
Reduced Corticosteroid Exposure Is Safe and Does Not Reduce Disease Control among Hodgkin Lymphoma Patients Treated with Escalated BEACOPP (eBEACOPP)

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Treatment Regimens
2.3. Outcome Measures and Statistical Analyses
3. Results
3.1. Patient Demographics and Treatment
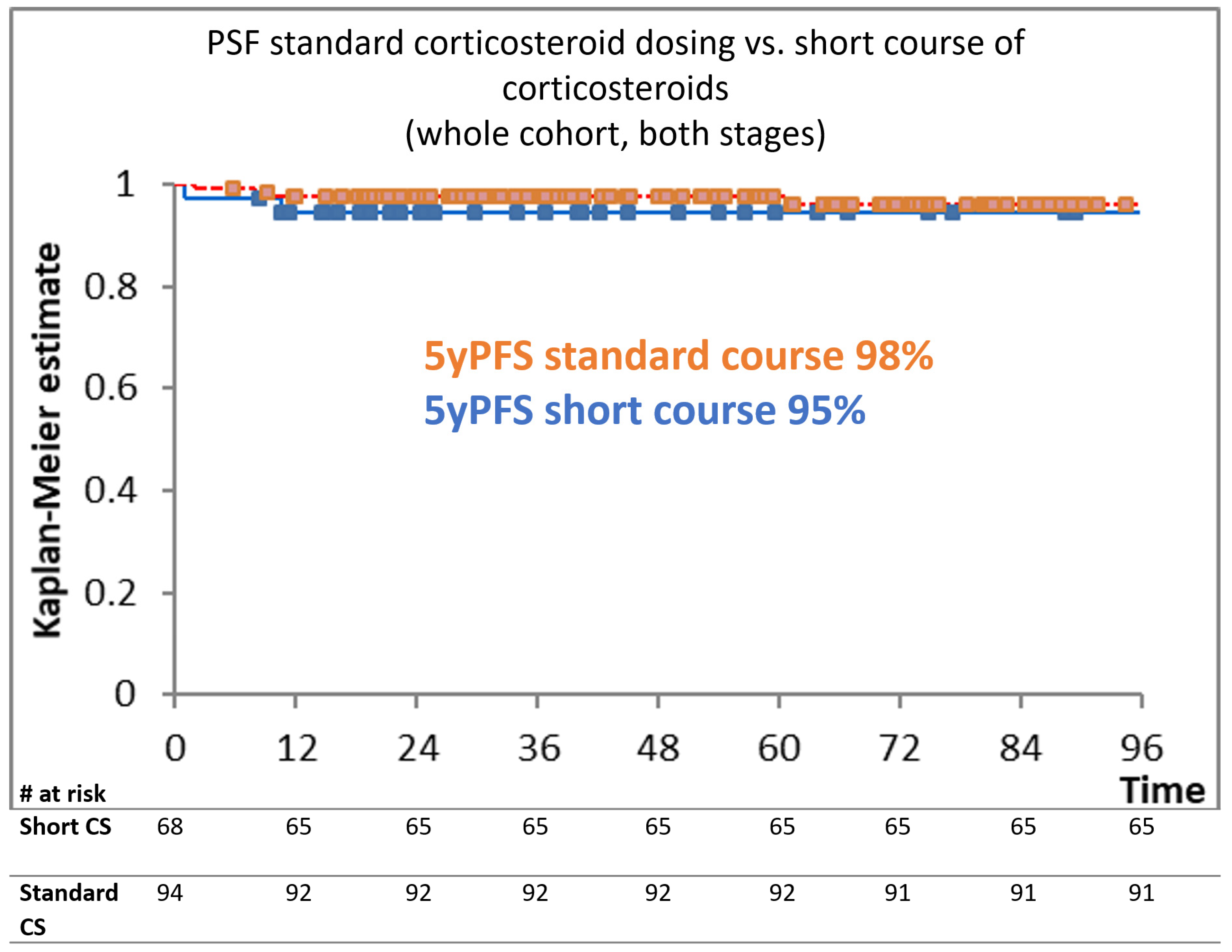
3.2. Efficacy
3.3. Toxicities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Engert, A.; Franklin, J.; Eich, H.T.; Brillant, C.; Sehlen, S.; Cartoni, C.; Herrmann, R.; Pfreundschuh, M.; Sieber, M.; Tesch, H.; et al. Two Cycles of Doxorubicin, Bleomycin, Vinblastine, and Dacarbazine Plus Extended-Field Radiotherapy Is Superior to Radiotherapy Alone in Early Favorable Hodgkin’s Lymphoma: Final Results of the GHSG HD7 Trial. J. Clin. Oncol. 2007, 25, 3495–3502. [Google Scholar] [CrossRef]
- Fermé, C.; Eghbali, H.; Meerwaldt, J.H.; Rieux, C.; Bosq, J.; Berger, F.; Girinsky, T.; Brice, P.; van’t Veer, M.B.; Walewski, J.A.; et al. Chemotherapy plus Involved-Field Radiation in Early-Stage Hodgkin’s Disease. N. Engl. J. Med. 2007, 357, 1916–1927. [Google Scholar] [CrossRef]
- Engert, A.; Plütschow, A.; Eich, H.T.; Lohri, A.; Dörken, B.; Borchmann, P.; Berger, B.; Greil, R.; Willborn, K.C.; Wilhelm, M.; et al. Reduced Treatment Intensity in Patients with Early-Stage Hodgkin’s Lymphoma. N. Engl. J. Med. 2010, 363, 640–652. [Google Scholar] [CrossRef]
- Borchmann, P.; Plütschow, A.; Kobe, C.; Greil, R.; Meissner, J.; Topp, M.S.; Ostermann, H.; Dierlamm, J.; Mohm, J.; Thiemer, J.; et al. PET-guided omission of radiotherapy in early-stage unfavourable Hodgkin lymphoma (GHSG HD17): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2021, 22, 223–234. [Google Scholar] [CrossRef] [PubMed]
- Chisesi, T.; Bellei, M.; Luminari, S.; Montanini, A.; Marcheselli, L.; Levis, A.; Gobbi, P.; Vitolo, U.; Stelitano, C.; Pavone, V.; et al. Long-term follow-up analysis of HD9601 trial comparing ABVD versus Stanford V versus MOPP/EBV/CAD in patients with newly diagnosed advanced-stage Hodgkin’s lymphoma: A study from the Intergruppo Italiano Linfomi. J. Clin. Oncol. 2011, 29, 4227–4233. [Google Scholar] [CrossRef] [PubMed]
- Fisher, R.I.; Gaynor, E.R.; Dahlberg, S.; Oken, M.M.; Grogan, T.M.; Mize, E.M.; Glick, J.H.; Coltman, C.A.; Miller, T.P. Comparison of a Standard Regimen (CHOP) with Three Intensive Chemotherapy Regimens for Advanced Non-Hodgkin’s Lymphoma. N. Engl. J. Med. 1993, 328, 1002–1006. [Google Scholar] [CrossRef] [PubMed]
