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.N.B.; Hause, D.J.; Novak, J.; Monjazeb, A.M.; Daly, M.E. Tumor Control and Toxicity after SBRT for Ultracentral, Central, and Paramediastinal Lung Tumors. Pract. Radiat. Oncol. 2019, 9, e196–e202. [Google Scholar] [CrossRef] [PubMed]
- Loi, M.; Franceschini, D.; Dominici, L.; Chiola, I.; Franzese, C.; D’Agostino, G.R.; Navarria, P.; Marzo, M.; Paganini, L.; Comito, T.; et al. Dose coverage impacts local control in ultra-central lung oligometastases treated with stereotactic radiotherapy. Strahlenther. Onkol. 2021, 197, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Breen, W.G.; Jeans, E.B.; Gergelis, K.R.; Garces, Y.I.; Park, S.S.; Merrell, K.W.; Peikert, T.D.; Mansfield, A.S.; Wigle, D.A.; Harmsen, W.S.; et al. Ablative radiotherapy for ultracentral lung cancers: Dosimetric, geometric, and volumetric predictors of outcomes and toxicity. Radiother. Oncol. 2021, 158, 246–252. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient ID | Age (Years), Sex | FU Period | Treatment Aim | Underlying Pulmonary Disease | Smoking Status | Stage | Location | Pathology | Recommended Treatment | Tumor Volume (cm3) | SBRT Dose | Response |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 75, F | 50.8 | Salvage s/p LULobectomy | no | never | rcT0N2 | 4R LN | ADC | Chemotherapy | 7.6 | 55 Gy/10 fx | SD |
| 2 | 57, M | 31.3 | Primary | Tuberculosis (10 years ago) | current (30PY) | cT3N0M0 | RUL bronchus | SqCC | Rt pneumonectomy | 22.5 | 50 Gy/10 fx | CR |
| 3 | 53, M | 2.7 | Salvage s/p RULobectomy | ILD, NTM | never | rcT2N0M1 | Main bronchus | ADC | Chemotherapy | 11 | 60 Gy/10 fx | PR |
| 4 | 65, M | 53.8 | Salvage s/p RULobectomy | no | never | rcT0N2 | 4R LN | ADC | Chemotherapy | 5.7 | 55 Gy/10 fx | CR |
| 5 | 68, M | 7.6 | Primary | Emphysema | ex-smoker (20PY) | cT2N0M0 | Lt hilar | LCNEC | Lt pneumonectomy | 21.3 | 50 Gy/10 fx | near CR |
| 6 | 51, M | 50.3 | Consolidation | no | ex-smoker (15PY) | ED, cT1aN1M1b | Lt subaortic, Lt hilar | SCC | Chemotherapy | 4.0 | 55 Gy/10 fx | CR |
| 7 | 62, M | 19.1 | Salvage s/p CCRT (interval 3.5 years) | Emphysema, PTE | Never | rcT0N2M0 | Lt prevascular, Lt hilar | SqCC | Chemotherapy | 67.4 | 55 Gy/10 fx | PD |
| 8 | 66, M | 5.9 | Primary | no | ex-smoker (28 PY) | cT2N0M0 | Lt main/lobar/segmental bronchi of LUL | SqCC | Lt pneumonectomy | 25.6 | 55 Gy/10 fx | CR |
| 9 | 66, M | 30.3 | Salvage | tuberculosis | current (55 PY) | rcT0N2M1 | LUL Lt prevascular | SqCC | Chemotherapy | 7.1 | 60 Gy/10 fx | PR |
| 10 | 48, F | 35.0 | Salvage | no | never | rcT0N2M1 | Rt hilar LN | ADC | Chemotherapy | 3.6 | 60 Gy/10 fx | CR |
| 11 | 62, M | 35.3 | Salvage s/p CCRT | COPD | never | rcT2N0M0 | RML/RLL central | SqCC | Chemotherapy | 29.1 | 55 Gy/10 fx | PD |
| 12 | 73, M | 13.9 | Salvage | no | never | rcT2N2M0 | RUL Rt hilar | ADC | Chemotherapy | 5.2 | 55 Gy/10 fx | near CR |
| 13 | 65, M | 12.6 | Primary | no | ex-smoker (40 PY) | cT2N1M0 | LUL Lt Interlobal LN | SqCC | Lt pneumonectomy | 47.2 | 60 Gy/10 fx | PR |
| 14 | 69, F | 12.5 | Salvage | no | never | ycT3N3M1c | LLL bronchus | ADC | Chemotherapy | 13.0 | 45 Gy/10 fx | PR |
| 15 | 58, M | 9.1 | Salvage | no | never | rcT4N0M0 | LLL | ADC | Chemotherapy | 42.2 | 50 Gy/10 fx | PD |
| 16 | 57, M | 10.9 | Salvage s/p LULobectomy | no | never | rcTxN2M0 | Lt hilar LN | LCNEC | Chemotherapy | 22.4 | 55 Gy/10 fx | near CR |
| 17 | 64, M | 3.4 | Salvage s/p LULobectomy | no | never | rcT2N3M1b | Lt subaortic LN | ADC | Chemotherapy | 87.4 | 55 Gy/10 fx | SD |
| 18 | 77, M | 13.0 | Primary | no | ex-smoker (30 PY) | cT2bN0M0 | LUL with LLL invasion | NA | Lt pneumonectomy | 28.9 | 60 Gy/10 fx | near CR |
| 19 | 68, M | 6.3 | Primary | Pneumoconiosis, COPD, old Tb (40 years ago) | ex-smoker (30 PY) | cT2N0M0 | LUL | SqCC | Lt pneumonectomy | 29.0 | 55 Gy/10 fx | PR |
