

Assessing the Effect of Enzymatic Debridement on the Scar Quality in Partial-Thickness Burns to Deep Dermal Burns of the Hand: A Long-Term Evaluation

Abstract
1. Introduction
2. Materials and Methods
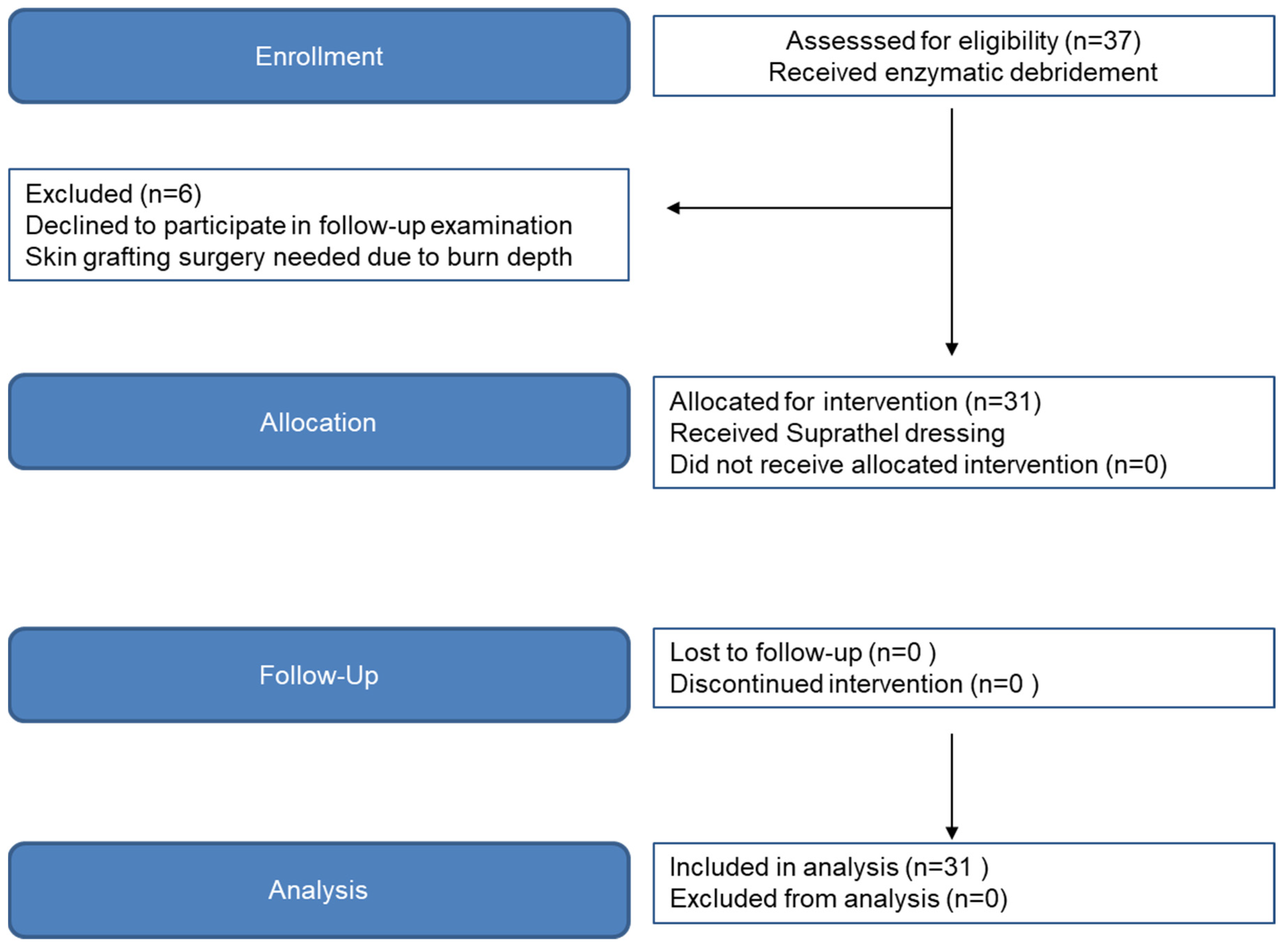
2.1. Patient Selection
2.2. Surgical Excision and Skin Grafting
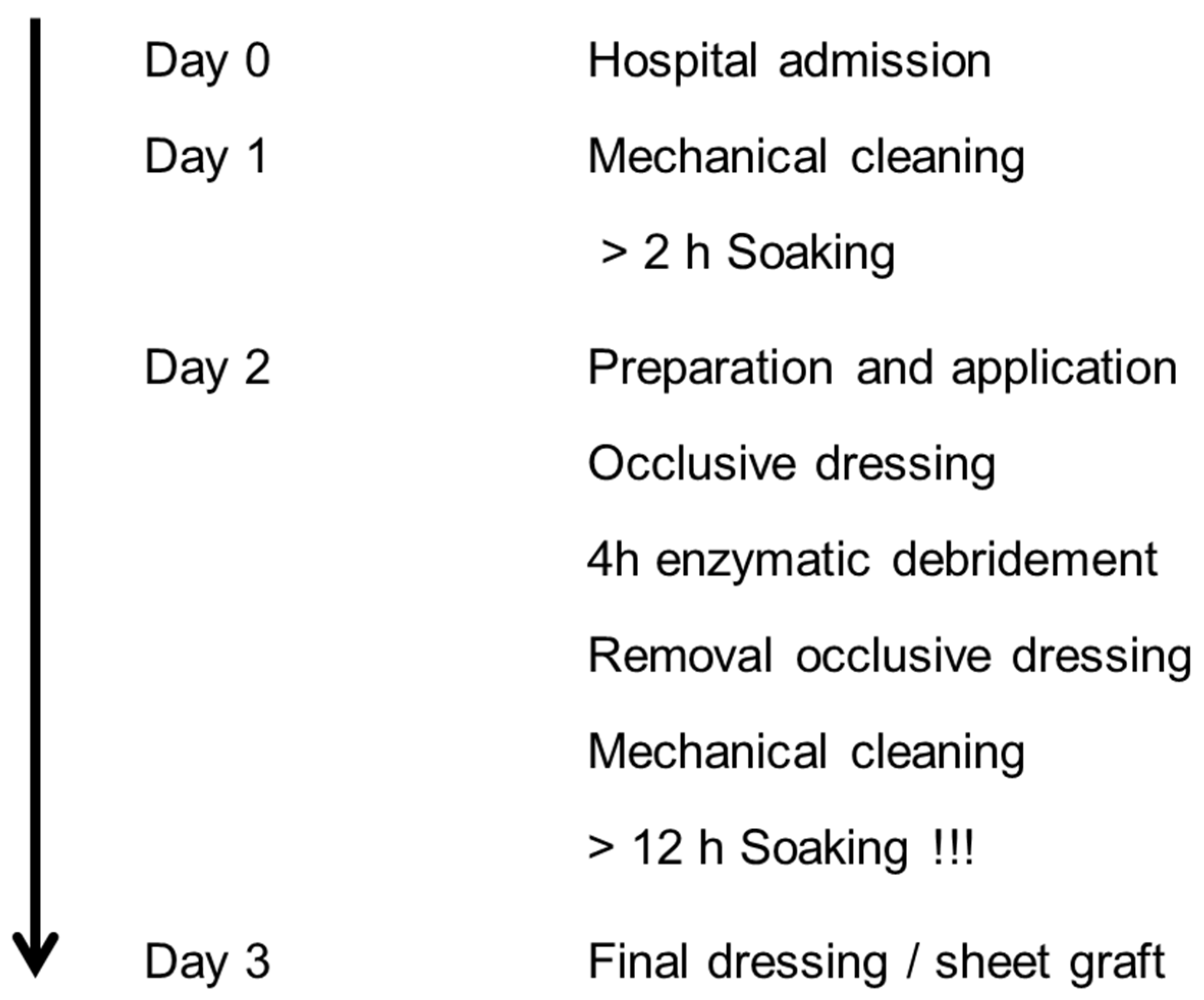
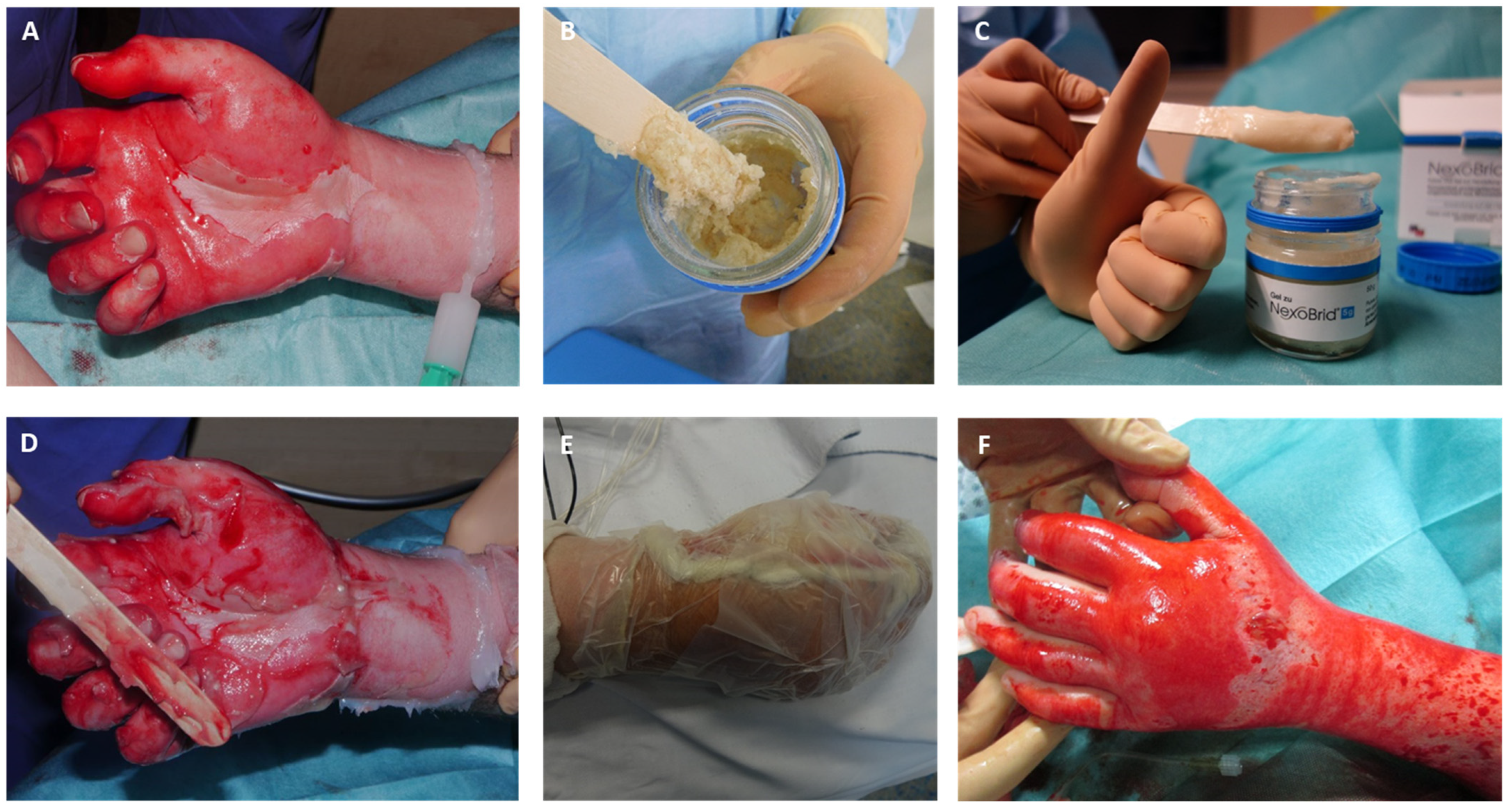
2.3. Enzymatic Debridement
2.4. Wound Evaluation
2.5. Twelve-Month Follow-Up Examination
2.6. Subjective Scar Evaluation
2.7. Objective Scar Evaluation
2.7.1. Mexameter® MX 18
2.7.2. Cutometer® Dual MPA 580
2.7.3. Tewameter TM300
2.7.4. O2C (Oxygen to See Device)
2.8. Statistical Analysis
3. Results
3.1. Enzymatic Debridement
3.2. Surgical Excision and Skin Grafting
3.3. DASH Questionnaire Result
3.4. POSAS (Patient/Observer) and Vancouver Scar Scale
3.5. Objective Scar Measurement
4. Discussion
5. Conclusions
6. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sabapathy, S.R.; Bajantri, B.; Bharathi, R.R. Management of post burn hand deformities. Indian J. Plast. Surg. Off. Publ. Assoc. Plast. Surg. India 2010, 43, S72–S79. [Google Scholar] [CrossRef]
- Germann, G.; Philipp, K. The burned hand. In Green’s Operative Hand Surgery; Elsevier Churchill Livingstone: Philadelphia, PA, USA, 2005; pp. 2159–2190. [Google Scholar]
- Philipp, K.; Gazyakan, E.; v Gregory, H.; Germann, G.; Öhlbauer, M.V.d. Erstversorgung bis zur Plastischen Chirurgie-Spezielle Behandlungsaspekte bei Verbrennungen der Hand. Der Klinikarzt. 2005, 34, 249–254. [Google Scholar] [CrossRef]
- Janzekovic, Z. A new concept in the early excision and immediate grafting of burns. J. Trauma 1970, 10, 1103–1108. [Google Scholar] [CrossRef] [PubMed]
- Krieger, Y.; Bogdanov-Berezovsky, A.; Gurfinkel, R.; Silberstein, E.; Sagi, A.; Rosenberg, L. Efficacy of enzymatic debridement of deeply burned hands. Burn. J. Int. Soc. Burn Inj. 2012, 38, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, L.; Krieger, Y.; Bogdanov-Berezovski, A.; Silberstein, E.; Shoham, Y.; Singer, A.J. A novel rapid and selective enzymatic debridement agent for burn wound management: A multi-center RCT. Burn. J. Int. Soc. Burn Inj. 2014, 40, 466–474. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, L.; Lapid, O.; Bogdanov-Berezovsky, A.; Glesinger, R.; Krieger, Y.; Silberstein, E.; Singer, A.J. Safety and efficacy of a proteolytic enzyme for enzymatic burn debridement: A preliminary report. Burn. J. Int. Soc. Burn Inj. 2004, 30, 843–850. [Google Scholar] [CrossRef] [PubMed]
- Schulz, A.; Perbix, W.; Shoham, Y.; Daali, S.; Charalampaki, C.; Fuchs, P.; Schiefer, J. Our initial learning curve in the enzymatic debridement of severely burned hands—Management and pit falls of initial treatments and our development of a post debridement wound treatment algorithm. Burn. J. Int. Soc. Burn Inj. 2016, 43, 326–336. [Google Scholar] [CrossRef] [PubMed]
- Schulz, A.; Fuchs, P.C.; Rothermundt, I.; Hoffmann, A.; Rosenberg, L.; Shoham, Y.; Oberländer, H.; Schiefer, J. Enzymatic debridement of deeply burned faces: Healing and early scarring based on tissue preservation compared to traditional surgical debridement. Burn. J. Int. Soc. Burn Inj. 2017, 43, 1233–1243. [Google Scholar] [CrossRef]