- Engert, A.; Haverkamp, H.; Kobe, C.; Markova, J.; Renner, C.; Ho, A.; Diehl, V. Reduced-intensity chemotherapy and PET-guided radiotherapy in patients with advanced stage Hodgkin’s lymphoma (HD15 trial): A randomised, open-label, phase 3 non-inferiority trial. Lancet 2012, 379, 1791–1799. [Google Scholar] [CrossRef] [PubMed]
- Merli, F.; Luminari, S.; Gobbi, P.G.; Cascavilla, N.; Mammi, C.; Ilariucci, F.; Stelitano, C.; Musso, M.; Baldini, L.; Galimberti, S.; et al. Long-term results of the HD2000 trial comparing ABVD versus BEACOPP versus COPP-EBV-CAD in untreated patients with advanced hodgkin lymphoma: A study by fondazione Italiana Linfomi. J. Clin. Oncol. 2016, 34, 1175–1181. [Google Scholar] [CrossRef] [PubMed]
- Viviani, S.; Zinzani, P.L.; Rambaldi, A.; Brusamolino, E.; Levis, A.; Bonfante, V.; Vitolo, U.; Pulsoni, A.; Liberati, A.M.; Specchia, G.; et al. ABVD versus BEACOPP for Hodgkin’s Lymphoma When High-Dose Salvage Is Planned. N. Engl. J. Med. 2011, 365, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Carde, P.; Karrasch, M.; Fortpied, C.; Brice, P.; Khaled, H.; Casasnovas, O.; Caillot, D.; Gaillard, I.; Bologna, S.; Ferme, C.; et al. Eight Cycles of ABVD Versus Four Cycles of BEACOPP escalated Plus Four Cycles of BEACOPP baseline in Stage III to IV, International Prognostic Score ≥ 3, High-Risk Hodgkin Lymphoma: First Results of the Phase III EORTC 20012 Intergro. J. Clin. Oncol. 2016, 34, 2028–2036. [Google Scholar] [CrossRef] [PubMed]
- Mounier, N.; Brice, P.; Bologna, S.; Briere, J.; Gaillard, I.; Heczko, M.; Gabarre, J.; Casasnovas, O.; Jaubert, J.; Colin, P.; et al. ABVD (8 cycles) versus BEACOPP (4 escalated cycles ≥ 4 baseline): Final results in stage III–IV low-risk Hodgkin lymphoma (IPS 0–2) of the LYSA H34 randomized trial†. Ann. Oncol. 2014, 25, 1622–1628. [Google Scholar] [CrossRef] [PubMed]
- Skoetz, N.; Will, A.; Monsef, I.; Brillant, C.; Engert, A.; von Tresckow, B. Comparison of first-line chemotherapy including escalated BEACOPP versus chemotherapy including ABVD for people with early unfavourable or advanced stage Hodgkin lymphoma. Cochrane Database Syst. Rev. 2017, 5, CD007941. [Google Scholar] [CrossRef] [PubMed]
- von Tresckow, B.; Plutschow, A.; Fuchs, M.; Klimm, B.; Markova, J.; Lohri, A.; Kral, Z.; Greil, R.; Topp, M.S.; Meissner, J.; et al. Dose-intensification in early unfavorable Hodgkin’s lymphoma: Final analysis of the German Hodgkin Study Group HD14 trial. J. Clin. Oncol. 2012, 30, 907–913. [Google Scholar] [CrossRef] [PubMed]
- Eichenauer, D.A.; Thielen, I.; Haverkamp, H.; Franklin, J.; Behringer, K.; Halbsguth, T.; Klimm, B.; Diehl, V.; Sasse, S.; Rothe, A.; et al. Therapy-related acute myeloid leukemia and myelodysplastic syndromes in patients with Hodgkin lymphoma: A report from the German Hodgkin Study Group. Blood 2014, 11, 1658–1664. [Google Scholar] [CrossRef] [PubMed]