| 20 | 64, M | 17.7 | Primary | COPD | ex-smoker (30 PY) | cT2N0M0 | LUL | SqCC | Lt pneumonectomy | 21.9 | 55 Gy/10 fx | near CR |
| Patient ID | Endobronchial Involvement | Anticoagulant Use | Bevacizumab Use | Dmax (%) | RT Complications (≥Grade 2) |
|---|---|---|---|---|---|
| 1 | No | No | No | 106.0 | Late grade 2 esophageal pain (3 months after SBRT) |
| 2 | Yes | No | No | 107.4 | None |
| 3 | No | Yes | No | 104.9 | None |
| 4 | No | No | No | 106.3 | None |
| 5 | Yes | Yes | No | 108.1 | None |
| 6 | No | No | No | 102.1 | Grade 2 radiation pneumonitis (3 months after SBRT) |
| 7 | No | No | No | 107 | None |
| 8 | Yes | Yes | No | 106.1 | None |
| 9 | No | No | No | 108.2 | None |
| 10 | No | No | No | 106.2 | None |
| 11 | No | No | No | 106.8 | Grade 2 radiation pneumonitis (8 months after SBRT) |
| 12 | No | No | No | 105.2 | None |
| 13 | Yes | No | No | 105.3 | None |
| 14 | Yes | No | No | 106.3 | None |
| 15 | No | Yes | No | 106.2 | None |
| 16 | No | No | No | 105.2 | None |
| 17 | No | No | No | 105.8 | None |
| 18 | No | No | No | 109.5 | None |
| 19 | Yes | No | No | 105.6 | Grade 5 massive hemoptysis (6 months after SBRT) |
| 20 | Yes | No | No | 104.7 | None |
| Study | No. of Pts (Lesions) | FU Period (Median, Months) | Tumor Location | Radiation Regimen (Gy/fx) | 2-Year LC (%) | 2-Year OS (%) | Toxicity (%, ≥Gr3) | Characteristics |
|---|---|---|---|---|---|---|---|---|
| Tekatli et al. (2016) [14] | 47 | 29.3 | UC | 60/12 | 100 | 20.1 | 38 | 38% were stageIIIA, 17% recurrent |
| Haseltine et al. (2016) [15] | 108 18 | 22.7 | Central and UC | 45/5 | - | - | 12 | Primary lung tumor (81%) and recurrent (19%) |
| Chang et al. (2018) [18] | 61 46 | 16.7 | Central vs. UC | 30–49/5 or ≥50/5 | 3.4 4.3 (LFR) | 57.7 50.4 | 3.5 8.7 | Metastatic lung cancer |
| Cong et al. (2019) [24] | 51 | 17.0 | UC | 35/5 | 54.5 (1yr) | - | 9.8 | Advanced UC-NSCLC |
| Nguyen et al. (2019) [26] | (69) (14) | 19.7 | Central and UC | 40–60/3–8 | 85 | 72 | 14.2 (≥Gr2) 14 | Central, UC and paramediastinal tumors |
| Lenglet et al. (2019) [16] | (60) (77) | 36 | Central and UC | 40–60/3–8 | 81 | Median 57 37 | 7.3 | Primary or recurrent lung cancer |
| Park et al. (2019) [8] | 8 | 7.6 | UC | 50–60/10 | 100 (1-year) | 87.5 (1-year) | 0 | Primary and recurrent |
| Lodeweges et al. (2021) [25] | 72 | 19 | UC | 60/12 | 85 | 52 | 21 | Early stage inoperable lung cancer |
| Loi (2021) [27] | 109 | 17 | UC | 50/5 or 45/6 or 48–60/8 or 50–70/10 | 78 | 55 | 6 | UC Oligometastasis (≤3) 66% NSCLC 13% Colorectal cancer |
| Breen et al. (2021) [28] | 110 | 30 | UC | 50/5 or 60/8 or 48/4 | 16 (LP) | 57 | Acute 5 Late 8 | Ablative, curative intent RT for UC NSCLC |
| Current study (2024) | 20 | 15.8 | UC | 45–60/10 | 76.2 | 62.4 | 5 | Primary (45%) and recurrent (55%) NSCLC |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rim, C.H.; Yoon, W.S.; Park, S. Safety and Efficacy of Moderate-Intensity Stereotactic Body Radiation Therapy for Ultra-Central Lung Tumor. Medicina 2024, 60, 538. https://doi.org/10.3390/medicina60040538
Rim CH, Yoon WS, Park S. Safety and Efficacy of Moderate-Intensity Stereotactic Body Radiation Therapy for Ultra-Central Lung Tumor. Medicina. 2024; 60(4):538. https://doi.org/10.3390/medicina60040538
Chicago/Turabian StyleRim, Chai Hong, Won Sup Yoon, and Sunmin Park. 2024. "Safety and Efficacy of Moderate-Intensity Stereotactic Body Radiation Therapy for Ultra-Central Lung Tumor" Medicina 60, no. 4: 538. https://doi.org/10.3390/medicina60040538
APA StyleRim, C. H., Yoon, W. S., & Park, S. (2024). Safety and Efficacy of Moderate-Intensity Stereotactic Body Radiation Therapy for Ultra-Central Lung Tumor. Medicina, 60(4), 538. https://doi.org/10.3390/medicina60040538