- Shoham, Y.; Gasteratos, K.; Singer, A.J.; Krieger, Y.; Silberstein, E.; Goverman, J. Bromelain-based enzymatic burn debridement: A systematic review of clinical studies on patient safety, efficacy and long-term outcomes. Int. Wound J. 2023, 20, 4364–4383. [Google Scholar] [CrossRef] [PubMed]
- Corrales-Benítez, C.; González-Peinado, D.; González-Miranda, Á.; Martínez-Méndez, J.R. Evaluation of burned hand function after enzymatic debridement. J. Plast. Reconstr. Aesthetic Surg. 2022, 75, 1048–1056. [Google Scholar] [CrossRef]
- Pertea, M.; Poroch, V.; Ciobanu, P.; Filip, A.; Velenciuc, N.; Lunca, S.; Panuta, A.; Buna-Arvinte, M.; Luca, S.; Veliceasa, B. Efficiency of Bromelain-Enriched Enzyme Mixture (NexoBrid™) in the Treatment of Burn Wounds. Appl. Sci. 2021, 11, 8134. [Google Scholar] [CrossRef]
- Singer, A.J.; McClain, S.A.; Taira, B.R.; Rooney, J.; Steinhauff, N.; Rosenberg, L. Rapid and selective enzymatic debridement of porcine comb burns with bromelain-derived Debrase: Acute-phase preservation of noninjured tissue and zone of stasis. J. Burn. Care Res. Off. Publ. Am. Burn Assoc. 2010, 31, 304–309. [Google Scholar] [CrossRef]
- Rosenberg, L.; Krieger, Y.; Silberstein, E.; Arnon, O.; Sinelnikov, I.A.; Bogdanov-Berezovsky, A.; Singer, A.J. Selectivity of a bromelain based enzymatic debridement agent: A porcine study. Burn. J. Int. Soc. Burn. Inj. 2012, 38, 1035–1040. [Google Scholar] [CrossRef]
- Heimbach, D.; Engrav, L.; Grube, B.; Marvin, J. Burn depth: A review. World J. Surg. 1992, 16, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, T.; Smith, J.; Kermode, J.; McIver, E.; Courtemanche, D.J. Rating the burn scar. J. Burn. Care Rehabil. 1990, 11, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Nedelec, B.; Correa, J.A.; Rachelska, G.; Armour, A.; LaSalle, L. Quantitative measurement of hypertrophic scar: Interrater reliability and concurrent validity. J. Burn. Care Res. Off. Publ. Am. Burn Assoc. 2008, 29, 501–511. [Google Scholar] [CrossRef] [PubMed]
- Powers, P.S.; Sarkar, S.; Goldgof, D.B.; Cruse, C.W.; Tsap, L.V. Scar assessment: Current problems and future solutions. J. Burn. Care Rehabil. 1999, 20, 54–60; Discussion 53. [Google Scholar] [CrossRef] [PubMed]
- Rennekampff, H.O.; Rabbels, J.; Reinhard, V.; Becker, S.T.; Schaller, H.E. Comparing the Vancouver Scar Scale with the cutometer in the assessment of donor site wounds treated with various dressings in a randomized trial. J. Burn. Care Res. Off. Publ. Am. Burn. Assoc. 2006, 27, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Draaijers, L.J.; Tempelman, F.R.H.; Botman, Y.A.M.; Tuinebreijer, W.E.; Middelkoop, E.; Kreis, R.W.; van Zuijlen, P.P.M. The patient and observer scar assessment scale: A reliable and feasible tool for scar evaluation. Plast. Reconstr. Surg. 2004, 113, 1960–1965; Discussion 6–7. [Google Scholar] [CrossRef] [PubMed]
- Durani, P.; McGrouther, D.A.; Ferguson, M.W. Current scales for assessing human scarring: A review. J. Plast. Reconstr. Aesthetic Surg. JPRAS 2009, 62, 713–720. [Google Scholar] [CrossRef]
- Stavrou, D.; Haik, J.; Weissman, O.; Goldan, O.; Tessone, A.; Winkler, E. Patient and observer scar assessment scale: How good is it? J. Wound Care 2009, 18, 171–176. [Google Scholar] [CrossRef]