- André, M.P.E.; Carde, P.; Viviani, S.; Bellei, M.; Fortpied, C.; Hutchings, M.; Gianni, A.M.; Brice, P.; Casasnovas, O.; Gobbi, P.G.; et al. Long-term overall survival and toxicities of ABVD vs BEACOPP in advanced Hodgkin lymphoma: A pooled analysis of four randomized trials. Cancer Med. 2020, 9, 6565–6575. [Google Scholar] [CrossRef] [PubMed]
- Van Nimwegen, F.A.; Schaapveld, M.; Janus, C.P.M.; Krol, A.D.G.; Petersen, E.J.; Raemaekers, J.M.M.; Kok, W.E.M.; Aleman, B.M.P.; Van Leeuwen, F.E. Cardiovascular disease after hodgkin lymphoma treatment 40-year disease risk. JAMA Intern. Med. 2015, 175, 1007–1017. [Google Scholar] [CrossRef] [PubMed]
- Aleman, B.M.P.; van den Belt-Dusebout, A.W.; Klokman, W.J.; Van’t Veer, M.B.; Bartelink, H.; van Leeuwen, F.E. Long-term cause-specific mortality of patients treated for Hodgkin’s disease. J. Clin. Oncol. 2003, 21, 3431–3439. [Google Scholar] [CrossRef]
- Gerardi, C.; Allocati, E.; Minoia, C.; Guarini, A.; Banzi, R. Long-term follow-up of classical hodgkin lymphoma and diffuse large B-cell lymphoma survivors: Aims and methodological approach for fondazione italiana linfomi systematic reviews. Cancers 2021, 13, 2976. [Google Scholar] [CrossRef]
- Behringer, K.; Mueller, H.; Goergen, H.; Thielen, I.; Eibl, A.D.; Stumpf, V.; Wessels, C.; Wiehlpütz, M.; Rosenbrock, J.; Halbsguth, T.; et al. Gonadal function and fertility in survivors after Hodgkin lymphoma treatment within the German Hodgkin study group HD13 to HD15 Trials. J. Clin. Oncol. 2013, 31, 231–239. [Google Scholar] [CrossRef]
- Ng, A.K.; van Leeuwen, F.E. Hodgkin lymphoma: Late effects of treatment and guidelines for surveillance. Semin. Hematol. 2016, 53, 209–215. [Google Scholar] [CrossRef]
- Hesketh, P.J.; Kris, M.G.; Basch, E.; Bohlke, K.; Barbour, S.Y.; Clark-Snow, R.A.; Danso, M.A.; Dennis, K.; Dupuis, L.L.; Dusetzina, S.B.; et al. Antiemetics: American Society of Clinical Oncology clinical practice guideline update. J. Clin. Oncol. 2017, 35, 3240–3261. [Google Scholar] [CrossRef]
- Van Staa, T.P.; Leufkens, H.G.M.; Cooper, C. The epidemiology of corticosteroid-induced osteoporosis: A meta-analysis. Osteoporos. Int. 2002, 13, 777–787. [Google Scholar] [CrossRef]
- Weinstein, R.S. Glucocorticoid-Induced Osteoporosis and Osteonecrosis. Endocrinol. Metab. Clin. N. Am. 2012, 41, 595–611. [Google Scholar] [CrossRef]
- Ofshenko, N.; Bercovich, E.; Mashiach, T.; Weiler-Sagie, M.; Militianu, D.; Dann, E.J. Reduction of the Vertebral Bone Mineral Density in Patients with Hodgkin Lymphoma Correlates with Their Age and the Treatment Regimen They Received. Cancers 2022, 14, 495. [Google Scholar] [CrossRef]
- Ko, Y.-S.; Ha, J.H.; Park, J.-W.; Lee, Y.-K.; Kim, T.-Y.; Koo, K.-H. Updating Osteonecrosis of the Femoral Head. Hip. Pelvis. 2023, 35, 147–156. [Google Scholar] [CrossRef]
- Ellis, J.; Macleod, U.; Sammon, D.; Lindsay, E.; Erskine, J.G. Osteonecrosis following treatment for Hodgkin’s disease. Clin. Lab. Haematol. 1994, 16, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Marková, J.; Zídka, M.; Feltl, D.; Mociková, H.K.T. Osteonecrosis as a complication of treating Hodgkin’s lymphoma after BEACOPP chemotherapy. Oncology 2004, 27, 135. [Google Scholar]
- Dann, E.J.; Blumenfeld, Z.; Bar-Shalom, R.; Avivi, I.; Ben-Shachar, M.; Goor, O.; Libster, D.; Gaitini, D.; Rowe, J.M.; Epelbaum, R. A 10-year experience with treatment of high and standard risk Hodgkin disease: Six cycles of tailored BEACOPP, with interim scintigraphy, are effective and female fertility is preserved. Am. J. Hematol. 2012, 87, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Fosså, A.; Fiskvik, I.H.; Kolstad, A.; Lauritzsen, G.F.; Aurlien, E.; Blystad, A.K.; Hole, K.H.; Ikonomou, I.M.; Holte, H. Two escalated followed by six standard BEACOPP in advanced-stage high-risk classical Hodgkin lymphoma: High cure rates but increased risk of aseptic osteonecrosis. Ann. Oncol. 2012, 23, 1254–1259. [Google Scholar] [CrossRef] [PubMed]
- Borchmann, S.; Müller, H.; Haverkamp, H.; Baues, C.; Marková, J.; Hüttmann, A.; Glunz, A.; Fuchs, M.; Borchmann, P.; Engert, A. Symptomatic osteonecrosis as a treatment complication in Hodgkin lymphoma: An analysis of the German Hodgkin Study Group (GHSG). Leukemia 2018, 33, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Basic-Kinda, S.; Karlak, I.; Durakovic, N.; Lubina, Z.I.; Livaja Radman, I.; Dotlic, S.; Peric, Z.; Hude, I.; Aurer, I. High incidence of aseptic hip necrosis in Hodgkin lymphoma patients treated with escalated BEACOPP receiving methylprednisolone. Intern. Med. J. 2018, 48, 523–529. [Google Scholar] [CrossRef]
- Diehl, V.; Franklin, J.; Hasenclever, D.; Tesch, H.; Pfreundschuh, M.; Lathan, B.; Paulus, U.; Sieber, M.; Rueffer, J.U.; Sextro, M.; et al. BEACOPP, a new dose-escalated and accelerated regimen, is at least as effective as COPP/ABVD in patients with advanced-stage Hodgkin’s lymphoma: Interim report from a trial of the German Hodgkin’s Lymphoma Study Group. J. Clin. Oncol. 1998, 16, 3810–3821. [Google Scholar] [CrossRef] [PubMed]
- Disease Stages and Risk Factors-GHSG-German Hodgkin Study Group. Available online: https://en.ghsg.org/disease-stages (accessed on 16 October 2022).