- van de Kar, A.L.; Corion, L.U.; Smeulders, M.J.; Draaijers, L.J.; van der Horst, C.M.; van Zuijlen, P.P. Reliable and feasible evaluation of linear scars by the Patient and Observer Scar Assessment Scale. Plast. Reconstr. Surg. 2005, 116, 514–522. [Google Scholar] [CrossRef] [PubMed]
- Beaton, D.E.; Katz, J.N.; Fossel, A.H.; Wright, J.G.; Tarasuk, V.; Bombardier, C. Measuring the whole or the parts? Validity, reliability, and responsiveness of the Disabilities of the Arm, Shoulder and Hand outcome measure in different regions of the upper extremity. J. Hand Ther. Off. J. Am. Soc. Hand Ther. 2001, 14, 128–146. [Google Scholar] [CrossRef]
- Khan, W.S.; Jain, R.; Dillon, B.; Clarke, L.; Fehily, M.; Ravenscroft, M. The ‘M2 DASH’-Manchester-modified Disabilities of Arm Shoulder and Hand score. Hand 2008, 3, 240–244. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Akhtar, N. The safety and efficacy of 3% Cannabis seeds extract cream for reduction of human cheek skin sebum and erythema content. Pak. J. Pharm. Sci. 2015, 28, 1389–1395. [Google Scholar] [PubMed]
- Choi, J.S.; Moon, J.H.; Lee, J.Y.; Seo, C.H.; Jun, A.Y.; Choi, E.H.; Jang, K.U. Effect of Intradermal Injection of Placenta Hydrolysate to Postburn Hyperpigmented Skin. J. Korean Burn. Soc. 2009, 12, 135–138. [Google Scholar]
- Ostovari, N.; Saadat, N.; Nasiri, S.; Moravvej, H.; Toossi, P. The 308-nm excimer laser in the darkening of the white lines of striae alba. J. Dermatol. Treat. 2010, 21, 229–231. [Google Scholar] [CrossRef] [PubMed]
- Qian, C.Y.; Yuan, C.; Tan, Y.M.; Liu, X.P.; Dong, Y.Q.; Yang, L.J.; Wang, X.M. Comparing performance of Chromameter(R), Mexameter(R) and full-field laser perfusion imaging for measurement of ultraviolet B light-induced erythema. Clin. Exp. Dermatol. 2015, 40, 438–440. [Google Scholar] [CrossRef]
- Eo, J.; Seo, Y.K.; Baek, J.H.; Choi, A.R.; Shin, M.K.; Koh, J.S. Facial skin physiology recovery kinetics during 180 min post-washing with a cleanser. Ski. Res. Technol. 2015, 22, 148–151. [Google Scholar] [CrossRef]
- Son, I.P.; Park, K.Y.; Kim, B.; Kim, M.N. Pilot Study of the Efficacy of 578 nm Copper Bromide Laser Combined with Intralesional Corticosteroid Injection for Treatment of Keloids and Hypertrophic Scars. Ann. Dermatol. 2014, 26, 156–161. [Google Scholar] [CrossRef]
- Draaijers, L.J.; Botman, Y.A.; Tempelman, F.R.; Kreis, R.W.; Middelkoop, E.; van Zuijlen, P.P. Skin elasticity meter or subjective evaluation in scars: A reliability assessment. Burn. J. Int. Soc. Burn Inj. 2004, 30, 109–114. [Google Scholar] [CrossRef]
- Klosova, H.; Stetinsky, J.; Bryjova, I.; Hledík, S.; Klein, L. Objective evaluation of the effect of autologous platelet concentrate on post-operative scarring in deep burns. Burn. J. Int. Soc. Burn. Inj. 2013, 39, 1263–1276. [Google Scholar] [CrossRef] [PubMed]