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for initial evaluation, staging, and response assessment of hodgkin and non-hodgkin lymphoma: The lugano classification. J. Clin. Oncol. 2014, 32, 3059–3067. [Google Scholar] [CrossRef] [PubMed]
- Cancer Institute, N. Common Terminology Criteria for Adverse Events (CTCAE) Common Terminology Criteria for Adverse Events (CTCAE) v5.0. 2017. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm (accessed on 30 December 2023).
- Lucijanić, M. Survival analysis in clinical practice: Analyze your own data using an Excel workbook. Croat. Med. J. 2016, 57, 77. [Google Scholar] [CrossRef]
- Borchmann, P.; Goergen, H.; Kobe, C.; Lohri, A.; Greil, R.; Eichenauer, D.A.; Zijlstra, J.M.; Markova, J.; Meissner, J.; Feuring-Buske, M.; et al. PET-guided treatment in patients with advanced-stage Hodgkin’s lymphoma (HD18): Final results of an open-label, international, randomised phase 3 trial by the German Hodgkin Study Group. Lancet 2017, 390, 2790–2802. [Google Scholar] [CrossRef]
- Gopal, A.K.; Chen, R.; Smith, S.E.; Ansell, S.M.; Rosenblatt, J.D.; Savage, K.J.; Connors, J.M.; Engert, A.; Larsen, E.K.; Chi, X.; et al. Durable remissions in a pivotal phase 2 study of brentuximab vedotin in relapsed or refractory Hodgkin lymphoma. Blood 2015, 125, 1236–1243. [Google Scholar] [CrossRef]
- Hude, I.; Sasse, S.; Engert, A.; Bröckelmann, P.J. The emerging role of immune checkpoint inhibition in malignant lymphoma. Haematologica 2017, 102, 30. [Google Scholar] [CrossRef]
- Connors, J.M.; Jurczak, W.; Straus, D.J.; Ansell, S.M.; Kim, W.S.; Gallamini, A.; Younes, A.; Alekseev, S.; Illés, Á.; Picardi, M.; et al. Brentuximab vedotin with chemotherapy for stage III or IV Hodgkin’s lymphoma. N. Engl. J. Med. 2018, 378, 331–344. [Google Scholar] [CrossRef] [PubMed]
- Wongso, D.; Fuchs, M.; Plütschow, A.; Klimm, B.; Sasse, S.; Hertenstein, B.; Maschmeyer, G.; Vieler, T.; Dührsen, U.; Lindemann, W.; et al. Treatment-related mortality in patients with advanced-stage Hodgkin lymphoma: An analysis of the German Hodgkin Study Group. J. Clin. Oncol. 2013, 31, 2819–2824. [Google Scholar] [CrossRef] [PubMed]
- Borchmann, P.; Haverkamp, H.; Diehl, V.; Cerny, T.; Markova, J.; Ho, A.D.; Eich, H.T.; Mueller-Hermelink, H.K.; Kanz, L.; Greil, R.; et al. Eight cycles of escalated-dose BEACOPP compared with four cycles of escalated-dose BEACOPP followed by four cycles of baseline-dose BEACOPP with or without radiotherapy in patients with advanced-stage hodgkin’s lymphoma: Final analysis of the HD12 trial of the German Hodgkin Study Group. J. Clin. Oncol. 2011, 29, 4234–4242. [Google Scholar]
- Johnson, P.; Federico, M.; Kirkwood, A.; Fosså, A.; Berkahn, L.; Carella, A.; d’Amore, F.; Enblad, G.; Franceschetto, A.; Fulham, M.; et al. Adapted Treatment Guided by Interim PET-CT Scan in Advanced Hodgkin’s Lymphoma. N. Engl. J. Med. 2016, 374, 2419–2429. [Google Scholar] [CrossRef] [PubMed]
- Gallamini, A.; Patti, C.; Viviani, S.; Rossi, A.; Fiore, F.; Di Raimondo, F.; Cantonetti, M.; Stelitano, C.; Feldman, T.; Gavarotti, P.; et al. Early chemotherapy intensification with BEACOPP in advanced-stage Hodgkin lymphoma patients with a interim-PET positive after two ABVD courses. Br. J. Haematol. 2011, 152, 551–560. [Google Scholar] [CrossRef] [PubMed]
- Barrington, S.F.; Kirkwood, A.A.; Franceschetto, A.; Fulham, M.J.; Roberts, T.H.; Almquist, H.; Brun, E.; Hjorthaug, K.; Viney, Z.N.; Pike, L.C.; et al. PET-CT for staging and early response: Results from the Response-Adapted Therapy in Advanced Hodgkin Lymphoma study. Blood 2016, 127, 1531–1538. [Google Scholar] [CrossRef] [PubMed]
- Radford, J.; Illidge, T.; Counsell, N.; Hancock, B.; Pettengell, R.; Johnson, P.; Wimperis, J.; Culligan, D.; Popova, B.; Smith, P.; et al. Results of a Trial of PET-Directed Therapy for Early-Stage Hodgkin’s Lymphoma. N. Engl. J. Med. 2015, 372, 1598–1607. [Google Scholar] [CrossRef]
- Kedmi, M.; Apel, A.; Davidson, T.; Levi, I.; Dann, E.J.; Polliack, A.; Ben-Bassat, I.; Nagler, A.; Avigdor, A. High-Risk, Advanced-Stage Hodgkin Lymphoma: The Impact of Combined Escalated BEACOPP and ABVD Treatment in Patients Who Rapidly Achieve Metabolic Complete Remission on Interim FDG-PET/CT Scan. Acta Haematol. 2016, 135, 156–161. [Google Scholar] [CrossRef]
- Damaschin, C.; Goergen, H.; Kreissl, S.; Plütschow, A.; Breywisch, F.; Mathas, S.; Meissner, J.; Sökler, M.; Topp, M.S.; Vucinic, V.; et al. Brentuximab vedotin-containing escalated BEACOPP variants for newly diagnosed advanced-stage classical Hodgkin lymphoma: Follow-up analysis of a randomized phase II study from the German Hodgkin Study Group. Leukemia 2022, 36, 580–582. [Google Scholar] [CrossRef]
- Borchmann, P.; Moccia, A.A.; Greil, R.; Schneider, G.; Hertzberg, M.; Schaub, V.; Hüttmann, A.; Keil, F.; Dierlamm, J.; Hänel, M.; et al. Brecadd is non-inferior to ebeacopp in patients with advanced stage classical hodgkin lymphoma: Efficacy results of the ghsg phase iii hd21 trial. Hematol. Oncol. 2023, 41, 881–882. [Google Scholar] [CrossRef]

{kind=link}
| Demographics | No Pts | |
|---|---|---|
| Total | 162 | |
| age (y) | ||
| min | 19 | |
| max | 59 | |
| median | 31 | |
| sex | ||
| male | 88 | |
| female | 74 | |
| stage | ||
| EU | 33 | |
| AS | 129 | |
| Bulky? | yes | 62 |
| Treatment | No of Pts |
|---|---|
| 6eBEACOPP | 98 |
| 4eBEACOPP | 12 |
| 2eBEACOPP + 2A(B)VD | 31 |
| 2eBEACOPP + 4ABVD | 1 |
| 4eBEACOPP + 2A(B)VD | 1 |
| 4eBEACOPP + 4A(B)VD | 3 |
| 5eBEACOPP + 1ABVD | 1 |
| 4eBEACOPP + 4b(BEA)COPP | 11 |
| 2eBEACOPP | 2 |
| 6eBEACOPP+2ABVD | 1 |
| 3eBEACOPP + 2ABVD + 2AVD | 1 |
| Emergency Hospitalization during Front Line Treatment | Short Course Corticosteroids | Standard Course Corticosteroids | p Value |
|---|---|---|---|