- Woo, M.S.; Moon, K.J.; Jung, H.Y.; Park, S.R.; Moon, T.K.; Kim, N.S.; Lee, B.C. Comparison of skin elasticity test results from the Ballistometer® and Cutometer®. Ski. Res. Technol. 2014, 20, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Anthonissen, M.; Daly, D.; Fieuws, S.; Massagé, P.; Van Brussel, M.; Vranckx, J.; Kerckhove, E.V.D. Measurement of elasticity and transepidermal water loss rate of burn scars with the Dermalab®. Burn. J. Int. Soc. Burn. Inj. 2013, 39, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Atiyeh, B.S.; El-Musa, K.A.; Dham, R. Scar quality and physiologic barrier function restoration after moist and moist-exposed dressings of partial-thickness wounds. Dermatol. Surg. Off. Publ. Am. Soc. Dermatol. Surg. 2003, 29, 14–20. [Google Scholar]
- Holzle, F.; Swaid, S.; Nolte, D.; Wolff, K.D. Nutritive perfusion at donor site after microvascular fibula transfer. Microsurgery 2003, 23, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Kolbenschlag, J.; Bredenbroeker, P.; Lehnhardt, M.; Daigeler, A.; Fischer, S.; Harati, K.; Goertz, O. Advanced Microcirculatory Parameters of Lower Extremity Free Flaps during Dangling and Their Influencing Factors. J. Reconstr. Microsurg. 2015, 31, 500–507. [Google Scholar] [PubMed]
- Rothenberger, J.; Amr, A.; Schaller, H.E.; Rahmanian-Schwarz, A. Evaluation of a non-invasive monitoring method for free flap breast reconstruction using laser doppler flowmetrie and tissue spectrophotometry. Microsurgery 2013, 33, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Kowalske, K.J. Hand burns. Phys. Med. Rehabil. Clin. N. Am. 2011, 22, 249–259, vi. [Google Scholar] [CrossRef]
- Kreymerman, P.A.; Andres, L.A.; Lucas, H.D.; Silverman, A.L.; Smith, A.A. Reconstruction of the burned hand. Plast. Reconstr. Surg. 2011, 127, 752–759. [Google Scholar] [CrossRef]
- Rosenberg, L.; Shoham, Y.; Krieger, Y.; Rubin, G.; Sander, F.; Koller, J.; Singer, A.J. Minimally invasive burn care: A review of seven clinical studies of rapid and selective debridement using a bromelain-based debriding enzyme (Nexobrid(R)). Ann. Burn. Fire Disasters 2015, 28, 264–274. [Google Scholar]
- Schulz, A.; Shoham, Y.; Rosenberg, L.; Rothermund, I.; Perbix, W.; Christian Fuchs, P.; Schiefer, J.L. Enzymatic Versus Traditional Surgical Debridement of Severely Burned Hands: A Comparison of Selectivity, Efficacy, Healing Time, and Three-Month Scar Quality. J. Burn. Care Res. Off. Publ. Am. Burn Assoc. 2017, 38, e745–e755. [Google Scholar] [CrossRef] [PubMed]
- Rubin, G.; Rinott, M.; Wolovelsky, A.; Rosenberg, L.; Shoham, Y.; Rozen, N. A new bromelain-based enzyme for the release of Dupuytren’s contracture: Dupuytren’s enzymatic bromelain-based release. Bone Jt. Res. 2016, 5, 175–177. [Google Scholar] [CrossRef] [PubMed]
- Cordts, T.; Horter, J.; Vogelpohl, J.; Kremer, T.; Kneser, U.; Hernekamp, J.F. Enzymatic debridement for the treatment of severely burned upper extremities—Early single center experiences. BMC Dermatol. 2016, 16, 8. [Google Scholar] [CrossRef] [PubMed]
- Rivas-Nicolls, D.; Aguilera-Sáez, J.; Gallardo-Calero, I.; Serracanta, J.; Gomez, P.; Palao, R.; Barret, J.P. Does Enzymatic Debridement Allow Us To Perform Conservative Treatment On Clinically Deep Hand Burns? A Retrospective Review. Ann. Burn. Fire Disasters 2020, 33, 239. [Google Scholar]
- Hirche, C.; Citterio, A.; Hoeksema, H.; Koller, J.; Lehner, M.; Martinez, J.R.; Monstrey, S.; Murray, A.; Plock, J.A.; Sander, F.; et al. Eschar removal by bromelain based enzymatic debridement (Nexobrid®) in burns: An European consensus. Burn. J. Int. Soc. Burn. Inj. 2017, 43, 1640–1653. [Google Scholar] [CrossRef] [PubMed]
- Hirche, C.; Almeland, S.K.; Dheansa, B.; Fuchs, P.; Governa, M.; Hoeksema, H.; Korzeniowski, T.; Lumenta, D.B.; Marinescu, S.; Martinez-Mendez, J.R.; et al. Eschar removal by bromelain based enzymatic debridement (Nexobrid®) in burns: European consensus guidelines update. Burn. J. Int. Soc. Burn. Inj. 2020, 46, 782–796. [Google Scholar] [CrossRef] [PubMed]
- Billner, M.; Promny, D.; Reichert, B. Possibilities and limitations of enzymatic debridement in burns of the hand. Handchir. Mikrochir. Plast. Chir. Organ Der Deutschsprachigen Arbeitsgemeinschaft Fur Handchir. Organ Der Deutschsprachigen Arbeitsgemeinschaft Fur Mikrochir. Der Peripher. Nerven Und Gefasse: Organ Der V 2019, 51, 372–376. [Google Scholar]
- Billner, M.; Hofmann, N.; Jaehn, T.; Püski, T.; Reichert, B. Enzymatisches Débridement als Therapieoption bei tiefdermalen Verbrennungen der Hand. Der Unfallchirurg 2019, 122, 323–327. [Google Scholar] [CrossRef]
- Dargan, D.; Kazzazi, D.; Limnatitou, D.; Cochrane, E.; Stubbington, Y.; Shokrollahi, K.; Ralston, D. Acute Management of Thermal Hand Burns in Adults: A 10-Year Review of the Literature. Ann. Plast. Surg. 2021, 86, 517–531. [Google Scholar] [CrossRef]
- Cherubino, M.; Valdatta, L.; Baroni, T.; Pellegatta, I.; Tamborini, F.; Garutti, L.; Di Summa, P.; Adani, R. Selective Enzymatic Debridement For The Management Of Acute Upper Limb Burns. Ann. Burn. Fire Disasters 2021, 34, 328–333. [Google Scholar]
- Zacharevskij, E.; Baranauskas, G.; Varkalys, K.; Rimdeika, R.; Kubilius, D. Comparison of non-surgical methods for the treatment of deep partial thickness skin burns of the hand. Burn. J. Int. Soc. Burn. Inj. 2018, 44, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Angst, F.; Schwyzer, H.K.; Aeschlimann, A.; Simmen, B.R.; Goldhahn, J. Measures of adult shoulder function: Disabilities of the Arm, Shoulder, and Hand Questionnaire (DASH) and its short version (QuickDASH), Shoulder Pain and Disability Index (SPADI), American Shoulder and Elbow Surgeons (ASES) Society standardized shoulder assessment form, Constant (Murley) Score (CS), Simple Shoulder Test (SST), Oxford Shoulder Score (OSS), Shoulder Disability Questionnaire (SDQ), and Western Ontario Shoulder Instability Index (WOSI). Arthritis Care Res. 2011, 63 (Suppl. S11), S174–S188. [Google Scholar]
- Kennedy, C.A. The DASH and QuickDASH Outcome Measure User’s Manual; Institute for Work & Health: Toronto, ON, Canada, 2011. [Google Scholar]
- Holmes, J.D.; Muir, I.F.; Rayner, C.R. A hypothesis of the healing of deep dermal burns and the significance for treatment. Br. J. Surg. 1983, 70, 611–613. [Google Scholar] [CrossRef]
- Esposito, G.; Gravante, G.; Montone, A. Use of early dermabrasion in pediatric burn patients. Plast. Reconstr. Surg. 2006, 118, 573–575. [Google Scholar] [CrossRef]
- Gravante, G.; Delogu, D.; Esposito, G.; Montone, A. Versajet hydrosurgery versus classic escharectomy for burn débridment: A prospective randomized trial. J. Burn. Care Res. Off. Publ. Am. Burn. Assoc. 2007, 28, 720–724. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number | Treatment | Age | Comorbidities | Injury Severity Score ISS | Third-Degree Burn (%) | TBSA (%) | Fitzpatrick Skin Phototype |