| % (No/Total) | % (No/Total) | ||
| Hospitalization (for any reason) | 53 (33/68) | 46 (43/94) | 0.75 |
| Febrile neutropenia | 43 (29/68) | 38 (36/94) | 0.62 |
| Treatment related death | 0 | 2% (2/94) | / |
| Late effects | |||
| Secondary neoplasms | 4 (3/68) | 2 (2/94) | 0.65 |
| Duration of Corticosteroid Treatment | Patient Designation | Description of Events | CTCAE Grade | Comment |
|---|---|---|---|---|
| short | Pt No 19 | femoroacetabular impigement, osteitis pubis, sacroileitis, ishiofemoral collision | 3 | affecting every-day living and limiting self-care |
| Pt No 20 | Mb Freiberg | 3 | right foot | |
| Pt No 68 | periarthritis humeroscapularis | 2 | right sided; had right supraclavicular lymphadenopathy at diagnosis | |
| standard | Pt No 78 | coxarthrosis | 2 | billateral |
| Pt No 111 | AVN | 3 | hip, right | |
| Pt No 112 | humeroscapular arthrosis | 2 | billateral, dominantly left, initially had lymphadenopathy in left neck regions | |
| Pt No 141 | tendinitis humeroscapularis; osteoporosis with pathological fractures | 3 | right hand side, initial lymphadenopathy on both sides of neck | |
| Pt No 142 | AVN | 3 | hips, billateral | |
| Pt No 143 | periarthritis humeroscapularis | 2 | billateral, had mediastinal irradiation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hude Dragičević, I.; Bašić-Kinda, S.; Markotić, H.; Morić-Perić, M.; Dujmović, D.; Radman, I.; Dreta, B.; Dotlić, S.; Ilić, I.; Galunić Bilić, L.; et al. Reduced Corticosteroid Exposure Is Safe and Does Not Reduce Disease Control among Hodgkin Lymphoma Patients Treated with Escalated BEACOPP (eBEACOPP). Medicina 2024, 60, 430. https://doi.org/10.3390/medicina60030430
Hude Dragičević I, Bašić-Kinda S, Markotić H, Morić-Perić M, Dujmović D, Radman I, Dreta B, Dotlić S, Ilić I, Galunić Bilić L, et al. Reduced Corticosteroid Exposure Is Safe and Does Not Reduce Disease Control among Hodgkin Lymphoma Patients Treated with Escalated BEACOPP (eBEACOPP). Medicina. 2024; 60(3):430. https://doi.org/10.3390/medicina60030430
Chicago/Turabian StyleHude Dragičević, Ida, Sandra Bašić-Kinda, Helena Markotić, Martina Morić-Perić, Dino Dujmović, Ivo Radman, Barbara Dreta, Snježana Dotlić, Ivana Ilić, Lea Galunić Bilić, and et al. 2024. "Reduced Corticosteroid Exposure Is Safe and Does Not Reduce Disease Control among Hodgkin Lymphoma Patients Treated with Escalated BEACOPP (eBEACOPP)" Medicina 60, no. 3: 430. https://doi.org/10.3390/medicina60030430
APA StyleHude Dragičević, I., Bašić-Kinda, S., Markotić, H., Morić-Perić, M., Dujmović, D., Radman, I., Dreta, B., Dotlić, S., Ilić, I., Galunić Bilić, L., Dobrenić, M., Kralik, M., & Aurer, I. (2024). Reduced Corticosteroid Exposure Is Safe and Does Not Reduce Disease Control among Hodgkin Lymphoma Patients Treated with Escalated BEACOPP (eBEACOPP). Medicina, 60(3), 430. https://doi.org/10.3390/medicina60030430