|---|---|---|---|---|---|---|---|
| Patient 1 | standard deviation | 28 | nicotine abuse | 4 | 0 | 7.5 | II |
| Patient 2 | standard deviation | 28 | nicotine abuse | 4 | 0 | 7.5 | II |
| Patient 3 | standard deviation | 29 | pollinosis | 25 | 38 | 78 | II |
| Patient 4 | standard deviation | 41 | none | 25 | 25 | 59 | II |
| Patient 5 | standard deviation | 25 | none | 9 | 0 | 24 | III |
| Patient 6 | standard deviation | 25 | none | 9 | 0 | 24 | III |
| Patient 7 | standard deviation | 55 | rheumatoid arthritis, hypertension, | 9 | 0 | 13 | II |
| Patient 8 | standard deviation | 55 | chronic lumbar pain syndrome | 9 | 0 | 13 | II |
| Patient 9 | standard deviation | 52 | alcohol abuse | 9 | 0 | 17 | II |
| Patient 10 | standard deviation | 28 | none | 25 | 22 | 51.5 | II |
| Patient 11 | standard deviation | 56 | nicotine abuse | 9 | 0 | 12 | III |
| Patient 12 | standard deviation | 56 | nicotine abuse | 9 | 0 | 12 | III |
| Patient 13 | standard deviation | 18 | none | 4 | 0 | 6 | II |
| Patient 14 | standard deviation | 48 | hypertension, cholezystolithiasis | 16 | 10 | 32 | II |
| Patient 15 | standard deviation | 48 | shoulder-arm syndrome | 16 | 8 | 32 | II |
| Patient 1 | EDNX | 36 | none | 4 | 0 | 6.5 | IV |
| Patient 2 | EDNX | 15 | none | 4 | 0 | 9 | II |
| Patient 3 | EDNX | 43 | suicidality, nicotine abuse | 25 | 25 | 43.5 | II |
| Patient 4 | EDNX | 43 | nicotine abuse | 25 | 12 | 43.5 | II |
| Patient 5 | EDNX | 38 | hypertension | 4 | 0 | 6.5 | II |
| Patient 6 | EDNX | 19 | none | 1 | 0 | 1 | III |
| Patient 7 | EDNX | 51 | ASS intolerance | 1 | 0 | 1.5 | II |
| Patient 8 | EDNX | 30 | none | 4 | 0 | 5 | III |
| Patient 9 | EDNX | 30 | none | 4 | 0 | 5 | III |
| Patient 10 | EDNX | 34 | chronic gastritis | 1 | 0 | 2 | III |
| Patient 11 | EDNX | 45 | hypertension | 4 | 0 | 7.5 | II |
| Patient 12 | EDNX | 62 | none | 1 | 0 | 2.2 | II |
| Patient 13 | EDNX | 50 | chronic gastritis | 4 | 0 | 6.5 | III |
| Patient 14 | EDNX | 48 | none | 1 | 0 | 0.6 | II |
| Patient 15 | EDNX | 33 | none | 4 | 0 | 7 | II |
| Patient 16 | EDNX | 29 | nicotine abuse | 1 | 0 | 1 | II |
| Patient 17 | EDNX | 28 | none | 1 | 0 | 3 | II |
| Patient 18 | EDNX | 47 | none | 1 | 0 | 4.5 | II |
| Patient 19 | EDNX | 27 | none | 1 | 0 | 0.5 | II |
| Patient 20 | EDNX | 22 | nicotine abuse | 1 | 0 | 4 | II |
| Patient 21 | EDNX | 54 | age-related hearing loss/presbyakusis | 9 | 0 | 0.5 | II |
| Patient 22 | EDNX | 43 | none | 16 | 12 | 24.25 | II |
| Patient 23 | EDNX | 43 | none | 16 | 15 | 24.25 | II |
| Patient 24 | EDNX | 52 | alcohol abuse | 9 | 0 | 17 | II |
| Patient 25 | EDNX | 28 | none | 25 | 32 | 51.5 | II |
| Patient 26 | EDNX | 44 | nicotine abuse | 1 | 0 | 1.5 | II |
| Patient 27 | EDNX | 30 | none | 1 | 0 | 4 | III |
| Patient 28 | EDNX | 30 | none | 25 | 28 | 65 | II |
| Patient 29 | EDNX | 54 | age-related hearing loss/presbyakusis | 9 | 0 | 23.1 | IV |
| Patient 30 | EDNX | 54 | depression | 1 | 0 | 23.1 | IV |
| Patient 31 | EDNX | 33 | nicotine abuse | 4 | 0 | 9 | II |
| EDNX Scar Evaluation | STD Scar Evaluation | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Min | Max | Mean | STD | Min | Max | Mean | STD | p Value | |
| Scar painful in the past weeks | 1 | 7 | 1.87 | 1.61 | 1 | 9 | 3.33 | 2.47 | 0.006 |
| Scar itching in the past weeks | 1 | 8 | 2.71 | 1.95 | 1 | 9 | 4.80 | 2.68 | 0.009 |
| Is the scar color different from the color of your normal skin at present? | 1 | 9 | 3.71 | 1.72 | 2 | 6 | 4.20 | 1.57 | 0.313 |
| Stiffness | 1 | 7 | 3.00 | 2.00 | 1 | 10 | 4.73 | 2.34 | 0.013 |
| Thickness difference from normal skin at present | 1 | 8 | 2.87 | 1.82 | 2 | 9 | 5.07 | 2.25 | 0.002 |
| More irregular than normal skin at present | 1 | 8 | 3.19 | 1.96 | 1 | 8 | 5.40 | 2.13 | 0.002 |
| EDNX Scar Evaluation | STD Scar Evaluation | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Min | Max | Mean | STD | Min | Max | Mean | STD | p Value | |
| Vascularity | 1 | 5 | 3.00 | 1.10 | 2 | 5 | 4.07 | 0.96 | 0.003 |
| Pigmentation | 1 | 7 | 3.16 | 1.46 | 2 | 6 | 3.93 | 1.16 | 0.052 |
| Thickness | 1 | 6 | 2.87 | 1.52 | 1 | 7 | 4.40 | 1.68 | 0.005 |
| Relief | 1 | 6 | 2.81 | 1.19 | 2 | 12 | 5.40 | 2.23 | 0.000 |
| Pliability | 1 | 5 | 2.52 | 1.06 | 1 | 7 | 4.33 | 1.68 | 0.000 |
| Surface Area | 1 | 7 | 2.71 | 1.66 | 1 | 6 | 4.07 | 1.58 | 0.007 |
| Overall Opinion | 1 | 7 | 3.06 | 1.46 | 2 | 7 | 4.47 | 1.41 | 0.004 |
| Vascularity (p = 0.575) | Pliability (p = 0.184) | Pigmentation (p = 0.007) | Height (p = 0.008) | ||||
|---|---|---|---|---|---|---|---|
| EDNX | STD | EDNX | STD | EDNX | STD | EDNX | STD |
| 20% Normal | 6.7% Normal | 23.3% Normal | 6.7% Normal | 10% Normal | 13.3 % Normal | 70% Normal | 26.7% Normal |
| 63.3% Pink | 80% Pink | 43.3% Supple | 40% Supple | 46.7% Hypopigmentation | 86.7% Hypopigmentation | 26.7% <2 | 66.7% <2 |
| 16.7% Red | 13.3% Red | 23.3% Yielding | 46.7% Yielding | 43.4% Hyperpigmentation | 0% Hyperpigmentation | 3.3% >2 and <5 | 6.7% >2 and <5 |
| 6.7% Firm | 6.7% Firm | ||||||
| 3.3% Banding | 0% Banding | ||||||
| Mean | STD | Min | Max | p | |||
|---|---|---|---|---|---|---|---|
| O2C | SO2 | EDNX | 60.9 | 24.1 | 0.8 | 95.0 | 0.188 |
| Healthy skin | 65.1 | 21.2 | 14.0 | 93.0 | |||
| rHb | EDNX | 101.8 | 42.7 | 55.0 | 372.0 | 0.008 | |
| Healthy skin | 96.0 | 46.7 | 64.0 | 401.0 | |||
| Flow | EDNX | 71.0 | 73.6 | 5.0 | 303.0 | 0.915 | |
| Healthy skin | 61.1 | 47.1 | 6.0 | 238.0 | |||
| Mexameter | Melanin | EDNX | 158.1 | 98.6 | 20.5 | 430.0 | 0.969 |
| Healthy skin | 157.4 | 75.2 | 30.0 | 327.0 | |||
| Erythema | EDNX | 497.9 | 114.6 | 85.0 | 688.0 | 0.003 | |
| Healthy skin | 449.4 | 80.4 | 332.0 | 653.0 | |||
| Tewameter | Standard_AW | EDNX | 0.2 | 0.1 | 0.0 | 0.5 | 0.878 |
| Healthy skin | 0.2 | 0.1 | 0.0 | 0.5 | |||
| SSWL | EDNX | 3.0 | 2.0 | 0.3 | 8.3 | 0.284 | |
| Healthy skin | 2.7 | 1.9 | 0.4 | 8.1 | |||
| Mean | EDNX | 24.7 | 5.5 | 10.0 | 36.0 | 0.498 | |
| Healthy skin | 24.5 | 4.4 | 10.0 | 30.0 | |||
| Cutometer | R0 | EDNX | 0.9 | 0.4 | 0.3 | 2.0 | 0.100 |
| Healthy skin | 1.0 | 0.4 | 0.1 | 2.1 | |||
| R2 | EDNX | 0.8 | 0.2 | 0.0 | 1.0 | 0.203 | |
| Healthy skin | 0.8 | 0.2 | 0.0 | 1.0 | |||
| F1 | EDNX | 0.2 | 0.2 | 0.0 | 1.0 | 0.939 | |
| Healthy skin | 0.2 | 0.1 | 0.0 | 0.6 |
| Title | Author | Year | Study Aim | Wounds Included | Study Design | Burn Depth | Follow Up Period | Evaluation Tools |
|---|---|---|---|---|---|---|---|---|
| Evaluation of burned hand function after enzymatic debridement | Corrales-Benítez et al. [11] | 2022 | Evaluation of outcome | 90 hands | prospective | partial thickness | 3 months, 1 year | VSS, DASH, MHOQ, goniometer |
| Enzymatic Versus Traditional Surgical Debridement of Severely Burned Hands: A Comparison of Selectivity, Efficacy, Healing Time, and Three-Month Scar Quality | Schulz et al. [43] | 2017 | Comparison surgical versus enzymatic debridement | 20 versus 20 hands | prospective | deep dermal - full thickness | 3 months | VSS |
| Selective Enzymatic Debridement For The Management Of Acute Upper Limb Burns | Cherubino et al. [52] | 2021 | Describe the efficacy of treatment of upper limb burns with NexoBrid® in a non-burn referral center | 18 hands | retrospective | POSAS, DASH | ||
| Comparison of non-surgical methods for the treatment of deep partial thickness skin burns of the hand | Zacharecskij et al. [53] | 2018 | Comparison of 4 non-surgical methods for the treatment of deep partial thickness skin burns of the hand | 87 hands | prospective | partial thickness | 6 months | DASH, VSS |
| Acute Management of Thermal Hand Burns in Adults: A 10-Year Review of the Literature | Dargan et al. [51] | 2021 | Literature review acute thermal hand burns treatment | literature review | ||||
| A novel rapid and selective enzymatic debridement agent for burn wound management: A multi-center RCT | Rosenberg et al. [6] | 2014 | Does rapid enzymatic debridement with the debriding enzymeNexoBridTM (NXB) reduce need for surgery? Comparison surgical debridement | 31 hands versus 41 hands | prospective | partial thickness-deep dermal | 2-4 years | VSS |
| Enzymatic debridement for the treatment of severely burned upper extremities—early single center experiences | Cordts et al. [45] | 2016 | Proofing the results of enzymatic debridement in upper extremity burn wounds. | 16 hands | prospective | partial thickness - full thickness | 3 months | DASH, VSS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heitzmann, W.; Schulz, A.; Fuchs, P.C.; Schiefer, J.L. Assessing the Effect of Enzymatic Debridement on the Scar Quality in Partial-Thickness Burns to Deep Dermal Burns of the Hand: A Long-Term Evaluation. Medicina 2024, 60, 481. https://doi.org/10.3390/medicina60030481
Heitzmann W, Schulz A, Fuchs PC, Schiefer JL. Assessing the Effect of Enzymatic Debridement on the Scar Quality in Partial-Thickness Burns to Deep Dermal Burns of the Hand: A Long-Term Evaluation. Medicina. 2024; 60(3):481. https://doi.org/10.3390/medicina60030481
Chicago/Turabian StyleHeitzmann, Wolfram, Alexandra Schulz, Paul Christian Fuchs, and Jennifer Lynn Schiefer. 2024. "Assessing the Effect of Enzymatic Debridement on the Scar Quality in Partial-Thickness Burns to Deep Dermal Burns of the Hand: A Long-Term Evaluation" Medicina 60, no. 3: 481. https://doi.org/10.3390/medicina60030481
APA StyleHeitzmann, W., Schulz, A., Fuchs, P. C., & Schiefer, J. L. (2024). Assessing the Effect of Enzymatic Debridement on the Scar Quality in Partial-Thickness Burns to Deep Dermal Burns of the Hand: A Long-Term Evaluation. Medicina, 60(3), 481. https://doi.org/10.3390/medicina60030481